
Physical Activity of Young Patients following Minimally Invasive Lateral Unicompartmental Knee Replacement
Abstract
1. Introduction
2. Patients and Methods
Statistics
3. Results
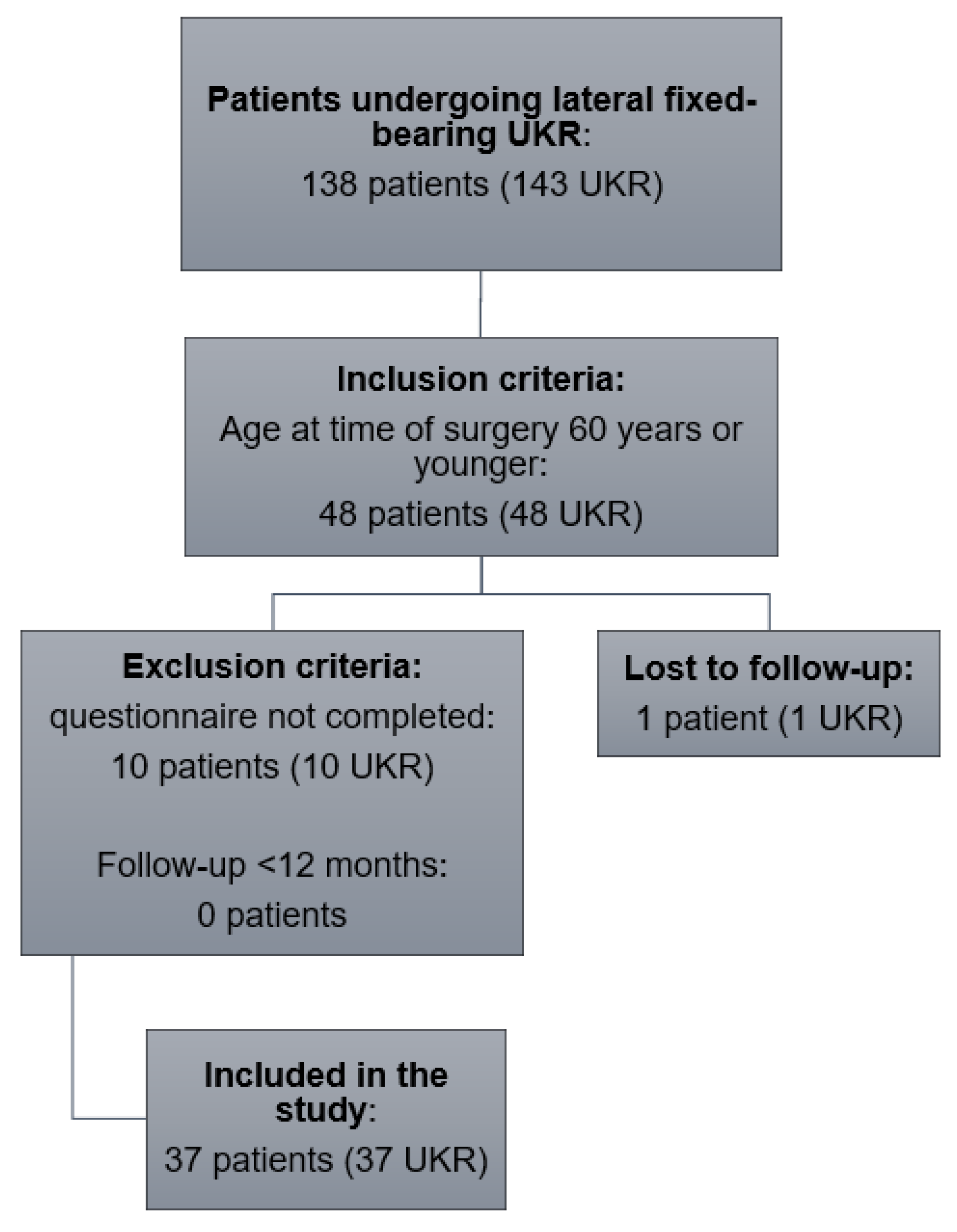
3.1. Demographics
3.2. Reoperation
3.3. Patient-Reported Outcome Measures
3.4. Radiological Outcome
3.5. Sporting Activities and Participation
3.6. Extent of Activities
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mohammad, H.R.; Kennedy, J.A.; Mellon, S.J.; Judge, A.; Dodd, C.A.; Murray, D.W. Ten-year clinical and radiographic results of 1000 cementless Oxford unicompartmental knee replacements. Knee Surg. Sport. Traumatol. Arthrosc. 2020, 28, 1479–1487. [Google Scholar] [CrossRef]
- Pandit, H.; Jenkins, C.; Gill, H.S.; Barker, K.; Dodd, C.A.; Murray, D.W. Minimally invasive Oxford phase 3 unicompartmental knee replacement: Results of 1000 cases. J. Bone Jt. Surg. Br. 2011, 93, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Liddle, A.D.; Judge, A.; Pandit, H.; Murray, D.W. Adverse outcomes after total and unicompartmental knee replacement in 101,330 matched patients: A study of data from the National Joint Registry for England and Wales. Lancet 2014, 384, 1437–1445. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, A.V., Jr.; Berend, K.R.; Walter, C.A.; Aziz-Jacobo, J.; Cheney, N.A. Is recovery faster for mobile-bearing unicompartmental than total knee arthroplasty? Clin. Orthop. Relat. Res. 2009, 467, 1450–1457. [Google Scholar] [CrossRef]
- Murray, D.W.; Liddle, A.D.; Dodd, C.A.; Pandit, H. Unicompartmental knee arthroplasty: Is the glass half full or half empty? Bone Jt. J. 2015, 97, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Liddle, A.D.; Pandit, H.; Judge, A.; Murray, D.W. Patient-reported outcomes after total and unicompartmental knee arthroplasty: A study of 14,076 matched patients from the national joint registry for England and Wales. Bone Jt. J. 2015, 97, 793–801. [Google Scholar] [CrossRef] [PubMed]
- Ollivier, M.; Parratte, S.; Argenson, J.N. Results and outcomes of unicompartmental knee arthroplasty. Orthop. Clin. North Am. 2013, 44, 287–300. [Google Scholar] [CrossRef]
- Bourne, R.B.; Chesworth, B.M.; Davis, A.M.; Mahomed, N.N.; Charron, K.D. Patient satisfaction after total knee arthroplasty: Who is satisfied and who is not? Clin. Orthop. Relat. Res. 2010, 468, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Presti, M.L.; Costa, G.G.; Cialdella, S.; Agrò, G.; Grassi, A.; Caravelli, S.; Mosca, M.; Muccioli, G.M.M.; Zaffagnini, S. Return to sports after unicompartmental knee arthroplasty: Reality or utopia? A 48-month follow-up prospective study. J. Knee Surg. 2019, 32, 186–191. [Google Scholar] [CrossRef]
- Walker, T.; Streit, J.; Gotterbarm, T.; Bruckner, T.; Merle, C.; Streit, M.R. Sports, physical activity and patient-reported outcomes after medial unicompartmental knee arthroplasty in young patients. J. Arthroplast. 2015, 30, 1911–1916. [Google Scholar] [CrossRef]
- Canetti, R.; Batailler, C.; Bankhead, C.; Neyret, P.; Servien, E.; Lustig, S. Faster return to sport after robotic-assisted lateral unicompartmental knee arthroplasty: A comparative study. Arch. Orthop. Trauma Surg. 2018, 138, 1765–1771. [Google Scholar] [CrossRef] [PubMed]
- Panzram, B.; Mandery, M.; Reiner, T.; Walker, T.; Merle, C.; Gotterbarm, T. Fast return to sports and high level of activity after cementless oxford unicompartmental knee arthroplasty. J. Knee Surg. 2021, 34, 1212–1219. [Google Scholar] [CrossRef] [PubMed]
- Tokuhara, Y.; Kadoya, Y.; Nakagawa, S.; Kobayashi, A.; Takaoka, K. The flexion gap in normal knees: An MRI study. J. Bone Jt. Surg. 2004, 86, 1133–1136. [Google Scholar] [CrossRef]
- Nakagawa, S.; Kadoya, Y.; Todo, S.; Kobayashi, A.; Sakamoto, H.; Freeman, M.A.R.; Yamano, Y. Tibiofemoral movement 3: Full flexion in the living knee studied by MRI. J. Bone Jt. Surg. 2000, 82, 1199–1200. [Google Scholar] [CrossRef]
- Bare, J.V.; Gill, H.S.; Beard, D.J.; Murray, D.W. A convex lateral tibial plateau for knee replacement. Knee 2006, 13, 122–126. [Google Scholar] [CrossRef]
- Notarnicola, A.; Maccagnano, G.; Fiore, A.; Spinarelli, A.; Montenegro, L.; Paoloni, M.; Pastore, F.; Tafuri, S.; Moretti, B. Baropodometry on patients after total knee arthroplasty. Musculoskelet. Surg. 2018, 102, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Walker, T.; Gotterbarm, T.; Bruckner, T.; Merle, C.; Streit, M.R. Return to sports, recreational activity and patient-reported outcomes after lateral unicompartmental knee arthroplasty. Knee Surg. Sport. Traumatol. Arthrosc. 2015, 23, 3281–3287. [Google Scholar] [CrossRef]
- Zimmerer, A.; Navas, L.; Kinkel, S.; Weiss, S.; Hauschild, M.; Miehlke, W.; Streit, M. Sports activity and patient-related outcomes after fixed-bearing lateral unicompartmental knee arthroplasty. Knee 2021, 28, 64–71. [Google Scholar] [CrossRef]
- Walker, T.; Hariri, M.; Eckert, J.; Panzram, B.; Reiner, T.; Merle, C.; Gotterbarm, T.; Moradi, B. Minimally invasive lateral unicompartmental knee replacement: Early results from an independent center using the Oxford fixed lateral prosthesis. Knee 2020, 27, 235–241. [Google Scholar] [CrossRef]
- Briggs, K.K.; Steadman, J.R.; Hay, C.J.; Hines, S.L. Lysholm score and Tegner activity level in individuals with normal knees. Am. J. Sport. Med. 2009, 37, 898–901. [Google Scholar] [CrossRef]
- Zahiri, C.A.; Schmalzried, T.P.; Szuszczewicz, E.S.; Amstutz, H.C. Assessing activity in joint replacement patients. J. Arthroplast. 1998, 13, 890–895. [Google Scholar] [CrossRef] [PubMed]
- Ware, J., Jr.; Kosinski, M.; Keller, S.D. A 12-item short-form health survey: Construction of scales and preliminary tests of reliability and validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef] [PubMed]
- Ho, J.C.; Stitzlein, R.N.; Green, C.J.; Stoner, T.; Froimson, M.I. Return to sports activity following UKA and TKA. J. Knee Surg. 2016, 29, 254–259. [Google Scholar] [CrossRef] [PubMed]
- Pietschmann, M.F.; Wohlleb, L.; Weber, P.; Schmidutz, F.; Ficklscherer, A.; Gulecyuz, M.F.; Safi, E.; Niethammer, T.R.; Jansson, V.; Müller, C.P.E. Sports activities after medial unicompartmental knee arthroplasty Oxford III-what can we expect? Int. Orthop. 2013, 37, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Hopper, G.P.; Leach, W.J. Participation in sporting activities following knee replacement: Total versus unicompartmental. Knee Surg. Sport. Traumatol. Arthrosc. 2008, 16, 973–979. [Google Scholar] [CrossRef]
- Chatterji, U.; Ashworth, M.J.; Lewis, P.L.; Dobson, P.J. Effect of total knee arthroplasty on recreational and sporting activity. ANZ J. Surg. 2005, 75, 405–408. [Google Scholar] [CrossRef]
- Matthews, D.J.; Hossain, F.S.; Patel, S.; Haddad, F.S. A cohort study predicts better functional outcomes and equivalent patient satisfaction following UKR compared with TKR. HSS J. 2013, 9, 21–24. [Google Scholar] [CrossRef]
- Plassard, J.; Masson, J.B.; Malatray, M.; Swan, J.; Luceri, F.; Roger, J.; Batailler, C.; Servien, E.; Lustig, S. Factors lead to return to sports and recreational activity after total knee replacement—A retrospective study. SICOT J. 2020, 6, 11. [Google Scholar] [CrossRef]
- Yang, K.Y.; Wang, M.C.; Yeo, S.J.; Lo, N.N. Minimally invasive unicondylar versus total condylar knee arthroplasty-early results of a matched-pair comparison. Singap. Med. J. 2003, 44, 559–562. [Google Scholar]
- Spinarelli, A.; Pesce, V.; Campagna, C.; Maccagnano, G.; Moretti, B. Painful knee prosthesis: CT scan to assess patellar angle and implant malrotation. Muscles Ligaments Tendons J. 2016, 6, 461–466. [Google Scholar] [CrossRef]
- Dagneaux, L.; Bourlez, J.; Degeorge, B.; Canovas, F. Return to sport after total or unicompartmental knee arthroplasty: An informative guide for residents to patients. EFORT Open Rev. 2017, 2, 496–501. [Google Scholar] [CrossRef]
- Healy, W.L.; Iorio, R.; Lemos, M.J. Athletic activity after joint replacement. Am. J. Sport. Med. 2001, 29, 377–388. [Google Scholar] [CrossRef]
- Kennedy, J.A.; Burn, E.; Mohammad, H.R.; Mellon, S.J.; Judge, A.; Murray, D.W. Lifetime revision risk for medial unicompartmental knee replacement is lower than expected. Knee Surg. Sport. Traumatol. Arthrosc. 2020, 28, 3935–3941. [Google Scholar] [CrossRef] [PubMed]
- Jassim, S.S.; Douglas, S.L.; Haddad, F.S. Athletic activity after lower limb arthroplasty: A systematic review of current evidence. Bone Jt. J. 2014, 96, 923–927. [Google Scholar] [CrossRef] [PubMed]
- Naal, F.D.; Fischer, M.; Preuss, A.; Goldhahn, J.; von Knoch, F.; Preiss, S.; Munzinger, U.; Drobny, T. Return to sports and recreational activity after unicompartmental knee arthroplasty. Am. J. Sport. Med. 2007, 35, 1688–1695. [Google Scholar] [CrossRef] [PubMed]
- Fisher, N.; Agarwal, M.; Reuben, S.F.; Johnson, D.S.; Turner, P.G. Sporting and physical activity following Oxford medial unicompartmental knee arthroplasty. Knee 2006, 13, 296–300. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.R.; Robinson, J.R.; Porteous, A.J.; Murray, J.R.; Hassaballa, M.A.; Artz, N.; Newman, J.H. Fixed bearing lateral unicompartmental knee arthroplasty-short to midterm survivorship and knee scores for 101 prostheses. Knee 2014, 21, 843–847. [Google Scholar] [CrossRef]
- Asadollahi, S.; Wilson, H.A.; Thomson, F.R.; Vaz, K.; Middleton, R.; Jenkins, C.; Alvand, A.; Bottomley, N.; Dodd, C.A.; Price, A.J.; et al. Early results of fixed-bearing unicompartmental knee replacement designed for the lateral compartment. J. Orthop. Surg. Res. 2022, 17, 146. [Google Scholar] [CrossRef]
- Pandit, H.; Jenkins, C.; Beard, D.J.; Price, A.J.; Gill, H.S.; Dodd, C.A.F.; Murray, D.W. Mobile bearing dislocation in lateral unicompartmental knee replacement. Knee 2010, 17, 392–397. [Google Scholar] [CrossRef]
- Weston-Simons, J.S.; Pandit, H.; Kendrick, B.J.; Jenkins, C.; Barker, K.; Dodd, C.A.F.; Murray, D.W. The mid-term outcomes of the Oxford domed lateral unicompartmental knee replacement. Bone Jt. J. 2014, 96, 59–64. [Google Scholar] [CrossRef]
- Kim, K.T.; Lee, S.; Kim, J.; Kim, J.W.; Kang, M.S. Clinical results of lateral unicompartmental knee arthroplasty: Minimum 2-year follow-up. Clin. Orthop. Surg. 2016, 8, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Demange, M.K.; Von Keudell, A.; Probst, C.; Yoshioka, H.; Gomoll, A.H. Patient-specific implants for lateral unicompartmental knee arthroplasty. Int. Orthop. 2015, 39, 1519–1526. [Google Scholar] [CrossRef] [PubMed]
- Lustig, S.; Lording, T.; Frank, F.; Debette, C.; Servien, E.; Neyret, P. Progression of medial osteoarthritis and long term results of lateral unicompartmental arthroplasty: 10 to 18 year follow-up of 54 consecutive implants. Knee 2014, 21, S26–S32. [Google Scholar] [CrossRef] [PubMed]
- Streit, M.R.; Streit, J.; Walker, T.; Bruckner, T.; Philippe, K.J.; Ewerbeck, V.; Merle, C.; Aldinger, P.R.; Gotterbarm, T. Minimally invasive Oxford medial unicompartmental knee arthroplasty in young patients. Knee Surg. Sport. Traumatol. Arthrosc. 2017, 25, 660–668. [Google Scholar] [CrossRef]
- Neufeld, M.E.; Albers, A.; Greidanus, N.V.; Garbuz, D.S.; Masri, B.A. A comparison of mobile and fixed-bearing unicompartmental knee arthroplasty at a minimum 10-Year follow-up. J. Arthroplast. 2018, 33, 1713–1718. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | |
|---|---|
| Number of patients | 37 |
| Mean follow-up in years (±SD) | 3.1 ± 1.5 |
| Mean age at time of surgery in years (±SD) | 52.8 ± 3.1 |
| Gender (%) | Female 22 (59.5%); Male 15 (40.5%) |
| Operated side (%) | Left 12 (32.4%); Right 25 (67.6%) |
| Mean body mass index (kg/m2) (±SD) | 30.0 ± 6.8 |
| Preoperative (Mean ± SD) | Postoperative (Mean ± SD) | |
|---|---|---|
| OKS *** | 26.9 ± 9.0 | 39.9 ± 8.1 |
| ROM *** | 121 ± 14.8 | 136 ± 9.3 |
| VAS *** | 7 ± 2.1 | 1.7 ± 2.1 |
| UCLA *** | 3.6 ± 1.8 | 6 + 1.5 |
| TAS *** | 2.2 ± 1.3 | 3.3 ± 1.3 |
| SF12-PCS | - | 43.43 ± 10.7 |
| SF12-MCS | - | 45.97 ± 11.1 |
| Physical Activity | Number of Patients Participating before Surgery (n/%) | Number of Patients Participating after Surgery (n/%) | Difference (n/%) |
|---|---|---|---|
| None | 5 (13.5) | 7 (18.9) | +2 (+ 5.4) |
| Biking | 23 (62.2) | 21 (56.8) | −2 (−5.4) |
| Hiking | 16 (43.2) | 13 (35.1) | −3 (−8.1) |
| Alpine skiing | 1 (2.7) | 0 (0) | −1 (−2.7) |
| Jogging | 4 (10.8) | 1 (2.7) | −3 (−8.1) |
| Golf | 1 (2.7) | 1 (2.7) | 0 (0) |
| Soccer | 6 (16.2) | 1 (2.7) | −5 (−13.5) * |
| Tennis | 2 (5.4) | 0 (0) | −2 (−5.4) |
| Nordic walking | 8 (21.6) | 8 (21.8) | 0 (0) |
| Hand-, Volley- and Basketball | 4 (10.8) | 1 (2.7) | −3 (−8.1) |
| Aqua aerobics | 3 (8.1) | 1 (2.7) | −2 (−5.4) |
| Long walks | 12 (32.4) | 11 (29.7) | −1 (−2.7) |
| Fitness training | 8 (21.6) | 6 (16.2) | −2 (−5.4) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hariri, M.; Hagemann, M.; Mick, P.; Deisenhofer, J.; Panzram, B.; Innmann, M.; Reiner, T.; Renkawitz, T.; Walker, T. Physical Activity of Young Patients following Minimally Invasive Lateral Unicompartmental Knee Replacement. J. Clin. Med. 2023, 12, 635. https://doi.org/10.3390/jcm12020635
Hariri M, Hagemann M, Mick P, Deisenhofer J, Panzram B, Innmann M, Reiner T, Renkawitz T, Walker T. Physical Activity of Young Patients following Minimally Invasive Lateral Unicompartmental Knee Replacement. Journal of Clinical Medicine. 2023; 12(2):635. https://doi.org/10.3390/jcm12020635
Chicago/Turabian StyleHariri, Mustafa, Merlin Hagemann, Paul Mick, Julian Deisenhofer, Benjamin Panzram, Moritz Innmann, Tobias Reiner, Tobias Renkawitz, and Tilman Walker. 2023. "Physical Activity of Young Patients following Minimally Invasive Lateral Unicompartmental Knee Replacement" Journal of Clinical Medicine 12, no. 2: 635. https://doi.org/10.3390/jcm12020635
APA StyleHariri, M., Hagemann, M., Mick, P., Deisenhofer, J., Panzram, B., Innmann, M., Reiner, T., Renkawitz, T., & Walker, T. (2023). Physical Activity of Young Patients following Minimally Invasive Lateral Unicompartmental Knee Replacement. Journal of Clinical Medicine, 12(2), 635. https://doi.org/10.3390/jcm12020635