

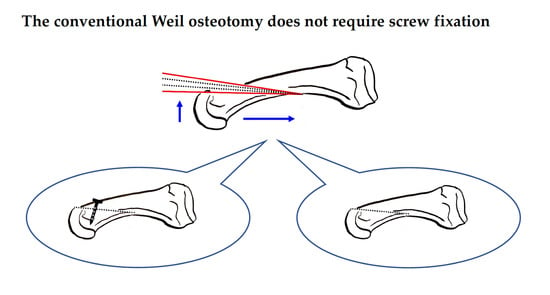
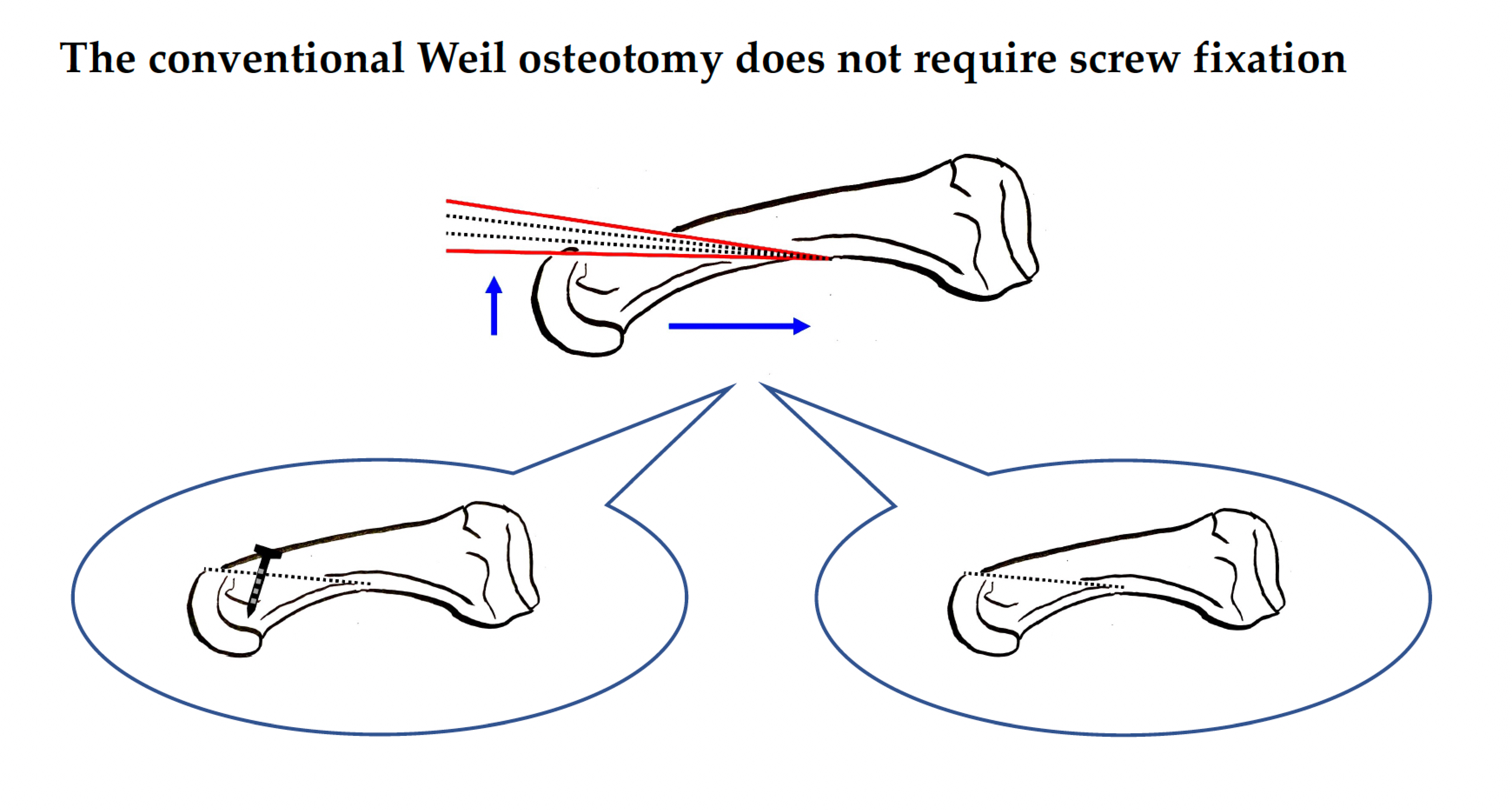
The Conventional Weil Osteotomy Does Not Require Screw Fixation

 ,
, 
(This article belongs to the Section Orthopedics)
Abstract
1. Introduction
2. Patients and Methods
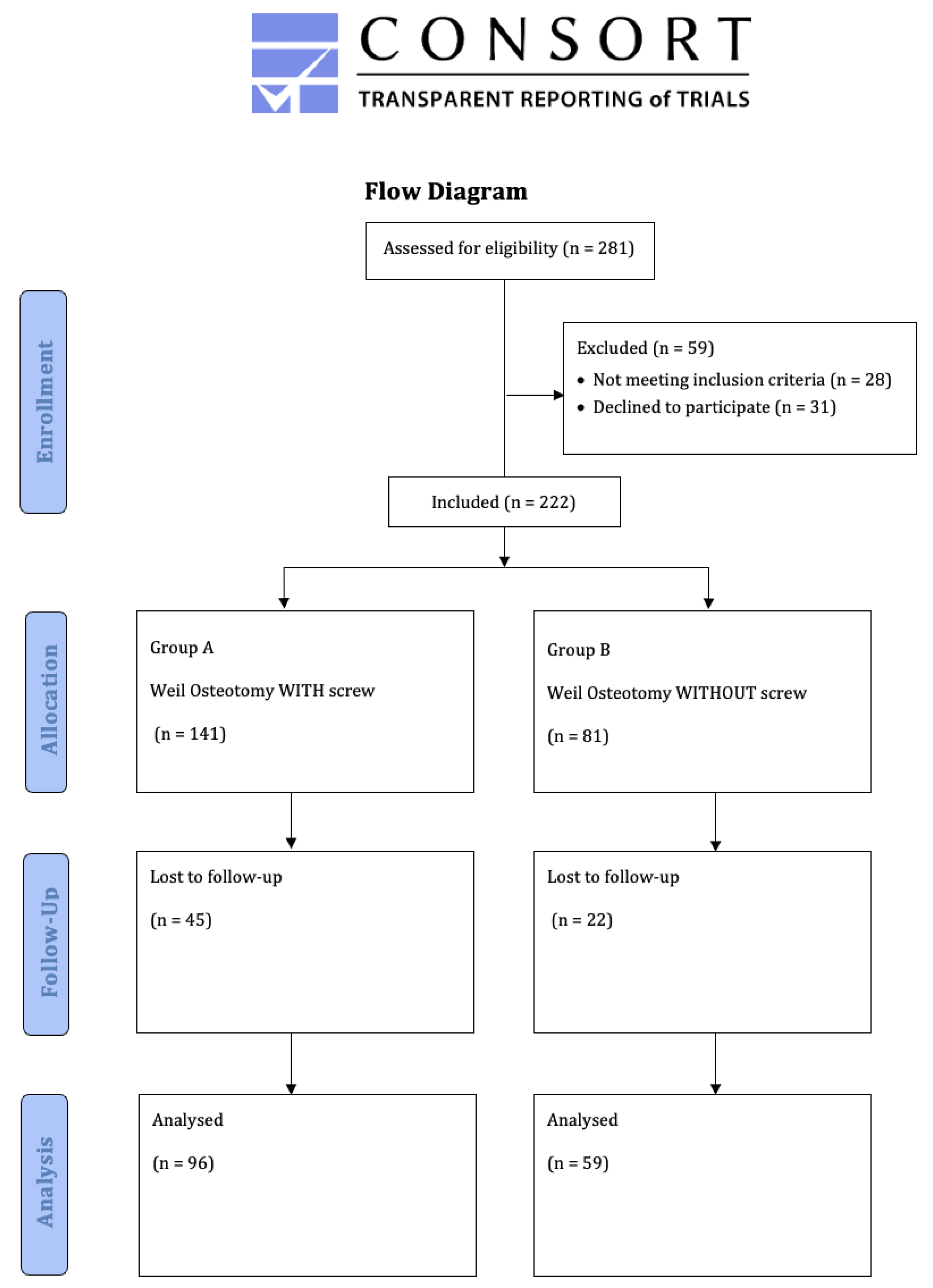
2.1. Population
2.2. Inclusion and Exclusion Criteria
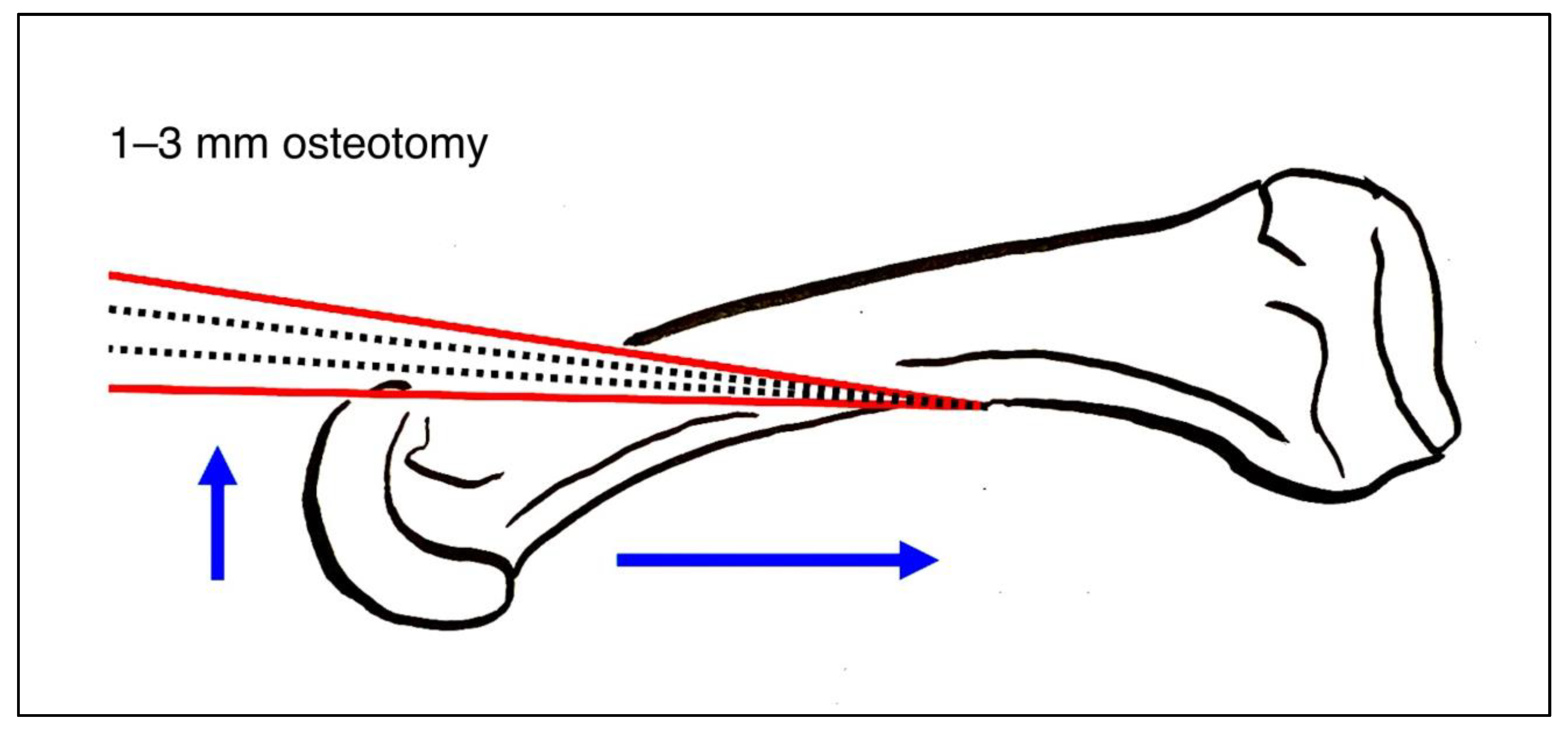
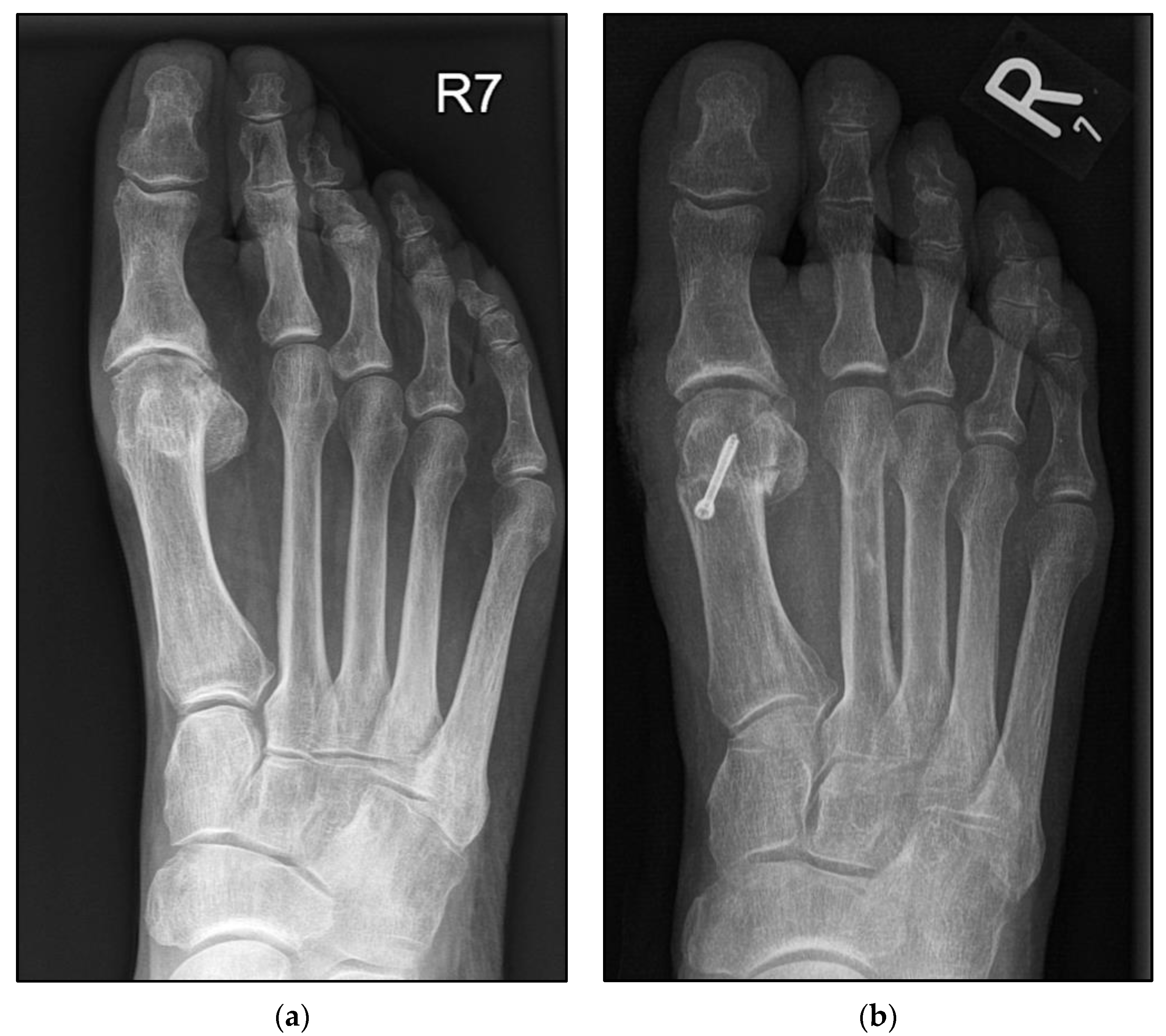
2.3. Surgical Procedure Using the Second Metatarsal as an Example
2.4. Rehabilitation Protocol
2.5. Assessment Methods
2.6. Statistical Analysis
3. Results
Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Henry, J.; Besse, J.L.; Fessy, M.H. Distal osteotomy of the lateral metatarsals: A series of 72 cases comparing the Weil osteotomy and the DMMO percutaneous osteotomy. Orthop. Traumatol. Surg. Res. 2011, 97, S57–S65. [Google Scholar] [CrossRef] [PubMed]
- Yeo, N.E.; Loh, B.; Chen, J.Y.; Yew, A.K.; Ng, S.Y. Comparison of early outcome of Weil osteotomy and distal metatarsal mini-invasive osteotomy for lesser toe metatarsalgia. J. Orthop. Surg. 2016, 24, 350–353. [Google Scholar] [CrossRef] [PubMed]
- Johansen, J.K.; Jordan, M.; Thomas, M. Clinical and radiological outcomes after Weil osteotomy compared to distal metatarsal metaphyseal osteotomy in the treatment of metatarsalgia—A prospective study. Foot. Ankle Surg. 2019, 25, 488–494. [Google Scholar] [CrossRef]
- Thomas, M.; Jordan, M. Minimally invasive correction of lesser toe deformities and treatment of metatarsalgia. Oper. Orthop. Traumatol. 2018, 30, 171–183. [Google Scholar] [CrossRef]
- Wagner, E.; O’Connell, L.A.; Radkievich, R.; Caicedo, N.; Mococain, P.; Wagner, P. Incidence of and Functional Significance of Floating Toe After Weil Osteotomy. Foot. Ankle Orthop. 2019, 4, 2473011419891956. [Google Scholar] [CrossRef] [PubMed]
- Krenn, S.; Albers, S.; Bock, P.; Mansfield, C.; Chraim, M.; Trnka, H.J. Minimally Invasive Distal Metatarsal Metaphyseal Osteotomy of the Lesser Toes: Learning Curve. Foot. Ankle Spec. 2018, 11, 263–268. [Google Scholar] [CrossRef]
- O’Kane, C.; Kilmartin, T.E. The surgical management of central metatarsalgia. Foot. Ankle Int. 2002, 23, 415–419. [Google Scholar] [CrossRef]
- Fleischer, A.E.; Klein, E.E.; Bowen, M.; McConn, T.P.; Sorensen, M.D.; Weil, L., Jr. Comparison of Combination Weil Metatarsal Osteotomy and Direct Plantar Plate Repair Versus Weil Metatarsal Osteotomy Alone for Forefoot Metatarsalgia. J. Foot Ankle Surg. 2020, 59, 303–306. [Google Scholar] [CrossRef]
- Reddy, V.B. Metatarsal Osteotomies: Complications. Foot. Ankle Clin. 2018, 23, 47–55. [Google Scholar] [CrossRef]
- Schuh, R.; Trnka, H.J. Metatarsalgia: Distal metatarsal osteotomies. Foot Ankle Clin. 2011, 16, 583–595. [Google Scholar] [CrossRef]
- Gould, J. Other Lesser Toe Problems. In The Handbook of Foot and Ankle Surgery: An Intellectual Approach to Complex Problems; JP Medical Ltd.: London, UK, 2013; p. 61. [Google Scholar] [CrossRef]
- Robinson, A.H.N.; Bhatia, M. Disorders of the forefoot. In Oxford Textbook of Trauma and Orthopaedics; Bulstrode, C., Wilson-MacDonald, J., Eastwood, D.M., McMaster, J., Fairbank, J., Singh, P.J., Bawa, S., Gikas, P.D., Bunker, T., Giddins, G., et al., Eds.; Oxford University Press: Oxford, UK, 2011; p. 0. [Google Scholar]
- Garg, R.; Thordarson, D.B.; Schrumpf, M.; Castaneda, D. Sliding oblique versus segmental resection osteotomies for lesser metatarsophalangeal joint pathology. Foot Ankle Int. 2008, 29, 1009–1014. [Google Scholar] [CrossRef] [PubMed]
- Trieb, K.; Hofstaetter, S.G.; Panotopoulos, J.; Wanivenhaus, A. The Weil osteotomy for correction of the severe rheumatoid forefoot. Int. Orthop. 2013, 37, 1795–1798. [Google Scholar] [CrossRef] [PubMed]
- Bobrov, D.S.; Slinjakov, L.J.; Rigin, N.V. The Primary Metatarsalgia: Pathogenesis, Biomechanics and Surgical Treatment. Vestn. Ross. Akad. Med. Nauk. 2017, 72, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Mocoçain Mac-iver, P.E.; Valderrama, C.; Radkievich, R.D.; Elgueta, S.; Salinas, D.A.; Díaz, A.K.; Zanolli de Solminihac, D.H. Incidence and Functional Impact of Floating Toe after Distal Metatarsal Minimal Invasive Osteotomy Compared to Open Modified Weil Osteotomy. Foot Ankle Orthop. 2022, 7, 2473011421S00818. [Google Scholar] [CrossRef]
- Highlander, P.; VonHerbulis, E.; Gonzalez, A.; Britt, J.; Buchman, J. Complications of the Weil osteotomy. Foot Ankle Spec. 2011, 4, 165–170. [Google Scholar] [CrossRef]
- Garcia-Fernandez, D.; Gil-Garay, E.; Lora-Pablos, D.; De-la-Cruz-Bertolo, J.; Llanos-Alcazar, L.F. Comparative study of the Weil osteotomy with and without fixation. Foot Ankle Surg. 2011, 17, 103–107. [Google Scholar] [CrossRef]
- Hofstaetter, S.G.; Hofstaetter, J.G.; Petroutsas, J.A.; Gruber, F.; Ritschl, P.; Trnka, H.J. The Weil osteotomy: A seven-year follow-up. J. Bone Joint. Surg. Br. 2005, 87, 1507–1511. [Google Scholar] [CrossRef]
- Migues, A.; Slullitel, G.; Bilbao, F.; Carrasco, M.; Solari, G. Floating-toe deformity as a complication of the Weil osteotomy. Foot Ankle Int. 2004, 25, 609–613. [Google Scholar] [CrossRef]
- Vandeputte, G.; Dereymaeker, G.; Steenwerckx, A.; Peeraer, L. The Weil osteotomy of the lesser metatarsals: A clinical and pedobarographic follow-up study. Foot Ankle Int. 2000, 21, 370–374. [Google Scholar] [CrossRef]
- Bougiouklis, D.; Tyllianakis, M.; Deligianni, D.; Panagiotopoulos, E. Comparison of the Weil and Triple Weil Osteotomies: A Clinical Retrospective Study. Cureus 2022, 14, e22220. [Google Scholar] [CrossRef]
- Fatima, M.; Ektas, N.; Scholes, C.; Symes, M.; Wines, A. The effect of osteotomy technique (flat-cut vs wedge-cut Weil) on pain relief and complication incidence following surgical treatment for metatarsalgia in a private metropolitan clinic: Protocol for a randomised controlled trial. Trials 2022, 23, 690. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | With Screw (n = 96) | Without Screw (n = 59) | All (n = 155) | p | |
|---|---|---|---|---|---|
| Age, years | Mean | 63.37 | 62.37 | 62.99 | 0.620 |
| SEM | 1.31 | 1.39 | 0.97 | ||
| Minimum | 26.00 | 33.00 | 26.00 | ||
| Maximum | 88.00 | 83.00 | 88.00 | ||
| BMI, kg/m2 | Mean | 26.91 | 25.72 | 26.465 | 0.174 |
| SEM | 0.56 | 0.62 | 0.422 | ||
| Minimum | 17.78 | 19.300 | 17.78 | ||
| Maximum | 42.50 | 39.40 | 42.50 | ||
| Sex, n (%) | Male | 17 (17.71) | 3 (5.08) | 20 (12.66) | 0.023 |
| Female | 79 (82.29) | 56 (94.92) | 135 (85.44) | ||
| Affected side, n (%) | Left | 46 (47.91) | 34 (57.63) | 80 (51.61) | 0.048 |
| Right | 40 (41.67) | 25 (42.37) | 65 (41.94) | ||
| Both sides | 10 (10.42) | 0 (0.00) | 10 (6.45) | ||
| Smoker, n (%) | Yes | 13 (13.54) | 6 (10.17) | 19 (12.26) | 0.537 |
| No | 83 (86.46) | 53 (89.83) | 136 (87.74) | ||
| Preexisting conditions (multiple answers), n (%) | Metabolic-syndrome-associated | 39 (40.63) | 24 (40.68) | 63 (40.64) | 0.726 |
| Rheumatism | 6 (6.25) | 2 (3.39) | 8 (5.16) | ||
| Others | 5 (5.21) | 5 (8.47) | 10 (6.45) | ||
| None | 21 (21.88) | 11 (18.64) | 32 (20.65) | ||
| n.a. | 25 (26.04) | 17 (28.82) | 42 (27.09) |
| Measurements | With Screw (n = 96) | Without Screw (n = 59) | All (n = 155) | p | |
|---|---|---|---|---|---|
| Follow-up in months | Mean | 59.30 | 44.11 | 54.77 | <0.001 |
| Range | (10.00–81.00) | (10.00–79.00) | 10.00–81.00 | ||
| Number of affected toes (MT 2–5) | 195 | 83 | 278 | ||
| Affected side | Left | 46 (47.91) | 34 (57.63) | 80 (51.61) | 0.048 |
| Right | 40 (41.67) | 25 (42.37) | 65 (41.94) | ||
| Both sides | 10 (10.42) | 0 (0.00) | 10 (6.45) | ||
| Simultaneous hallux valgus surgery, n (%) | Yes | 64 (66.67) | 48 (81.36) | 112 (72.26) | 0.048 |
| No | 32 (33.33) | 11 (18.64) | 43 (27.74) | ||
| VAS-FA | Mean | 77.35 | 73.76 | 75.46 | 0.343 |
| SEM | 2.22 | 3.17 | 1.40 | ||
| Minimum | 12 | 19.84 | 12.85 | ||
| Maximum | 99.21 | 99.40 | 99.40 | ||
| SF-12 (physical component summary) | Mean | 41.55 | 42.80 | 42.01 | 0.527 |
| SEM | 1.21 | 1.57 | 0.96 | ||
| Minimum | 14.90 | 18.19 | 14.90 | ||
| Maximum | 60.36 | 63.53 | 63.53 | ||
| SF-12 (mental component summary) | Mean | 49.97 | 52.67 | 50.98 | 0.134 |
| SEM | 1.13 | 1.34 | 0.87 | ||
| Minimum | 26.56 | 22.98 | 22.98 | ||
| Maximum | 66.84 | 66.44 | 66.84 | ||
| Revision surgery needed, n (%) | Yes | 26 (27.10) | 5 (8.47) | 31 (20.00) | 0.005 |
| No | 70 (72.90) | 54 (91.53) | 124 (80.00) | ||
| Would you have the procedure again? | Yes | 64 (66.67) | 39 (66.10) | 103 (66.45) | 0.798 |
| No | 23 (23.95) | 16 (27.12) | 39 (25.16) | ||
| Undecided | 9 (9.34) | 4 (6.8) | 13 (8.39) | ||
| Footwear (multiple answer), n (%) | Orthotic insoles | 52 (54.17) | 31 (52.54) | 83 (53.55) | 0.705 |
| Shoe adaption | 6 (6.25) | 2 (3.39) | 8 (5.16) | ||
| Conflict with the shoe, n (%) | Yes | 27 (28.13) | 9 (15.25) | 36 (23.23) | 0.075 |
| No | 63 (65.63) | 45 (76.27) | 108 (69.68) | ||
| n.a. | 6 (6.25) | 5 (8.48) | 11 (7.10) |
| Measurements | With Screw (n = 195) | Without Screw (n = 83) | All (n = 278) | p | |
|---|---|---|---|---|---|
| Affected toes | MT 2 and 3 | 37 (38.54) | 22 (37.29) | 59 (38.06) | <0.001 */ 0.877 |
| MT 2–4 | 21 (21.88) | 1 (1.70) | 22 (14.19) | ||
| MT 2–5 | 6 (6.25) | 0 (0.00) | 6 (3.87) | ||
| MT 3 and 4 | 1 (1.04) | 0 (0.00) | 1 (0.65) | ||
| MT 4 and 5 | 1 (1.04) | 0 (0.00) | 1 (0.65) | ||
| Isolated MT 2 | 24 (25.00) | 32 (45.24) | 56 (36.13) | ||
| Isolated MT 3 | 2 (2.08) | 1 (1.70) | 3 (1.94) | ||
| Isolated MT 4 | 1 (1.04) | 3 (5.09) | 4 (2.58) | ||
| Isolated MT 5 | 3 (3.13) | 0 (0.00) | 3 (1.94) | ||
| All over MT 2 | 88 (45.13) | 54 (65.06) | 142 (51.08) | ||
| Toe mobility 1–4, n (%) ** | 1 | 148 (75.90) | 54 (65.10) | 202 (72.66) | 0.396 |
| 2 | 16 (8.21) | 17 (20.48) | 33 (11.87) | ||
| 3 | 16 (8.21) | 5 (6.02) | 21 (7.55) | ||
| 4 | 1 (0.51) | 0 (0.00) | 1 (0.36) | ||
| n.a. | 14 (7.18) | 7 (8.43) | 21 (7.55) | ||
| Minor complications (multiple answers), n (%) | |||||
| Delayed wound healing | 9 (4.62) | 4 (4.82) | 6 (2.16) | 0.320 | |
| Delayed union | 5 (2.56) | 0 (0.00) | 5 (1.80) | ||
| Persistent swelling | 3 (1.53) | 2 (2.40) | 5 (1.80) | ||
| Toe cramps | 8 (4.10) | 3 (3.61) | 11 (3.96) | ||
| Dysesthesia | 2 (1.03) | 5 (6.02) | 7 (2.52) | ||
| Recurrent metatarsalgia | 13 (6.67) | 3 (3.61) | 16 (5.76) | ||
| Revision surgery (multiple answers), n (%) | |||||
| Implant removal and arthrolysis | 53 (27.18) | - | 53 (19.06) | 0.015 | |
| Isolated MTP joint arthrolysis | 5 (2.56) | 9 (10.84) | 14 (5.04) | ||
| Revision Weil osteotomy | 11 (5.64) | 1 (1.20) | 12 (4.32) | ||
| Infection debridement | 5 (2.56) | 0 (0.00) | 5 (1.80) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boss, A.; Herrmann, E.; Gramlich, Y.; Klug, A.; Neun, O.; Manegold, S.; Hoffmann, R.; Fischer, S. The Conventional Weil Osteotomy Does Not Require Screw Fixation. J. Clin. Med. 2023, 12, 428. https://doi.org/10.3390/jcm12020428
Boss A, Herrmann E, Gramlich Y, Klug A, Neun O, Manegold S, Hoffmann R, Fischer S. The Conventional Weil Osteotomy Does Not Require Screw Fixation. Journal of Clinical Medicine. 2023; 12(2):428. https://doi.org/10.3390/jcm12020428
Chicago/Turabian StyleBoss, Anastasia, Eva Herrmann, Yves Gramlich, Alexander Klug, Oliver Neun, Sebastian Manegold, Reinhard Hoffmann, and Sebastian Fischer. 2023. "The Conventional Weil Osteotomy Does Not Require Screw Fixation" Journal of Clinical Medicine 12, no. 2: 428. https://doi.org/10.3390/jcm12020428
APA StyleBoss, A., Herrmann, E., Gramlich, Y., Klug, A., Neun, O., Manegold, S., Hoffmann, R., & Fischer, S. (2023). The Conventional Weil Osteotomy Does Not Require Screw Fixation. Journal of Clinical Medicine, 12(2), 428. https://doi.org/10.3390/jcm12020428