
Krebs von den Lungen-6 (KL-6) Levels in Post-COVID Follow-Up: Differences According to the Severity of COVID-19

 , , , , ,
, , , , ,  , ,
, ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design and Objectives
2.2. Patient Population and COVID-19 Database
- -
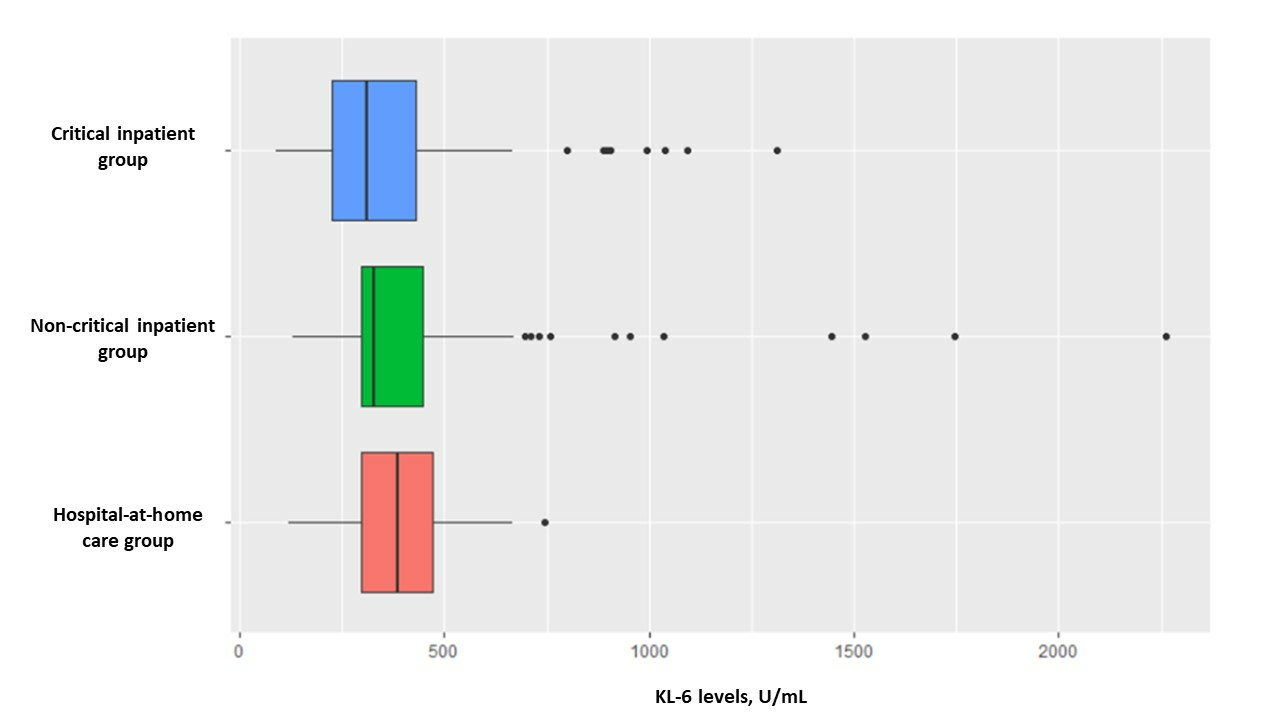
- Group 1: Severe COVID-19. Critical inpatient group. Patients requiring admission to the intensive and/or intermediate care units.
- -
- Group 2: Moderate COVID-19. Non-critical inpatient group. Patients who were hospitalised but who did not require admission to the intensive and/or intermediate care units.
- -
- Group 3: Mild COVID-19. Hospital-at-home care group. Treated at home.
2.3. Variables
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics at Admission
3.2. Baseline Characteristics Compared by Group
3.3. Characteristics of Each Group at Follow-Up
3.4. Associations with KL-6
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Attaway, A.H.; Scheraga, R.G.; Bhimraj, A.; Biehl, M.; Hatipoğlu, U. Severe COVID-19 pneumonia: Pathogenesis and clinical management. BMJ 2021, 372, n436. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Xiao, M.; Zhang, S.; Xia, P.; Cao, W.; Jiang, W.; Chen, H.; Ding, X.; Zhao, H.; Zhang, H.; et al. Coagulopathy and Antiphospholipid Antibodies in Patients with COVID-19. N. Engl. J. Med. 2020, 382, e38. [Google Scholar] [CrossRef] [PubMed]
- Ahmadian, E.; Khatibi, S.M.H.; Soofiyani, S.R.; Abediazar, S.; Shoja, M.M.; Ardalan, M.; Vahed, S.Z. COVID-19 and kidney injury: Pathophysiology and molecular mechanisms. Rev. Med. Virol. 2021, 31, e2176. [Google Scholar] [CrossRef]
- La Via, L.; Dezio, V.; Santonocito, C.; Astuto, M.; Morelli, A.; Huang, S.; Vieillard-Baron, A.; Sanfilippo, F. Full and simplified assessment of left ventricular diastolic function in COVID-19 patients admitted to ICU: Feasibility, incidence, and association with mortality. Echocardiography 2022, 39, 1391–1400. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.; Vieillard-Baron, A.; Evrard, B.; Prat, G.; Chew, M.S.; Balik, M.; Clau-Terré, F.; De Backer, D.; Dessap, A.M.; Orde, S.; et al. Echocardiography phenotypes of right ventricular involvement in COVID-19 ARDS patients and ICU mortality: Post-hoc (exploratory) analysis of repeated data from the ECHO-COVID study. Intensive Care Med. 2023, 49, 946–956. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Gutiérrez-Gutiérrez, B.; del Toro, M.D.; Borobia, A.M.; Carcas, A.; Jarrín, I.; Yllescas, M.; Ryan, P.; Pachón, J.; Carratalà, J.; Berenguer, J.; et al. Identification and validation of clinical phenotypes with prognostic implications in patients admitted to hospital with COVID-19: A multicentre cohort study. Lancet Infect. Dis. 2021, 21, 783–792. [Google Scholar] [CrossRef]
- World Health Organization. Home Care for Patients with Suspected or Confirmed COVID-19 and Management of Their Contacts: Interim Guidance, 12 August 2020. World Health Organization. Available online: https://apps.who.int/iris/handle/10665/333782 (accessed on 13 February 2022).
- Sykes, D.L.; Holdsworth, L.; Jawad, N.; Gunasekera, P.; Morice, A.H.; Crooks, M.G. Post-COVID-19 Symptom Burden: What is Long-COVID and How Should We Manage It? Lung 2021, 199, 113–119. [Google Scholar] [CrossRef]
- Montani, D.; Savale, L.; Noel, N.; Meyrignac, O.; Colle, R.; Gasnier, M.; Corruble, E.; Beurnier, A.; Jutant, W.M.; Pham, T.; et al. Post-acute COVID-19 syndrome. Eur. Respir. Rev. 2022, 31, 210185. [Google Scholar] [CrossRef]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef]
- Maamar, M.; Artime, A.; Pariente, E.; Fierro, P.; Ruiz, Y.; Gutiérrez, S.; Tobalina, M.; Díaz-Salazar, S.; Ramos, C.; Olmos, J.M.; et al. Post-COVID-19 syndrome, low-grade inflammation and inflammatory markers: A cross-sectional study. Curr. Med. Res. Opin. 2022, 38, 901–909. [Google Scholar] [CrossRef]
- Zhou, M.; Yin, Z.; Xu, J.; Wang, S.; Liao, T.; Wang, K.; Li, Y.; Yang, F.; Wang, Z.; Yang, G.; et al. Inflammatory Profiles and Clinical Features of Coronavirus 2019 Survivors 3 Months After Discharge in Wuhan, China. J. Infect. Dis. 2021, 224, 1473–1488. [Google Scholar] [CrossRef]
- Maruyama, S.; Nakamori, Y.; Nakano, H.; Tsuyumu, K.; Kanayama, S.; Iwamura, H.; Wada, D.; Yoshihara, T.; Saito, F.; Yoshiya, K.; et al. Peak value of serum KL-6 may be useful for predicting poor prognosis of severe COVID-19 patients. Eur. J. Med. Res. 2022, 27, 69. [Google Scholar] [CrossRef]
- Ware, L.B.; Matthay, M.A. Alveolar fluid clearance is impaired in the majority of patients with acute lung injury and the acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 2001, 163, 1376–1383. [Google Scholar] [CrossRef]
- Bergantini, L.; Bargagli, E.; D’Alessandro, M.; Refini, R.; Cameli, P.; Galasso, L.; Scapellato, C.; Montagnani, F.; Scolletta, S.; Franchi, F.; et al. Prognostic bioindicators in severe COVID-19 patients. Cytokine 2021, 141, 155455. [Google Scholar] [CrossRef] [PubMed]
- Naderi, N.; Rahimzadeh, M. Krebs von den Lungen-6 (KL-6) as a clinical marker for severe COVID-19: A systematic review and meta-analyses. Virology 2022, 566, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Matuszewski, M.; Szarpak, L.; Rafique, Z.; Peacock, F.W.; Pruc, M.; Szwed, P.; Chirico, F.; Navolokina, A.; Ladny, J.R.; Denegri, A. Prediction Value of KREBS Von Den Lungen-6 (KL-6) Biomarker in COVID-19 Patients: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 6600. [Google Scholar] [CrossRef] [PubMed]
- D’alessandro, M.; Bergantini, L.; Cameli, P.; Curatola, G.; Remediani, L.; Bennett, D.; Bianchi, F.; Perillo, F.; Volterrani, L.; Mazzei, M.A.; et al. Serial KL-6 measurements in COVID-19 patients. Intern. Emerg. Med. 2021, 16, 1541–1545. [Google Scholar] [CrossRef] [PubMed]
- Deng, K.; Fan, Q.; Yang, Y.; Deng, X.; He, R.; Tan, Y.; Lan, Y.; Deng, X.; Pan, Y.; Wang, Y.; et al. Prognostic roles of KL-6 in disease severity and lung injury in COVID-19 patients: A longitudinal retrospective analysis. J. Med. Virol. 2021, 93, 2505–2512. [Google Scholar] [CrossRef] [PubMed]
- Borobia, A.M.; Carcas, A.J.; Arnalich, F.; Álvarez-Sala, R.; Monserrat-Villatoro, J.; Quintana, M.; Figueira, J.C.; Santos-Olmo, R.M.T.; García-Rodríguez, J.; Martín-Vega, A.; et al. A Cohort of Patients with COVID-19 in a Major Teaching Hospital in Europe. J. Clin. Med. 2020, 9, E1733. [Google Scholar] [CrossRef]
- EuroQol Group. EuroQol—A new facility for the measurement of health-related quality of life. Health Policy Amst. Neth. 1990, 16, 199–208. [Google Scholar] [CrossRef]
- Garrod, R.; Bestall, J.C.; Paul, E.A.; Wedzicha, J.A.; Jones, P.W. Development and validation of a standardized measure of activity of daily living in patients with severe COPD: The London Chest Activity of Daily Living scale (LCADL). Respir. Med. 2000, 94, 589–596. [Google Scholar] [CrossRef] [PubMed]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Karadeniz, H.; Güler, A.A.; Özger, H.S.; Yıldız, P.A.; Erbaş, G.; Bozdayı, G.; Bulut, T.D.; Gülbahar, Ö.; Yapar, D.; Küçük, H.; et al. The Prognostic Value of Lung Injury and Fibrosis Markers, KL-6, TGF-β1, FGF-2 in COVID-19 Patients. Biomark. Insights 2022, 17, 11772719221135444. [Google Scholar] [CrossRef]
- Yamaya, T.; Hagiwara, E.; Baba, T.; Kitayama, T.; Murohashi, K.; Higa, K.; Sato, Y.; Otoshi, R.; Tabata, E.; Shintani, R.; et al. Serum Krebs von den Lungen-6 levels are associated with mortality and severity in patients with coronavirus disease 2019. Respir. Investig. 2021, 59, 596–601. [Google Scholar] [CrossRef]
- Awano, N.; Inomata, M.; Kuse, N.; Tone, M.; Takada, K.; Muto, Y.; Fujimoto, K.; Akagi, Y.; Mawatari, M.; Ueda, A.; et al. Serum KL-6 level is a useful biomarker for evaluating the severity of coronavirus disease 2019. Respir. Investig. 2020, 58, 440–447. [Google Scholar] [CrossRef] [PubMed]
- Sato, H.; Callister, M.; Mumby, S.; Quinlan, G.; Welsh, K.; Dubois, R.; Evans, T. KL-6 levels are elevated in plasma from patients with acute respiratory distress syndrome. Eur. Respir. J. 2004, 23, 142–145. [Google Scholar] [CrossRef]
- Hirasawa, Y.; Kohno, N.; Yokoyama, A.; Inoue, Y.; Abe, M.; Hiwada, K. KL-6, a human MUC1 mucin, is chemotactic for human fibroblasts. Am. J. Respir. Cell Mol. Biol. 1997, 17, 501–507. [Google Scholar] [CrossRef]
- Ishikawa, N.; Hattori, N.; Yokoyama, A.; Kohno, N. Utility of KL-6/MUC1 in the clinical management of interstitial lung diseases. Respir. Investig. 2012, 50, 3–13. [Google Scholar] [CrossRef]
- Satoh, H.; Kurishima, K.; Ishikawa, H.; Ohtsuka, M. Increased levels of KL-6 and subsequent mortality in patients with interstitial lung diseases. J. Intern. Med. 2006, 260, 429–434. [Google Scholar] [CrossRef]
- Jiang, Y.; Luo, Q.; Han, Q.; Huang, J.; Ou, Y.; Chen, M.; Wen, Y.; Mosha, S.S.; Deng, K.; Chen, R. Sequential changes of serum KL-6 predict the progression of interstitial lung disease. J. Thorac. Dis. 2018, 10, 4705–4714. [Google Scholar] [CrossRef] [PubMed]
- Xue, M.; Zheng, P.; Bian, X.; Huang, Z.; Huang, H.; Zeng, Y.; Hu, H.; Liu, X.; Zhou, L.; Sun, B.; et al. Exploration and correlation analysis of changes in Krebs von den Lungen-6 levels in COVID-19 patients with different types in China. Biosci. Trends 2020, 14, 290–296. [Google Scholar] [CrossRef]
- Fox, S.E.; Akmatbekov, A.; Harbert, J.L.; Li, G.; Quincy Brown, J.; Vander Heide, R.S. Pulmonary and cardiac pathology in African American patients with COVID-19: An autopsy series from New Orleans. Lancet Respir. Med. 2020, 8, 681–686. [Google Scholar] [CrossRef] [PubMed]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in Covid-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef]
- Frix, A.N.; Schoneveld, L.; Ladang, A.; Henket, M.; Duysinx, B.; Vaillant, F.; Misset, B.; Moutschen, M.; Louis, R.; Cavalier, E.; et al. Could KL-6 levels in COVID-19 help to predict lung disease? Respir. Res. 2020, 21, 309. [Google Scholar] [CrossRef]
- Lin, J.; Yan, H.; Chen, H.; He, C.; Lin, C.; He, H.; Zhang, S.; Shi, S.; Lin, K. COVID-19 and coagulation dysfunction in adults: A systematic review and meta-analysis. J. Med. Virol. 2021, 93, 934–944. [Google Scholar] [CrossRef] [PubMed]
- Hanif, F.M.; Majid, Z.; Ahmed, S.; Luck, N.H.; Mubarak, M. Hepatic manifestations of coronavirus disease 2019 infection: Clinical and laboratory perspective. World J. Virol. 2022, 11, 453–466. [Google Scholar] [CrossRef]
- Caballero-Alvarado, J.; Zavaleta Corvera, C.; Merino Bacilio, B.; Ruiz Caballero, C.; Lozano-Peralta, K. Post-COVID cholangiopathy: A narrative review. Gastroenterol. Hepatol. 2022. ahead of print. [Google Scholar] [CrossRef]

{kind=link}
| Total (n = 802) | Group 1 (n = 59) | Group 2 (n = 296) | Group 3 (n = 447) | p * | |
|---|---|---|---|---|---|
| Men, n (%) | 362 (45.2) | 40 (67.8) | 162 (54.9) | 160 (35.8) | <0.001 |
| Age, years | 59 (48–70) | 61 (54–68) | 68 (57–77) | 53 (42–62) | <0.001 |
| Current smoker, n (%) | 30 (7) | 7 (23.3) | 20 (6.9) | 3 (2.8) | 0.001 |
| Comorbidities | |||||
| Obesity, n (%) | 63 (14.7) | 9 (29) | 47 (16.4) | 7 (6.4) | 0.003 |
| Systemic hypertension, n (%) | 159 (36.4) | 15 (48.4) | 127 (43.2) | 17 (15.2) | <0.001 |
| Dyslipidaemia, n (%) | 133 (30.4) | 11 (35.5) | 108 (36.6) | 14 (12.5) | <0.001 |
| Diabetes mellitus, n (%) | 68 (15.6) | 7 (22.6) | 52 (17.7) | 9 (8) | 0.030 |
| COPD, n (%) | 40 (9.2) | 3 (9.7) | 26 (8.9) | 1 (0.9) | 0.015 |
| Neoplastic disease, n (%) | 37 (8.5) | 2 (6.5) | 33 (11.2) | 2 (1.8) | 0.009 |
| Kidney disease, n (%) | 17 (3.9) | 0 | 17 (5.8) | 0 | 0.014 |
| Liver disease, n (%) | 9 (2.1) | 1 (3.2) | 8 (2.7) | 0 | 0.204 |
| Oxygen therapy at admission | 291 (69.5) | 27 (96.4) | 257 (88) | 7 (7.1) | <0.001 |
| Laboratory results at admission | |||||
| White blood cell count, ×103/µL | 5.9 (4.8–7.6) | 8.4 (7.3–11.1) | 5.9 (4.7–7.4) | 5.8 (5.1–7.4) | <0.001 |
| Absolute lymphocyte count, ×103/µL | 1.5 (0.9–2) | 1.1 (0.8–1.3) | 1.3 (0.8–1.9) | 1.9 (1.5–2.3) | <0.001 |
| Platelet count, ×103/µL | 257 (200–325) | 355 (254.5–446.5) | 242.5 (188–315) | 265.5 (224.5–321.2) | <0.001 |
| C–reactive protein, mg/L | 41.4 (7.6–124.9) | 136.3 (43.4–249.1) | 78 (21.4–139.9) | 1.7 (0.5–7.8) | <0.001 |
| Fibrinogen, mg/dL | 408.5 (300–658) | 391 (240–658) | 489 (325.3–725) | 328 (260–391) | <0.001 |
| Ferritin, ng/mL | 164 (62–440) | 555 (355–1012) | 209 (84–579) | 66 (28–131) | <0.001 |
| D–dimer, ng/mL | 532 (322–1.113) | 2368 (841–6084) | 600 (368.8–1109.5) | 270 (160–402.5) | <0.001 |
| Glomerular filtration rate, mL/min/1.73 m2 | 79 (63.5–86) | 68.5 (0.5–0.9) | 79 (62.3–85.8) | 84 (77–89) | <0.001 |
| Gamma–glutamyl transferase, UI/L | 32 (19–69.8) | 123 (43.5–303.5) | 38 (21–76) | 20 (15–26.3) | <0.001 |
| Alanine aminotransferase, UI/L | 27 (19–49) | 64 (39–102.5) | 28 (19.5–50.5) | 21 (18–33) | <0.001 |
| Aspartate aminotransferase, UI/L | 26.5 (18–41) | 52 (25.5–81.5) | 28 (20–43) | 18 (15–27) | <0.001 |
| Total (n = 802) | Group 1 (n = 59) | Group 2 (n = 296) | Group 3 (n = 447) | p * | |
|---|---|---|---|---|---|
| Symptomatology | |||||
| Dyspnoea, n (%) | 351 (66.6) | 34 (66.7) | 117 (59.1) | 200 (71.9) | 0.014 |
| Fatigue, n (%) | 233 (44.5) | 22 (43.1) | 69 (35.4) | 142 (51.1) | 0.003 |
| Myalgia, n (%) | 223 (42.4) | 26 (51) | 67 (34) | 130 (46.8) | 0.009 |
| Cough, n (%) | 106 (20.1) | 14 (27.5) | 33 (16.7) | 59 (21.2) | 0.184 |
| Thoracic pain, n (%) | 79 (14.8) | 7 (13.7) | 26 (13.1) | 46 (16.3) | 0.598 |
| Fever, n (%) | 23 (4.4) | 0 | 6 (3) | 17 (6.1) | 0.073 |
| Vital signs and anthropometry | |||||
| Heart rate, beats per minute | 83 (74–91) | 80 (73.5–83.5) | 81 (72–90) | 84 (75–93) | 0.470 |
| SpO2, % | 97 (96–98) | 97 (96–98) | 96 (95–97) | 97 (96–98) | <0.001 |
| Body mass index, kg/m2 | 25 (23–29) | 27 (25–31) | 25 (24–29) | 25 (23–29) | 0.038 |
| HADS | 12 (7–18) | 11 (6.5–17) | 11 (6–17.3) | 12 (7–19) | 0.298 |
| EuroQoL | |||||
| Time trade-off value | 0.8 (0.7–0.9) | 0.7 (0.3–0.9) | 0.8 (0.7–0.9) | 0.8 (0.6–0.9) | 0.041 |
| Visual analogue scale value | 0.7 (0.6– 0.8) | 0.6 (0.4–0.8) | 0.7 (0.6–0.8) | 0.7 (0.6–0.8) | 0.038 |
| EuroQoL-visual analogue scale | 70 (55–80) | 70 (55–82.5) | 70 (60–80) | 60 (50–73.8) | 0.010 |
| LCADL scale | 20 (16–28) | 19 (15–30.5) | 20 (16–27) | 20 (16–28.5) | 0.541 |
| LCADL self-care domain | 4 (4–6) | 5 (4–7) | 4 (4–6) | 4 (4–6) | 0.345 |
| LCADL domestic activities domain | 6 (6–11) | 6 (4–12) | 6 (6–10) | 6 (6–12) | 0.322 |
| LCADL physical activities domain | 4 (3–6) | 4 (3–6) | 4 (3–6) | 4 (3–6) | 0.542 |
| LCADL leisure activities domain | 4 (3–6) | 4 (3–6.5) | 4 (3–5) | 4 (3–6) | 0.485 |
| Laboratory results at 6 months | |||||
| White blood cell count, ×103/µL | 6.5 (5.4–7.6) | 6.5 (5.4–7.9) | 6.5 (5.4–7.6) | 6.4 (5.4–7.6) | 0.908 |
| Absolute lymphocyte count, ×103/µL | 1.9 (1.6–2.4) | 2.2 (1.6–2.7) | 1.9 (1.5–2.7) | 1.9 (1.6–2.4) | 0.082 |
| Platelet count, ×103/µL | 244 (207–291) | 258.5 (209.5–313.5) | 226 (191–283.5) | 251 (215–293) | <0.001 |
| C-reactive protein, mg/L | 2.7 (0.6–14.4) | 4.9 (1.2–17.6) | 2.5 (0.7–10.5) | 2.6 (0.5–15.7) | 0.003 |
| Fibrinogen, mg/dL | 336 (276–413) | 343 (302.3–462) | 336.5 (282–409) | 336 (271–412) | 0.320 |
| Ferritin, ng/mL | 80.5 (36–174.3) | 107 (64–166) | 89.5 (42–164.5) | 75 (31–183) | 0.340 |
| D-dimer, ng/mL | 330 (210–565) | 450 (230–965) | 370 (250–610) | 290 (190–485) | <0.001 |
| Glomerular filtration rate, mL/min/1.73 m2 | 78 (67–84) | 81 (72–82) | 77 (64.8–84) | 78 (69–86) | 0.491 |
| Gamma-glutamyl transferase, UI/L | 23 (16–35) | 33.5 (17–43.5) | 24 (18–34) | 21 (15–33) | 0.003 |
| Alanine aminotransferase, UI/L | 23 (17–34) | 24 (17–40) | 23 (18–33) | 24 (17–35) | 0.929 |
| Aspartate aminotransferase, UI/L | 19 (15–26) | 19 (14.5–26) | 20 (16–27) | 19 (15–25) | 0.394 |
| KL-6, U/mL | 326 (240.3–440.3) | 381.5 (304–511.8) | 372 (249–483) | 298 (231.5–398) | <0.001 |
| KL-6 Levels | ||
|---|---|---|
| rho | p | |
| SpO2, % | −0.006 | 0.986 |
| EuroQoL | ||
| Time trade-off value | 0.028 | 0.565 |
| Visual analogue scale value | 0.029 | 0.547 |
| EuroQoL-VAS | 0.107 | 0.152 |
| LCADL scale | 0.016 | 0.737 |
| LCADL self-care domain | 0.073 | 0.139 |
| LCADL domestic activities domain | −0.032 | 0.524 |
| LCADL physical activities domain | 0.049 | 0.322 |
| LCADL leisure activities domain | 0.037 | 0.454 |
| Laboratory results at follow-up | ||
| White blood cell count, ×103/uL | 0.099 | 0.004 |
| Absolute lymphocyte count, ×103/µL | 0.099 | 0.044 |
| Platelet count, ×103/µL | −0.41 | 0.407 |
| Fibrinogen, mg/dL | 0.197 | <0.001 |
| Ferritin, ng/mL | 0.204 | <0.001 |
| D-dimer, ng/mL | 0.199 | <0.001 |
| Glomerular filtration rate, mL/min/1.73 m2 | −0.038 | 0.622 |
| Gamma-glutamyl transferase, UI/L | 0.176 | <0.001 |
| Alanine aminotransferase, UI/L | 0.120 | 0.016 |
| Aspartate aminotransferase, UI/L | 0.124 | 0.014 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carpio, C.; Qasem, A.; Buño, A.; Borobia, A.M.; Arnalich, F.; Rey, V.; Lázaro, T.; Mariscal, P.; Laorden, D.; Salgueiro, G.; et al. Krebs von den Lungen-6 (KL-6) Levels in Post-COVID Follow-Up: Differences According to the Severity of COVID-19. J. Clin. Med. 2023, 12, 6299. https://doi.org/10.3390/jcm12196299
Carpio C, Qasem A, Buño A, Borobia AM, Arnalich F, Rey V, Lázaro T, Mariscal P, Laorden D, Salgueiro G, et al. Krebs von den Lungen-6 (KL-6) Levels in Post-COVID Follow-Up: Differences According to the Severity of COVID-19. Journal of Clinical Medicine. 2023; 12(19):6299. https://doi.org/10.3390/jcm12196299
Chicago/Turabian StyleCarpio, Carlos, Ana Qasem, Antonio Buño, Alberto M. Borobia, Francisco Arnalich, Vega Rey, Teresa Lázaro, Pablo Mariscal, Daniel Laorden, Giorgina Salgueiro, and et al. 2023. "Krebs von den Lungen-6 (KL-6) Levels in Post-COVID Follow-Up: Differences According to the Severity of COVID-19" Journal of Clinical Medicine 12, no. 19: 6299. https://doi.org/10.3390/jcm12196299
APA StyleCarpio, C., Qasem, A., Buño, A., Borobia, A. M., Arnalich, F., Rey, V., Lázaro, T., Mariscal, P., Laorden, D., Salgueiro, G., Moreno, A., Peiró, C., Lorenzo, Ó., Álvarez-Sala, R., on behalf of COVID@HULP Working Group, & on behalf of POSTCOVID@HULP Working Group. (2023). Krebs von den Lungen-6 (KL-6) Levels in Post-COVID Follow-Up: Differences According to the Severity of COVID-19. Journal of Clinical Medicine, 12(19), 6299. https://doi.org/10.3390/jcm12196299