
Clinical Reproducibility of the Stone Volume Measurement: A “Kidney Stone Calculator” Study

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Kidney Stone Calculator Software
2.2. Experimental Setup
2.3. Statistical Analysis
3. Results
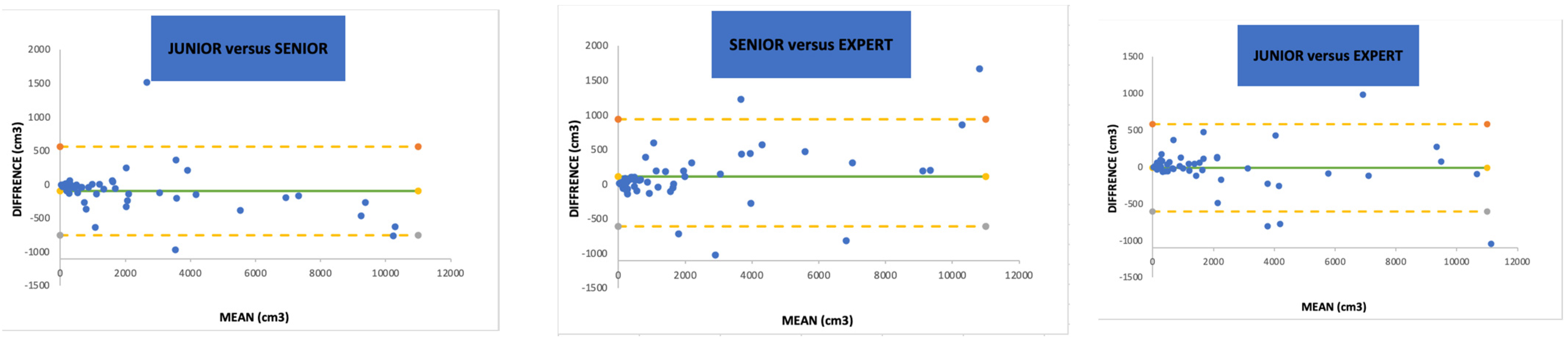
3.1. Inter-Observer Analysis
3.2. Intra-Observer and Subgroup Analyses
4. Discussion
4.1. Reproducibility and Agreement
4.2. Stone Burden Evaluation
4.3. Clinical Implications
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stamatelou, K.; Goldfarb, D.S. Epidemiology of Kidney Stones. Healthcare 2023, 11, 424. [Google Scholar] [CrossRef] [PubMed]
- Türk, C.; Petřík, A.; Sarica, K.; Seitz, C.; Skolarikos, A.; Straub, M.; Knoll, T. EAU Guidelines on diagnosis and conservative management of urolithiasis. Eur. Urol. 2016, 69, 468–474. [Google Scholar] [CrossRef] [PubMed]
- Türk, C.; Petřík, A.; Sarica, K.; Seitz, C.; Skolarikos, A.; Straub, M.; Knoll, T. EAU Guidelines on interventional treatment for urolithiasis. Eur. Urol. 2016, 69, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Assimos, D.; Krambeck, A.; Miller, N.L.; Monga, M.; Murad, M.H.; Nelson, C.P.; Pace, K.T.; Pais, V.M.; Pearle, M.S.; Preminger, G.M.; et al. Surgical management of stones: American urological association/endourological society guideline, Part I. J. Urol. 2016, 196, 1153–1160. [Google Scholar] [CrossRef]
- Ventimiglia, E.; Traxer, O. What is moses effect: A historical perspective. J. Endourol. 2019, 33, 353–357. [Google Scholar] [CrossRef]
- Traxer, O.; Sierra, A.; Corrales, M. Which is the best laser for lithotripsy? Thulium fiber laser. Eur. Urol. Open Sci. 2022, 44, 15–17. [Google Scholar] [CrossRef]
- Chugh, S.; Pietropaolo, A.; Montanari, E.; Sarica, K.; Somani, B.K. Predictors of urinary infections and urosepsis after ureteroscopy for stone disease: A systematic review from EAU section of urolithiasis (EULIS). Curr. Urol. Rep. 2020, 21, 16. [Google Scholar] [CrossRef]
- Panthier, F.; Doizi, S.; Illoul, L.; Berthe, L.; Traxer, O. Developing free three-dimensional software for surgical planning for kidney stones: Volume is better than diameter. Eur. Urol. Focus 2021, 7, 589–590. [Google Scholar] [CrossRef] [PubMed]
- Ackermann, D.; Griffith, D.P.; Dunthorn, M.; Newman, R.C.; Finlayson, B. Calculation of stone volume and urinary stone staging with computer assistance. J. Endourol. 1989, 3, 355–360. [Google Scholar] [CrossRef]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.-C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef]
- Panthier, F.; Traxer, O.; Yonneau, L.; Lebret, T.; Berthe, L.; Illoul, L.; Timsit, M.-O.; Mejean, A.; Doizi, S.; Audenet, F. Evaluation of a free 3D software for kidney stones’ surgical planning: “Kidney stone calculator” a pilot study. World J. Urol. 2021, 39, 3607–3614. [Google Scholar] [CrossRef] [PubMed]
- Danilovic, A.; Rocha, B.A.; Marchini, G.S.; Traxer, O.; Batagello, C.; Vicentini, F.C.; Torricelli, F.C.M.; Srougi, M.; Nahas, W.C.; Mazzucchi, E. Computed tomography window affects kidney stones measurements. Int. Braz. J. Urol. 2019, 45, 948–955. [Google Scholar] [CrossRef] [PubMed]
- Partik, B.L.; Stadler, A.; Schamp, S.; Koller, A.; Voracek, M.; Heinz, G.; Helbich, T.H. 3D Versus 2D Ultrasound: Accuracy of volume measurement in human cadaver kidneys. Investig. Radiol. 2002, 37, 489–495. [Google Scholar] [CrossRef]
- Recommandations de Bonne Pratique—Prise en Charge des Calculs et de la Lithiase Urinaires: Diagnostic, Traitement, Suivi et Prévention Secondaire. 2022. Available online: https://www.urofrance.org/recommandation/recommandations-de-bonne-pratique-pour-la-prise-en-charge-des-calculs-et-de-la-lithiase-urinaires-diagnostic-traitement-suivi-et-prevention-secondaire-argumentaire/ (accessed on 1 June 2023).
- Jendeberg, J.; Geijer, H.; Alshamari, M.; Lidén, M. Prediction of spontaneous ureteral stone passage: Automated 3D-measurements perform equal to radiologists, and linear measurements equal to volumetric. Eur. Radiol. 2018, 28, 2474–2483. [Google Scholar] [CrossRef]
- Selby, M.G.; Vrtiska, T.J.; Krambeck, A.E.; McCollough, C.H.; Elsherbiny, H.E.; Bergstralh, E.J.; Lieske, J.C.; Rule, A.D. Quantification of Asymptomatic Kidney Stone Burden by Computed Tomography for Predicting Future Symptomatic Stone Events. Urology 2015, 85, 45–50. [Google Scholar] [CrossRef]
- Ito, H.; Kawahara, T.; Terao, H.; Ogawa, T.; Yao, M.; Kubota, Y.; Matsuzaki, J. The most reliable preoperative assessment of renal stone burden as a predictor of stone-free status after flexible ureteroscopy with holmium laser lithotripsy: A single-center experience. Urology 2012, 80, 524–528. [Google Scholar] [CrossRef]
- Ito, H.; Kawahara, T.; Terao, H.; Ogawa, T.; Yao, M.; Kubota, Y.; Matsuzaki, J. Evaluation of preoperative measurement of stone surface area as a predictor of stone-free status after combined ureteroscopy with holmium laser lithotripsy: A single-center experience. J. Endourol. 2013, 27, 715–721. [Google Scholar] [CrossRef]
- Ito, H.; Kawahara, T.; Terao, H.; Ogawa, T.; Yao, M.; Kubota, Y.; Matsuzaki, J. Utility and limitation of cumulative stone diameter in predicting urinary stone burden at flexible ureteroscopy with holmium laser lithotripsy: A single-center experience. PLoS ONE 2013, 8, e65060. [Google Scholar] [CrossRef]
- Ko, J.P.; Rusinek, H.; Jacobs, E.L.; Babb, J.S.; Betke, M.; McGuinness, G.; Naidich, D.P. Small Pulmonary Nodules: Volume Measurement at Chest CT—Phantom Study. Radiology 2003, 228, 864–870. [Google Scholar] [CrossRef]
- Goo, J.M.; Tongdee, T.; Tongdee, R.; Yeo, K.; Hildebolt, C.F.; Bae, K.T. Volumetric Measurement of Synthetic Lung Nodules with Multi–Detector Row CT: Effect of Various Image Reconstruction Parameters and Segmentation Thresholds on Measurement Accuracy. Radiology 2005, 235, 850–856. [Google Scholar] [CrossRef]
- Elton, D.C.; Turkbey, E.B.; Pickhardt, P.J.; Summers, R.M. A deep learning system for automated kidney stone detection and volumetric segmentation on noncontrast CT scans. Med. Phys. 2022, 49, 2545–2554. [Google Scholar] [CrossRef] [PubMed]
- Durutović, O.; Filipović, A.; Milićević, K.; Somani, B.; Emiliani, E.; Skolarikos, A.; Janković, M.M. 3D Imaging Segmentation and 3D Rendering Process for a Precise Puncture Strategy During PCNL—A Pilot Study. Front. Surg. 2022, 9, 891596. [Google Scholar] [CrossRef] [PubMed]
- Ziemba, J.B.; Li, P.; Gurnani, R.; Kawamoto, S.; Fishman, E.K.; Fung, G.; Ludwig, W.W.; Stoianovici, D.; Matlaga, B.R. A User-Friendly Application to Automate CT Renal Stone Measurement. J. Endourol. 2018, 32, 685–691. [Google Scholar] [CrossRef]
- Patel, S.R.; Stanton, P.; Zelinski, N.; Borman, E.J.; Pozniak, M.A.; Nakada, S.Y.; Pickhardt, P.J. Automated renal stone volume measurement by noncontrast computerized tomography is more reproducible than manual linear size measurement. J. Urol. 2011, 186, 2275–2279. [Google Scholar] [CrossRef]
- Corrales, M.; Sierra, A.; Doizi, S.; Traxer, O. Risk of Sepsis in Retrograde Intrarenal Surgery: A Systematic Review of the Literature. Eur. Urol. Open Sci. 2022, 44, 84–91. [Google Scholar] [CrossRef]
- Kuroda, S.; Ito, H.; Sakamaki, K.; Tabei, T.; Kawahara, T.; Fujikawa, A.; Makiyama, K.; Yao, M.; Uemura, H.; Matsuzaki, J. A new prediction model for operative time of flexible ureteroscopy with lithotripsy for the treatment of renal stones. PLoS ONE 2018, 13, e0192597. [Google Scholar] [CrossRef] [PubMed]
- Tufano, A.; Frisenda, M.; Rossi, A.; Viscuso, P.; Mantica, G.; Bove, P.; Leonardi, R.; Calarco, A. External validation of Resorlu-Unsal stone score in predicting outcomes after retrograde intrarenal surgery. Experience from a single institution. Arch. Ital. Urol. Androl. 2022, 94, 311–314. [Google Scholar] [CrossRef]
- Reimer, R.P.; Klein, K.; Rinneburger, M.; Zopfs, D.; Lennartz, S.; Salem, J.; Heidenreich, A.; Maintz, D.; Haneder, S.; Große Hokamp, N. Manual kidney stone size measurements in computed tomography are most accurate using multiplanar image reformatations and bone window settings. Sci. Rep. 2021, 11, 16437. [Google Scholar] [CrossRef]
- Rassweiler-Seyfried, M.-C.; Otto, C.; Haneder, S.; Riffel, P.; Stein, J.; Ritter, M. Impact of Multiparametric Stone Measurement in Noncontrast Computer Tomography on Ureterorenoscopic Stone Removal. Urol. Int. 2021, 105, 600–604. [Google Scholar] [CrossRef]
- Umbach, R.; Müller, J.-K.; Wendt-Nordahl, G.; Knoll, T.; Jessen, J.P. In-vitro comparison of different slice thicknesses and kernel settings for measurement of urinary stone size by computed tomography. Urolithiasis 2019, 47, 583–586. [Google Scholar] [CrossRef]
- Doyle, P.W.; Kavoussi, N.L. Machine learning applications to enhance patient specific care for urologic surgery. World J. Urol. 2022, 40, 679–686. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Xiao, C.; Liu, Y.; Chen, Z.; Hassan, H.; Su, L.; Liu, J.; Li, H.; Xie, W.; Zhong, W.; et al. Deep Segmentation Networks for Segmenting Kidneys and Detecting Kidney Stones in Unenhanced Abdominal CT Images. Diagnostics 2022, 12, 1788. [Google Scholar] [CrossRef] [PubMed]
- Babajide, R.; Lembrikova, K.; Ziemba, J.; Ding, J.; Li, Y.; Fermin, A.S.; Fan, Y.; Tasian, G.E. Automated Machine Learning Segmentation and Measurement of Urinary Stones on CT Scan. Urology 2022, 169, 41–46. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variables | Value | ||
|---|---|---|---|
| Patients | 50 | ||
| Age | 48 (38–61) | ||
| Gender | Female | 26 (52%) | |
| Male | 24 (48%) | ||
| Stone history | Renal colic | 40 (80%) | |
| Previous surgical procedure | 43 (86%) | ||
| Anatomical urinary tract abnormality | 14 (28%) | ||
| Stone characteristics | Side | Left | 27 (54%) |
| Right | 23 (46%) | ||
| Number of calculi | 1 | 24 (48%) | |
| 2 or 3 | 18 (36%) | ||
| >3 | 8 (16%) | ||
| Complex | 15 (30%) | ||
| Localization | Lower pole | 19 (38%) | |
| Renal pelvic | 15 (30%) | ||
| Other | 16 (32%) | ||
| Density, median (UH) | 1100 (716–1546) | ||
| Density (UH) | >1000 UH | 31 (62%) | |
| Maximum diameter, median (mm) | 15 (10–23) | ||
| Segmented stone burden, median (mm3) | 923 (314–3032) | ||
| Homogeneous calculi | 27 (54%) | ||
| (a) | |||
|---|---|---|---|
| Paired concordance | Junior versus senior urologist | ||
| Lin CCC (CI) | 0.99 (0.98–1) | ||
| Student’s t-test (p) | 0.87 | ||
| Paired concordance | Senior urologist versus expert endourologist | ||
| Lin CCC (CI) | 0.99 (0.98–0.99) | ||
| Student’s t-test (p) | 0.85 | ||
| Paired concordance | Junior versus expert endourologist | ||
| Lin CCC (CI) | 0.99 (0.99–1) | ||
| Student’s t-test (p) | 0.98 | ||
| Overall concordance (Kendall CCC) | 0.99 (p < 0.0001) | ||
| (b) | |||
| Case number | Median volume (mm3) and Q1–Q3 | ||
| Junior urologist | Senior urologist | Expert endourologist | |
| 1 | 1720 (1675–1787) | 1664 (1645–1691) | 1609 (1598–1680) |
| 2 | 1210 (1177–1216) | 1209 (1196–1239) | 1165 (1155–1191) |
| 3 | 92 (92–96) | 63.16 (59.31–63.63) | 83 (82–90) |
| 4 | 681 (672–684) | 636.5 (632.8–642) | 706 (630–710) |
| 5 | 255 (249–265) | 314.4 (312.1–320,5) | 244 (225–248) |
| 6 | 154 (141–159) | 169.9 (161–170.8) | 121 (119–178) |
| 7 | 2184 (2154–2198) | 1857 (1817–1970) | 2049 (2023–2049) |
| 8 | 190 (190–196) | 204 (201–211) | 178 (165–181) |
| 9 | 648 (640–654) | 604 (571.7–617.8) | 664 (640–680) |
| 10 | 472 (468–493) | 424.1 (422.6–468) | 530 (528–547) |
| 11 | 1605 (1557–1610) | 1643 (1600–1660) | 1649 (1616–1706) |
| 12 | 7404 (7311–7567) | 7238 (7100–7360) | 6423 (6423–6679) |
| 13 | 7040 (6582–7047) | 6844 (6815–6896) | 7156 (7003–7178) |
| 14 | 1903 (1900–1926) | 3414 (3345–3518) | 2391 (2377–2408) |
| 15 | 987 (984–1034) | 988 (921–994) | 856 (824–856) |
| 16 | 3114 (3059–3132) | 2988 (2921–2994) | 3132 (3132–3154) |
| 17 | 177 (168–183) | 176 (175–178) | 120 (112–120) |
| 18 | 312 (308–339) | 315 (314–319) | 215 (213–242) |
| 19 | 1913 (1905–1980) | 2161 (2129–2203) | 1440 (1440–1440) |
| 20 | 92 (83–96) | 82 (81–82) | 80 (77–84) |
| 21 | 2180 (2173–2218) | 1942 (1887–1983) | 2057 (2048–2059) |
| 22 | 983 (932–1009) | 613 (565–624) | 1006 (2048–2059) |
| 23 | 3371 (3313–3469) | 3731 (3731–3811) | 4178 (4178–4178) |
| 24 | 31 (30–33) | 26 (25–27) | 34 (25–34) |
| 25 | 4016 (3990–4017) | 3047 (3024–3052) | 4276 (4276–4276) |
| 26 | 9518 (9449–9521) | 9247 (9167–9263) | 9446 (9430–9459) |
| 27 | 901 (897–948) | 858 (828–864) | 886 (886–886) |
| 28 | 375 (399–399) | 343 (339–351) | 442 (395–444) |
| 29 | 385 (384–399) | 356 (340–357) | 211 (211–211) |
| 30 | 499 (485–503) | 495 (482–498) | 463 (463–497) |
| 31 | 4257 (4239–4265) | 4105 (4028–4106) | 3830 (3581–4063) |
| 32 | 128 (126–134) | 123 (121–125) | 162 (161–162) |
| 33 | 5733 (5681–5740) | 5352 (5305–5366) | 5823 (5822–5826) |
| 34 | 1378 (1354–1399) | 1312 (1312–1332) | 1497 (1497–1504) |
| 35 | 346 (313–355) | 216 (216–224) | 261 (261–261) |
| 36 | 1393 (1235–1696) | 756 (755–758) | 1352 (1346–1372) |
| 37 | 873 (808–880) | 604 (599–627) | 510 (489–550) |
| 38 | 252 (241–254) | 226 (224–228) | 254 (250–260) |
| 39 | 297 (288–301) | 294 (277–323) | 361 (361–362) |
| 40 | 9485 (9473–9499) | 9021 (8707–9069) | 9212 (9212–9212) |
| 41 | 10,606 (10,337–10,624) | 9982 (9924–10,011) | 11,652 (11,652–11,652) |
| 42 | 3805 (3723–3892) | 4015 (4007–4136) | 4581 (4581–4756) |
| 43 | 249 (230–276) | 152 (145–159) | 234 (231–240) |
| 44 | 266 (263–271) | 240 (234–241) | 273 (269–284) |
| 45 | 1567 (1460–1786) | 1621 (1494–1660) | 1512 (1470–1514) |
| 46 | 1187 (1037–1233) | 1042 (1019–1076) | 1234 (1208–1234) |
| 47 | 2172 (2169–2200) | 2033 (1019–1076) | 2343 (2300–2412) |
| 48 | 3671 (3660–3690) | 3464 (3448–3493) | 3897 (3578–4001) |
| 49 | 10,621 (10,599–10,647) | 9858 (9849–9916) | 10,717 (10,717–10,717) |
| 50 | 593 (559–598) | 470 (461–485) | 530 (524–532) |
| Coefficient of variation (%) | 6.3% | 4.2% | 4.6% |
| Intra-operator concordance (Kendall CCC) | 0.98 (p < 0.0001) | 1 (p < 0.0001) | 0.99 (p < 0.0001) |
| (c) | |||
| Homogenous | Heterogenous | p-value (Mann–Whitney test) | |
| Median coefficient of variation (%) | 11.8% | 11% | 0.51 |
| Complex | Non-complex | p-value (Mann–Whitney test) | |
| Median coefficient of variation (%) | 13% | 8.1% | 0.02 |
| Unique | Multiple | p-value (Mann–Whitney test) | |
| Median coefficient of variation (%) | 12.1% | 11% | 0.78 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peyrottes, A.; Chicaud, M.; Fourniol, C.; Doizi, S.; Timsit, M.-O.; Méjean, A.; Yonneau, L.; Lebret, T.; Audenet, F.; Traxer, O.; et al. Clinical Reproducibility of the Stone Volume Measurement: A “Kidney Stone Calculator” Study. J. Clin. Med. 2023, 12, 6274. https://doi.org/10.3390/jcm12196274
Peyrottes A, Chicaud M, Fourniol C, Doizi S, Timsit M-O, Méjean A, Yonneau L, Lebret T, Audenet F, Traxer O, et al. Clinical Reproducibility of the Stone Volume Measurement: A “Kidney Stone Calculator” Study. Journal of Clinical Medicine. 2023; 12(19):6274. https://doi.org/10.3390/jcm12196274
Chicago/Turabian StylePeyrottes, Arthur, Marie Chicaud, Cyril Fourniol, Steeve Doizi, Marc-Olivier Timsit, Arnaud Méjean, Laurent Yonneau, Thierry Lebret, François Audenet, Olivier Traxer, and et al. 2023. "Clinical Reproducibility of the Stone Volume Measurement: A “Kidney Stone Calculator” Study" Journal of Clinical Medicine 12, no. 19: 6274. https://doi.org/10.3390/jcm12196274
APA StylePeyrottes, A., Chicaud, M., Fourniol, C., Doizi, S., Timsit, M.-O., Méjean, A., Yonneau, L., Lebret, T., Audenet, F., Traxer, O., & Panthier, F. (2023). Clinical Reproducibility of the Stone Volume Measurement: A “Kidney Stone Calculator” Study. Journal of Clinical Medicine, 12(19), 6274. https://doi.org/10.3390/jcm12196274