
Outcome Analysis of Speed Gate Cannulation during Standard Infrarenal Endovascular Aneurysm Repair

 ,
,  , and
, and
Abstract
:1. Introduction
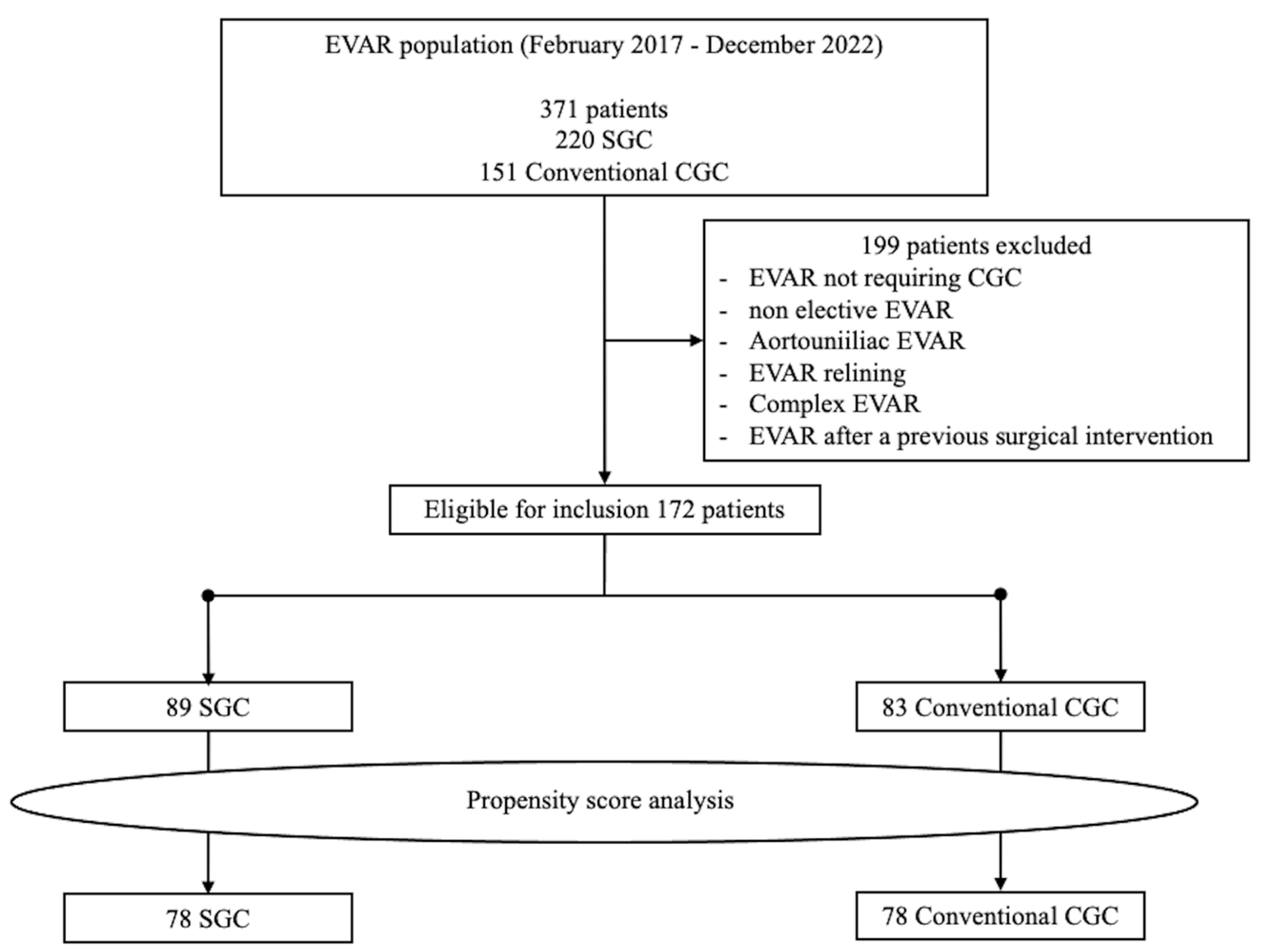
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Steuer, J.; Lachat, M.; Veith, F.J.; Wanhainen, A. Endovascular grafts for abdominal aortic aneurysm. Eur. Heart J. 2016, 37, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Pakeliani, D.; Lachat, M.; Blohmé, L.; Kobayashi, M.; Chaykovska, L.; Pfammatter, T.; Puippe, G.; Veith, F.J.; Pecoraro, F. Improved technique for sheath supported contralateral limb gate cannulation in endovascular abdominal aortic aneurysm repair. Vasa 2020, 49, 39–42, Erratum in Vasa 2021, 50, 158. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Epidemiology 2007, 18, 800–804. [Google Scholar] [CrossRef] [PubMed]
- Titus, J.M.; Cragg, A.; Alden, P.; Alexander, J.; Manunga, J.; Stephenson, E.; Skeik, N.; Sullivan, T. A prospective randomized comparison of contralateral snare versus retrograde gate cannulation in endovascular aneurysm repair. J. Vasc. Surg. 2017, 66, 387–391. [Google Scholar] [CrossRef]
- Wolf, Y.G.; Tillich, M.; Lee, W.; Rubin, G.D.; Fogarty, T.J.; Zarins, C.K. Impact of aortoiliac tortuosity on endovascular repair of abdominal aortic aneurysms: Evaluation of 3D computer-based assessment. J. Vasc. Surg. 2001, 34, 594–599. [Google Scholar] [CrossRef] [PubMed]
- Turchino, D.; Peluso, A.; Accarino, G.; Accarino, G.; De Rosa, C.; D’Angelo, A.; Machi, P.; Mirabella, D.; Pecoraro, F.; del Guercio, L.; et al. A Multicenter Experience of Three Different “Iliac Branched” Stent Grafts for the Treatment of Aorto-Iliac and/or Iliac Aneurysms. Ann. Vasc. Surg. 2023, 94, 331–340. [Google Scholar] [CrossRef] [PubMed]
- Elahwal, M.; Nash, T.; Yusuf, S.W. Through and Through Wire Technique for Stabilization of EVAR Main Body during Contralateral Limb Deployment. Ann. Vasc. Surg. 2021, 74, 515–517. [Google Scholar] [CrossRef] [PubMed]
- Dinoto, E.; Ferlito, F.; Mirabella, D.; Tortomasi, G.; Bajardi, G.; Pecoraro, F. Type 1A endoleak detachable coil embolization after endovascular aneurysm sealing: Case report. Int. J. Surg. Case Rep. 2021, 83, 106024. [Google Scholar] [CrossRef] [PubMed]
- Pecoraro, F.; Dinoto, E.; Mirabella, D.; Ferlito, F.; Farina, A.; Pakeliani, D.; Lachat, M.; Urso, F.; Bajardi, G. Endovascular Treatment of Spontaneous and Isolated Infrarenal Acute Aortic Syndrome with Unibody Aortic Stent-Grafts. World J. Surg. 2020, 44, 4267–4274. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Q.; Huang, L.; Huang, X.; Peng, M. Endovascular repair of abdominal aortic aneurysm with severely angulated neck and tortuous artery access: Case report and literature review. BMC Surg. 2015, 15, 20. [Google Scholar] [CrossRef] [PubMed]
- Dang, W.; Kilian, M.; Peterson, M.D.; Cinà, C. Relationship between access side used to deliver the main body of bifurcated prostheses for endovascular aneurysm repair and speed of cannulation of the contralateral limb. J. Vasc. Surg. 2010, 51, 33–37.e1. [Google Scholar] [CrossRef]
- Yagihashi, K.; Nishimaki, H.; Ogawa, Y.; Chiba, K.; Murakami, K.; Ro, D.; Ono, H.; Sakurai, Y.; Miyairi, T.; Nakajima, Y. Early and Mid-Term Results of Endovascular Aortic Repair Using a Crossed-Limb Technique for Patients with Severely Splayed Iliac Angulation. Ann. Vasc. Dis. 2018, 11, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Murphy, E.H.; Arko, F.R. Technical Tips for Abdominal Aortic Endografting. Semin. Vasc. Surg. 2008, 21, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Pecoraro, F.; Bracale, U.M.; Farina, A.; Badalamenti, G.; Ferlito, F.; Lachat, M.; Dinoto, E.; Asti, V.; Bajardi, G. Single-Center Experience and Preliminary Results of Intravascular Ultrasound in Endovascular Aneurysm Repair. Ann. Vasc. Surg. 2019, 56, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Mazzaccaro, D.; Sciarrini, M.; Nano, G. The challenge of gate cannulation during endovascular aortic repair: A hypothesis of simplification. Med. Hypotheses 2016, 94, 43–46. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Unmatched Cohort | Matched Cohort | ||||||
|---|---|---|---|---|---|---|---|
| Variables | SGC (89) | STD (83) | p | SGC (78) | STD (78) | SE Diff | p |
| Age, y, (SD) | 78 [±8] | 81 [±9] | 0.16 | 78 [±8] | 81 [±9] | −6.4 | 0.21 |
| Male gender, n (%) | 63 (70.8) | 67 (80.7) | 0.94 | 62 (79.5) | 63 (80.8) | 0.12 | 1 |
| Associated comorbidities | |||||||
| Hypertension, n (%) | 81 (91) | 67 (80.7) | <0.001 | 65 (83.3) | 59 (75.6) | 0.07 | 0.66 |
| Ever smoker, n (%) | 48 (53.9) | 49 (59) | 0.9 | 47 (60.2) | 46 (59) | 0.11 | 0.9 |
| COPD, n (%) | 11 (12.3) | 15 (18.1) | 0.6 | 10 (12.8) | 10 (12.8) | 0.12 | 0.77 |
| CVD, n (%) | 8 (9) | 7 (8.4) | 0.4 | 6 (7.7) | 6 (7.7) | 0.14 | 0.75 |
| PAD, n (%) | 11 (12.3) | 17 (20.5) | <0.001 | 10 (12.8) | 11 (14.1) | 0.12 | 0.74 |
| Diabetes, n (%) | 41 (46.1) | 48 (57.8) | 0.2 | 35 (44.9) | 27 (34.6) | 0.13 | 0.55 |
| Lipid Disorder, n (%) | 63 (70.8) | 55 (66.3) | <0.001 | 57 (73.1) | 54 (69.2) | 0.15 | 0.42 |
| CAD, n (%) | 44 (49.4) | 42 (50.6) | 0.3 | 35 (44.9) | 41 (52.6) | 0.11 | 0.58 |
| Previous CI, n (%) | 21 (23.6) | 27 (32.5) | 0.5 | 17 (21.8) | 18 (23.1) | 0.05 | 0.66 |
| Preop GFR < 60 mL/min, n (%) | 10 (11.2) | 12 (14.4) | 0.4 | 9 (11.5) | 9 (11.5) | 0.11 | 0.71 |
| LVEF < 50%, n (%) | 13 (14.6) | 15 (18.1) | 0.4 | 12 (15.4) | 13 (16.7) | 0.15 | 0.75 |
| Preoperative NYHA classification | |||||||
| I, n (%) | 69 (77.5) | 57 (68.7) | 0.5 | 60 (76.9) | 56 (71.8) | 0.09 | 0.89 |
| II, n (%) | 12 (13.5) | 16 (19.3) | 0.6 | 11 (14.1) | 14 (18) | 0.11 | 0.71 |
| III, n (%) | 5 (5.6) | 6 (7.2) | <0.001 | 4 (5.1) | 5 (6.4) | 0.13 | 0.77 |
| IV, n (%) | 3 (3.4) | 4 (4.8) | 0.3 | 3 (3.8) | 3 (3.8) | 0.08 | 0.91 |
| ASA classification | |||||||
| I, n (%) | 0 | 0 | 1 | 0 | 0 | - | 1 |
| II, n (%) | 0 | 0 | 1 | 0 | 0 | - | 1 |
| III, n (%) | 63 (70.8) | 61 (73.5) | 0.4 | 59 (75.7) | 58 (74.4) | 0.13 | 0.66 |
| IV, n (%) | 26 (29.2) | 22 (26.5) | 0.5 | 19 (24.3) | 20 (25.6) | 0.11 | 0.74 |
| Aneurysm behavior | |||||||
| MATD, mm [IQR] | 64 [55–71] | 66 [55–77] | 0.42 | 65 [55–69] | 65 [55–70] | 3.7 | 0.35 |
| Neck length, mm [IQR] | 13 [10–19] | 15 [11–22] | 0.12 | 14 [10–19] | 15 [11–21] | 6.8 | 0.18 |
| Neck angle, ° [IQR] | 43 [25–55] | 34 [22–41] | 0.05 | 38 [23–40] | 39 [24–40] | 4.8 | 0.37 |
| Neck diameter, mm [IQR] | 26 [22–29] | 24 [20–27] | 0.6 | 24 [21–28] | 24 [20–28] | 7.2 | 0.36 |
| Right CIA involvement, n (%) | 17 (19.1) | 13 (15.7) | 0.73 | 15 (19.2) | 12 (15.4) | 0.11 | 0.42 |
| Left CIA involvement, n (%) | 7 (7.9) | 9 (10.8) | 0.65 | 6 (7.7) | 8 (10.2) | 0.12 | 0.39 |
| Fusiform Shape, n (%) | 63 (70.8) | 59 (71.1) | 0.8 | 58 (74.4) | 55 (70.5) | 0.3 | 0.71 |
| Unmatched Cohort | Matched Cohort | ||||||
|---|---|---|---|---|---|---|---|
| Variables | SGC (89) | STD (83) | p | SGC (78) | STD (78) | SE Diff | p |
| Stents graft fabric | |||||||
| Endurant, n (%) | 64 (71.9) | 63 (75.9) | 0.42 | 58 (74.4) | 59 (75.6) | 0.12 | 1 |
| Endologix, n (%) | 16 (18) | 13 (15.7) | 0.5 | 13 (16.7) | 12 (15.4) | 0.12 | 1 |
| Zenith, n (%) | 5 (5.6) | 4 (4.8) | 0.3 | 4 (5.1) | 4 (5.1) | 0.15 | 1 |
| Excluder, n (%) | 4 (4.5) | 3 (3.6) | 0.3 | 3 (3.8) | 3 (3.8) | 0.13 | 1 |
| Number of components, n [IQR] | 2 [1–3] | 3 [1–4] | 0.16 | 2 [1–3] | 3 [1–3] | 1 | 0.8 |
| “Ballerina” configuration, n (%) | 48 (54) | 42 (50.6) | 0.54 | 41 (52.6) | 41 (52.6) | 0.21 | 0.71 |
| Operative time, min [IQR] | 66 [60–75] | 79 [68–85] | 0.73 | 73 [67–85] | 77 [74–86] | 2.1 | 0.07 |
| CGC time, min [IQR] | 3 [1–5] | 12 [7–17] | <0.001 | 4 [1–6] | 8 [6–14] | 1.2 | 0.001 |
| Mean contrast medium, mL [IQR] | 55 [45–72] | 81 [77–93] | <0.001 | 61 [50–72] | 77 [71–92] | 1.3 | 0.03 |
| Fluoroscopy time, min [IQR] | 11 [8–14] | 21 [13–23] | <0.001 | 12 [9–16] | 17 [12–25] | 1.4 | 0.001 |
| DAP, G*cm2 [IQR] | 14 [9–18] | 32 [28–36] | <0.001 | 15 [9–21] | 26 [16–34] | 0.1 | <0.001 |
| CGC Fluoroscopy time, sec [IQR] | 45 [27] | 96 [32] | <0.001 | 45 [26–65] | 96 [70–133] | 1 | 0.001 |
| CGC Time | |||||
|---|---|---|---|---|---|
| Aneurysm Behavior | Stents Graft Fabric | ||||
| MATD | Correlation | −0.108 | Endurant | Correlation | −0.043 |
| Sig (2-t) | 0.48 | Sig (2-t) | 0.777 | ||
| Neck length | Correlation | −0.139 | Endologix | Correlation | 0.164 |
| Sig (2-t) | 0.161 | Sig (2-t) | 0.281 | ||
| Neck angle | Correlation | −0.347 | Zenith | Correlation | −0.1 |
| Sig (2-t) | 0.02 | Sig (2-t) | 0.513 | ||
| Neck diameter | Correlation | 0.05 | Excluder | Correlation | −0.144 |
| Sig (2-t) | 0.744 | Sig (2-t) | −0.344 | ||
| Right CIA involvement | Correlation | 0.1 | Number of components | Correlation | −0.22 |
| Sig (2-t) | 0.513 | Sig (2-t) | 0.146 | ||
| Left CIA involvement | Correlation | 0.154 | “Ballerina” configuration | Correlation | −0.093 |
| Sig (2-t) | 0.312 | Sig (2-t) | 0.544 | ||
| Sacciform Shape | Correlation | 0.387 | Operative time | Correlation | −0.071 |
| Sig (2-t) | 0.04 | Sig (2-t) | 0.644 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mirabella, D.; Evola, S.; Dinoto, E.; Setacci, C.; Pakeliani, D.; Setacci, F.; Annicchiarico, P.; Pecoraro, F. Outcome Analysis of Speed Gate Cannulation during Standard Infrarenal Endovascular Aneurysm Repair. J. Clin. Med. 2023, 12, 6263. https://doi.org/10.3390/jcm12196263
Mirabella D, Evola S, Dinoto E, Setacci C, Pakeliani D, Setacci F, Annicchiarico P, Pecoraro F. Outcome Analysis of Speed Gate Cannulation during Standard Infrarenal Endovascular Aneurysm Repair. Journal of Clinical Medicine. 2023; 12(19):6263. https://doi.org/10.3390/jcm12196263
Chicago/Turabian StyleMirabella, Domenico, Salvatore Evola, Ettore Dinoto, Carlo Setacci, David Pakeliani, Francesco Setacci, Paolo Annicchiarico, and Felice Pecoraro. 2023. "Outcome Analysis of Speed Gate Cannulation during Standard Infrarenal Endovascular Aneurysm Repair" Journal of Clinical Medicine 12, no. 19: 6263. https://doi.org/10.3390/jcm12196263
APA StyleMirabella, D., Evola, S., Dinoto, E., Setacci, C., Pakeliani, D., Setacci, F., Annicchiarico, P., & Pecoraro, F. (2023). Outcome Analysis of Speed Gate Cannulation during Standard Infrarenal Endovascular Aneurysm Repair. Journal of Clinical Medicine, 12(19), 6263. https://doi.org/10.3390/jcm12196263