




The Effect of the COVID-19 Pandemic on Self-Reported Health Status and Smoking and Drinking Habits in the General Urban Population
 , , , , , ,
, , , , , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
3. Statistical Analysis
4. Results
5. Discussion
6. Conclusions
7. Study Limitation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Elling, J.M.; Crutzen, R.; Talhout, R.; de Vries, H. Tobacco smoking and smoking cessation in times of COVID-19. Tob. Prev. Cessat. 2020, 6, 39. [Google Scholar] [CrossRef] [PubMed]
- Clerkin, K.J.; Fried, J.A.; Raikhelkar, J.; Sayer, G.; Griffin, J.M.; Masoumi, A.; Jain, S.S.; Burkhoff, D.; Kumaraiah, D.; Rabbani, L.; et al. COVID-19 and Cardiovascular Disease. Circulation 2020, 141, 1648–1655. [Google Scholar] [CrossRef] [PubMed]
- Cevik, M.; Bamford, C.G.G.; Ho, A. COVID-19 pandemic-a focused review for clinicians. Clin. Microbiol. Infect. 2020, 26, 842–847. [Google Scholar] [CrossRef] [PubMed]
- WHO. Coronavirus (COVID-19) Statistics. Available online: https://covid19.who.int/region/euro/country/pl (accessed on 28 December 2022).
- Postawy Polaków Wobec Palenia Tytoniu—Raport 2019. Available online: https://www.gov.pl/web/gis/postawy-polakow-wobec-palenia-tytoniu--raport-2017 (accessed on 3 January 2023).
- Schuckit, M.A. Alcohol-use disorders. Lancet 2009, 373, 492–501. [Google Scholar] [CrossRef] [PubMed]
- OECD. Data Alcohol Consumption. Available online: https://data.oecd.org/healthrisk/alcohol-consumption.htm (accessed on 3 January 2023).
- Chlabicz, M.; Jamiolkowski, J.; Laguna, W.; Sowa, P.; Paniczko, M.; Lapinska, M.; Szpakowicz, M.; Drobek, N.; Raczkowski, A.; Kaminski, K.A. A Similar Lifetime CV Risk and a Similar Cardiometabolic Profile in the Moderate and High Cardiovascular Risk Populations: A Population-Based Study. J. Clin. Med. 2021, 10, 1584. [Google Scholar] [CrossRef]
- Chlabicz, M.; Jamiolkowski, J.; Laguna, W.; Dubatowka, M.; Sowa, P.; Lapinska, M.; Szpakowicz, A.; Zieleniewska, N.; Zalewska, M.; Raczkowski, A.; et al. Effectiveness of Lifestyle Modification vs. Therapeutic, Preventative Strategies for Reducing Cardiovascular Risk in Primary Prevention-A Cohort Study. J. Clin. Med. 2022, 11, 688. [Google Scholar] [CrossRef]
- Saunders, J.B.; Aasland, O.G. WHO Collaborative Project on Identification and Treatment of Persons with Harmful Alcohol Consumption. Report on Phase I. In Development of a Screening Instrument; WHO: Geneva, Switzerland, 1987. [Google Scholar]
- Higgins-Biddle, J.C.; Babor, T.F. A review of the Alcohol Use Disorders Identification Test (AUDIT), AUDIT-C, and USAUDIT for screening in the United States: Past issues and future directions. Am. J. Drug Alcohol. Abuse 2018, 44, 578–586. [Google Scholar] [CrossRef]
- Heatherton, T.F.; Kozlowski, L.T.; Frecker, R.C.; Fagerstrom, K.O. The Fagerstrom Test for Nicotine Dependence: A revision of the Fagerstrom Tolerance Questionnaire. Br. J. Addict. 1991, 86, 1119–1127. [Google Scholar] [CrossRef]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The Satisfaction With Life Scale. J. Pers. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef]
- Le Foll, B.; Piper, M.E.; Fowler, C.D.; Tonstad, S.; Bierut, L.; Lu, L.; Jha, P.; Hall, W.D. Tobacco and nicotine use. Nat. Rev. Dis. Primers 2022, 8, 19. [Google Scholar] [CrossRef]
- Kayhan Tetik, B.; Gedik Tekinemre, I.; Tas, S. The Effect of the COVID-19 Pandemic on Smoking Cessation Success. J. Community Health 2021, 46, 471–475. [Google Scholar] [CrossRef] [PubMed]
- Nyman, A.L.; Spears, C.A.; Churchill, V.; Do, V.V.; Henderson, K.C.; Massey, Z.B.; Reynolds, R.M.; Huang, J. Associations between COVID-19 risk perceptions and smoking and quitting behavior among U.S. adults. Addict. Behav. Rep. 2021, 14, 100394. [Google Scholar] [CrossRef] [PubMed]
- Celik, F.G.N.; Demirel, G. Impact of a Coronavirus Pandemic on Smoking Behavior in University Students: An Online Survey in Turkiye. Turk. J. Pharm. Sci. 2022, 19, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Roberts, A.; Rogers, J.; Mason, R.; Siriwardena, A.N.; Hogue, T.; Whitley, G.A.; Law, G.R. Alcohol and other substance use during the COVID-19 pandemic: A systematic review. Drug Alcohol. Depend. 2021, 229, 109150. [Google Scholar] [CrossRef]
- Killgore, W.D.S.; Cloonan, S.A.; Taylor, E.C.; Lucas, D.A.; Dailey, N.S. Alcohol dependence during COVID-19 lockdowns. Psychiatry Res. 2021, 296, 113676. [Google Scholar] [CrossRef]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef]
- Choi, H.G.; Kim, S.Y.; Joo, Y.H.; Cho, H.J.; Kim, S.W.; Jeon, Y.J. Incidence of Asthma, Atopic Dermatitis, and Allergic Rhinitis in Korean Adults before and during the COVID-19 Pandemic Using Data from the Korea National Health and Nutrition Examination Survey. Int. J. Environ. Res. Public. Health 2022, 19, 4274. [Google Scholar] [CrossRef]
- Loewenthal, L.; Menzies-Gow, A. FeNO in Asthma. Semin. Respir. Crit. Care Med. 2022, 43, 635–645. [Google Scholar] [CrossRef]
- Barnes, P.J.; Dweik, R.A.; Gelb, A.F.; Gibson, P.G.; George, S.C.; Grasemann, H.; Pavord, I.D.; Ratjen, F.; Silkoff, P.E.; Taylor, D.R.; et al. Exhaled nitric oxide in pulmonary diseases: A comprehensive review. Chest 2010, 138, 682–692. [Google Scholar] [CrossRef]
- Gewurz, H. Biology of C-reactive protein and the acute phase response. Hosp. Pract. 1982, 17, 67–81. [Google Scholar] [CrossRef]
- McFadyen, J.D.; Kiefer, J.; Braig, D.; Loseff-Silver, J.; Potempa, L.A.; Eisenhardt, S.U.; Peter, K. Dissociation of C-Reactive Protein Localizes and Amplifies Inflammation: Evidence for a Direct Biological Role of C-Reactive Protein and Its Conformational Changes. Front. Immunol. 2018, 9, 1351. [Google Scholar] [CrossRef] [PubMed]
- Maamar, M.; Artime, A.; Pariente, E.; Fierro, P.; Ruiz, Y.; Gutierrez, S.; Tobalina, M.; Diaz-Salazar, S.; Ramos, C.; Olmos, J.M.; et al. Post-COVID-19 syndrome, low-grade inflammation and inflammatory markers: A cross-sectional study. Curr. Med. Res. Opin. 2022, 38, 901–909. [Google Scholar] [CrossRef] [PubMed]
- Gul, M.; Ozyilmaz, S.; Bastug Gul, Z.; Kacmaz, C.; Satilmisoglu, M.H. Evaluation of cardiac injury with biomarkers and echocardiography after COVID-19 infection. J. Physiol. Pharmacol. 2022, 73, 89–95. [Google Scholar] [CrossRef]
- Wang, W.; Zhu, L.; Zheng, S.; Ji, Y.; Xiang, Y.; Lv, B.; Xiong, L.; Li, Z.; Yi, S.; Huang, H.; et al. Survey on the Progression of Myopia in Children and Adolescents in Chongqing During COVID-19 Pandemic. Front. Public Health 2021, 9, 646770. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variable | Population before the COVID-19 Pandemic N = 713 | Population during the COVID-19 Pandemic N = 509 | p |
|---|---|---|---|
| Age, years | 48.7 ± 15.4 | 49.3 ± 14.5 | 0.487 |
| Male sex, n (%) | 322 (45.2) | 248 (48.7) | 0.219 |
| Height, cm | 170.1 ± 10.1 | 170.8 ± 9.5 | 0.179 |
| Weight, kg | 77.9 ± 16.7 | 79.3 ± 16.2 | 0.072 |
| BMI, kg/m2 | 26.8 ± 4.9 | 27.2 ± 5.2 | 0.388 |
| WHR | 0.88 ± 0.1 | 0.86 ± 0.1 | 0.006 |
| Laboratory parameters | |||
| hs-CRP, mg/L | 1.5 ± 3.6 | 1.7 ± 3.1 | 0.001 |
| FeNO, ppb | 18.7 ± 15.4 | 21.3 ± 18.8 | <0.001 |
| WBC, 103/uL | 6.25 ± 1.6 | 5.8 ± 1.5 | <0.001 |
| Hgb, g/dL | 14.1 ± 1.4 | 13.9 ± 1.3 | 0.057 |
| Hct, % | 41.1 ± 3.8 | 40.9 ± 3.7 | 0.396 |
| PLT × 109/L | 236 ± 62.8 | 235.9 ± 60.3 | 0.821 |
| Spirometry | |||
| FVC, L | 4.3 ± 1.2 | 4.3 ± 1.1 | 0.678 |
| FEV1/FVC, % | 79.1 ± 6.9 | 78.9 ± 6.6 | 0.302 |
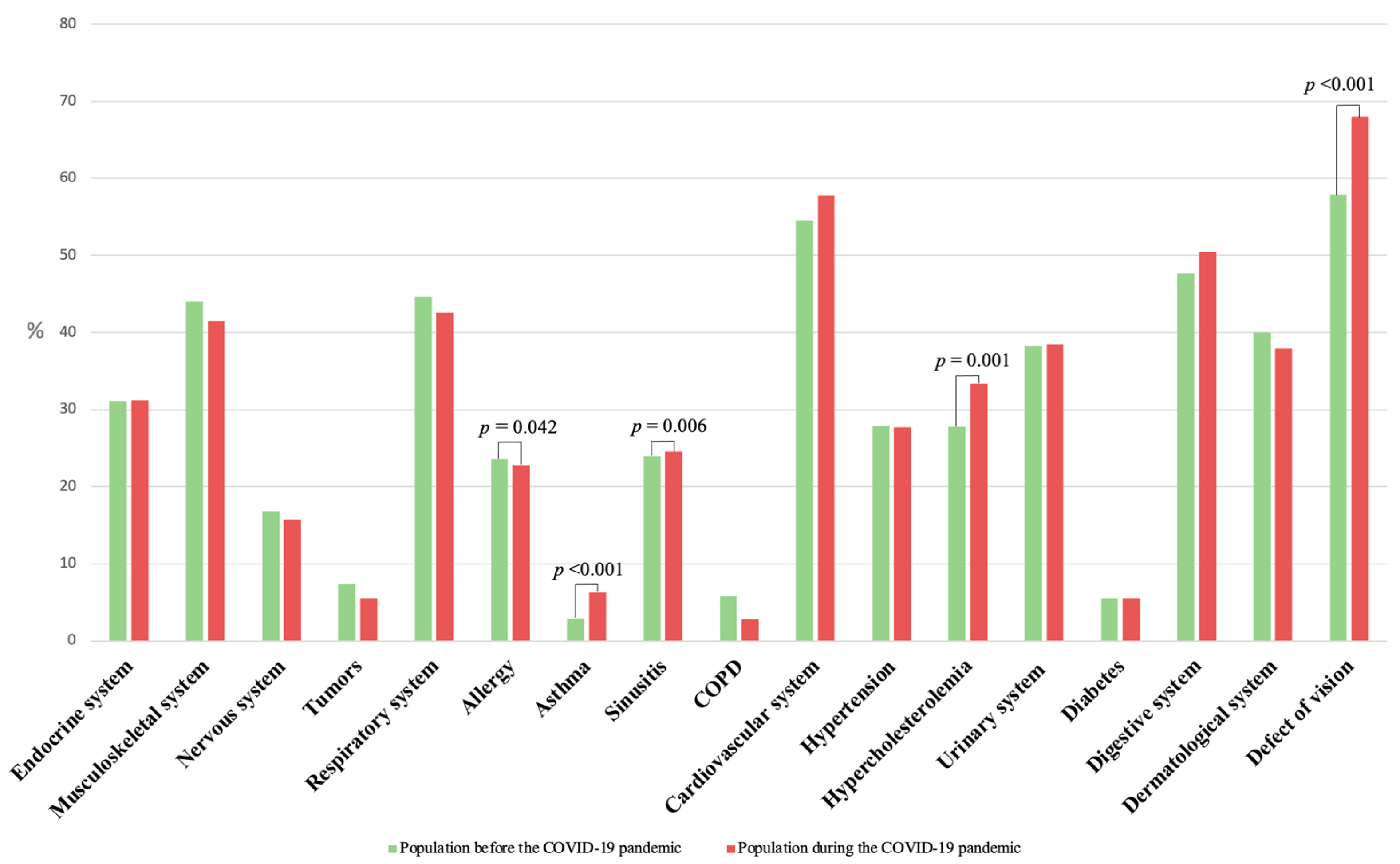
| Disease | Population before the COVID-19 Pandemic N = 713 | Population during the COVID-19 Pandemic N = 509 | p |
|---|---|---|---|
| Endocrine system | 222 (31.1) | 159 (31.2) | 0.901 |
| Musculoskeletal system | 314 (44.0) | 211 (41.5) | 0.369 |
| Nervous system | 120 (16.8) | 80 (15.7) | 0.636 |
| Tumors | 53 (7.4) | 28 (5.5) | 0.184 |
| Respiratory system | 318 (44.6) | 217 (42.6) | 0.678 |
| Allergy | 168 (23.6) | 116 (22.8) | 0.042 |
| Asthma | 21 (2.9) | 32 (6.3) | <0.001 |
| Sinusitis | 171 (24.0) | 125 (24.6) | 0.006 |
| COPD | 41 (5.8) | 14 (2.8) | 0.076 |
| Cardiovascular system | 389 (54.6) | 294 (57.8) | 0.262 |
| Hypertension | 199 (27.9) | 141 (27.7) | 0.469 |
| Hypercholesterolemia | 198 (27.8) | 170 (33.4) | 0.001 |
| Urinary system | 273 (38.3) | 196 (38.5) | 0.941 |
| Diabetes | 39 (5.5) | 28 (5.5) | 0.168 |
| Digestive system | 340 (47.7) | 257 (50.5) | 0.270 |
| Dermatological system | 285 (40.0) | 193 (37.9) | 0.506 |
| Defect of vision | 413 (57.9) | 346 (68.0) | <0.001 |
| Lifestyle Habits | Population before the COVID-19 Pandemic N = 713 | Population during the COVID-19 Pandemic N = 509 | p |
|---|---|---|---|
| Smoking habits | |||
| Ever smoked cigarettes | 402 (56.4) | 289 (56.8) | 0.998 |
| Currently smoking | 136 (19.1) | 94 (18.5) | 0.795 |
| Number of cigarettes smoked during the day | 14.0 ± 9.1 | 10.7 ± 7.1 | 0.005 |
| The highest number of cigarettes smoked during the day | 20.7 ± 10.6 | 16.7 ± 7.4 | 0.117 |
| Individuals planning to quit smoking within 6 months | 46 (33.8) | 37 (39.4) | 0.049 |
| Fagerström Test for Nicotine Dependence score | 3.2 ± 2.3 | 2.4 ± 2.2 | 0.007 |
| Drinking habits | |||
| Drinking alcoholic beverages in the last 30 days | 512 (71.8) | 361 (70.9) | 0.564 |
| Drinking beer in the last 30 days | 326 (45.7) | 195 (38.3) | 0.404 |
| Drinking alcohol in the last 30 days | 232 (32.5) | 147 (28.9) | 0.930 |
| Drinking liqueurs, fruit liqueurs, drink in the last 30 days | 115 (16.1) | 70 (13.8) | 0.808 |
| Drinking wine in the last 30 days | 222 (31.1) | 152 (29.9) | 0.300 |
| How many times have a beer been drunk in the last 30 days | 5.9 ± 6.7 | 9.6 ± 5.4 | 0.908 |
| Beer quantity in milliliters drunk in the last 30 days | 2243.5 ± 3221.5 | 1327.8 ± 1337.2 | 0.991 |
| How many times has alcohol been drunk in the last 30 days | 2.7 ± 2.5 | 3.0 ± 3.7 | 0.720 |
| Alcohol quantity in milliliters drunk in the last 30 days | 331.9 ± 417.9 | 324.2 ± 364.4 | 0.4366 |
| How many times has liqueurs, fruit liqueurs, drinks drunk in the last 30 days | 2.9 ± 2.7 | 2.3 ± 2.3 | 0.018 |
| Liqueurs, fruit liqueurs, drink quantity in milliliters drunk in the last 30 days | 195.8 ± 282.2 | 339.9 ± 449.5 | 0.052 |
| How many times have wine been drunk in the last 30 days | 4.9 ± 4.1 | 2.6 ± 2.2 | 0.153 |
| Wine quantity in milliliters drunk in the last 30 days | 343.7 ± 427 | 389.4 ± 403.7 | 0.144 |
| Alcohol Use Disorders Identification Test score | 4 ± 3.7 | 3.6 ± 3.0 | 0.329 |
| The Satisfaction with Life Scale (SWLS) | |||
| SWLS | 22.7 ± 5.2 | 22.4 ± 5.2 | 0.407 |
| Variable | p |
|---|---|
| Age | 0.724 |
| Sex | 0.327 |
| BMI | 0.184 |
| Education | 0.493 |
| Income | 0.482 |
| FeNO, ppb | 0.722 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chlabicz, M.; Szum-Jakubowska, A.; Sowa, P.; Chlabicz, M.; Sołomacha, S.; Kiszkiel, Ł.; Minarowski, Ł.; Guziejko, K.; Laskowski, P.P.; Moniuszko-Malinowska, A.M.; et al. The Effect of the COVID-19 Pandemic on Self-Reported Health Status and Smoking and Drinking Habits in the General Urban Population. J. Clin. Med. 2023, 12, 6241. https://doi.org/10.3390/jcm12196241
Chlabicz M, Szum-Jakubowska A, Sowa P, Chlabicz M, Sołomacha S, Kiszkiel Ł, Minarowski Ł, Guziejko K, Laskowski PP, Moniuszko-Malinowska AM, et al. The Effect of the COVID-19 Pandemic on Self-Reported Health Status and Smoking and Drinking Habits in the General Urban Population. Journal of Clinical Medicine. 2023; 12(19):6241. https://doi.org/10.3390/jcm12196241
Chicago/Turabian StyleChlabicz, Magdalena, Aleksandra Szum-Jakubowska, Paweł Sowa, Małgorzata Chlabicz, Sebastian Sołomacha, Łukasz Kiszkiel, Łukasz Minarowski, Katarzyna Guziejko, Piotr P. Laskowski, Anna M. Moniuszko-Malinowska, and et al. 2023. "The Effect of the COVID-19 Pandemic on Self-Reported Health Status and Smoking and Drinking Habits in the General Urban Population" Journal of Clinical Medicine 12, no. 19: 6241. https://doi.org/10.3390/jcm12196241
APA StyleChlabicz, M., Szum-Jakubowska, A., Sowa, P., Chlabicz, M., Sołomacha, S., Kiszkiel, Ł., Minarowski, Ł., Guziejko, K., Laskowski, P. P., Moniuszko-Malinowska, A. M., & Kamiński, K. A. (2023). The Effect of the COVID-19 Pandemic on Self-Reported Health Status and Smoking and Drinking Habits in the General Urban Population. Journal of Clinical Medicine, 12(19), 6241. https://doi.org/10.3390/jcm12196241