
Dialysis Patients Respond Adequately to Influenza Vaccination Irrespective of Dialysis Modality and Chronic Inflammation

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Influenza Vaccination
2.3. Demographics and Clinical Data
2.4. Influenza Antibody Titers and Outcome Measures
2.5. Statistical Analysis
3. Results
3.1. Study Population
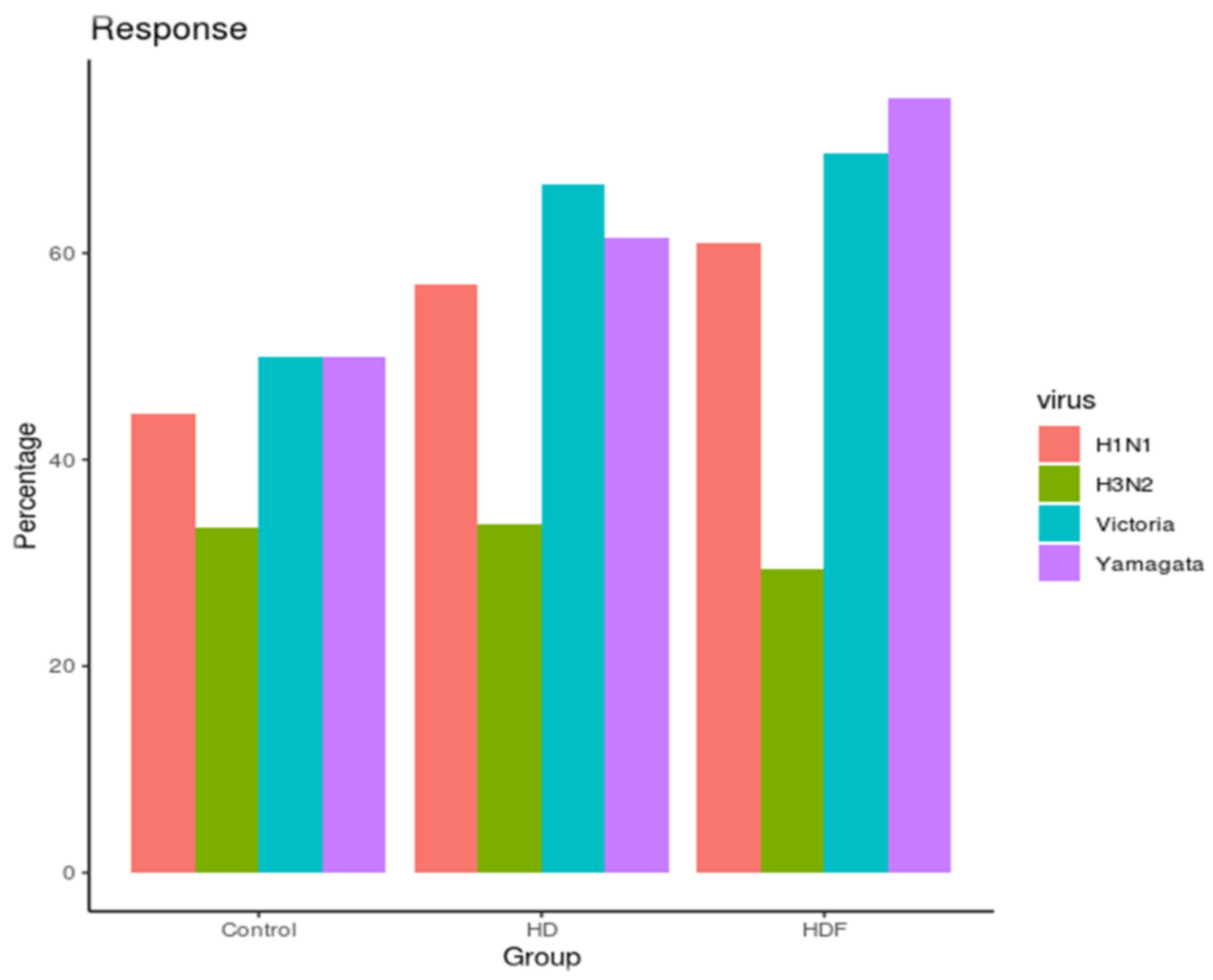
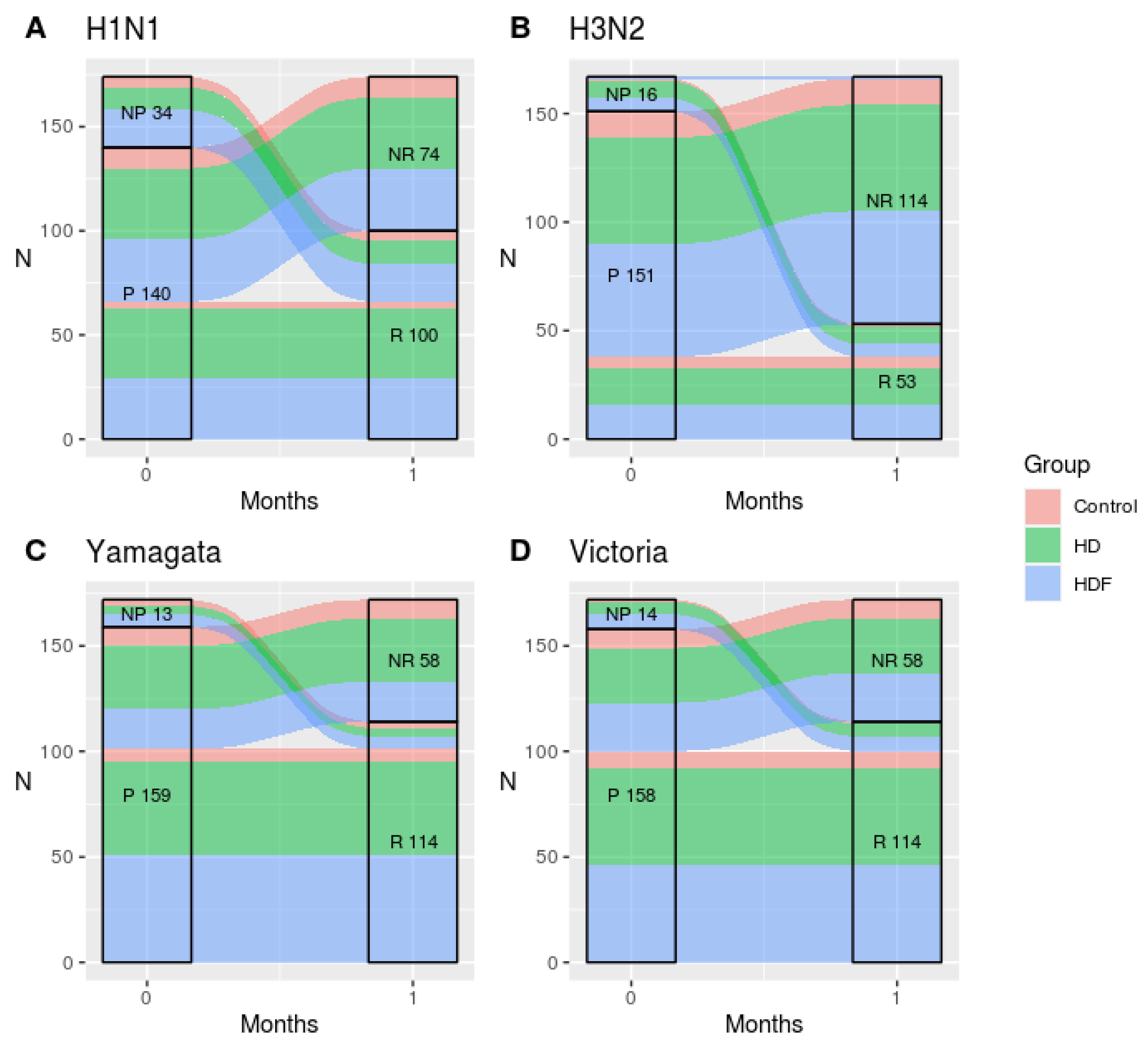
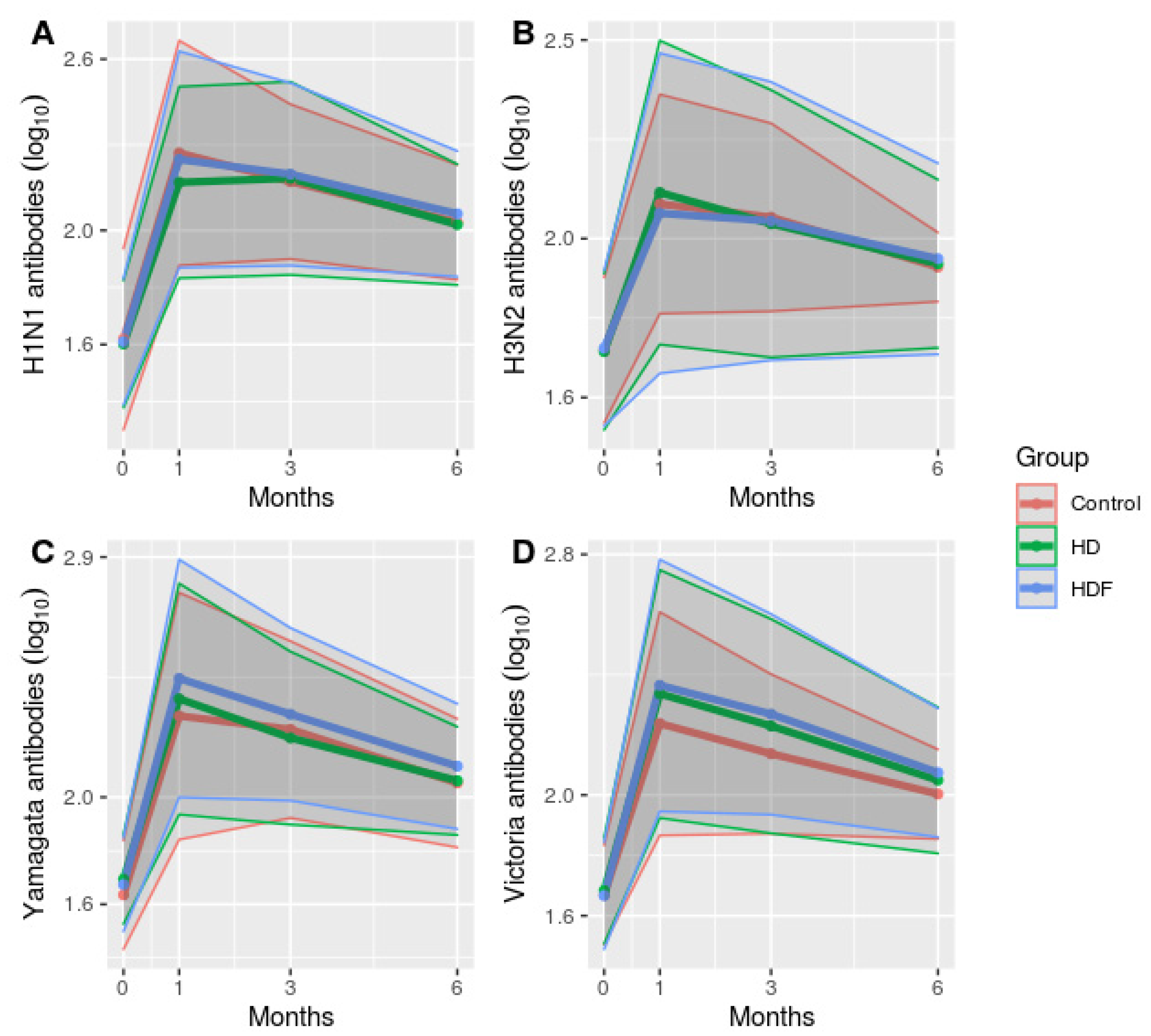
3.2. Immune Response to Influenza Vaccination
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Piret, J.; Boivin, G. Pandemics throughout History. Front. Microbiol. 2021, 11, 631736. [Google Scholar] [CrossRef]
- Plotkin, S.A. Vaccines: Past, present and future. Nat. Med. 2005, 11 (Suppl. S4), S5–S11. [Google Scholar] [CrossRef] [PubMed]
- Plotkin, S. History of vaccination. Proc. Natl. Acad. Sci. USA 2014, 111, 12283–12287. [Google Scholar] [CrossRef] [PubMed]
- Buchy, P.; Buisson, Y.; Cintra, O.; Dwyer, D.E.; Nissen, M.; de Lejarazu, R.O.; Petersen, E. COVID-19 pandemic: Lessons learned from more than a century of pandemics and current vaccine development for pandemic control. Int. J. Infect. Dis. 2021, 112, 300–317. [Google Scholar] [CrossRef] [PubMed]
- Kilbourne, E.D. Influenza Pandemics of the 20th Century. Emerg. Infect. Dis. 2006, 12, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Paules, C.I.; Sullivan, S.G.; Subbarao, K.; Fauci, A.S. Chasing Seasonal Influenza—The Need for a Universal Influenza Vaccine. N. Engl. J. Med. 2018, 378, 7–9. [Google Scholar] [CrossRef]
- Eleftheriadis, T.; Antoniadi, G.; Liakopoulos, V.; Kartsios, C.; Stefanidis, I. Disturbances of acquired immunity in hemodialysis patients. Semin. Dial. 2007, 20, 440–451. [Google Scholar] [CrossRef]
- Betjes, M.G.H. Immune cell dysfunction and inflammation in end-stage renal disease. Nat. Rev. Nephrol. 2013, 9, 255–265. [Google Scholar] [CrossRef]
- Vaziri, N.D.; Pahl, M.V.; Crum, A.; Norris, K. Effect of uremia on structure and function of immune system. J. Ren. Nutr. 2012, 22, 149–156. [Google Scholar] [CrossRef]
- Kuroki, Y.; Tsuchida, K.; Go, I.; Aoyama, M.; Naganuma, T.; Takemoto, Y.; Nakatani, T. A study of innate immunity in patients with end-stage renal disease: Special reference to toll-like receptor-2 and -4 expression in peripheral blood monocytes of hemodialysis patients. Int. J. Mol. Med. 2007, 19, 783–790. [Google Scholar] [CrossRef]
- Fernández-Fresnedo, G.; Ramos, M.A.; González-Pardo, M.C.; de Francisco, A.L.; López-Hoyos, M.; Arias, M. B lymphopenia in uremia is related to an accelerated in vitro apoptosis and dysregulation of Bcl-2. Nephrol. Dial. Transplant. 2000, 15, 502–510. [Google Scholar] [CrossRef]
- Ando, M.; Shibuya, A.; Tsuchiya, K.; Akiba, T.; Nitta, K. Reduced expression of Toll-like receptor 4 contributes to impaired cytokine response of monocytes in uremic patients. Kidney Int. 2006, 70, 358–362. [Google Scholar] [CrossRef]
- Kato, S.; Chmielewski, M.; Honda, H.; Pecoits-Filho, R.; Matsuo, S.; Yuzawa, Y.; Tranaeus, A.; Stenvinkel, P.; Lindholm, B. Aspects of immune dysfunction in end-stage renal disease. Clin. J. Am. Soc. Nephrol. 2008, 3, 1526–1533. [Google Scholar] [CrossRef]
- Wakasugi, M.; Kawamura, K.; Yamamoto, S.; Kazama, J.J.; Narita, I. High mortality rate of infectious diseases in dialysis patients: A comparison with the general population in Japan. Ther. Apher. Dial. 2012, 16, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Marcelli, D.; Marelli, C.; Richards, N. Influenza A(H1N1)v pandemic in the dialysis population: First wave results from an international survey. Nephrol. Dial. Transplant. 2009, 24, 3566–3572. [Google Scholar] [CrossRef] [PubMed]
- Vaccines against influenza WHO position paper—November 2012. Wkly. Epidemiol. Rec. 2012, 87, 461–476.
- Mastalerz-Migas, A.; Gwiazda, E.; Brydak, L.B. Effectiveness of influenza vaccine in patients on hemodialysis—A review. Med. Sci. Monit. 2013, 19, 1013–1018. [Google Scholar] [CrossRef] [PubMed]
- Ghadiani, M.H.; Besharati, S.; Mousavinasab, N.; Jalalzadeh, M. Response rates to HB vaccine in CKD stages 3-4 and hemodialysis patients. J. Res. Med. Sci. 2012, 17, 527–533. [Google Scholar]
- Krüger, S.; Müller-Steinhardt, M.; Kirchner, H.; Kreft, B. A 5-year follow-up on antibody response after diphtheria and tetanus vaccination in hemodialysis patients. Am. J. Kidney Dis. 2001, 38, 1264–1270. [Google Scholar] [CrossRef]
- Pourfarziani, V.; Ramezani, M.B.; Taheri, S.; Izadi, M.; Einollahi, B. Immunogenicity of pneumococcal vaccination in renal transplant recipients and hemodialysis patients: A comparative controlled trial. Ann. Transplant. 2008, 13, 43–47. [Google Scholar]
- Vandecasteele, S.J.; De Bacquer, D.; Caluwe, R.; Ombelet, S.; Van Vlem, B. Immunogenicity and safety of the 13-valent Pneumococcal Conjugate vaccine in 23-valent pneumococcal polysaccharide vaccine-naive and pre-immunized patients under treatment with chronic haemodialysis: A longitudinal quasi-experimental phase IV study. Clin. Microbiol. Infect. 2018, 24, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Mitra, S.; Stein, G.E.; Bhupalam, S.; Havlichek, D.H. Immunogenicity of 13-Valent Conjugate Pneumococcal Vaccine in Patients 50 Years and Older with End-Stage Renal Disease and on Dialysis. Clin. Vaccine Immunol. 2016, 23, 884–887. [Google Scholar] [CrossRef] [PubMed]
- Espi, M.; Charmetant, X.; Barba, T.; Koppe, L.; Pelletier, C.; Kalbacher, E.; Chalencon, E.; Mathias, V.; Ovize, A.; Cart-Tanneur, E.; et al. The ROMANOV study found impaired humoral and cellular immune responses to SARS-CoV-2 mRNA vaccine in virus-unexposed patients receiving maintenance hemodialysis. Kidney Int. 2021, 100, 928–936. [Google Scholar] [CrossRef] [PubMed]
- El Karoui, K.; De Vriese, A.S. COVID-19 in dialysis: Clinical impact, immune response, prevention, and treatment. Kidney Int. 2022, 101, 883–894. [Google Scholar] [CrossRef]
- Merino, A.; Portolés, J.; Selgas, R.; Ojeda, R.; Buendia, P.; Ocaña, J.; Bajo, M.A.; del Peso, G.; Carracedo, J.; Ramírez, R.; et al. Effect of different dialysis modalities on microinflammatory status and endothelial damage. Clin. J. Am. Soc. Nephrol. 2010, 5, 227–234. [Google Scholar] [CrossRef]
- den Hoedt, C.H.; Bots, M.L.; Grooteman, M.P.C.; van der Weerd, N.C.; Mazairac, A.H.A.; Penne, E.L.; Levesque, R.; ter Wee, P.M.; Nubé, M.J.; Blankestijn, P.J.; et al. Online hemodiafiltration reduces systemic inflammation compared to low-flux hemodialysis. Kidney Int. 2014, 86, 423–432. [Google Scholar] [CrossRef]
- Carracedo, J.; Merino, A.; Nogueras, S.; Carretero, D.; Berdud, I.; Ramírez, R.; Tetta, C.; Rodríguez, M.; Martín-Malo, A.; Aljama, P. On-line hemodiafiltration reduces the proinflammatory CD14+CD16+ monocyte-derived dendritic cells: A prospective, crossover study. J. Am. Soc. Nephrol. 2006, 17, 2315–2321. [Google Scholar] [CrossRef]
- Ficociello, L.H.; Busink, E.; Sawin, D.-A.; Winter, A. Global real-world data on hemodiafiltration: An opportunity to complement clinical trial evidence. Semin. Dial. 2022, 35, 440–445. [Google Scholar] [CrossRef]
- Blankestijn, P.J.; Vernooij, R.W.M.; Hockham, C.; Strippoli, G.F.M.; Canaud, B.; Hegbrant, J.; Barth, C.; Covic, A.; Cromm, K.; Cucui, A.; et al. Effect of Hemodiafiltration or Hemodialysis on Mortality in Kidney Failure. N. Engl. J. Med. 2023, 389, 700–709. [Google Scholar] [CrossRef]
- Morena, M.; Jaussent, A.; Chalabi, L.; Leray-Moragues, H.; Chenine, L.; Debure, A.; Thibaudin, D.; Azzouz, L.; Patrier, L.; Maurice, F.; et al. Treatment tolerance and patient-reported outcomes favor online hemodiafiltration compared to high-flux hemodialysis in the elderly. Kidney Int. 2017, 91, 1495–1509. [Google Scholar] [CrossRef]
- WHO. Recommendations for Influenza Virus Vaccine Composition for the 2017 Southern Hemisphere Season. Available online: https://www.ecdc.europa.eu/en/news-events/who-recommendations-influenza-virus-vaccine-composition-2017-southern-hemisphere-season (accessed on 31 May 2023).
- EMA. Regulatory Information—EU Recommendations for Composition of 2016/2017 Seasonal Influenza Vaccines. European Medicines Agency. Available online: https://www.ema.europa.eu/en/news/regulatory-information-eu-recommendations-composition-20162017-seasonal-influenza-vaccines (accessed on 31 May 2023).
- EMA. Harmonisation of Requirements for Influenza Vaccines. European Medicines Agency. Available online: https://www.ema.europa.eu/en/harmonisation-requirements-influenza-vaccines (accessed on 2 June 2023).
- Center for Biologics Evaluation and Research. Clinical Data Needed to Support the Licensure of Pandemic Influenza Vaccines. U.S. Food and Drug Administration. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/clinical-data-needed-support-licensure-pandemic-influenza-vaccines (accessed on 2 June 2023).
- de Jong, J.C.; Palache, A.M.; Beyer, W.E.P.; Rimmelzwaan, G.F.; Boon, A.C.M.; Osterhaus, A.D.M.E. Haemagglutination-inhibiting antibody to influenza virus. Dev. Biol. 2003, 115, 63–73. [Google Scholar]
- R Development Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022; ISBN 3-900051-07-0. [Google Scholar]
- Krueger, K.M.; Ison, M.G.; Ghossein, C. Practical Guide to Vaccination in All Stages of CKD, Including Patients Treated by Dialysis or Kidney Transplantation. Am. J. Kidney Dis. 2020, 75, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Kosmadakis, G.; Albaret, J.; Correia, E.D.C.; Somda, F.; Aguilera, D. Vaccination practices in dialysis patients: A narrative review. Semin. Dial. 2018, 31, 507–518. [Google Scholar] [CrossRef] [PubMed]
- DaRoza, G.; Loewen, A.; Djurdjev, O.; Love, J.; Kempston, C.; Burnett, S.; Kiaii, M.; Taylor, P.A.; Levin, A. Stage of chronic kidney disease predicts seroconversion after hepatitis B immunization: Earlier is better. Am. J. Kidney Dis. 2003, 42, 1184–1192. [Google Scholar] [CrossRef] [PubMed]
- Kreft, B.; Klouche, M.; Kreft, R.; Kirchner, H.; Sack, K. Low efficiency of active immunization against diphtheria in chronic hemodialysis patients. Kidney Int. 1997, 52, 212–216. [Google Scholar] [CrossRef]
- Brydak, L.B.; Tadeusz, S.; Magdalena, M. Antibody response to influenza vaccination in healthy adults. Viral Immunol. 2004, 17, 609–615. [Google Scholar] [CrossRef]
- Scharpé, J.; Peetermans, W.E.; Vanwalleghem, J.; Maes, B.; Bammens, B.; Claes, K.; Osterhaus, A.D.; Vanrenterghem, Y.; Evenepoel, P. Immunogenicity of a standard trivalent influenza vaccine in patients on long-term hemodialysis: An open-label trial. Am. J. Kidney Dis. 2009, 54, 77–85. [Google Scholar] [CrossRef]
- Keitel, W.A.; Voronca, D.C.; Atmar, R.L.; Paust, S.; Hill, H.; Wolff, M.C.; Bellamy, A.R.; VTEU H5N1 Vaccine Working Group. Effect of recent seasonal influenza vaccination on serum antibody responses to candidate pandemic influenza A/H5N1 vaccines: A meta-analysis. Vaccine 2019, 37, 5535–5543. [Google Scholar] [CrossRef]
- Panichi, V.; Rizza, G.M.; Paoletti, S.; Bigazzi, R.; Aloisi, M.; Barsotti, G.; Rindi, P.; Donati, G.; Antonelli, A.; Panicucci, E.; et al. Chronic inflammation and mortality in haemodialysis: Effect of different renal replacement therapies. Results from the RISCAVID study. Nephrol. Dial. Transplant. 2008, 23, 2337–2343. [Google Scholar] [CrossRef]
- Ohmit, S.E.; Petrie, J.G.; Cross, R.T.; Johnson, E.; Monto, A.S. Influenza hemagglutination-inhibition antibody titer as a correlate of vaccine-induced protection. J. Infect. Dis. 2011, 204, 1879–1885. [Google Scholar] [CrossRef]
- Hannoun, C.; Megas, F.; Piercy, J. Immunogenicity and protective efficacy of influenza vaccination. Virus Res. 2004, 103, 133–138. [Google Scholar] [CrossRef] [PubMed]
- EMA. Influenza Vaccines—Non-Clinical and Clinical Module Scientific Guideline. European Medicines Agency. Available online: https://www.ema.europa.eu/en/influenza-vaccines-non-clinical-clinical-module-scientific-guideline (accessed on 21 June 2023).
- Manley, H.J.; Lacson, E.K.; Aweh, G.; Chen Li, N.; Weiner, D.E.; Miskulin, D.C.; Hsu, C.M.; Kapoian, T.; Hayney, M.S.; Meyer, K.B.; et al. Seroresponse to Inactivated and Recombinant Influenza Vaccines Among Maintenance Hemodialysis Patients. Am. J. Kidney Dis. 2022, 80, 309–318. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Total | Control | HD | HDF | p-Value HD vs. Control | p-Value HDF vs. Control | p-Value HD vs. HDF | |
|---|---|---|---|---|---|---|---|
| N | 189 | 18 | 87 | 84 | |||
| Age | 62.6 ± 13.4 | 60.9 ± 11.6 | 65.3 ± 13.4 | 60.2 ± 13.3 | <0.05 | NS | <0.05 |
| Male/Female | 122/67 | 6/12 | 63/24 | 53/32 | <0.05 | <0.05 | <0.05 |
| Diabetes | 50 (26.5%) | 2 (12.5%) | 30 (34.5%) | 19 (22.6%) | <0.05 | <0.05 | <0.05 |
| Dialysis vintage (months) | NA | 45.1 ± 41.3 | 62 ± 61.4 | NA | NA | <0.05 | |
| CVC | NA | 19 (21.8%) | 6 (7.1%) | NA | NA | <0.05 | |
| Fistula | NA | 49 (56.3%) | 63 (75%) | NA | NA | <0.05 | |
| Graft | NA | 18 (20.7%) | 15 (17.9%) | NA | NA | NS | |
| HDF volume (L) | NA | NA | 19.79 ± 4.06 | NA | NA | NA | |
| CRP | 0.969 ± 1.58 | 0.331 ± 0.337 | 0.995 ± 1.567 | 0.987 ± 1.649 | NS | NS | NS |
| IL-6 | 5.81 ± 10.15 | 0.76 ± 2.2 | 7.53 ± 10.76 | 5.27 ± 10.25 | <0.05 | <0.05 | <0.05 |
| Control (%) | HD (%) | HDF (%) | Total (%) | P | |
|---|---|---|---|---|---|
| H1N1 | |||||
| SR | 44.4% | 57% | 61% | 57.5% | 0.43 |
| SP-month 0 | 72.2% | 87.1% | 77.2% | 81.3% | 0.16 |
| SP-month 1 | 100% | 100% | 100% | 100% | NA |
| SP-month 3 | 100% | 100% | 100% | 100% | NA |
| SP-month 6 | 100% | 100% | 100% | 100% | NA |
| H3N2 | |||||
| SR | 33.3% | 33.8% | 29.3% | 31.7% | 0.83 |
| SP-month 0 | 94.4% | 90.6% | 91.1% | 91.2% | 0.87 |
| SP-month 1 | 100% | 100% | 98.7% | 99.4% | 0.54 |
| SP-month 3 | 100% | 100% | 98.7% | 99.4% | 0.52 |
| SP-month 6 | 100% | 100% | 98.6% | 99.4% | 0.55 |
| Yamagata | |||||
| SR | 50% | 61.5% | 75.0% | 66.3% | 0.06 |
| SP-month 0 | 83.3% | 95.3% | 92.4% | 92.9% | 0.2 |
| SP-month 1 | 100% | 100% | 100% | 100% | NA |
| SP-month 3 | 100% | 100% | 100% | 100% | NA |
| SP-month 6 | 100% | 100% | 100% | 100% | NA |
| Victoria | |||||
| SR | 50% | 66.7% | 69.7% | 66.3% | 0.28 |
| SP-month 0 | 94.4% | 92.9% | 91.1% | 92.3% | 0.85 |
| SP-month 1 | 100% | 100% | 100% | 100% | NA |
| SP-month 3 | 100% | 100% | 100% | 100% | NA |
| SP-month 6 | 100% | 100% | 100% | 100% | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pleros, C.; Adamidis, K.; Kantartzi, K.; Griveas, I.; Baltsavia, I.; Moustakas, A.; Kalliaropoulos, A.; Fraggedaki, E.; Petra, C.; Damianakis, N.; et al. Dialysis Patients Respond Adequately to Influenza Vaccination Irrespective of Dialysis Modality and Chronic Inflammation. J. Clin. Med. 2023, 12, 6205. https://doi.org/10.3390/jcm12196205
Pleros C, Adamidis K, Kantartzi K, Griveas I, Baltsavia I, Moustakas A, Kalliaropoulos A, Fraggedaki E, Petra C, Damianakis N, et al. Dialysis Patients Respond Adequately to Influenza Vaccination Irrespective of Dialysis Modality and Chronic Inflammation. Journal of Clinical Medicine. 2023; 12(19):6205. https://doi.org/10.3390/jcm12196205
Chicago/Turabian StylePleros, Christos, Konstantinos Adamidis, Konstantia Kantartzi, Ioannis Griveas, Ismini Baltsavia, Aristides Moustakas, Antonios Kalliaropoulos, Evaggelia Fraggedaki, Christina Petra, Nikolaos Damianakis, and et al. 2023. "Dialysis Patients Respond Adequately to Influenza Vaccination Irrespective of Dialysis Modality and Chronic Inflammation" Journal of Clinical Medicine 12, no. 19: 6205. https://doi.org/10.3390/jcm12196205
APA StylePleros, C., Adamidis, K., Kantartzi, K., Griveas, I., Baltsavia, I., Moustakas, A., Kalliaropoulos, A., Fraggedaki, E., Petra, C., Damianakis, N., Mentis, A., Drosataki, E., Petrakis, I., Passadakis, P., Panagopoulos, P., Stylianou, K., & Panagoutsos, S. (2023). Dialysis Patients Respond Adequately to Influenza Vaccination Irrespective of Dialysis Modality and Chronic Inflammation. Journal of Clinical Medicine, 12(19), 6205. https://doi.org/10.3390/jcm12196205