
The Triglyceride–Glucose Index Might Be a Better Indicator for Predicting Poor Cardiovascular Outcomes in Chronic Coronary Syndrome
 , , , , , , , , , and
, , , , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
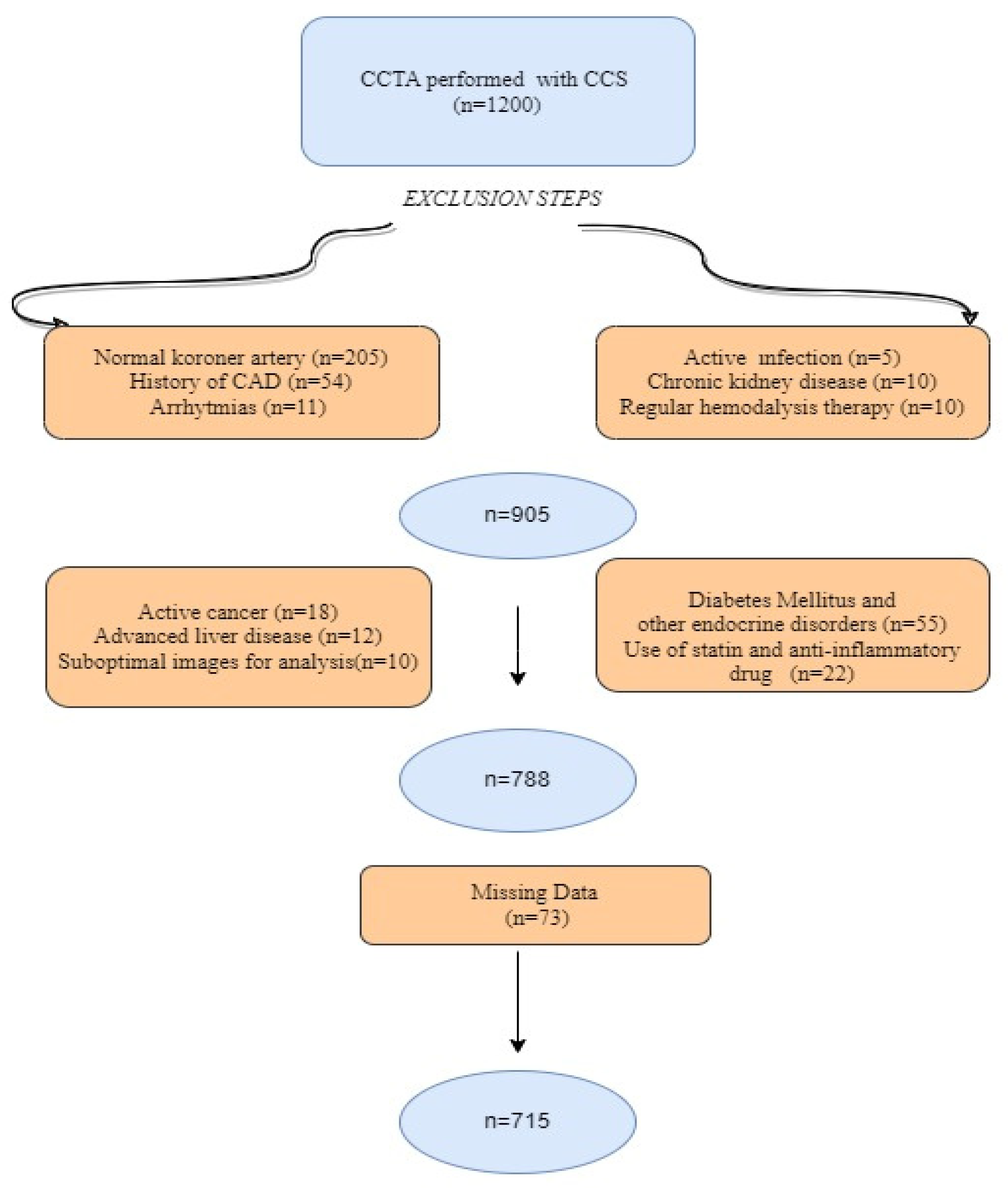
2.1. Study Population
2.2. Definitions and Risk Factors
2.3. CCTA Scan and Data Analysis
2.4. Medical Treatment and Follow-Up
2.5. Outcomes
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
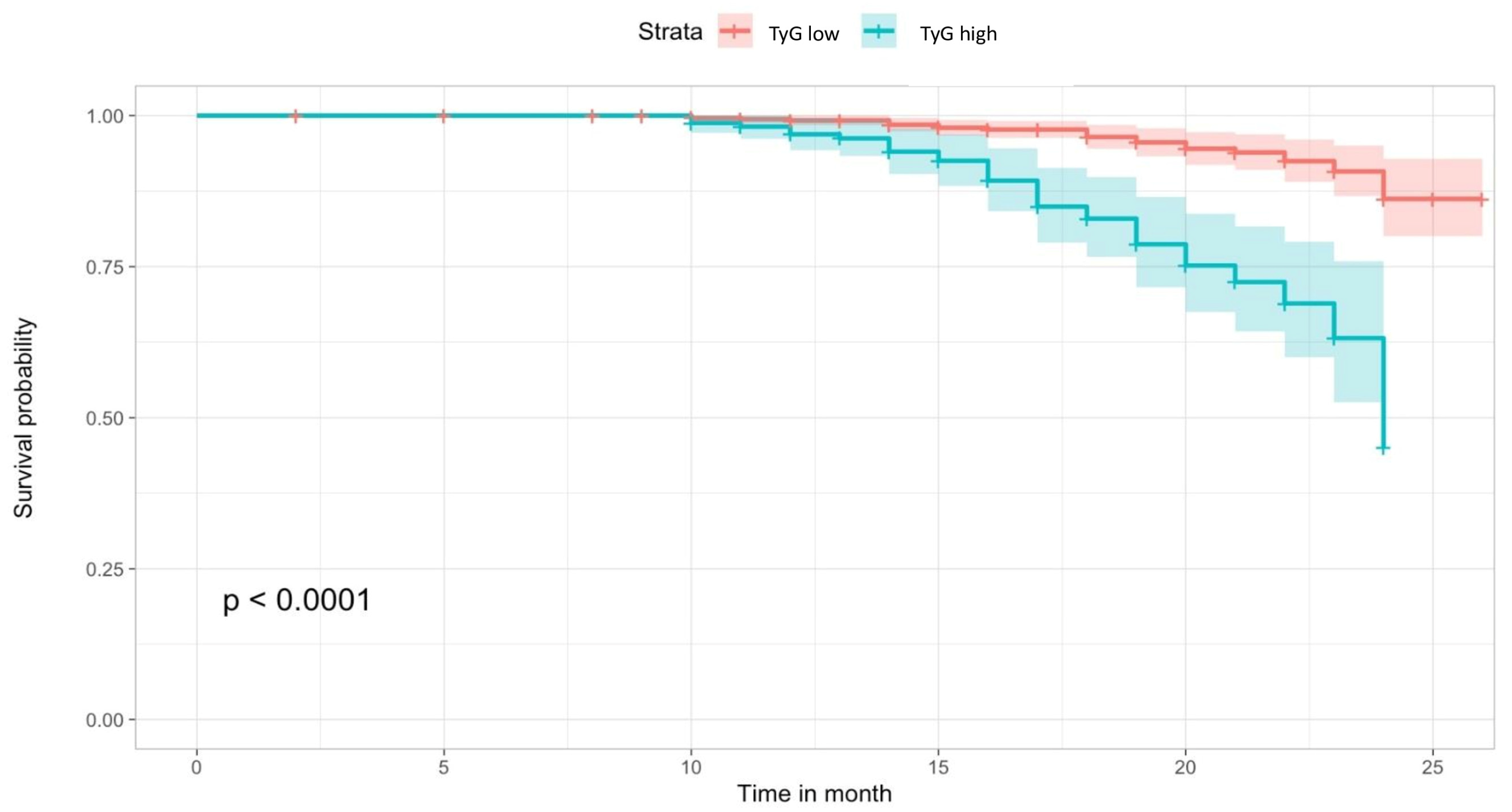
3.2. Primary and Secondary Outcomes
3.3. Independent Predictors of MACEs at Follow-Up
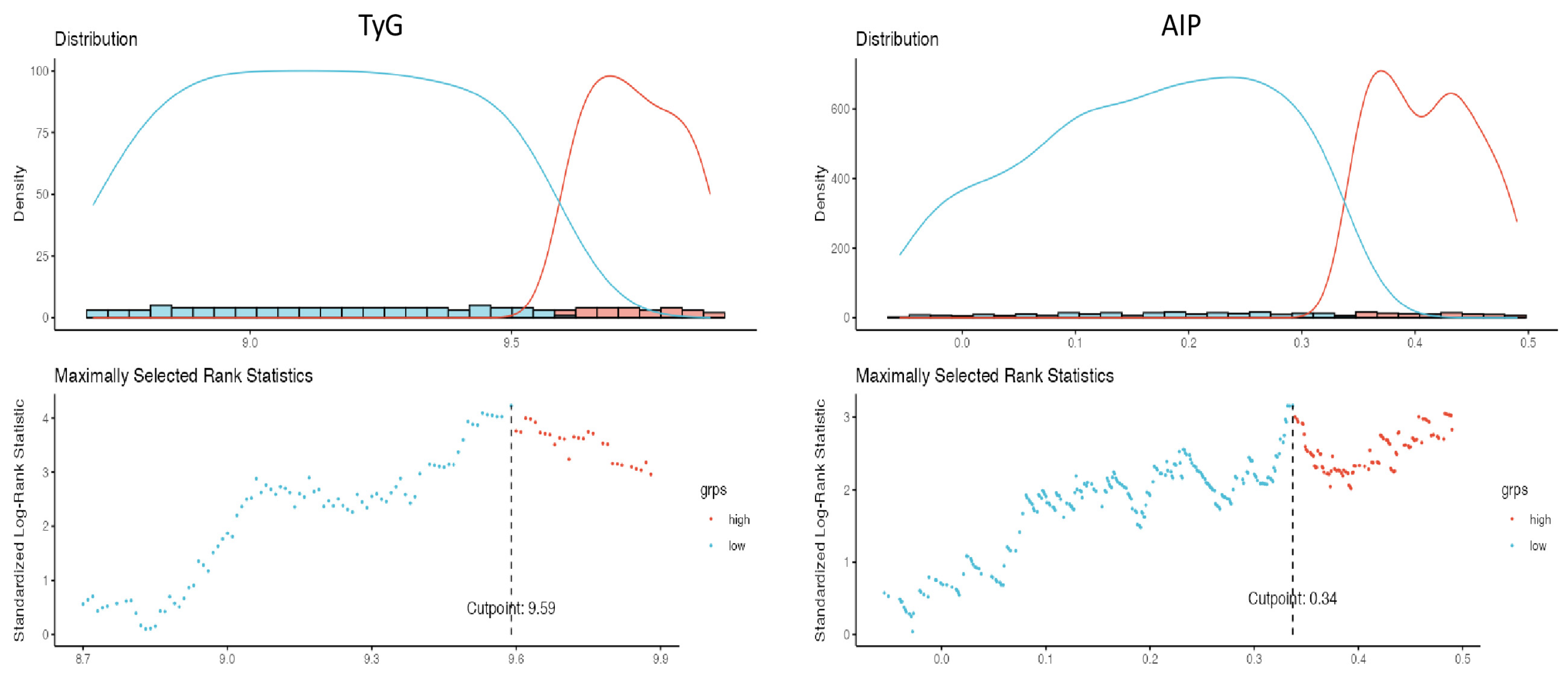
3.4. Diagnostic Performance of TyG and AIP for Cardiovascular Outcomes
4. Discussion
5. Study Limitation
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ford, T.J.; Corcoran, D.; Berry, C. Stable coronary syndromes: Pathophysiology, diagnostic advances and therapeutic need. Heart 2018, 104, 284–292. [Google Scholar] [PubMed]
- Weber, C.; Noels, H. Atherosclerosis: Current pathogenesis and therapeutic options. Nat. Med. 2011, 17, 1410–1422. [Google Scholar] [CrossRef] [PubMed]
- Knuuti, J.; Wijns, W.; Saraste, A.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; Agewall, S.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes: The Task Force for the diagnosis and management of chronic coronary syndromes of the European Society of Cardiology (ESC). Europ. Heart J. 2019, 41, 407–477. [Google Scholar] [CrossRef] [PubMed]
- Sniderman, A.D.; Williams, K.; Contois, J.H.; Monroe, H.M.; McQueen, M.J.; de Graaf, J.; Furberg, C.D. A meta-analysis of low-density lipoprotein cholesterol, non-high-density lipoprotein cholesterol, and apolipoprotein B as markers of cardiovascular risk. Circ. Cardiovasc. Qual. Outcomes 2011, 4, 337–345. [Google Scholar] [CrossRef]
- Rao Kondapally Seshasai, S.; Kaptoge, S.; Thompson, A.; Di Angelantonio, E.; Gao, P.; Sarwar, N.; Whincup, P.H.; Mukamal, K.J.; Gillum, R.F.; Holme, I.; et al. Diabetes mellitus, fasting glucose, and risk of cause-specific death. N. Engl. J. Med. 2011, 364, 829–841. [Google Scholar] [PubMed]
- Moon, S.; Park, J.S.; Ahn, Y. The cut-off values of triglycerides and glucose index for metabolic syndrome in American and Korean adolescents. J. Korean Med. Sci. 2017, 32, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Wang, B.; Liu, Y.; Sun, X.; Luo, X.; Wang, C.; Li, L.; Zhang, L.; Ren, Y.; Zhao, Y.; et al. Cumulative increased risk of incident type 2 diabetes mellitus with increasing triglyceride glucose index in normal-weight people: The Rural Chinese Cohort Study. Cardiovasc. Diabetol. 2017, 16, 30. [Google Scholar] [CrossRef]
- Zhu, X.W.; Deng, F.Y.; Lei, S.F. Meta-analysis of the atherogenic index of plasma and other lipid parameters in relation to risk of type 2 diabetes mellitus. Prim. Care Diabetes 2015, 9, 60–67. [Google Scholar] [CrossRef]
- Niroumand, S.; Khajedaluee, M.; Khadem-Rezaiyan, M.; Abrishami, M.; Juya, M.; Khodaee, G.; Dadgarmoghaddam, M. Atherogenic Index of Plasma (AIP): A marker of cardiovascular disease. Med. J. Islam. Repub. Iran 2015, 29, 240. [Google Scholar]
- Cai, G.; Shi, G.; Xue, S.; Lu, W. The atherogenic index of plasma is a strong and independent predictor for coronary artery disease in the Chinese Han population. Medicine 2017, 96, e8058. [Google Scholar] [CrossRef]
- Yueqiao, S.; Wenjun, F.; Chao, H.; Jingyi, L.; Lixian, S. Atherogenic Index of Plasma, Triglyceride-Glucose Index and Monocyte-to-Lymphocyte Ratio for Predicting Subclinical Coronary Artery Disease. Am. J. Med. Sci. 2021, 362, 285–290. [Google Scholar]
- Mao, Q.; Zhou, D.; Li, Y.; Wang, Y.; Xu, S.C.; Zhao, X.H. The Triglyceride-Glucose Index Predicts Coronary Artery Disease Severity and Cardiovascular Outcomes in Patients with Non-ST-Segment Elevation Acute Coronary Syndrome. Dis. Markers 2019, 2019, e6891537. [Google Scholar] [CrossRef] [PubMed]
- Jin, J.L.; Cao, Y.X.; Wu, L.G.; You, X.-D.; Guo, Y.-L.; Wu, N.-Q.; Zhu, C.-G.; Gao, Y.; Dong, Q.-T.; Hui-Zhang, W.; et al. Triglyceride glucose index for predicting cardiovascular outcomes in patients with coronary artery disease. J. Thorac. Dis. 2011, 11, 6137–6146. [Google Scholar] [CrossRef]
- Hunsicker, L.G.; Adler, S.; Caggiula, A.; Greene, T.; Kusek, J.W.; Rogers, N.L.; Teschan, P.E. Predictors of the progression of renal disease in the Modification of Diet in Renal Disease Study. Kidney Int. 1997, 51, 1908–1919. [Google Scholar] [PubMed]
- Chobanian, A.V.; Bakris, G.L.; Black, H.R.; Cushman, W.C.; Green, L.A.; Izzo, J.L.; Jones, D.W.; Materson, B.J.; Oparil, S.; Wright, J.T.; et al. Treatment of high blood pressure. National high blood pressure education program coordinating c. Seventh report ofthe joint national committee on prevention, detection, e valuation, and treatment of high blood pressure. Hypertension 2003, 42, 1206–1252. [Google Scholar] [CrossRef] [PubMed]
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the national cholesterol education program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef] [PubMed]
- Saremi, F.; Achenbach, S. Coronary plaque characterization using CT. AJR Am. J. Roentgenol. 2015, 204, 249–260. [Google Scholar] [CrossRef] [PubMed]
- Min, J.K.; Shaw, L.J.; Devereux, R.B.; Okin, P.M.; Weinsaft, J.W.; Russo, D.J.; Lippolis, N.J.; Berman, D.S.; Callister, T.Q. Prognostic value of multidetector coronary computed tomographic angiography for prediction of all-cause mortality. J. Am. Coll. Cardiol. 2007, 50, 1161–1170. [Google Scholar] [CrossRef]
- Min, J.K.; Dunning, A.; Lin, F.Y.; Achenbach, S.; Al-Mallah, M.H.; Berman, D.S.; Budoff, M.J.; Cademartiri, F.; Callister, T.Q.; Chang, H.-J.; et al. Rationale and design of the CONFIRM (Coronary CT Angiography Evaluation for Clinical Outcomes: An International Multicenter) Registry. J. Cardiovasc. Comput. Tomogr. 2011, 5, 8492. [Google Scholar] [CrossRef]
- Shen, S.; Lu, Y.; Qi, H.; Li, F.; Shen, Z.; Wu, L.; Yang, C.; Wang, L.; Shui, K.; Wang, Y.; et al. Association between ideal cardiovascular health and the atherogenic index of plasma. Medicine 2016, 95, e3866. [Google Scholar] [CrossRef]
- Dobiásová, M.; Frohlich, J.; Sedová, M.; Cheung, M.C.; Brown, B.G. Cholesterol esterification and atherogenic index of plasma correlate with lipoprotein size and findings on coronary angiography. J. Lipid Res. 2011, 52, 566–571. [Google Scholar] [CrossRef] [PubMed]
- Dobiásová, M.; Frohlich, J. The plasma parameter log (TG/HDL-C) as an atherogenic index: Correlation with lipoprotein particle size and esterification rate in apoB-lipoprotein-depleted plasma (FER(HDL)). Clin. Biochem 2001, 34, 583–588. [Google Scholar] [CrossRef] [PubMed]
- Wu1, T.T.; GAO, Y.; Zheng, Y.Y.; Ma, Y.-T.; Xie, X. Atherogenic index of plasma (AIP): A novel predictive indicator for the coronary artery disease in postmenopausal women. Lipids Health Dis. 2018, 17, 197. [Google Scholar]
- Yildiz, G.; Duman, A.; Aydin, H.; Yilmaz, A.; Hür, E.; Mağden, K.; Cetin, G.; Candan, F. Evaluation of association between atherogenic index of plasma and intima-media thickness of the carotid artery for subclinic atherosclerosis in patients on maintenance hemodialysis. Hemodial. Int. 2013, 17, 397–405. [Google Scholar] [CrossRef] [PubMed]
- Lv, L.; Zhou, Y.; Chen, X.; Gong, L.; Wu, J.; Luo, W.; Shen, Y.; Han, S.; Hu, J.; Wang, Y.; et al. Relationship between the TyG ındex and diabetic kidney disease in patients with type-2 diabetes mellitus. Diabetes Metab. Syndr. Obes. 2021, 14, 3299–3306. [Google Scholar] [CrossRef] [PubMed]
- Vasques, A.C.; Novaes, F.S.; de Oliveira, M.S.; Souza, J.R.M.; Yamanaka, A.; Pareja, J.C.; Tambascia, M.A.; Saad, M.J.A.; Geloneze, B. TyG index performs better than HOMA in a Brazilian population: A hyperglycemic clamp validated study. Diabetes Res. Clin. Pract. 2011, 93, 98–100. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.; Yu, S.; Chi, C.; Fan, X.; Tang, J.; Ji, H.; Teliewubai, J.; Zhang, Y.; Xu, Y. Association between macro- and microvascular damage and the triglyceride glucose index in community-dwelling elderly individuals: The Northern Shanghai Study. Cardiovasc. Diabetol. 2019, 18, 95. [Google Scholar] [CrossRef] [PubMed]
- Mehta, R.H.; Westerhout, C.M.; Zheng, Y.; Giugliano, R.P.; Huber, K.; Prabhakaran, D.; Harrington, R.A.; Newby, K.L.; Armstrong, P.W.; EARLY ACS Investigators. Association of metabolic syndrome and its components with outcomes among patients with high-risk non-ST-segment elevation acute coronary syndromes. Am. Heart J. 2014, 168, 182–188. [Google Scholar] [CrossRef]
- Ormazabal, V.; Nair, S.; Elfeky, O.; Aguayo, C.; Salomon, C.; Zuniga, F.A. Association between insulin resistance and the development of cardiovascular disease. Cardiovasc. Diabetol. 2018, 17, 122. [Google Scholar] [CrossRef]
- Dehghan, M.; Mente, A.; Zhang, X.; Swaminathan, S.; Li, W.; Mohan, V.; Iqbal, R.; Kumar, R.; Wentzel-Viljoen, E.; Rosengren, A.; et al. Associations of fats and carbohydrate intake with cardiovascular disease and mortality in 18 countries from five continents (PURE): A prospective cohort study. Lancet 2017, 390, 2050–2062. [Google Scholar] [CrossRef]
- Tolunay, H.; Fırtına, S. Triglyceride Glucose Index and The Triglyceride/HDL Ratio as Predictors of Coronary Artery Disease. Düzce Ünv. Sağlık Bil. Enst. Der. 2021, 11, 235–241. [Google Scholar]
- Kalyoncuoglu, M.; Ozkan, A.A.; Kaya, A.; Yuksel, Y.; Dogan, N.; Gurmen, A.T. A new predictor of in-stent restenosis in patients undergoing elective percutaneous coronary İntervention: Triglyceride glucose İndex. Int. J. Cardiovasc. Acad. 2021, 7, 50. [Google Scholar] [CrossRef]
- Zhu, Y.; Liu, K.; Chen, M.; Liu, Y.; Gao, A.; Hu, C.; Li, H.; Zhu, H.; Han, H.; Zhang, J.; et al. Triglyceride-glucose index is associated with in-stent restenosis in patients with acute coronary syndrome after percutaneous coronary intervention with drug-eluting stents. Cardiovasc. Diabetol. 2021, 20, 137. [Google Scholar] [CrossRef]
- Luo, E.; Wang, D.; Yan, G.; Qiao, Y.; Liu, B.; Hou, J.; Tang, C. High triglyceride-glucose index is associated with poor prognosis in patients with acute ST-elevation myocardial infarction after percutaneous coronary intervention. Cardiovasc. Diabetol. 2019, 18, 150. [Google Scholar] [CrossRef] [PubMed]
- Chiu, T.H.; Tsai, H.J.; Chiou, H.Y.C.; Wu, P.Y.; Huang, J.C.; Chen, S.C. A high triglyceride-glucose index is associated with left ventricular dysfunction and atherosclerosis. Int. J. Med. Sci. 2021, 18, 1051–1057. [Google Scholar] [CrossRef] [PubMed]
- Bertolone, D.T.; Gallinoro, E.; Esposito, G.; Manabe, S.; Niimi, N.; Gatate, Y.; Sawano, M.; Nakano, S. Contemporary management of stable coronary artery disease. High Blood Press. Cardiovasc. Prev. 2022, 29, 207–219. [Google Scholar] [CrossRef] [PubMed]
- Conte, E.; Mushtaq, S.; Marchetti, D.; Mallia, V.; Belmonte, M.; Melotti, E.; Pontone, G.; Pepi, M.; Andreini, D. Potential application of cardiac computed tomography for early detection of coronary atherosclerosis: From calcium score to advanced atherosclerosis analysis. J. Clin. Med. 2021, 10, 521. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variables | TyG | p-Value * | ||
|---|---|---|---|---|
| Overall | Low | High | ||
| (≤9.59) | (>9.59) | |||
| (n = 715) | (n = 453) | (n = 262) | ||
| Demographic features and risk factors | ||||
| Age; median, (IQR) | 55 (49–62) | 54 (48–61) | 57 (50–65) | <0.001 |
| Male; n (%) | 415 (58) | 252 (55.2) | 163 (62.2) | 0.069 |
| Hypertension; n (%) | 305 (42.6) | 176 (38.8) | 129 (49.2) | 0.012 |
| HL; n (%) | 165 (24.5) | 101 (23.7) | 64 (25.9) | 0.511 |
| Smoking; n (%) | 41 (5.7) | 23 (5.2) | 18 (6.8) | 0.255 |
| Family history of CAD; n (%) | 109 (15.2) | 73 (16.1) | 36 (13.7) | 0.364 |
| BMI | 23.6 (22.7–24.6) | 23.7 (22.5–24.4) | 23.7 (23.0–24.3) | 0.315 |
| Angiographic results, n (%) | ||||
| CAD-RADS (3, 4a, 4b, 5); n (%) | 257 (35.9) | 58 (12.8) | 199 (75.9) | <0.001 |
| Laboratory findings | ||||
| Total cholesterol, mmol/L; Median (IQR) | 4.49 (3.91–5.25) | 4.23 (3.72–4.70) | 5.13 (4.60–5.84) | 0.567 |
| Triglyceride, mmol/L; Median (IQR) | 2.09 (1.62–2.63) | 1.74(1.21–2.10) | 2.77 (2.41–3.44) | <0.001 |
| HDL-C, mmol/L; Median (IQR) | 1.14 (1.02–1.31) | 1.19(1.03–1.31) | 1.12(0.98–1.31) | 0.001 |
| LDL-C, mmol/L; Median (IQR) | 3.03 (2.31–3.60) | 2.5 (2.0–3.4) | 3.2 (2.4–3.7) | <0.001 |
| Creatinine, mg/dL; Median (IQR) | 0.81 (0.72–0.93) | 0.7 (0.6–0.9) | 0.83 (0.74–0.91) | 0.014 |
| e-GFR, mL/min/1.73 m2; Median (IQR) | 92 (85–101) | 93 (87–102) | 91 (82–101) | 0.003 |
| Glucose, mg/dL; Median (IQR) | 114 (102–129) | 108 (96–122) | 125 (114–157) | <0.001 |
| WBC, 103/dL; Median (IQR) | 7.7 (6.6–9.3) | 7.4 (6.5–8.9) | 8.6 (7.0–9.9) | <0.001 |
| Hemoglobin, g/dL; Median (IQR) | 13.7 (12.7–14.8) | 13.9 (12.6–14.9) | 14 (12.9–15.3) | 0.341 |
| Platelet count, 103/dL; Median (IQR) | 260 (231–294) | 253 (225–284) | 275 (251–305) | <0.001 |
| Lymphocyte, cells/µL, Median (IQR) | 2.2 (1.9–2.5) | 2.3 (1.8–2.5) | 2.1 (1.9–2.3) | <0.001 |
| Monocytes, cells/µL; Median (IQR) | 0.61 (0.53–0.75) | 0.6 (0.51–0.72) | 0.65 (0.53–0.81) | 0.003 |
| Neutrophils, cells/µL; Median (IQR) | 4.4 (3.8–5.4) | 4.2 (3.7–4.8) | 5.2 (4.5–6.5) | <0.001 |
| CRP, mg/L; Median (IQR) | 5.4 (4.2–7.9) | 4.9 (3.9–6.1) | 7.6 (5.5–9.3) | <0.001 |
| Albumin, g/dl; Median (IQR) | 4.6 (4.4–4.7) | 4.4 (4.4–4.7) | 4.6 (4.5–4.7) | 0.003 |
| Medications prescribed at discharge, n (%) | ||||
| Antiplatelets, n (%) | 545 (76.2) | 340 (75.0) | 205 (78.2) | 0.901 |
| B-blockers, n (%) | 350 (48.9) | 218 (48.1) | 132 (50.3) | 0.801 |
| ACEIs or ARBs | 210 (29.3) | 125 (27.5) | 85 (32.4) | 0.855 |
| OAD, n (%) | 183 (25.5) | 119 (26.2) | 64 (24.4) | 0.948 |
| Antihyperlipidemic, n (%) | 165 (23.0) | 104 (22.9) | 61 (23.2) | 0.645 |
| Statins, n (%) | 155 (21.6) | 98 (21.6) | 57 (21.7) | 0.763 |
| Fenofibrate, n (%) | 10 (1.3) | 6 (1.3) | 4 (1.5) | 0.851 |
| TyG | ||||
|---|---|---|---|---|
| Overall | Low Group | High Group | p-Value * | |
| (≤9.59) | (>9.59) | |||
| The primary outcome, n (%) | ||||
| MACE | 66 (9.2) | 17 (3.8) | 49 (18.7) | <0.001 |
| Secondary outcomes, n (%) | ||||
| Cerebrovascular events | 10 (1.4) | 3 (0.7) | 7 (2.7) | <0.001 |
| Hospitalization for heart failure | 13 (1.8) | 4 (0.9) | 9 (3.4) | 0.003 |
| Non-fatal MI | 17 (2.4) | 3 (0.7) | 14 (5.3) | <0.001 |
| Non-cardiac Mortality | 11 (1.5) | 2 (0.4) | 9 (3.4) | <0.001 |
| Cardiac Mortality | 15 (2.1) | 5 (1.1) | 10 (3.8) | 0.002 |
| Unadjusted | |||
|---|---|---|---|
| Variable | HR | 95% CI | p-Value * |
| Age | 1.03 | 1.02–1.07 | <0.001 |
| Gender (male reference) | 0.63 | 0.44–1.01 | 0.056 |
| Hypertension | 2.29 | 1.47–3.35 | <0.001 |
| Hyperlipidemia | 1.46 | 1.12–2.35 | 0.021 |
| Hemoglobin | 0.89 | 0.81–0.97 | 0.119 |
| Creatinine, mg/dL | 0.96 | 0.41–3.75 | 0.934 |
| CRP; mg/dL | 1.03 | 1.01–1.12 | <0.001 |
| Family history of CAD | 1.10 | 0.67–1.87 | 0.599 |
| Smoking | 1.15 | 0.81–1.57 | 0.311 |
| LDL-C, mmol/L | 0.89 | 0.71–1.09 | 0.337 |
| HDL-C, mmol/L | 0.66 | 0.53–0.72 | 0.289 |
| OAD, n (%) | 0.74 | 0.61–0.91 | 0.323 |
| Antihyperlipidemic, n (%) | 0.91 | 0.72–0.99 | 0.453 |
| BMI | 1.01 | 0.90–1.27 | 0.396 |
| CAD-RADS (3, 4a, 4b, 5) | 4.74 | 3.35–7.45 | <0.001 |
| TyG index | 4.29 | 3.11–6.79 | <0.001 |
| AIP | 3.42 | 3.00–5.68 | <0.001 |
| Adjusted Model 1 | Adjusted Model 2 | |||||
|---|---|---|---|---|---|---|
| Variable | HR | 95% CI | p-Value | HR | 95% CI | p-Value * |
| Age | 1.05 | 1.01–1.09 | <0.001 | 1.04 | 1.02–1.06 | <0.001 |
| Hypertension | 1.03 | 1.02–3.58 | 0.041 | 1.46 | 1.00–2.41 | 0.045 |
| Hyperlipidemia | 1.07 | 0.79–2.41 | 0.286 | 1.32 | 0.78–1.97 | 0.374 |
| CRP; mg/dL | 1.06 | 0.93–1.09 | 0.121 | 1.09 | 0.87–1.21 | 0.261 |
| CAD-RADS (3, 4a, 4b, 5) | 2.87 | 1.75–5.11 | <0.001 | 2.73 | 1.57–4.85 | 0.002 |
| AIP | 2.79 | 0.873–7.8 | 0.091 | - | - | - |
| TyG index | - | - | - | 2.11 | 1.55–3.12 | 0.003 |
| Likelihood Ratio X2 | Nagelkerke’s Adjusted R2 | Akaike Information Criteria | Harrel’s C-Index (Model AUC) | |
|---|---|---|---|---|
| TyG | 23.07 | 0.412 | 422 | 0.688 |
| AIP | 14.32 | 0.332 | 435 | 0.660 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Erdoğan, A.; İnan, D.; Genç, Ö.; Yıldız, U.; Demirtola, A.İ.; Çetin, İ.; Güler, Y.; Tekin, A.F.; Barutçu, S.; Güler, A.; et al. The Triglyceride–Glucose Index Might Be a Better Indicator for Predicting Poor Cardiovascular Outcomes in Chronic Coronary Syndrome. J. Clin. Med. 2023, 12, 6201. https://doi.org/10.3390/jcm12196201
Erdoğan A, İnan D, Genç Ö, Yıldız U, Demirtola Aİ, Çetin İ, Güler Y, Tekin AF, Barutçu S, Güler A, et al. The Triglyceride–Glucose Index Might Be a Better Indicator for Predicting Poor Cardiovascular Outcomes in Chronic Coronary Syndrome. Journal of Clinical Medicine. 2023; 12(19):6201. https://doi.org/10.3390/jcm12196201
Chicago/Turabian StyleErdoğan, Aslan, Duygu İnan, Ömer Genç, Ufuk Yıldız, Ayşe İrem Demirtola, İlyas Çetin, Yeliz Güler, Ali Fuat Tekin, Süleyman Barutçu, Ahmet Güler, and et al. 2023. "The Triglyceride–Glucose Index Might Be a Better Indicator for Predicting Poor Cardiovascular Outcomes in Chronic Coronary Syndrome" Journal of Clinical Medicine 12, no. 19: 6201. https://doi.org/10.3390/jcm12196201
APA StyleErdoğan, A., İnan, D., Genç, Ö., Yıldız, U., Demirtola, A. İ., Çetin, İ., Güler, Y., Tekin, A. F., Barutçu, S., Güler, A., & Karagöz, A. (2023). The Triglyceride–Glucose Index Might Be a Better Indicator for Predicting Poor Cardiovascular Outcomes in Chronic Coronary Syndrome. Journal of Clinical Medicine, 12(19), 6201. https://doi.org/10.3390/jcm12196201