Diagnostic Puzzles and Cause-Targeted Treatment Strategies in Myocardial Infarction with Non-Obstructive Coronary Arteries: An Updated Review



 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Pathophysiologic Mechanisms
2.1. Plaque Disruption
- Transient vessel occlusion may occur at the rupture site before intrinsic thrombolysis. Spontaneous thrombolysis or autolysis of a coronary thrombosis has been proposed as an explanation for the absence of sub-occlusive or occlusive thrombi during coronary angiography in MINOCA, especially when the procedure is performed late, and antithrombotic and antiplatelet agents are promptly administered [9];
- Distal embolization of the thrombus, with or without angiographically evident small-vessel occlusion, is another possibility;
- Flush occlusion of the ostium of a side branch may also occur without apparent signs in invasive angiography.
2.2. Epicardial Coronary Vasospasm
2.3. Coronary Microvascular Dysfunction
2.4. Spontaneous Coronary Artery Dissection
2.5. Coronary Artery Embolism
3. MINOCA Mimics
3.1. Takotsubo Syndrome
3.2. Myocarditis
3.3. Pulmonary Embolism
3.4. Thrombophilia
- Factor V Leiden: present in 12% of the cases;
- Protein C or S deficiency: identified in 3% of the patients;
- Factor XII deficiency: observed in 3% of the cases [36].
- Antiphospholipid syndrome: identified in 15.5% of the patients;
- Inherited thrombophilia: found in 23.8% of the cases [74].
3.5. Oxygen Supply/Demand Imbalance Myocardial Infarction
4. Diagnostic Tools in MINOCA
4.1. Angiographic Re-Appraisal, Clinical Evaluation and Laboratory Testing
4.2. Echocardiography
4.3. Cardiac Ventriculography
4.4. Intracoronary Imaging
4.5. Invasive Functional Coronary Tests
4.6. Cardiac Magnetic Resonance
4.7. Coronary Computed Tomography Angiography
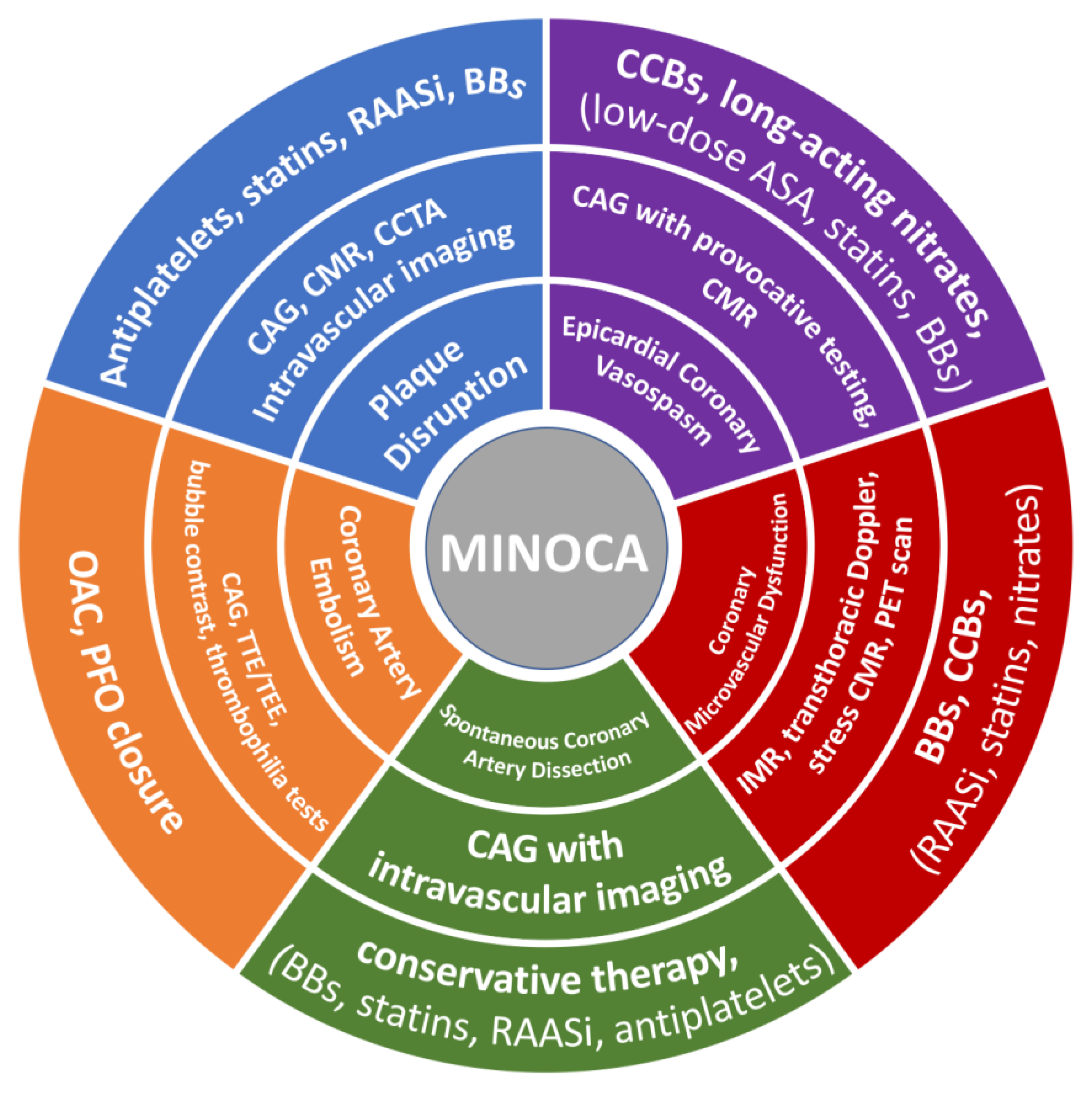
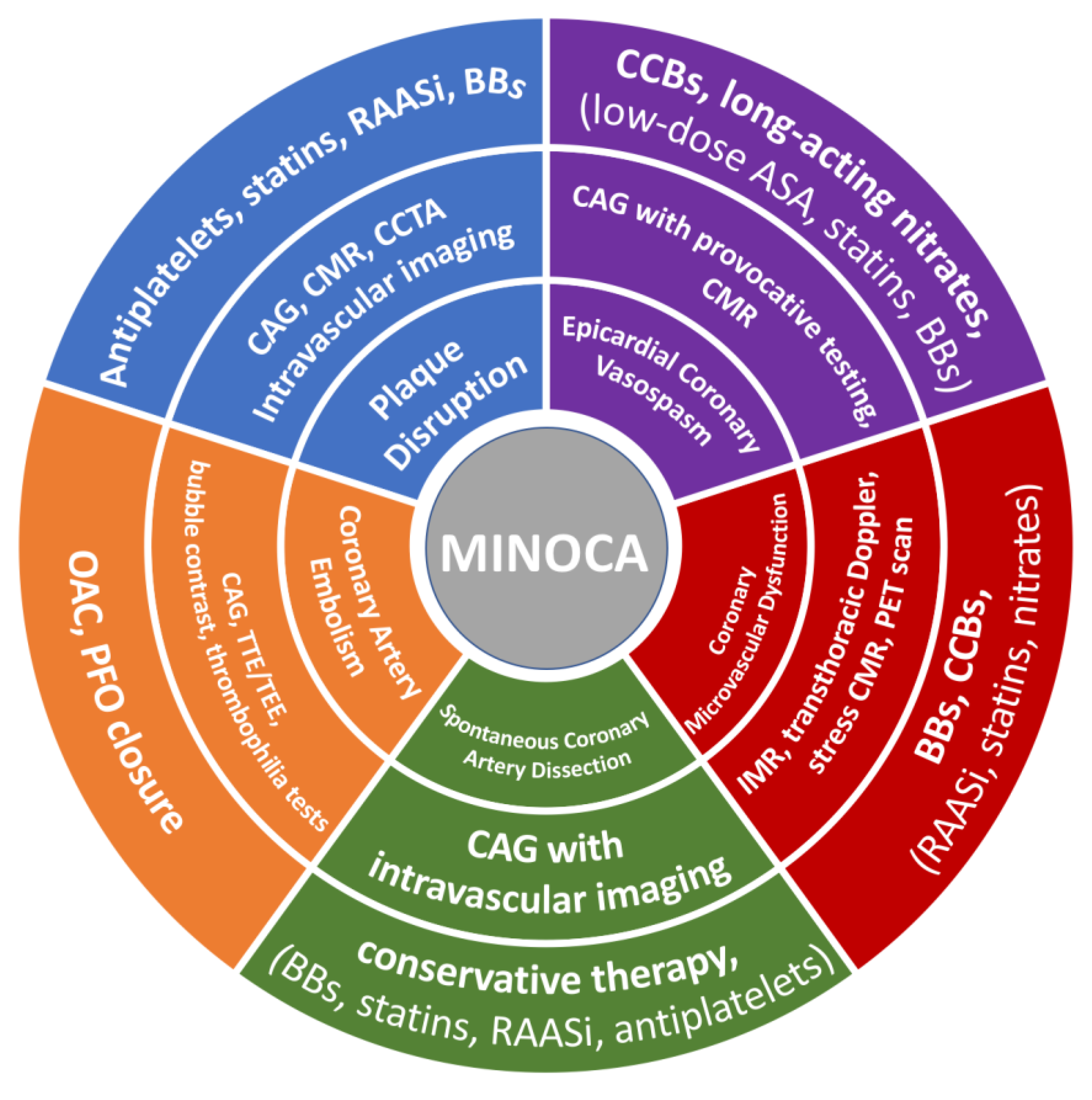
5. Cause-Targeted Treatment
5.1. The General Approach to Management in Patients with MINOCA
5.2. Plaque Disruption
5.3. Epicardial Coronary Vasospasm
5.4. Coronary Microvascular Dysfunction
5.5. Spontaneous Coronary Artery Dissection
5.6. Coronary Artery Embolism
6. Prognosis in MINOCA
6.1. MINOCA vs. Other Populations (MI-CAD, Angina, General Population)
6.2. Underutilization of Secondary Prevention Medication in MINOCA
7. Future Implications
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rallidis, L.S.; Xenogiannis, I.; Brilakis, E.S.; Bhatt, D.L. Causes, Angiographic Characteristics, and Management of Premature Myocardial Infarction: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2022, 79, 2431–2449. [Google Scholar] [CrossRef]
- Agewall, S.; Beltrame, J.F.; Reynolds, H.R.; Niessner, A.; Rosano, G.; Caforio, A.L.; De Caterina, R.; Zimarino, M.; Roffi, M.; Kjeldsen, K.; et al. ESC working group position paper on myocardial infarction with non-obstructive coronary arteries. Eur. Heart J. 2017, 38, 143–153. [Google Scholar] [CrossRef]
- Tamis-Holland, J.E.; Jneid, H.; Reynolds, H.R.; Agewall, S.; Brilakis, E.S.; Brown, T.M.; Lerman, A.; Cushman, M.; Kumbhani, D.J.; Arslanian-Engoren, C.; et al. Contemporary Diagnosis and Management of Patients with Myocardial Infarction in the Absence of Obstructive Coronary Artery Disease: A Scientific Statement from the American Heart Association. Circulation 2019, 139, E891–E908. [Google Scholar] [CrossRef]
- Merlo, A.C.; Troccolo, A.; Piredda, E.; Porto, I.; Gil Ad, V. Myocardial Infarction With Non-obstructive Coronary Arteries: Risk Factors and Associated Comorbidities. Front. Cardiovasc. Med. 2022, 9, 895053. [Google Scholar] [CrossRef]
- Scalone, G.; Niccoli, G.; Crea, F. Editor’s Choice—Pathophysiology, diagnosis and management of MINOCA: An update. Eur Heart J. Acute Cardiovasc. Care 2019, 8, 54–62. [Google Scholar] [CrossRef]
- Pasupathy, S.; Air, T.; Dreyer, R.P.; Tavella, R.; Beltrame, J.F. Response to Letter Regarding Article, “Systematic Review of Patients Presenting With Suspected Myocardial Infarction and Nonobstructive Coronary Arteries”. Circulation 2015, 132, e232. [Google Scholar] [CrossRef]
- Niccoli, G.; Camici, P.G. Myocardial infarction with non-obstructive coronary arteries: What is the prognosis? Eur. Heart J. Suppl. J. Eur. Soc. Cardiol. 2020, 22 (Suppl. E), E40–E45. [Google Scholar] [CrossRef]
- Iqbal, S.N.; Feit, F.; Mancini, G.J.; Wood, D.; Patel, R.; Pena-Sing, I.; Attubato, M.; Yatskar, L.; Slater, J.N.; Hochman, J.S.; et al. Characteristics of plaque disruption by intravascular ultrasound in women presenting with myocardial infarction without obstructive coronary artery disease. Am. Heart J. 2014, 167, 715–722. [Google Scholar] [CrossRef]
- Montone, R.A.; Niccoli, G.; Fracassi, F.; Russo, M.; Gurgoglione, F.; Cammà, G.; Lanza, G.A.; Crea, F. Patients with acute myocardial infarction and non-obstructive coronary arteries: Safety and prognostic relevance of invasive coronary provocative tests. Eur. Heart J. 2018, 39, 91–98. [Google Scholar] [CrossRef]
- Choo, E.H.; Chang, K.; Lee, K.Y.; Lee, D.; Kim, J.G.; Ahn, Y.; Kim, Y.J.; Chae, S.C.; Cho, M.C.; Kim, C.J.; et al. Prognosis and Predictors of Mortality in Patients Suffering Myocardial Infarction with Non-Obstructive Coronary Arteries. J. Am. Heart Assoc. 2019, 8, e011990. [Google Scholar] [CrossRef]
- Chong, J.H.; Baumbach, A.; Khanji, M.Y. A Middle-aged Woman with Recurrent Chest Pain with Troponin Elevation and Unobstructed Coronary Arteries. JAMA Cardiol. 2021, 6, 600–601. [Google Scholar] [CrossRef]
- Lindahl, B.; Baron, T.; Albertucci, M.; Prati, F. Myocardial infarction with non-obstructive coronary artery disease. EuroIntervention 2021, 17, E875–E887. [Google Scholar] [CrossRef]
- Manfrini, O.; Morrell, C.; Das, R.; Barth, J.H.; Hall, A.S.; Gale, C.P.; Cenko, E.; Bugiardini, R. Effects of angiotensin-converting enzyme inhibitors and beta blockers on clinical outcomes in patients with and without coronary artery obstructions at angiography (from a Register-Based Cohort Study on Acute Coronary Syndromes). Am. J. Cardiol. 2014, 113, 1628–1633. [Google Scholar] [CrossRef]
- Ciliberti, G.; Coiro, S.; Tritto, I.; Benedetti, M.; Guerra, F.; Del Pinto, M.; Finocchiaro, G.; Cavallini, C.; Capucci, A.; Kaski, J.C.; et al. Predictors of poor clinical outcomes in patients with acute myocardial infarction and non-obstructed coronary arteries (MINOCA). Int. J. Cardiol. 2018, 267, 41–45. [Google Scholar] [CrossRef]
- Amsterdam, E.A.; Wenger, N.K.; Brindis, R.G.; Casey, D.E., Jr.; Ganiats, T.G.; Holmes, D.R., Jr.; Jaffe, A.S.; Jneid, H.; Kelly, R.F.; Kontos, M.C.; et al. 2014 AHA/ACC Guideline for the Management of Patients with Non-ST-Elevation Acute Coronary Syndromes: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2014, 64, e139–e228. [Google Scholar] [CrossRef]
- Serpytis, R.; Majauskiene, E.; Navickas, P.; Lizaitis, M.; Glaveckaite, S.; Rucinskas, K.; Petrulioniene, Z.; Valeviciene, N.; Samalavicius, R.S.; Berukstis, A.; et al. Randomized Pilot Trial on Optimal Treatment Strategy, Myocardial Changes, and Prognosis of Patients with Myocardial Infarction with Nonobstructive Coronary Arteries (MINOCA). Am. J. Med. 2022, 135, 103–109. [Google Scholar] [CrossRef]
- Pasupathy, S.; Tavella, R.; Beltrame, J.F. Myocardial Infarction with Nonobstructive Coronary Arteries (MINOCA): The Past, Present, and Future Management. Circulation 2017, 135, 1490–1493. [Google Scholar] [CrossRef]
- Mukherjee, D. Myocardial Infarction with Nonobstructive Coronary Arteries: A Call for Individualized Treatment. J. Am. Heart Assoc. 2019, 8, e013361. [Google Scholar] [CrossRef]
- Smilowitz, N.R.; Mahajan, A.M.; Roe, M.T.; Hellkamp, A.S.; Chiswell, K.; Gulati, M.; Reynolds, H.R. Mortality of Myocardial Infarction by Sex, Age, and Obstructive Coronary Artery Disease Status in the ACTION Registry-GWTG (Acute Coronary Treatment and Intervention Outcomes Network Registry-Get with the Guidelines). Circ. Cardiovasc. Qual. Outcomes 2017, 10, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef] [PubMed]
- Byrne, R.A.; Rossello, X.; Coughlan, J.J.; Barbato, E.; Berry, C.; Chieffo, A.; Claeys, M.J.; Dan, G.A.; Dweck, M.R.; Galbraith, M.; et al. 2023 ESC Guidelines for the management of acute coronary syndromes: Developed by the task force on the management of acute coronary syndromes of the European Society of Cardiology (ESC). Eur Heart J. 2023, ehad191. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, H.R.; Srichai, M.B.; Iqbal, S.N.; Slater, J.N.; Mancini, G.B.; Feit, F.; Pena-Sing, I.; Axel, L.; Attubato, M.J.; Yatskar, L.; et al. Mechanisms of myocardial infarction in women without angiographically obstructive coronary artery disease. Circulation 2011, 124, 1414–1425. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, H.R.; Maehara, A.; Kwong, R.Y.; Sedlak, T.; Saw, J.; Smilowitz, N.R.; Mahmud, E.; Wei, J.; Marzo, K.; Matsumura, M.; et al. Coronary Optical Coherence Tomography and Cardiac Magnetic Resonance Imaging to Determine Underlying Causes of Myocardial Infarction with Nonobstructive Coronary Arteries in Women. Circulation 2021, 143, 624–640. [Google Scholar] [CrossRef] [PubMed]
- Gerbaud, E.; Arabucki, F.; Nivet, H.; Barbey, C.; Cetran, L.; Chassaing, S.; Seguy, B.; Lesimple, A.; Cochet, H.; Montaudon, M.; et al. OCT and CMR for the Diagnosis of Patients Presenting with MINOCA and Suspected Epicardial Causes. JACC Cardiovasc. Imaging 2020, 13, 2619–2631. [Google Scholar] [CrossRef]
- Opolski, M.P. Mechanisms of myocardial infarction with nonobstructive coronary atherosclerosis: A multifaceted play of different actors with guarded prognosis. Curr. Opin. Cardiol. 2020, 35, 697–704. [Google Scholar] [CrossRef]
- Taruya, A.; Tanaka, A.; Nishiguchi, T.; Ozaki, Y.; Kashiwagi, M.; Yamano, T.; Matsuo, Y.; Ino, Y.; Kitabata, H.; Takemoto, K.; et al. Lesion characteristics and prognosis of acute coronary syndrome without angiographically significant coronary artery stenosis. Eur. Heart J. Cardiovasc. Imaging. 2020, 21, 202–209. [Google Scholar] [CrossRef]
- Crea, F.; Liuzzo, G. Pathogenesis of acute coronary syndromes. J. Am. Coll. Cardiol. 2013, 61, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Virmani, R.; Kolodgie, F.D.; Burke, A.P.; Farb, A.; Schwartz, S.M. Lessons from sudden coronary death: A comprehensive morphological classification scheme for atherosclerotic lesions. Arterioscler. Thromb. Vasc. Biol. 2000, 20, 1262–1275. [Google Scholar] [CrossRef]
- Kolodgie, F.D.; Burke, A.P.; Farb, A.; Weber, D.K.; Kutys, R.; Wight, T.N.; Virmani, R. Differential accumulation of proteoglycans and hyaluronan in culprit lesions: Insights into plaque erosion. Arterioscler. Thromb. Vasc. Biol. 2002, 22, 1642–1648. [Google Scholar] [CrossRef]
- Ambrose, J.A.; Tannenbaum, M.A.; Alexopoulos, D.; Hjemdahl-Monsen, C.E.; Leavy, J.; Weiss, M.; Borrico, S.; Gorlin, R.; Fuster, V. Angiographic progression of coronary artery disease and the development of myocardial infarction. J. Am. Coll. Cardiol. 1988, 12, 56–62. [Google Scholar] [CrossRef]
- Beltrame, J.F.; Crea, F.; Kaski, J.C.; Ogawa, H.; Ong, P.; Sechtem, U.; Shimokawa, H.; Bairey Merz, C.N. International standardization of diagnostic criteria for vasospastic angina. Eur. Heart J. 2017, 38, 2565–2568. [Google Scholar] [CrossRef] [PubMed]
- Seitz, A.; Martínez Pereyra, V.; Sechtem, U.; Ong, P. Update on coronary artery spasm 2022—A narrative review. Int. J. Cardiol. 2022, 359, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Marrone, A.; Pavasini, R.; Scollo, E.; Gibiino, F.; Pompei, G.; Caglioni, S.; Biscaglia, S.; Campo, G.; Tebaldi, M. Acetylcholine Use in Modern Cardiac Catheterization Laboratories: A Systematic Review. J. Clin. Med. 2022, 11, 1129. [Google Scholar] [CrossRef]
- Kaski, J.C. Provocative tests for coronary artery spasm in MINOCA: Necessary and safe? Eur. Heart J. 2018, 39, 99–101. [Google Scholar] [CrossRef] [PubMed]
- Ong, P.; Athanasiadis, A.; Borgulya, G.; Vokshi, I.; Bastiaenen, R.; Kubik, S.; Hill, S.; Schäufele, T.; Mahrholdt, H.; Kaski, J.C.; et al. Clinical usefulness, angiographic characteristics, and safety evaluation of intracoronary acetylcholine provocation testing among 921 consecutive white patients with unobstructed coronary arteries. Circulation 2014, 129, 1723–1730. [Google Scholar] [CrossRef]
- Pasupathy, S.; Air, T.; Dreyer, R.P.; Tavella, R.; Beltrame, J.F. Systematic review of patients presenting with suspected myocardial infarction and nonobstructive coronary arteries. Circulation 2015, 131, 861–870. [Google Scholar] [CrossRef]
- Godo, S.; Suda, A.; Takahashi, J.; Yasuda, S.; Shimokawa, H. Coronary Microvascular Dysfunction. Arterioscler. Thromb. Vasc. Biol. 2021, 41, 1625–1637. [Google Scholar] [CrossRef]
- Ong, P.; Camici, P.G.; Beltrame, J.F.; Crea, F.; Shimokawa, H.; Sechtem, U.; Kaski, J.C.; Bairey Merz, C.N. International standardization of diagnostic criteria for microvascular angina. Int. J. Cardiol. 2018, 250, 16–20. [Google Scholar] [CrossRef]
- Nishi, T.; Kume, T.; Yamada, R.; Okamoto, H.; Koto, S.; Yamashita, M.; Ueno, M.; Kamisaka, K.; Sasahira, Y.; Enzan, A.; et al. Layered Plaque in Organic Lesions in Patients with Coronary Artery Spasm. J. Am. Heart Assoc. 2022, 11, e024880. [Google Scholar] [CrossRef]
- Montone, R.A.; Rinaldi, R.; Del Buono, M.G.; Gurgoglione, F.; La Vecchia, G.; Russo, M.; Caffè, A.; Burzotta, F.; Leone, A.M.; Romagnoli, E.; et al. Safety and prognostic relevance of acetylcholine testing in patients with stable myocardial ischaemia or myocardial infarction and non-obstructive coronary arteries. EuroIntervention 2022, 18, e666–e676. [Google Scholar] [CrossRef]
- Noel Bairey Merz, C.; Pepine, C.J.; Walsh, M.N.; Fleg, J.L. Ischemia and No Obstructive Coronary Artery Disease (INOCA): Developing Evidence-Based Therapies and Research Agenda for the Next Decade. Circulation 2017, 135, 1075–1092. [Google Scholar] [CrossRef]
- Beltrame, J.F.; Limaye, S.B.; Horowitz, J.D. The coronary slow flow phenomenon—A new coronary microvascular disorder. Cardiology 2002, 97, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Fearon, W.F.; Farouque, H.M.O.; Balsam, L.B.; Caffarelli, A.D.; Cooke, D.T.; Robbins, R.C.; Fitzgerald, P.J.; Yeung, A.C.; Yock, P.G. Comparison of coronary thermodilution and Doppler velocity for assessing coronary flow reserve. Circulation 2003, 108, 2198–2200. [Google Scholar] [CrossRef] [PubMed]
- Kaski, J.-C.; Crea, F.; Gersh, B.J.; Camici, P.G. Reappraisal of Ischemic Heart Disease. Circulation 2018, 138, 1463–1480. [Google Scholar] [CrossRef] [PubMed]
- Camici, P.G.; Crea, F. Coronary Microvascular Dysfunction. N. Engl. J. Med. 2007, 356, 830–840. [Google Scholar] [CrossRef]
- Camici, P.G.; Tschöpe, C.; Di Carli, M.F.; Rimoldi, O.; Van Linthout, S. Coronary microvascular dysfunction in hypertrophy and heart failure. Cardiovasc. Res. 2020, 116, 806–816. [Google Scholar] [CrossRef]
- Chan, N.; Premawardhana, D.; Al-Hussaini, A.; Wood, A.; Bountziouka, V.; Kotecha, D.; Swahn, E.; Palmefors, H.; Pagonis, C.; Lawesson, S.S.; et al. Pregnancy and Spontaneous Coronary Artery Dissection: Lessons from Survivors and Nonsurvivors. Circulation 2022, 146, 69–72. [Google Scholar] [CrossRef]
- Saw, J. Coronary angiogram classification of spontaneous coronary artery dissection. Catheter. Cardiovasc. Interv. Off. J. Soc. Card. Angiogr. Interv. 2014, 84, 1115–1122. [Google Scholar] [CrossRef]
- Saw, J.; Humphries, K.; Aymong, E.; Sedlak, T.; Prakash, R.; Starovoytov, A.; Mancini, G.B.J. Spontaneous Coronary Artery Dissection: Clinical Outcomes and Risk of Recurrence. J. Am. Coll. Cardiol. 2017, 70, 1148–1158. [Google Scholar] [CrossRef]
- Boulmpou, A.; Kassimis, G.; Zioutas, D.; Meletidou, M.; Mouselimis, D.; Tsarouchas, A.; Tzikas, S.; Vassilikos, V.; Kanonidis, I.; Tsounos, I.; et al. Spontaneous Coronary Artery Dissection (SCAD): Case Series and Mini Review. Cardiovasc. Revasc. Med. 2020, 21, 1450–1456. [Google Scholar] [CrossRef]
- Saw, J.; Mancini, G.B.J.; Humphries, K.H. Contemporary Review on Spontaneous Coronary Artery Dissection. J. Am. Coll. Cardiol. 2016, 68, 297–312. [Google Scholar] [CrossRef] [PubMed]
- Gu, W.; Zhou, J.; Peng, Y.; Cai, H.; Wang, H.; Wan, W.; Li, H.; Xu, C.; Chen, L. Prognostic Significance of Serum Chloride Level Reduction in Patients with Chronic Heart Failure with Different Ejection Fractions. Int. Heart J. 2023, 64, 700–707. [Google Scholar] [CrossRef] [PubMed]
- Saw, J.; Starovoytov, A.; Humphries, K.; Sheth, T.; So, D.; Minhas, K.; Brass, N.; Lavoie, A.; Bishop, H.; Lavi, S.; et al. Canadian spontaneous coronary artery dissection cohort study: In-hospital and 30-day outcomes. Eur. Heart J. 2019, 40, 1188–1197. [Google Scholar] [CrossRef] [PubMed]
- Hayes, S.N.; Kim, E.S.; Saw, J.; Adlam, D.; Arslanian-Engoren, C.; Economy, K.E.; Ganesh, S.K.; Gulati, R.; Lindsay, M.E.; Mieres, J.H.; et al. Spontaneous Coronary Artery Dissection: Current State of the Science: A Scientific Statement from the American Heart Association. Circulation 2018, 137, e523–e557. [Google Scholar] [CrossRef] [PubMed]
- Maehara, A.; Mintz, G.S.; Castagna, M.T.; Pichard, A.D.; Satler, L.F.; Waksman, R.; Suddath, W.O.; Kent, K.M.; Weissman, N.J. Intravascular ultrasound assessment of spontaneous coronary artery dissection. Am. J. Cardiol. 2002, 89, 466–468. [Google Scholar] [CrossRef]
- Tweet, M.S.; Hayes, S.N.; Pitta, S.R.; Simari, R.D.; Lerman, A.; Lennon, R.J.; Gersh, B.J.; Khambatta, S.; Best, P.J.; Rihal, C.S.; et al. Clinical features, management, and prognosis of spontaneous coronary artery dissection. Circulation 2012, 126, 579–588. [Google Scholar] [CrossRef]
- Clare, R.; Duan, L.; Phan, D.; Simari, R.D.; Lerman, A.; Lennon, R.J.; Gersh, B.J.; Khambatta, S.; Best, P.J.; Rihal, C.S.; et al. Characteristics and Clinical Outcomes of Patients with Spontaneous Coronary Artery Dissection. J. Am. Heart Assoc. 2019, 8, e012570. [Google Scholar] [CrossRef]
- Eleid, M.F.; Guddeti, R.R.; Tweet, M.S.; Lerman, A.; Singh, M.; Best, P.J.; Vrtiska, T.J.; Prasad, M.; Rihal, C.S.; Hayes, S.N.; et al. Coronary artery tortuosity in spontaneous coronary artery dissection: Angiographic characteristics and clinical implications. Circ. Cardiovasc. Interv. 2014, 7, 656–662. [Google Scholar] [CrossRef]
- Liang, K.; Williams, M.; Bucciarelli-Ducci, C. Cardiac magnetic resonance imaging unmasks presumed embolic myocardial infarction due to patent foramen ovale case report. Eur. Heart J. Case Rep. 2022, 6, ytac029. [Google Scholar] [CrossRef]
- Kent, D.M.; Ruthazer, R.; Weimar, C.; Mas, J.L.; Serena, J.; Homma, S.; Di Angelantonio, E.; Di Tullio, M.R.; Lutz, J.S.; Elkind, M.S.; et al. An index to identify stroke-related vs incidental patent foramen ovale in cryptogenic stroke. Neurology 2013, 81, 619–625. [Google Scholar] [CrossRef]
- Lacey, M.J.; Raza, S.; Rehman, H.; Puri, R.; Bhatt, D.L.; Kalra, A. Coronary Embolism: A Systematic Review. Cardiovasc. Revasc. Med. 2020, 21, 367–374. [Google Scholar] [CrossRef] [PubMed]
- Kardasz, I.; De Caterina, R. Myocardial infarction with normal coronary arteries: A conundrum with multiple aetiologies and variable prognosis: An update. J. Intern. Med. 2007, 261, 330–348. [Google Scholar] [CrossRef] [PubMed]
- Waksman, R.; Ghazzal, Z.M.; Baim, D.S.; Steenkiste, A.R.; Yeh, W.; Detre, K.M.; King, S.B. Myocardial infarction as a complication of new interventional devices. Am. J. Cardiol. 1996, 78, 751–756. [Google Scholar] [CrossRef] [PubMed]
- Khawaja, M.Z.; Sohal, M.; Valli, H.; Dworakowski, R.; Pettit, S.J.; Roy, D.; Newton, J.; Schneider, H.; Manoharan, G.; Doshi, S.; et al. Standalone balloon aortic valvuloplasty: Indications and outcomes from the UK in the transcatheter valve era. Catheter. Cardiovasc. Interv. Off. J. Soc. Card. Angiogr. Interv. 2013, 81, 366–373. [Google Scholar] [CrossRef] [PubMed]
- Chikkabasavaiah, N.; Rajendran, R.; Beeresha, P.; Ramesh, B. Percutaneous Coronary Intervention for Coronary Thrombo-embolism during Balloon Mitral Valvuloplasty in a Pregnant Woman. Heart Lung Circ. 2016, 25, e29–e31. [Google Scholar] [CrossRef]
- Ribeiro, H.B.; Nombela-Franco, L.; Urena, M.; Mok, M.; Pasian, S.; Doyle, D.; DeLarochellière, R.; Côté, M.; Laflamme, L.; DeLarochellière, H.; et al. Coronary obstruction following transcatheter aortic valve implantation: A systematic review. JACC Cardiovasc. Interv. 2013, 6, 452–461. [Google Scholar] [CrossRef]
- Ghadri, J.-R.; Wittstein, I.S.; Prasad, A.; Sharkey, S.; Dote, K.; Akashi, Y.J.; Cammann, V.L.; Crea, F.; Galiuto, L.; Desmet, W.; et al. International Expert Consensus Document on Takotsubo Syndrome (Part I): Clinical Characteristics, Diagnostic Criteria, and Pathophysiology. Eur. Heart J. 2018, 39, 2032–2046. [Google Scholar] [CrossRef]
- Sherrid, M.V.; Swistel, D.G.; Olivotto, I.; Pieroni, M.; Wever-Pinzon, O.; Riedy, K.; Bach, R.G.; Husaini, M.; Cresci, S.; Reyentovich, A.; et al. Syndrome of Reversible Cardiogenic Shock and Left Ventricular Ballooning in Obstructive Hypertrophic Cardiomyopathy. J. Am. Heart Assoc. 2021, 10, e021141. [Google Scholar] [CrossRef]
- Hausvater, A.; Smilowitz, N.R.; Saw, J.; Sherrid, M.; Ali, T.; Espinosa, D.; Mersha, R.; DeFonte, M.; Reynolds, H.R. Spontaneous Coronary Artery Dissection in Patients with a Provisional Diagnosis of Takotsubo Syndrome. J. Am. Heart Assoc. 2019, 8, e013581. [Google Scholar] [CrossRef]
- Chou, A.Y.; Sedlak, T.; Aymong, E.; Sheth, T.; Starovoytov, A.; Humphries, K.H.; Mancini, G.B.; Saw, J. Spontaneous Coronary Artery Dissection Misdiagnosed as Takotsubo Cardiomyopathy: A Case Series. Can. J. Cardiol. 2015, 31, 1073.e5–1073.e8. [Google Scholar] [CrossRef]
- Kato, K.; Lyon, A.R.; Ghadri, J.-R.; Templin, C. Takotsubo syndrome: Aetiology, presentation and treatment. Heart 2017, 103, 1461–1469. [Google Scholar] [CrossRef] [PubMed]
- Hausvater, A.; Pasupathy, S.; Tornvall, P.; Gandhi, H.; Tavella, R.; Beltrame, J.; Agewall, S.; Ekenbäck, C.; Brolin, E.B.; Hochman, J.S.; et al. ST-segment elevation and cardiac magnetic resonance imaging findings in myocardial infarction with non-obstructive coronary arteries. Int. J. Cardiol. 2019, 287, 128–131. [Google Scholar] [CrossRef] [PubMed]
- Collste, O.; Sörensson, P.; Frick, M.; Agewall, S.; Daniel, M.; Henareh, L.; Ekenbäck, C.; Eurenius, L.; Guiron, C.; Jernberg, T.; et al. Myocardial infarction with normal coronary arteries is common and associated with normal findings on cardiovascular magnetic resonance imaging: Results from the Stockholm Myocardial Infarction with Normal Coronaries study. J. Intern. Med. 2013, 273, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Stepien, K.; Nowak, K.; Wypasek, E.; Zalewski, J.; Undas, A. High prevalence of inherited thrombophilia and antiphospholipid syndrome in myocardial infarction with non-obstructive coronary arteries: Comparison with cryptogenic stroke. Int. J. Cardiol. 2019, 290, 1–6. [Google Scholar] [CrossRef] [PubMed]
- López-Cuenca, A.; Gómez-Molina, M.; Flores-Blanco, P.J.; Sánchez-Martínez, M.; García-Narbon, A.; De Las Heras-Gómez, I.; Sánchez-Galian, M.J.; Guerrero-Pérez, E.; Valdés, M.; Manzano-Fernández, S.; et al. Comparison between type-2 and type-1 myocardial infarction: Clinical features, treatment strategies and outcomes. J. Geriatr. Cardiol. 2016, 13, 15–22. [Google Scholar] [CrossRef]
- Baron, T.; Hambraeus, K.; Sundström, J.; Erlinge, D.; Jernberg, T.; Lindahl, B. Type 2 myocardial infarction in clinical practice. Heart 2015, 101, 101–106. [Google Scholar] [CrossRef]
- Reynolds, H.R.; Smilowitz, N.R. Myocardial Infarction with Nonobstructive Coronary Arteries. Annu. Rev. Med. 2023, 74, 171–188. [Google Scholar] [CrossRef]
- Herling de Oliveira, L.L.; Correia, V.M.; Nicz, P.F.G.; Soares, P.R.; Scudeler, T.L. MINOCA: One Size Fits All? Probably Not-A Review of Etiology, Investigation, and Treatment. J. Clin. Med. 2022, 11, 5497. [Google Scholar] [CrossRef]
- Tamis-Holland, J.E.; Jneid, H. Myocardial infarction with nonobstructive coronary arteries (MINOCA): It’s time to face reality! J. Am. Heart Assoc. 2018, 7, e009635. [Google Scholar] [CrossRef]
- Occhipinti, G.; Bucciarelli-Ducci, C.; Capodanno, D. Diagnostic pathways in myocardial infarction with non-obstructive coronary artery disease (MINOCA). Eur. Heart J. Acute Cardiovasc. Care 2021, 10, 813–822. [Google Scholar] [CrossRef]
- Foà, A.; Canton, L.; Bodega, F.; Bergamaschi, L.; Paolisso, P.; De Vita, A.; Villano, A.; Mattioli, A.V.; Tritto, I.; Morrone, D.; et al. Myocardial infarction with nonobstructive coronary arteries: From pathophysiology to therapeutic strategies. J. Cardiovasc. Med. 2023, 24 (Suppl. S2), e134–e146. [Google Scholar] [CrossRef] [PubMed]
- Chaulin, A.M. On the Effect of Heterophilic Antibodies on Serum Levels of Cardiac Troponins: A Brief Descriptive Review. Life 2022, 12, 1114. [Google Scholar] [CrossRef] [PubMed]
- Barrett, T.J.; Lee, A.H.; Smilowitz, N.R.; Hausvater, A.; Fishman, G.I.; Hochman, J.S.; Reynolds, H.R.; Berger, J.S. Whole-Blood Transcriptome Profiling Identifies Women with Myocardial Infarction with Nonobstructive Coronary Artery Disease. Circ. Genomic. Precis. Med. 2018, 11, e002387. [Google Scholar] [CrossRef]
- Gudenkauf, B.; Hays, A.G.; Tamis-Holland, J.; Trost, J.; Ambinder, D.I.; Wu, K.C.; Arbab-Zadeh, A.; Blumenthal, R.S.; Sharma, G. Role of Multimodality Imaging in the Assessment of Myocardial Infarction with Nonobstructive Coronary Arteries: Beyond Conventional Coronary Angiography. J. Am. Heart Assoc. 2022, 11, e022787. [Google Scholar] [CrossRef] [PubMed]
- Citro, R.; Okura, H.; Ghadri, J.R.; Izumi, C.; Meimoun, P.; Izumo, M.; Dawson, D.; Kaji, S.; Eitel, I.; Kagiyama, N.; et al. Multimodality imaging in takotsubo syndrome: A joint consensus document of the European Association of Cardiovascular Imaging (EACVI) and the Japanese Society of Echocardiography (JSE). J. Echocardiogr. 2020, 18, 199–224. [Google Scholar] [CrossRef]
- Hurst, R.T.; Prasad, A.; Askew, J.W., 3rd; Sengupta, P.P.; Tajik, A.J. Takotsubo cardiomyopathy: A unique cardiomyopathy with variable ventricular morphology. JACC Cardiovasc. Imaging 2010, 3, 641–649. [Google Scholar] [CrossRef]
- Kubo, T.; Imanishi, T.; Takarada, S.; Kuroi, A.; Ueno, S.; Yamano, T.; Tanimoto, T.; Matsuo, Y.; Masho, T.; Kitabata, H.; et al. Assessment of culprit lesion morphology in acute myocardial infarction: Ability of optical coherence tomography compared with intravascular ultrasound and coronary angioscopy. J. Am. Coll. Cardiol. 2007, 50, 933–939. [Google Scholar] [CrossRef]
- Di Vito, L.; Prati, F.; Arbustini, E.; Crea, F.; Maseri, A. A “stable” coronary plaque rupture documented by repeated OCT studies. JACC Cardiovasc. Imaging 2013, 6, 835–836. [Google Scholar] [CrossRef]
- Ciliberti, G.; Seshasai, S.R.K.; Ambrosio, G.; Kaski, J.C. Safety of intracoronary provocative testing for the diagnosis of coronary artery spasm. Int. J. Cardiol. 2017, 244, 77–83. [Google Scholar] [CrossRef]
- Eitel, I.; Behrendt, F.; Schindler, K.; Kivelitz, D.; Gutberlet, M.; Schuler, G.; Thiele, H. Differential diagnosis of suspected apical ballooning syndrome using contrast-enhanced magnetic resonance imaging. Eur. Heart J. 2008, 29, 2651–2659. [Google Scholar] [CrossRef]
- Lurz, P.; Luecke, C.; Eitel, I.; Föhrenbach, F.; Frank, C.; Grothoff, M.; de Waha, S.; Rommel, K.P.; Lurz, J.A.; Klingel, K.; et al. Comprehensive Cardiac Magnetic Resonance Imaging in Patients with Suspected Myocarditis: The MyoRacer-Trial. J. Am. Coll. Cardiol. 2016, 67, 1800–1811. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, V.M.; Schulz-Menger, J.; Holmvang, G.; Kramer, C.M.; Carbone, I.; Sechtem, U.; Kindermann, I.; Gutberlet, M.; Cooper, L.T.; Liu, P.; et al. Cardiovascular Magnetic Resonance in Nonischemic Myocardial Inflammation: Expert Recommendations. J. Am. Coll. Cardiol. 2018, 72, 3158–3176. [Google Scholar] [CrossRef] [PubMed]
- Saberio, L.P.; Eck, B.L.; Reza, R.; Nguyen, C.; Tang, W.H.W.; Flamm, S.D.; Seiberlich, N.; Lima da Cruz, G.; Prieto, C.; Kwon, D.H.; et al. Fingerprinting MINOCA. JACC Case Rep. 2023, 7, 101722. [Google Scholar] [CrossRef]
- Poon, M.; Lesser, J.R.; Biga, C.; Blankstein, R.; Kramer, C.M.; Min, J.K.; Noack, P.S.; Farrow, C.; Hoffman, U.; Murillo, J.; et al. Current Evidence and Recommendations for Coronary CTA First in Evaluation of Stable Coronary Artery Disease. J. Am. Coll. Cardiol. 2020, 76, 1358–1362. [Google Scholar] [CrossRef]
- Abdelrahman, K.M.; Chen, M.Y.; Dey, A.K.; Blankstein, R.; Kramer, C.M.; Min, J.K.; Noack, P.S.; Farrow, C.; Hoffman, U.; Murillo, J.; et al. Coronary Computed Tomography Angiography From Clinical Uses to Emerging Technologies: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2020, 76, 1226–1243. [Google Scholar] [CrossRef]
- Gonzalez, J.A.; Lipinski, M.J.; Flors, L.; Shaw, P.W.; Kramer, C.M.; Salerno, M. Meta-Analysis of Diagnostic Performance of Coronary Computed Tomography Angiography, Computed Tomography Perfusion, and Computed Tomography-Fractional Flow Reserve in Functional Myocardial Ischemia Assessment Versus Invasive Fractional Flow Reserve. Am. J. Cardiol. 2015, 116, 1469–1478. [Google Scholar] [CrossRef]
- Oikonomou, E.K.; Marwan, M.; Desai, M.Y.; Mancio, J.; Alashi, A.; Hutt Centeno, E.; Thomas, S.; Herdman, L.; Kotanidis, C.P.; Thomas, K.E.; et al. Non-invasive detection of coronary inflammation using computed tomography and prediction of residual cardiovascular risk (the CRISP CT study): A post-hoc analysis of prospective outcome data. Lancet 2018, 392, 929–939. [Google Scholar] [CrossRef]
- Nakanishi, R.; Alani, A.; Matsumoto, S.; Li, D.; Fahmy, M.; Abraham, J.; Dailing, C.; Broersen, A.; Kitslaar, P.H.; Nasir, K.; et al. Changes in Coronary Plaque Volume: Comparison of Serial Measurements on Intravascular Ultrasound and Coronary Computed Tomographic Angiography. Tex. Heart Inst. J. 2018, 45, 84–91. [Google Scholar] [CrossRef]
- Villines, T.C.; Rodriguez Lozano, P. Transitioning From Stenosis to Plaque Burden in the Cardiac CT Era: The Changing Risk Paradigm. J. Am. Coll. Cardiol. 2020, 76, 2814–2816. [Google Scholar] [CrossRef]
- von Knebel Doeberitz, P.L.; De Cecco, C.N.; Schoepf, U.J.; Schoepf, U.J.; Duguay, T.M.; Albrecht, M.H.; van Assen, M.; Bauer, M.J.; Savage, R.H.; Pannell, J.T.; et al. Coronary CT angiography-derived plaque quantification with artificial intelligence CT fractional flow reserve for the identification of lesion-specific ischemia. Eur. Radiol. 2019, 29, 2378–2387. [Google Scholar] [CrossRef]
- Rampidis, G.P. The Role of Cardiac Computed Tomography in the Diagnostic Evaluation and Risk Stratification of Patients with Myocardial Infarction and Non-Obstructive Coronary Arteries (MINOCA): Rationale and Design of the MINOCA-GR Study. BMJ Open 2022, 12, e054698. [Google Scholar] [CrossRef] [PubMed]
- Gaibazzi, N.; Martini, C.; Botti, A.; Pinazzi, A.; Bottazzi, B.; Palumbo, A.A. Coronary Inflammation by Computed Tomography Pericoronary Fat Attenuation in MINOCA and Tako-Tsubo Syndrome. J. Am. Heart Assoc. 2019, 8, e013235. [Google Scholar] [CrossRef]
- Linde, J.J.; Kelbæk, H.; Hansen, T.F.; Sigvardsen, P.E.; Torp-Pedersen, C.; Bech, J.; Heitmann, M.; Nielsen, O.W.; Høfsten, D.; Kühl, J.T.; et al. Coronary CT Angiography in Patients with Non-ST-Segment Elevation Acute Coronary Syndrome. J. Am. Coll. Cardiol. 2020, 75, 453–463. [Google Scholar] [CrossRef] [PubMed]
- Tweet, M.S.; Gulati, R.; Williamson, E.E.; Vrtiska, T.J.; Hayes, S.N. Multimodality Imaging for Spontaneous Coronary Artery Dissection in Women. JACC Cardiovasc. Imaging 2016, 9, 436–450. [Google Scholar] [CrossRef]
- Scholtz, J.-E.; Addison, D.; Bittner, D.O.; Janjua, S.; Foldyna, B.; Hedgire, S.; Staziaki, P.V.; Januzzi, J.L., Jr.; Nagurney, J.T. Diagnostic Performance of Coronary CTA in Intermediate-to-High-Risk Patients for Suspected Acute Coronary Syndrome: Results From an Emergency Department Registry. JACC Cardiovasc. Imaging 2018, 11, 1369–1371. [Google Scholar] [CrossRef]
- Amsterdam, E.A.; Wenger, N.K.; Brindis, R.G.; Casey, D.E., Jr.; Ganiats, T.G.; Holmes, D.R., Jr.; Jaffe, A.S.; Jneid, H.; Kelly, R.F.; Kontos, M.C.; et al. 2014 AHA/ACC Guideline for the Management of Patients with Non-St-Elevation Acute Coronary Syndromes: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014, 130, e344–e426. [Google Scholar] [CrossRef] [PubMed]
- Smilowitz, N.R.; Dubner, R.; Hellkamp, A.S.; Widmer, R.J.; Reynolds, H.R. Variability of discharge medical therapy for secondary prevention among patients with myocardial infarction with non-obstructive coronary arteries (MINOCA) in the United States. PLoS ONE 2021, 16, e0255462. [Google Scholar] [CrossRef]
- Maddox, T.M.; Ho, P.M.; Roe, M.; Dai, D.; Tsai, T.T.; Rumsfeld, J.S. Utilization of secondary prevention therapies in patients with nonobstructive coronary artery disease identified during cardiac catheterization: Insights from the National Cardiovascular Data Registry Cath-PCI Registry. Circ. Cardiovasc. Qual. Outcomes 2010, 3, 632–641. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D. Fourth Universal Definition of Myocardial Infarction (2018). Circulation 2018, 138, e618–e651. [Google Scholar] [CrossRef]
- O’Gara, P.T.; Kushner, F.G.; Ascheim, D.D.; Casey, D.E., Jr.; Chung, M.K.; de Lemos, J.A.; Ettinger, S.M.; Fang, J.C.; Fesmire, F.M.; Franklin, B.A.; et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: A report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation 2013, 127, 362–425. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, S.; Zhao, F.; Mehta, S.R.; Chrolavicius, S.; Tognoni, G.; Fox, K.K. Effects of Clopidogrel in Addition to Aspirin in Patients with Acute Coronary Syndromes without St-Segment Elevation. N. Engl. J. Med. 2001, 345, 494–502. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Jiang, L. Addition of clopidogrel to aspirin in 45 852 patients with acute myocardial infarction: Randomised placebo-controlled trial. Lancet 2005, 366, 1607–1621. [Google Scholar] [CrossRef] [PubMed]
- Roffi, M.; Patrono, C.; Collet, J.-P.; Mueller, C.; Valgimigli, M.; Andreotti, F.; Bax, J.J.; Borger, M.A.; Brotons, C.; Chew, D.P.; et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2016, 37, 267–315. [Google Scholar] [CrossRef]
- Prati, F.; Uemura, S.; Souteyrand, G.; Virmani, R.; Motreff, P.; Di Vito, L.; Biondi-Zoccai, G.; Halperin, J.; Fuster, V.; Ozaki, Y.; et al. OCT-based diagnosis and management of STEMI associated with intact fibrous cap. JACC Cardiovasc. Imaging 2013, 6, 283–287. [Google Scholar] [CrossRef]
- Gould, K.L.; Johnson, N.P.; Bateman, T.M.; Beanlands, R.S.; Bengel, F.M.; Bober, R.; Camici, P.G.; Cerqueira, M.D.; Chow, B.J.W.; Di Carli, M.F.; et al. Anatomic versus physiologic assessment of coronary artery disease. Role of coronary flow reserve, fractional flow reserve, and positron emission tomography imaging in revascularization decision-making. J. Am. Coll. Cardiol. 2013, 62, 1639–1653. [Google Scholar] [CrossRef]
- Johnson, T.W.; Räber, L.; di Mario, C.; Bourantas, C.; Jia, H.; Mattesini, A.; Gonzalo, N.; de la Torre Hernandez, J.M.; Prati, F.; Koskinas, Κ.; et al. Clinical use of intracoronary imaging. Part 2: Acute coronary syndromes, ambiguous coronary angiography findings, and guiding interventional decision-making: An expert consensus document of the European Association of Percutaneous Cardiovascular Interven. Eur. Heart J. 2019, 40, 2566–2584. [Google Scholar] [CrossRef]
- Samaras, A.; Papazoglou, A.S.; Balomenakis, C.; Bekiaridou, A.; Moysidis, D.V.; Rampidis, G.P.; Kampaktsis, P.N.; Apostolidou-Kiouti, F.; Haidich, A.B.; Kassimis, G.; et al. Prognostic impact of secondary prevention medical therapy following myocardial infarction with non-obstructive coronary arteries: A Bayesian and frequentist meta-analysis. Eur. Heart J. Open 2022, 2, oeac077. [Google Scholar] [CrossRef]
- De Filippo, O.; Russo, C.; Manai, R.; Borzillo, I.; Savoca, F.; Gallone, G.; Bruno, F.; Ahmad, M.; De Ferrari, G.M.; D’Ascenzo, F.; et al. Impact of secondary prevention medical therapies on outcomes of patients suffering from Myocardial Infarction with NonObstructive Coronary Artery disease (MINOCA): A meta-analysis. Int. J. Cardiol. 2022, 368, 1–9. [Google Scholar] [CrossRef]
- Lindahl, B.; Baron, T.; Erlinge, D.; Hadziosmanovic, N.; Nordenskjöld, A.; Gard, A.; Jernberg, T. Medical Therapy for Secondary Prevention and Long-Term Outcome in Patients with Myocardial Infarction with Nonobstructive Coronary Artery Disease. Circulation 2017, 135, 1481–1489. [Google Scholar] [CrossRef]
- Paolisso, P.; Bergamaschi, L.; Saturi, G.; D’Angelo, E.C.; Magnani, I.; Toniolo, S.; Stefanizzi, A.; Rinaldi, A.; Bartoli, L.; Angeli, F.; et al. Secondary prevention medical therapy and outcomes in patients with myocardial infarction with non-obstructive coronary artery disease. Front. Pharmacol. 2020, 10, 1606. [Google Scholar] [CrossRef] [PubMed]
- Grassi, G.; Seravalle, G.; Mancia, G. Sympathetic activation in cardiovascular disease: Evidence, clinical impact and therapeutic implications. Eur. J. Clin. Investig. 2015, 45, 1367–1375. [Google Scholar] [CrossRef] [PubMed]
- Abdu, F.A.; Liu, L.; Mohammed, A.Q.; Luo, Y.; Xu, S.; Auckle, R.; Xu, Y.; Che, W. Myocardial infarction with non-obstructive coronary arteries (MINOCA)in Chinese patients: Clinical features, treatment and 1 year follow-up. Int. J. Cardiol. 2019, 287, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Ciliberti, G.; Verdoia, M.; Merlo, M.; Zilio, F.; Vatrano, M.; Bianco, F.; Mancone, M.; Zaffalon, D.; Bonci, A.; Boscutti, A.; et al. Pharmacological therapy for the prevention of cardiovascular events in patients with myocardial infarction with non-obstructed coronary arteries (MINOCA): Insights from a multicentre national registry. Int. J. Cardiol. 2021, 327, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, S.; Sleight, P.; Pogue, J.; Bosch, J.; Davies, R.; Dagenais, G. Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. N. Engl. J. Med. 2000, 342, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Abdu, F.A.; Liu, L.; Mohammed, A.-Q.; Xu, B.; Yin, G.; Xu, S.; Xu, Y.; Che, W. Effect of Secondary Prevention Medication on the Prognosis in Patients with Myocardial Infarction with Nonobstructive Coronary Artery Disease. J. Cardiovasc. Pharmacol. 2020, 76, 678–683. [Google Scholar] [CrossRef]
- Hara, H.; Nakamura, M.; Yokouchi, I.; Kimura, K.; Nemoto, N.; Ito, S.; Ono, T.; Itaya, H.; Shiba, M.; Wada, M. Aggressive statin therapy in multicenter and effectiveness for the reduction of intra-myocardial damage caused by non-ST elevation acute coronary syndrome: AMERICA study. Ther. Adv. Cardiovasc. Dis. 2009, 3, 357–365. [Google Scholar] [CrossRef]
- Kereiakes, D.J. Adjunctive pharmacotherapy before percutaneous coronary intervention in non-ST-elevation acute coronary syndromes: The role of modulating inflammation. Circulation 2003, 108 (Suppl. S1), III-22–III-27. [Google Scholar] [CrossRef]
- Cheema, A.N.; Yanagawa, B.; Verma, S.; Bagai, A.; Liu, S. Myocardial infarction with nonobstructive coronary artery disease (MINOCA): A review of pathophysiology and management. Curr. Opin. Cardiol. 2021, 36, 589–596. [Google Scholar] [CrossRef]
- Song, J.K. Coronary Artery Vasospasm. Korean Circ. J. 2018, 48, 767–777. [Google Scholar] [CrossRef]
- Chahine, R.A.; Feldman, R.L.; Giles, T.D.; Nicod, P.; Raizner, A.E.; Weiss, R.J.; Vanov, S.K. Randomized placebo-controlled trial of amlodipine in vasospastic angina. J. Am. Coll. Cardiol. 1993, 21, 1365–1370. [Google Scholar] [CrossRef] [PubMed]
- Yasue, H.; Takizawa, A.; Nagao, M.; Nishida, S.; Horie, M.; Kubota, J.; Omote, S.; Takaoka, K.; Okumura, K. Long-term prognosis for patients with variant angina and influential factors. Circulation 1988, 78, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Beltrame, J.F.; Crea, F.; Kaski, J.C.; Ogawa, H.; Ong, P.; Sechtem, U.; Shimokawa, H.; Bairey Merz, C.N. The who, what, why, when, how and where of vasospastic angina. Circ. J. 2016, 80, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, A.; Taruya, A.; Shibata, K.; Fuse, K.; Katayama, Y.; Yokoyama, M.; Kashiwagi, M.; Shingo, O.; Akasaka, T.; Kato, N.; et al. Coronary artery lumen complexity as a new marker for refractory symptoms in patients with vasospastic angina. Sci. Rep. 2021, 11, 13. [Google Scholar] [CrossRef]
- Miyamoto, S.; Ogawa, H.; Soejima, H.; Takazoe, K.; Kajiwara, I.; Shimomura, H.; Sakamoto, T.; Yoshimura, M.; Kugiyama, K.; Yasue, H.; et al. Enhanced platelet aggregation in the coronary circulation after coronary spasm. Thromb. Res. 2001, 103, 377–386. [Google Scholar] [CrossRef]
- Beltrame, J.F.; Crea, F.; Camici, P. Advances in coronary microvascular dysfunction. Heart Lung Circ. 2009, 18, 19–27. [Google Scholar] [CrossRef]
- Lanza, G.A.; Sestito, A.; Sgueglia, G.A.; Infusino, F.; Manolfi, M.; Crea, F.; Maseri, A. Current clinical features, diagnostic assessment and prognostic determinants of patients with variant angina. Int. J. Cardiol. 2007, 118, 41–47. [Google Scholar] [CrossRef]
- Lanza, G.A.; Colonna, G.; Pasceri, V.; Maseri, A. Atenolol versus amlodipine versus isosorbide-5-mononitrate on anginal symptoms in syndrome X. Am. J. Cardiol. 1999, 84, 854–856. [Google Scholar] [CrossRef]
- Masumoto, A.; Mohri, M.; Takeshita, A. Three-year follow-up of the Japanese patients with microvascular angina attributable to coronary microvascular spasm. Int. J. Cardiol. 2001, 81, 151–156. [Google Scholar] [CrossRef]
- Kilic, S.; Aydın, G.; Çoner, A.; Doğan, Y.; Arican Özlük, Ö.; Çelik, Y.; Ungan, I.; Tascanov, M.B.; Düz, R.; Polat, V.; et al. Prevalence and clinical profile of patients with myocardial infarction with non-obstructive coronary arteries in Turkey (MINOCA-TR): A national multi-center, observational study. Anatol. J. Cardiol. 2020, 23, 176–182. [Google Scholar] [CrossRef]
- Lerman, A.; Burnett, J.C., Jr.; Higano, S.T.; McKinley, L.J.; Holmes, D.R., Jr. Long-term L-arginine supplementation improves small-vessel coronary endothelial function in humans. Circulation 1998, 97, 2123–2128. [Google Scholar] [CrossRef] [PubMed]
- Saha, S.; Ete, T.; Kapoor, M.; Jha, P.K.; Megeji, R.D.; Kavi, G.; Warjri, S.B.; Mishra, A. Effect of Ranolazine in Patients with Chest Pain and Normal Coronaries—A Hospital Based Study. J. Clin. Diagn. Res. 2017, 11, OC14–OC16. [Google Scholar] [CrossRef] [PubMed]
- Suhrs, H.E.; Michelsen, M.M.; Prescott, E. Treatment strategies in coronary microvascular dysfunction: A systematic review of interventional studies. Microcirculation 2019, 26, e12430. [Google Scholar] [CrossRef]
- Yip, A.; Saw, J. Spontaneous coronary artery dissection. Cardiovasc. OCT Imaging 2015, 5, 119–128. [Google Scholar] [CrossRef]
- Rashid, H.N.Z.; Wong, D.T.L.; Wijesekera, H.; Gutman, S.J.; Shanmugam, V.B.; Gulati, R.; Malaipan, Y.; Meredith, I.T.; Psaltis, P.J. Incidence and characterisation of spontaneous coronary artery dissection as a cause of acute coronary syndrome—A single-centre Australian experience. Int. J. Cardiol. 2016, 202, 336–338. [Google Scholar] [CrossRef]
- Rogowski, S.; Maeder, M.T.; Weilenmann, D.; Haager, P.K.; Ammann, P.; Rohner, F.; Joerg, L.; Rickli, H. Spontaneous Coronary Artery Dissection: Angiographic Follow-Up and Long-Term Clinical Outcome in a Predominantly Medically Treated Population. Catheter. Cardiovasc. Interv. Off. J. Soc. Card. Angiogr. Interv. 2017, 89, 59–68. [Google Scholar] [CrossRef]
- Adlam, D.; Alfonso, F.; Maas, A.; Vrints, C. European Society of Cardiology, acute cardiovascular care association, SCAD study group: A position paper on spontaneous coronary artery dissection. Eur. Heart J. 2018, 39, 3353–3368. [Google Scholar] [CrossRef]
- Alkhouli, M.; Cole, M.; Ling, F.S. Coronary Artery Fenestration Prior to Stenting in Spontaneous Coronary Artery Dissection. Catheter. Cardiovasc. Interv. 2016, 88, E23–E27. [Google Scholar] [CrossRef]
- Mahmoud, A.N.; Taduru, S.S.; Mentias, A.; Mahtta, D.; Barakat, A.F.; Saad, M.; Elgendy, A.Y.; Mojadidi, M.K.; Omer, M.; Abuzaid, A.; et al. Trends of Incidence, Clinical Presentation, and in-Hospital Mortality among Women with Acute Myocardial Infarction with or without Spontaneous Coronary Artery Dissection: A Population-Based Analysis. JACC Cardiovasc. Interv. 2018, 11, 80–90. [Google Scholar] [CrossRef]
- Beltrame, J.F. Assessing patients with myocardial infarction and nonobstructed coronary arteries (MINOCA). J. Intern. Med. 2013, 273, 182–185. [Google Scholar] [CrossRef]
- Pelliccia, F.; Pasceri, V.; Niccoli, G.; Tanzilli, G.; Speciale, G.; Gaudio, C.; Crea, F.; Camici, P.G. Predictors of Mortality in Myocardial Infarction and Nonobstructed Coronary Arteries: A Systematic Review and Meta-Regression. Am. J. Med. 2020, 133, 73–83.e4. [Google Scholar] [CrossRef] [PubMed]
- Pasupathy, S.; Lindahl, B.; Litwin, P.; Tavella, R.; Williams, M.J.; Air, T.; Zeitz, C.; Smilowitz, N.R.; Reynolds, H.R.; Eggers, K.M.; et al. Survival in Patients with Suspected Myocardial Infarction with Nonobstructive Coronary Arteries: A Comprehensive Systematic Review and Meta-Analysis from the MINOCA Global Collaboration. Circ. Cardiovasc. Qual. Outcomes 2021, 14, e007880. [Google Scholar] [CrossRef] [PubMed]
- Bugiardini, R.; Manfrini, O.; De Ferrari, G.M. Unanswered Questions for Management of Acute Coronary Syndrome. Arch. Intern. Med. 2006, 166, 1391–1395. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, S.; Jones, D.A.; Anand, V.; Mohiddin, S. Diagnosis and management of patients with acute cardiac symptoms, troponin elevation and culprit-free angiograms. Heart 2012, 98, 974–981. [Google Scholar] [CrossRef]
- Nordenskjöld, A.M.; Baron, T.; Eggers, K.M.; Jernberg, T.; Lindahl, B. Predictors of adverse outcome in patients with myocardial infarction with non-obstructive coronary artery (MINOCA) disease. Int. J. Cardiol. 2018, 261, 18–23. [Google Scholar] [CrossRef]
- Niccoli, G.; Montone, R.A.; Di Vito, L.; Gramegna, M.; Refaat, H.; Scalone, G.; Leone, A.M.; Trani, C.; Burzotta, F.; Porto, I.; et al. Plaque rupture and intact fibrous cap assessed by optical coherence tomography portend different outcomes in patients with acute coronary syndrome. Eur. Heart J. 2015, 36, 1377–1384. [Google Scholar] [CrossRef] [PubMed]
- Safdar, B.; Spatz, E.S.; Dreyer, R.P.; Beltrame, J.F.; Lichtman, J.H.; Spertus, J.A.; Reynolds, H.R.; Geda, M.; Bueno, H.; Dziura, J.D.; et al. Presentation, clinical profile, and prognosis of young patients with myocardial infarction with nonobstructive coronary arteries (MINOCA): Results from the VIRGO study. J. Am. Heart Assoc. 2018, 7, e009174. [Google Scholar] [CrossRef]
- Kang, W.Y.; Jeong, M.H.; Ahn, Y.K.; Kim, J.H.; Chae, S.C.; Kim, Y.J.; Hur, S.H.; Seong, I.W.; Hong, T.J.; Choi, D.H.; et al. Are patients with angiographically near-normal coronary arteries who present as acute myocardial infarction actually safe? Int. J. Cardiol. 2011, 146, 207–212. [Google Scholar] [CrossRef]
- Planer, D.; Mehran, R.; Ohman, E.M.; White, H.D.; Newman, J.D.; Xu, K.; Stone, G.W. Prognosis of patients with non-ST-segment-elevation myocardial infarction and nonobstructive coronary artery disease: Propensity-matched analysis from the acute catheterization and urgent intervention triage strategy trial. Circ. Cardiovasc. Interv. 2014, 7, 285–293. [Google Scholar] [CrossRef]
- Grodzinsky, A.; Arnold, S.V.; Gosch, K.; Spertus, J.A.; Foody, J.M.; Beltrame, J.; Maddox, T.M.; Parashar, S.; Kosiborod, M. Angina frequency after acute myocardial infarction in patients without obstructive coronary artery disease. Eur. Heart J. Qual. Care Clin. Outcomes 2015, 1, 92–99. [Google Scholar] [CrossRef]
- Di Fiore, D.P.; Beltrame, J.F. Chest pain in patients with “normal angiography”: Could it be cardiac? Int. J. Evid. Based Healthc. 2013, 11, 56–68. [Google Scholar] [CrossRef] [PubMed]
- Andersson, H.B.; Pedersen, F.; Engstrøm, T.; Helqvist, S.; Jensen, M.K.; Jørgensen, E.; Kelbæk, H.; Räder, S.B.E.W.; Saunamäki, K.; Bates, E.; et al. Long-term survival and causes of death in patients with ST-elevation acute coronary syndrome without obstructive coronary artery disease. Eur. Heart J. 2018, 39, 102–110. [Google Scholar] [CrossRef] [PubMed]
- Barr, P.R.; Harrison, W.; Smyth, D.; Flynn, C.; Lee, M.; Kerr, A.J. Myocardial Infarction without Obstructive Coronary Artery Disease is Not a Benign Condition (ANZACS-QI 10). Heart Lung Circ. 2018, 27, 165–174. [Google Scholar] [CrossRef]
- Rossini, R.; Capodanno, D.; Lettieri, C.; Azimi, A.; Mæng, M.; Jensen, L.O.; Torp-Pedersen, C. Long-term outcomes of patients with acute coronary syndrome and nonobstructive coronary artery disease. Am. J. Cardiol. 2013, 112, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Ramanath, V.S.; Armstrong, D.F.; Grzybowski, M.; Rahnama-Mohagdam, S.; Tamhane, U.U.; Gordon, K.; Froehlich, J.B.; Eagle, K.A.; Jackson, E.A. Receipt of cardiac medications upon discharge among men and women with acute coronary syndrome and nonobstructive coronary artery disease. Clin. Cardiol. 2010, 33, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Adatia, F.; Galway, S.; Grubisic, M.; Lee, M.; Daniele, P.; Humphries, K.H.; Sedlak, T.L. Cardiac Medication Use in Patients with Acute Myocardial Infarction and Nonobstructive Coronary Artery Disease. J. Women’s Health 2017, 26, 1185–1192. [Google Scholar] [CrossRef]
- Bainey, K.R.; Welsh, R.C.; Alemayehu, W.; Westerhout, C.M.; Traboulsi, D.; Anderson, T.; Brass, N.; Armstrong, P.W.; Kaul, P. Population-level incidence and outcomes of myocardial infarction with non-obstructive coronary arteries (MINOCA): Insights from the Alberta contemporary acute coronary syndrome patients invasive treatment strategies (COAPT) study. Int. J. Cardiol. 2018, 264, 12–17. [Google Scholar] [CrossRef]
- Mileva, N.; Paolisso, P.; Gallinoro, E.; Fabbricatore, D.; Munhoz, D.; Bergamaschi, L.; Belmonte, M.; Panayotov, P.; Pizzi, C.; Barbato, E.; et al. Diagnostic and Prognostic Role of Cardiac Magnetic Resonance in MINOCA: Systematic Review and Meta-Analysis. JACC Cardiovasc. Imaging 2023, 16, 376–389. [Google Scholar] [CrossRef]
- Kumar, V.; Rosenzweig, R.; Asalla, S.; Nehra, S.; Prabhu, S.D.; Bansal, S.S. TNFR1 Contributes to Activation-Induced Cell Death of Pathological CD4+ T Lymphocytes During Ischemic Heart Failure. JACC Basic Transl. Sci. 2022, 7, 1038–1049. [Google Scholar] [CrossRef]
- Lillo, R.; Graziani, F.; Franceschi, F.; Iannaccone, G.; Massetti, M.; Olivotto, I.; Crea, F.; Liuzzo, G. Inflammation across the spectrum of hypertrophic cardiac phenotypes. Heart Fail. Rev. 2023, 28, 1065–1075. [Google Scholar] [CrossRef]
- Matthia, E.L.; Setteducato, M.L.; Elzeneini, M.; Vernace, N.; Salerno, M.; Kramer, C.M.; Keeley, E.C. Circulating Biomarkers in Hypertrophic Cardiomyopathy. J. Am. Heart Assoc. 2022, 11, e027618. [Google Scholar] [CrossRef] [PubMed]
- Becker, R.C.; Owens, A.P.; Sadayappan, S. Tissue-level inflammation and ventricular remodeling in hypertrophic cardiomyopathy. J. Thromb. Thrombolysis 2020, 49, 177–183. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| 1. AMI (Modified from the ‘Fourth Universal Definition of Myocardial Infarction’ Criteria): | 2. Non-Obstructive Coronary Arteries on Angiography [Absence of Obstructive Disease on Angiography (i.e., No Coronary Artery Stenosis ≥ 50%) in Any Major Epicardial Vessel]: | 3. No Specific Alternate Diagnosis for the Clinical Presentation: |
|---|---|---|
|
| Non-ischaemic causes such as sepsis, heart failure, cardiomyopathy, pulmonary embolism, cardiac contusion, aortic dissection, Takotsubo syndrome and myocarditis |
|
| MINOCA Specific Cause: | Helpful Diagnostic Tool: |
|---|---|
| Atherosclerotic plaque disruption | Invasive Coronary Angiography + Cardiac Magnetic Resonance |
| Coronary embolism | Invasive Coronary Angiography |
| SCAD | Invasive Coronary Angiography + intravascular imaging |
| Epicardial or microvascular spasm | Invasive Coronary Angiography + provocative testing |
| Coronary microvascular dysfunction | Invasive Coronary Angiography + index of microvascular resistance |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Samaras, A.; Moysidis, D.V.; Papazoglou, A.S.; Rampidis, G.; Kampaktsis, P.N.; Kouskouras, K.; Efthymiadis, G.; Ziakas, A.; Fragakis, N.; Vassilikos, V.; et al. Diagnostic Puzzles and Cause-Targeted Treatment Strategies in Myocardial Infarction with Non-Obstructive Coronary Arteries: An Updated Review. J. Clin. Med. 2023, 12, 6198. https://doi.org/10.3390/jcm12196198
Samaras A, Moysidis DV, Papazoglou AS, Rampidis G, Kampaktsis PN, Kouskouras K, Efthymiadis G, Ziakas A, Fragakis N, Vassilikos V, et al. Diagnostic Puzzles and Cause-Targeted Treatment Strategies in Myocardial Infarction with Non-Obstructive Coronary Arteries: An Updated Review. Journal of Clinical Medicine. 2023; 12(19):6198. https://doi.org/10.3390/jcm12196198
Chicago/Turabian StyleSamaras, Athanasios, Dimitrios V. Moysidis, Andreas S. Papazoglou, Georgios Rampidis, Polydoros N. Kampaktsis, Konstantinos Kouskouras, Georgios Efthymiadis, Antonios Ziakas, Nikolaos Fragakis, Vasileios Vassilikos, and et al. 2023. "Diagnostic Puzzles and Cause-Targeted Treatment Strategies in Myocardial Infarction with Non-Obstructive Coronary Arteries: An Updated Review" Journal of Clinical Medicine 12, no. 19: 6198. https://doi.org/10.3390/jcm12196198
APA StyleSamaras, A., Moysidis, D. V., Papazoglou, A. S., Rampidis, G., Kampaktsis, P. N., Kouskouras, K., Efthymiadis, G., Ziakas, A., Fragakis, N., Vassilikos, V., & Giannakoulas, G. (2023). Diagnostic Puzzles and Cause-Targeted Treatment Strategies in Myocardial Infarction with Non-Obstructive Coronary Arteries: An Updated Review. Journal of Clinical Medicine, 12(19), 6198. https://doi.org/10.3390/jcm12196198