
Harnessing Machine Learning for Prediction of Postoperative Pulmonary Complications: Retrospective Cohort Design

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Patients and Postoperative Pulmonary Complications
2.3. Dataset
2.4. Machine Learning
2.5. Feature Importance and Simplified Models
2.6. Statistics and Metrics
3. Results
3.1. Patient Characteristics
3.2. Model Performance
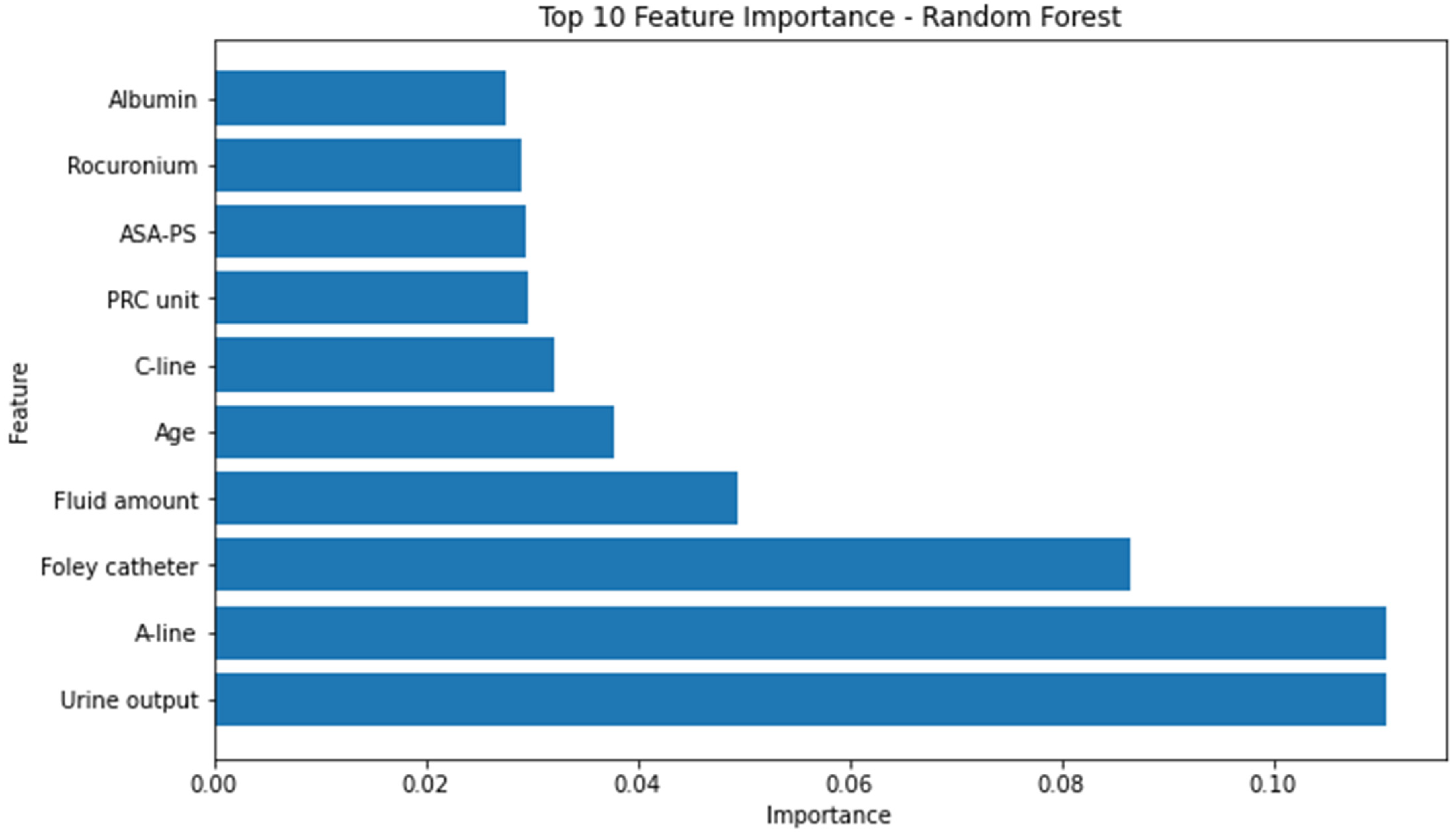
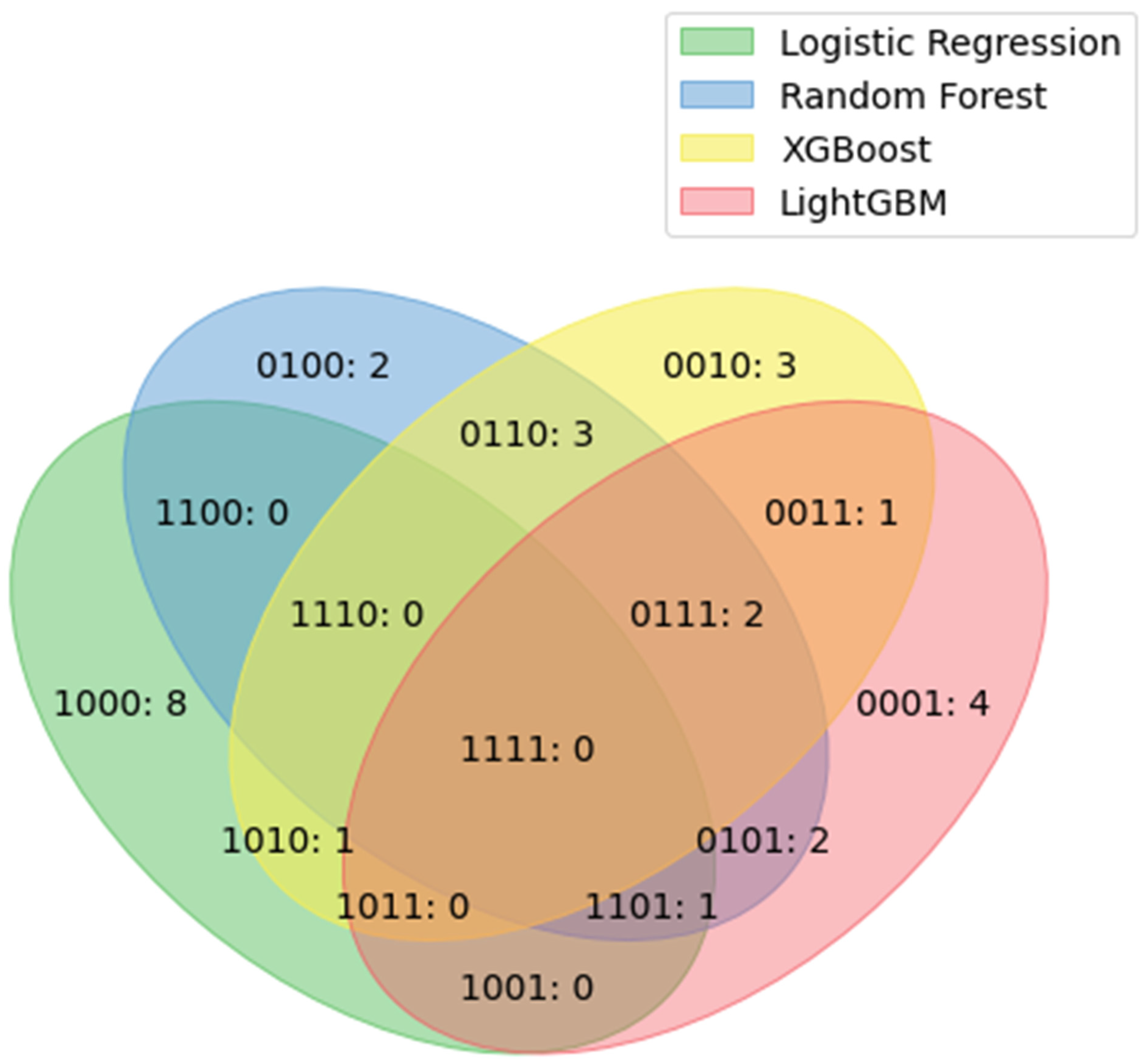
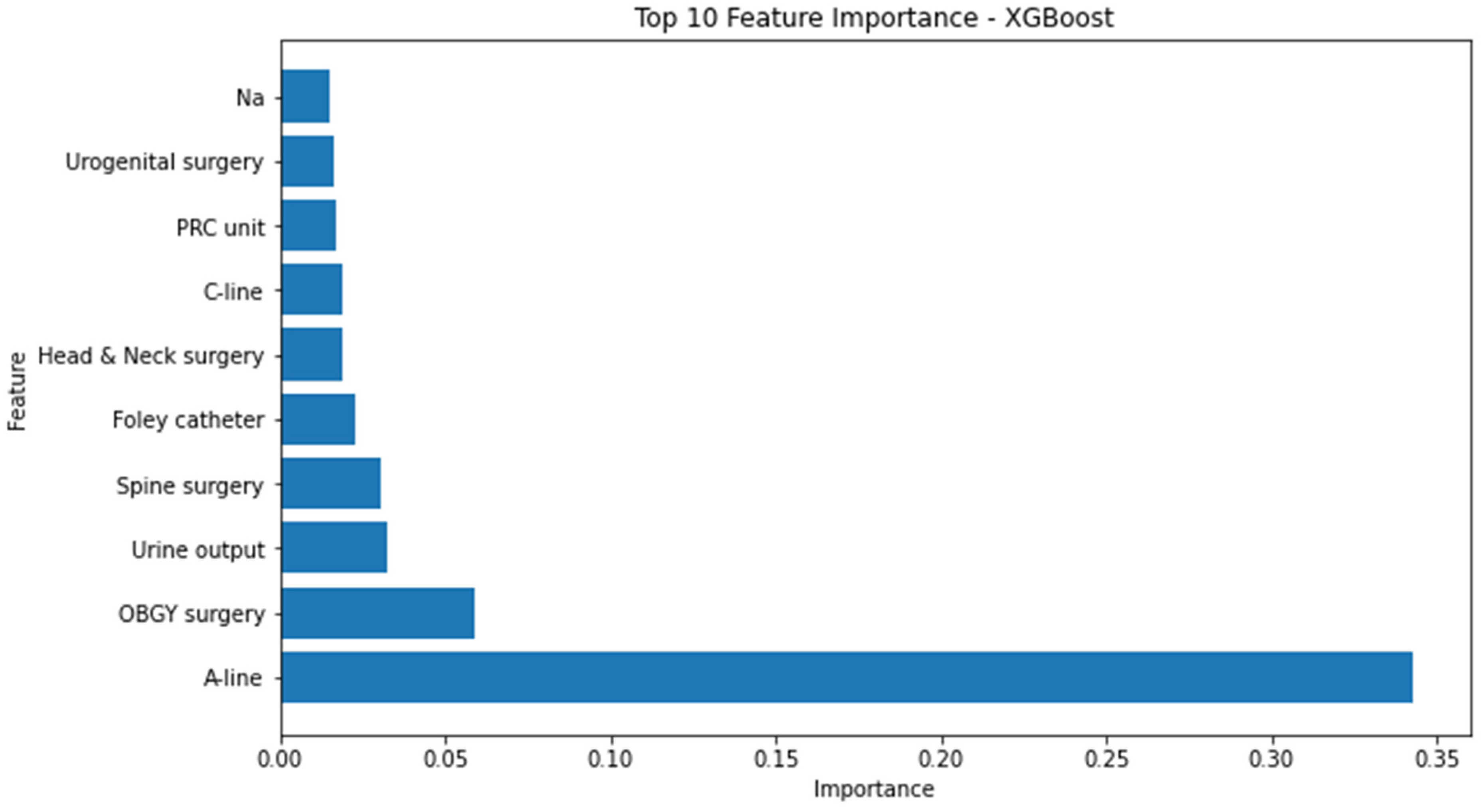
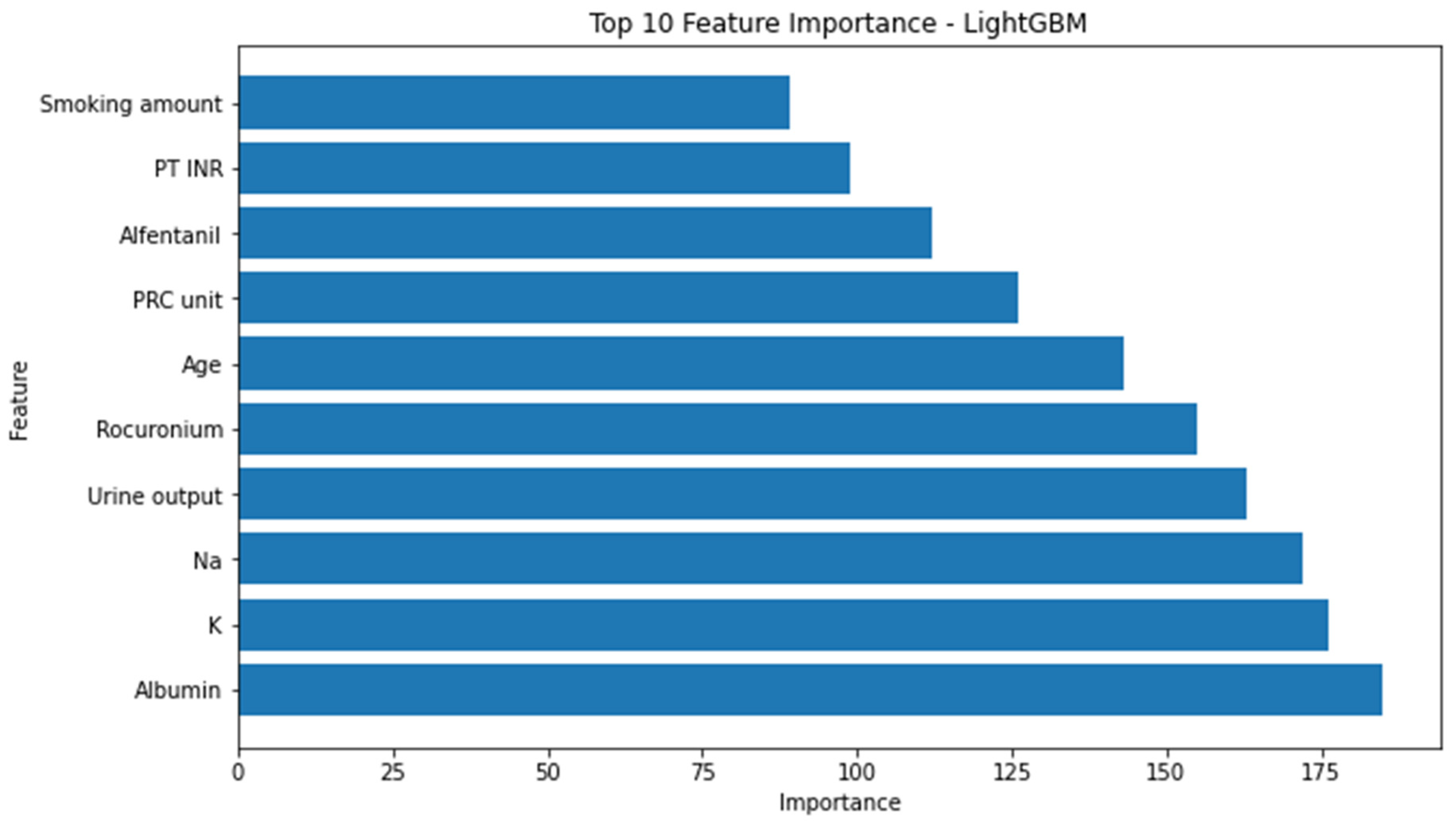
3.3. Feature Importance
3.4. Evaluation of Simplicity Model
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

Appendix B

References
- Lawrence, V.A.; Cornell, J.E.; Smetana, G.W. Strategies to reduce postoperative pulmonary complications after noncardiothoracic surgery: Systematic review for the American College of Physicians. Ann. Intern. Med. 2006, 144, 596–608. [Google Scholar] [CrossRef] [PubMed]
- Fisher, B.W.; Majumdar, S.R.; McAlister, F.A. Predicting pulmonary complications after nonthoracic surgery: A systematic review of blinded studies. Am. J. Med. 2002, 112, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Miskovic, A.; Lumb, A.B. Postoperative pulmonary complications. Br. J. Anaesth. 2017, 118, 317–334. [Google Scholar] [CrossRef] [PubMed]
- Gupta, H.; Gupta, P.K.; Fang, X.; Miller, W.J.; Cemaj, S.; Forse, R.A.; Morrow, L.E. Development and validation of a risk calculator predicting postoperative respiratory failure. Chest 2011, 140, 1207–1215. [Google Scholar] [CrossRef]
- Qaseem, A.; Snow, V.; Fitterman, N.; Hornbake, E.R.; Lawrence, V.A.; Smetana, G.W.; Weiss, K.; Owens, D.K.; for the Clinical Efficacy Assessment Subcommittee of the American College of Physicians. Risk assessment for and strategies to reduce perioperative pulmonary complications for patients undergoing noncardiothoracic surgery: A guideline from the American College of Physicians. Ann. Intern. Med. 2006, 144, 575–580. [Google Scholar] [CrossRef]
- Kim, J.H.; Kim, Y.; Yoo, K.; Kim, M.; Kang, S.S.; Kwon, Y.-S.; Lee, J.J. Prediction of Postoperative Pulmonary Edema Risk Using Machine Learning. J. Clin. Med. 2023, 12, 1804. [Google Scholar] [CrossRef]
- Peng, X.; Zhu, T.; Chen, G.; Wang, Y.; Hao, X. A multicenter prospective study on postoperative pulmonary complications prediction in geriatric patients with deep neural network model. Front. Surg. 2022, 9, 976536. [Google Scholar] [CrossRef]
- Xue, B.; Li, D.; Lu, C.; King, C.R.; Wildes, T.; Avidan, M.S.; Kannampallil, T.; Abraham, J. Use of machine learning to develop and evaluate models using preoperative and intraoperative data to identify risks of postoperative complications. JAMA Netw. Open 2021, 4, e212240. [Google Scholar] [CrossRef]
- Xue, Q.; Wen, D.; Ji, M.-H.; Tong, J.; Yang, J.-J.; Zhou, C.-M. Developing machine learning algorithms to predict pulmonary complications after emergency gastrointestinal surgery. Front. Med. 2021, 8, 655686. [Google Scholar] [CrossRef]
- Javaid, M.; Haleem, A.; Pratap Singh, R.; Suman, R.; Rab, S. Significance of machine learning in healthcare: Features, pillars and applications. Int. J. Intell. Netw. 2022, 3, 58–73. [Google Scholar] [CrossRef]
- LightGBM. Available online: https://lightgbm.readthedocs.io/en/v3.3.2/ (accessed on 30 January 2023).
- Scalable and Flexible Gradient Boosting. Available online: https://xgboost.ai/ (accessed on 30 January 2023).
- XGBoost. Available online: https://xgboost.readthedocs.io/en/stable/ (accessed on 30 January 2023).
- sklearn.neural_network.MLPClassifier. Available online: https://scikit-learn.org/stable/modules/generated/sklearn.neural_network.MLPClassifier.html (accessed on 30 January 2023).
- sklearn.linear_model.LogisticRegression. Available online: https://scikit-learn.org/stable/modules/generated/sklearn.linear_model.LogisticRegression.html (accessed on 30 January 2023).
- Bergstra, J.; Bengio, Y. Random search for hyper-parameter optimization. J. Mach. Learn. Res. 2012, 13, 281–305. [Google Scholar]
- Chen, T.; He, T.; Benesty, M.; Khotilovich, V.; Tang, Y.; Cho, H.; Chen, K.; Mitchell, R.; Cano, I.; Zhou, T. Xgboost: Extreme gradient boosting. R Package Version 0.4–2 2015, 1, 1–4. [Google Scholar]
- Ke, G.; Meng, Q.; Finley, T.; Wang, T.; Chen, W.; Ma, W.; Ye, Q.; Liu, T.-Y. Lightgbm: A highly efficient gradient boosting decision tree. Adv. Neural Inf. Process. Syst. 2017, 30, 3149–3157. [Google Scholar]
- Chawla, N.V.; Bowyer, K.W.; Hall, L.O.; Kegelmeyer, W.P. SMOTE: Synthetic minority over-sampling technique. J. Artif. Intell. Res. 2002, 16, 321–357. [Google Scholar] [CrossRef]
- Feurer, M.; Hutter, F. Hyperparameter optimization. In Automated Machine Learning; Springer: Cham, Switzerland, 2019; pp. 3–33. [Google Scholar]
- Pudjihartono, N.; Fadason, T.; Kempa-Liehr, A.W.; O’Sullivan, J.M. A review of feature selection methods for machine learning-based disease risk prediction. Front. Bioinform. 2022, 2, 927312. [Google Scholar] [CrossRef]
- Wang, Q.; Lu, Y.; Zhang, X.; Hahn, J. Region of Interest Selection for Functional Features. Neurocomputing 2021, 422, 235–244. [Google Scholar] [CrossRef]
- Abawajy, J.; Darem, A.; Alhashmi, A.A. Feature Subset Selection for Malware Detection in Smart IoT Platforms. Sensors 2021, 21, 1374. [Google Scholar] [CrossRef]
- Faubel, S. Pulmonary complications after acute kidney injury. Adv. Chronic Kidney Dis. 2008, 15, 284–296. [Google Scholar] [CrossRef]
- Turcios, N.L. Pulmonary complications of renal disorders. Paediatr. Respir. Rev. 2012, 13, 44–49. [Google Scholar] [CrossRef]
- Benson, A.B. Pulmonary complications of transfused blood components. Crit. Care Nurs. Clin. N. Am. 2012, 24, 403–418. [Google Scholar] [CrossRef][Green Version]
- Grey, S.; Bolton-Maggs, P. Pulmonary complications of transfusion: Changes, challenges, and future directions. Transfus. Med. 2020, 30, 442–449. [Google Scholar] [CrossRef] [PubMed]
- Cammu, G. Residual Neuromuscular Blockade and Postoperative Pulmonary Complications: What Does the Recent Evidence Demonstrate? Curr. Anesth. Rep. 2020, 10, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, D.A.; Witkowski, E.; Gao, L.; Meireles, O.; Rosman, G. Artificial Intelligence in Anesthesiology: Current Techniques, Clinical Applications, and Limitations. Anesthesiology 2020, 132, 379–394. [Google Scholar] [CrossRef]
- Shalbaf, R.; Behnam, H.; Sleigh, J.W.; Steyn-Ross, A.; Voss, L.J. Monitoring the depth of anesthesia using entropy features and an artificial neural network. J. Neurosci. Methods 2013, 218, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Murabito, P.; Astuto, M.; Sanfilippo, F.; La Via, L.; Vasile, F.; Basile, F.; Cappellani, A.; Longhitano, L.; Distefano, A.; Li Volti, G. Proactive Management of Intraoperative Hypotension Reduces Biomarkers of Organ Injury and Oxidative Stress during Elective Non-Cardiac Surgery: A Pilot Randomized Controlled Trial. J. Clin. Med. 2022, 11, 392. [Google Scholar] [CrossRef]
- Sanfilippo, F.; La Via, L.; Dezio, V.; Amelio, P.; Genoese, G.; Franchi, F.; Messina, A.; Robba, C.; Noto, A. Inferior vena cava distensibility from subcostal and trans-hepatic imaging using both M-mode or artificial intelligence: A prospective study on mechanically ventilated patients. Intensive Care Med. Exp. 2023, 11, 40. [Google Scholar] [CrossRef]
- Wijnberge, M.; Geerts, B.F.; Hol, L.; Lemmers, N.; Mulder, M.P.; Berge, P.; Schenk, J.; Terwindt, L.E.; Hollmann, M.W.; Vlaar, A.P.; et al. Effect of a Machine Learning–Derived Early Warning System for Intraoperative Hypotension vs Standard Care on Depth and Duration of Intraoperative Hypotension During Elective Noncardiac Surgery: The HYPE Randomized Clinical Trial. JAMA 2020, 323, 1052–1060. [Google Scholar] [CrossRef]
- Khan, B.; Fatima, H.; Qureshi, A.; Kumar, S.; Hanan, A.; Hussain, J.; Abdullah, S. Drawbacks of Artificial Intelligence and Their Potential Solutions in the Healthcare Sector. In Biomedical Materials & Devices; Springer: Cham, Switzerland, 2023; pp. 1–8. [Google Scholar] [CrossRef]
- Takada, T.; Nijman, S.; Denaxas, S.; Snell, K.I.E.; Uijl, A.; Nguyen, T.-L.; Asselbergs, F.W.; Debray, T.P.A. Internal-external cross-validation helped to evaluate the generalizability of prediction models in large clustered datasets. J. Clin. Epidemiol. 2021, 137, 83–91. [Google Scholar] [CrossRef]
- Boge, F.J.; Grünke, P.; Hillerbrand, R. Minds and Machines Special Issue: Machine Learning: Prediction Without Explanation? Minds Mach. 2022, 32, 1–9. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Non-PPCs (n = 101,557) | PPCs (n = 9655) | ASD | |
|---|---|---|---|
| Age | 52 (39, 63) | 67 (56, 77) | 0.92 |
| Male sex | 49,313 (48.6) | 5144 (53.3) | 0.09 |
| Order of surgery | 1 (1, 1) | 1 (1, 1) | 0.19 |
| Cooperative surgery (count) | 1 (1, 1) | 1 (1, 1) | 0.13 |
| Body mass index | 24.2 (21.9, 26.7) | 24 (21.5, 26.6) | 0.07 |
| Congestive heart failure | 2910 (2.9) | 1021 (10.6) | 0.33 |
| Cardiac arrhythmia | 3846 (3.8) | 890 (9.2) | 0.23 |
| Valvular diseases | 601 (0.6) | 247 (2.6) | 0.17 |
| Pulmonary circulation disorders | 440 (0.4) | 298 (3.1) | 0.22 |
| Peripheral vascular disorders | 2200 (2.2) | 442 (4.6) | 0.14 |
| Hypertension, uncomplicated | 11471 (11.3) | 2189 (22.7) | 0.31 |
| Hypertension, complicated | 5033 (5.0) | 971 (10.1) | 0.20 |
| Paralysis | 424 (0.4) | 137 (1.4) | 0.11 |
| Other neurological disorders | 3310 (3.3) | 759 (7.9) | 0.21 |
| Chronic pulmonary diseases | 9176 (9.0) | 1526 (15.8) | 0.21 |
| Diabetes, uncomplicated | 6374 (6.3) | 1218 (12.6) | 0.22 |
| Diabetes, complicated | 6471 (6.4) | 1352 (14.0) | 0.26 |
| Hypothyroidism | 2225 (2.2) | 327 (3.4) | 0.07 |
| Renal failure | 3597 (3.5) | 1022 (10.6) | 0.29 |
| Liver disease | 4710 (4.6) | 847 (8.8) | 0.17 |
| Peptic ulcer disease (excluding bleeding) | 1853 (1.8) | 272 (2.8) | 0.07 |
| AIDS/HIV | 22 (0.0) | 1 (0.0) | 0.01 |
| Lymphoma | 402 (0.4) | 76 (0.8) | 0.05 |
| Metastatic cancer | 1112 (1.1) | 276 (2.9) | 0.13 |
| Solid tumor without metastasis | 17,016 (16.8) | 3429 (35.5) | 0.44 |
| Rheumatoid arthritis/collagen vascular diseases | 2532 (2.5) | 289 (3.0) | 0.03 |
| Coagulopathy | 697 (0.7) | 209 (2.2) | 0.13 |
| Obesity | 845 (0.8) | 78 (0.8) | 0.00 |
| Weight loss | 338 (0.3) | 63 (0.7) | 0.05 |
| Fluid and electrolyte disorders | 2621 (2.6) | 844 (8.7) | 0.28 |
| Blood-loss anemia | 312 (0.3) | 25 (0.3) | 0.01 |
| Deficiency anemia | 3012 (3.0) | 611 (6.3) | 0.16 |
| Alcohol abuse | 2106 (2.1) | 370 (3.8) | 0.11 |
| Drug abuse | 1647 (1.6) | 193 (2.0) | 0.03 |
| Psychoses | 660 (0.6) | 128 (1.3) | 0.07 |
| Depression | 5449 (5.4) | 869 (9.0) | 0.14 |
| Unconsciousness | 1780 (1.8) | 1490 (15.4) | 0.56 |
| Alcohol (consumption/unknown) | 27,481 (27.1)/4774 (4.7) | 2038 (21.1)/584 (6.0) | 0.03 |
| Smoking amount (packs) | 0 (0, 0) | 0 (0, 0) | 0.03 |
| Smoking duration (years) | 0 (0, 0) | 0 (0, 0) | 0.15 |
| Emergency | 15,986 (15.7) | 2828 (29.3) | 0.33 |
| ASA-PS | 1.08 | ||
| 1 | 30,415 (29.9) | 419 (4.3) | |
| 2 | 51,757 (51.0) | 3254 (33.7) | |
| 3 | 18,367 (18.1) | 5022 (52.0) | |
| 4 | 969 (1.0) | 908 (9.4) | |
| 5 | 37 (0.0) | 52 (0.5) | |
| 6 | 12 (0.0) | 0 (0.0) |
| Non-PPCs (n = 101,557) | PPCs (n = 9655) | ASD | |
|---|---|---|---|
| General anesthesia | 87,884 (86.5) | 9160 (94.9) | 0.30 |
| Inhalation anesthetics | 85,174 (83.9) | 8062 (83.5) | 0.01 |
| N2O | 13,982 (13.8) | 1274 (13.2) | 0.02 |
| Anesthesia time (min) | 100 (65, 150) | 175 (115, 270) | 0.82 |
| Surgery time (min) | 65 (35, 110) | 125 (75, 210) | 0.77 |
| Intraoperative fluid administration | 450 (300, 800) | 1400 (700, 2400) | 0.93 |
| Intraoperative urine output | 0 (0, 15) | 150 (35, 400) | 0.63 |
| Arterial line | 26,167 (25.8) | 8466 (87.7) | 1.62 |
| Central venous line | 5978 (5.9) | 5111 (52.9) | 1.28 |
| Foley catheter | 31,762 (31.3) | 8101 (83.9) | 1.27 |
| Levin tube | 1267 (1.2) | 1185 (12.3) | 0.50 |
| Patient-controlled analgesia (intravenous/other) | 43,863 (43.2)/142 (0.1) | 6951 (72.0)/4 (0.0) | 0.60 |
| Intraoperative packed red blood cells | 0 (0, 0) | 0 (0, 1) | 0.56 |
| Intraoperative FFP | 0 (0, 0) | 0 (0, 0) | 0.44 |
| Intraoperative PC | 0 (0, 0) | 0 (0, 0) | 0.18 |
| Intraoperative cryoprecipitate | 0 (0, 0) | 0 (0, 0) | 0.05 |
| Rocuronium | 40 (30, 50) | 50 (40, 90) | 0.54 |
| Vecuronium | 0 (0, 0) | 0 (0, 0) | 0.33 |
| Atracurium | 0 (0, 0) | 0 (0, 0) | 0.24 |
| Cisatracurium | 0 (0, 0) | 0 (0, 0) | 0.21 |
| Succinylcholine | 0 (0, 0) | 0 (0, 0) | 0.06 |
| Pyridostigmine | 0 (0, 15) | 0 (0, 15) | 0.12 |
| Neostigmine | 0 (0, 2) | 0 (0, 2) | 0.28 |
| Sugammadex | 0 (0, 0) | 0 (0, 0) | 0.24 |
| Fentanyl | 0.04 (0, 1) | 0.8 (0, 1.2) | 0.53 |
| Alfentanil | 0 (0, 0) | 0 (0, 0.25) | 0.14 |
| Sufentanil | 0 (0, 0) | 0 (0, 0) | 0.30 |
| Remifentanil | 1 (0, 1) | 1 (1, 2) | 0.48 |
| Pethidine | 0 (0, 0) | 0 (0, 0) | 0.02 |
| BUN | 13.8 (11.1, 17) | 15.4 (12, 20.2) | 0.38 |
| Cr | 0.8 (0.66, 0.92) | 0.81 (0.69, 1) | 0.24 |
| GFR | 91.3 (78.2, 106.7) | 82.8 (65.3, 101.25) | 0.27 |
| PT | 12.5 (11.8, 13.1) | 12.6 (11.7, 13.5) | 0.16 |
| aPTT | 33.9 (31.3, 36.9) | 33.3 (30.1, 37) | 0.03 |
| INR | 0.99 (0.94, 1.04) | 1.02 (0.96, 1.1) | 0.29 |
| Platelet count | 245 (207, 289) | 224 (178, 279) | 0.21 |
| Na | 140 (138, 141) | 139 (137, 141) | 0.24 |
| K | 4.2 (3.9, 4.4) | 4 (3.8, 4.3) | 0.28 |
| Uric acid | 4.8 (3.9, 5.9) | 4.7 (3.6, 5.9) | 0.09 |
| Protein | 7.2 (6.8, 7.5) | 6.8 (6.2, 7.2) | 0.62 |
| Albumin | 4.4 (4.2, 4.6) | 4.1 (3.6, 4.4) | 0.77 |
| Robotic surgery | 2153 (2.1) | 450 (4.7) | 0.14 |
| Laparoscopic surgery | 17811 (17.5) | 1931 (20.0) | 0.06 |
| Heart surgery | 81 (0.1) | 334 (3.5) | 0.32 |
| Abdominal surgery (minor/major) | 14,959 (14.7)/2362 (2.3) | 1274 (13.2)/1441 (14.9) | 0.40 |
| Breast surgery (minor/major) | 4577 (4.5)/10 (0.0) | 31 (0.3)/6 (0.1) | 0.29 |
| Ear surgery | 2479 (2.4) | 22 (0.2) | 0.22 |
| Endocrine surgery (minor/major) | 1651 (1.6)/1396 (1.4) | 68 (0.7)/25 (0.3) | 0.16 |
| Eye surgery | 2049 (2.0) | 16 (0.2) | 0.20 |
| Head and neck surgery (minor/major) | 12,361 (12.2)/76 (0.1) | 132 (1.4)/26 (0.3) | 0.43 |
| Musculoskeletal surgery (minor/major) | 28,873 (28.4)/1227 (1.2) | 1524 (15.8)/665 (6.9) | 0.02 |
| Neurosurgery (minor/major) | 2787 (2.7)/985 (1.0) | 646 (6.7)/55 (0.6) | 0.39 |
| OBGY surgery (minor/major) | 9486 (9.3)/238 (0.2) | 169 (1.8)/55 (0.6) | 0.27 |
| Spine surgery (minor/major) | 2928 (2.9)/1719 (1.7) | 361 (3.7)/480 (5.0) | 0.19 |
| Thoracic surgery (minor/major) | 262 (0.3)/114 (0.1) | 355 (3.7)/281 (2.9) | 0.39 |
| Transplantation surgery (minor/major) | 25 (0.0)/45 (0.0) | 12 (0.1)/50 (0.5) | 0.11 |
| Urogenital surgery (minor/major) | 8789 (8.7)/575 (0.6) | 267 (2.8)/456 (4.7) | 0.06 |
| Vascular surgery (minor/major) | 630 (0.6)/20 (0.0) | 159 (1.6)/61 (0.6) | 0.16 |
| Skin and soft tissue surgery (minor/major) | 4041 (4.0)/88 (0.1) | 114 (1.2)/31 (0.3) | 0.13 |
| Accuracy (95% CI) | Recall (95% CI) | Precision (95% CI) | AUROC (95% CI) | F1 Score (95% CI) | |
|---|---|---|---|---|---|
| Logistic regression | 0.866 (0.861–0.87) | 0.647 (0.626–0.669) | 0.352 (0.336–0.368) | 0.767 (0.756–0.778) | 0.456 (0.439–0.472) |
| Random forest | 0.912 (0.908–0.915) | 0.564 (0.542–0.587) | 0.492 (0.471–0.513) | 0.754 (0.743–0.766) | 0.526 (0.507–0.544) |
| MLP neural network | 0.899 (0.895–0.903) | 0.471 (0.448–0.493) | 0.425 (0.404–0.446) | 0.705 (0.694–0.716) | 0.446 (0.427–0.465) |
| XG boost | 0.924 (0.92–0.927) | 0.427 (0.405–0.449) | 0.582 (0.556–0.607) | 0.699 (0.688–0.71) | 0.492 (0.471–0.512) |
| Light GBM | 0.924 (0.921–0.928) | 0.452 (0.43–0.475) | 0.583 (0.557–0.607) | 0.711 (0.699–0.722) | 0.509 (0.488–0.53) |
| Accuracy (95% CI) | Recall (95% CI) | Precision (95% CI) | AUROC (95% CI) | F1 Score (95% CI) | |
|---|---|---|---|---|---|
| Logistic regression | 0.769 (0.764–0.775) | 0.69 (0.67–0.711) | 0.227 (0.216–0.238) | 0.733 (0.723–0.744) | 0.342 (0.328–0.355) |
| Random forest | 0.894 (0.89–0.898) | 0.574 (0.553–0.596) | 0.419 (0.4–0.438) | 0.749 (0.738–0.761) | 0.485 (0.466–0.502) |
| XG boost | 0.907 (0.904–0.911) | 0.401 (0.379–0.424) | 0.461 (0.437–0.485) | 0.678 (0.667–0.689) | 0.429 (0.408–0.449) |
| Light GBM | 0.916 (0.913–0.92) | 0.277 (0.257–0.297) | 0.537 (0.506–0.567) | 0.627 (0.617–0.637) | 0.365 (0.343–0.387) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.-H.; Cheon, B.-R.; Kim, M.-G.; Hwang, S.-M.; Lim, S.-Y.; Lee, J.-J.; Kwon, Y.-S. Harnessing Machine Learning for Prediction of Postoperative Pulmonary Complications: Retrospective Cohort Design. J. Clin. Med. 2023, 12, 5681. https://doi.org/10.3390/jcm12175681
Kim J-H, Cheon B-R, Kim M-G, Hwang S-M, Lim S-Y, Lee J-J, Kwon Y-S. Harnessing Machine Learning for Prediction of Postoperative Pulmonary Complications: Retrospective Cohort Design. Journal of Clinical Medicine. 2023; 12(17):5681. https://doi.org/10.3390/jcm12175681
Chicago/Turabian StyleKim, Jong-Ho, Bo-Reum Cheon, Min-Guan Kim, Sung-Mi Hwang, So-Young Lim, Jae-Jun Lee, and Young-Suk Kwon. 2023. "Harnessing Machine Learning for Prediction of Postoperative Pulmonary Complications: Retrospective Cohort Design" Journal of Clinical Medicine 12, no. 17: 5681. https://doi.org/10.3390/jcm12175681
APA StyleKim, J.-H., Cheon, B.-R., Kim, M.-G., Hwang, S.-M., Lim, S.-Y., Lee, J.-J., & Kwon, Y.-S. (2023). Harnessing Machine Learning for Prediction of Postoperative Pulmonary Complications: Retrospective Cohort Design. Journal of Clinical Medicine, 12(17), 5681. https://doi.org/10.3390/jcm12175681