
Influence of a Structured Microbiological Endotracheal Monitoring Program on the Outcome of Critically Ill COVID-19 Patients: An Observational Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Microbiological Screening
2.3. Data and Statistical Analysis
3. Results
3.1. Baseline Characteristics of Patients with Coinfection and VAP
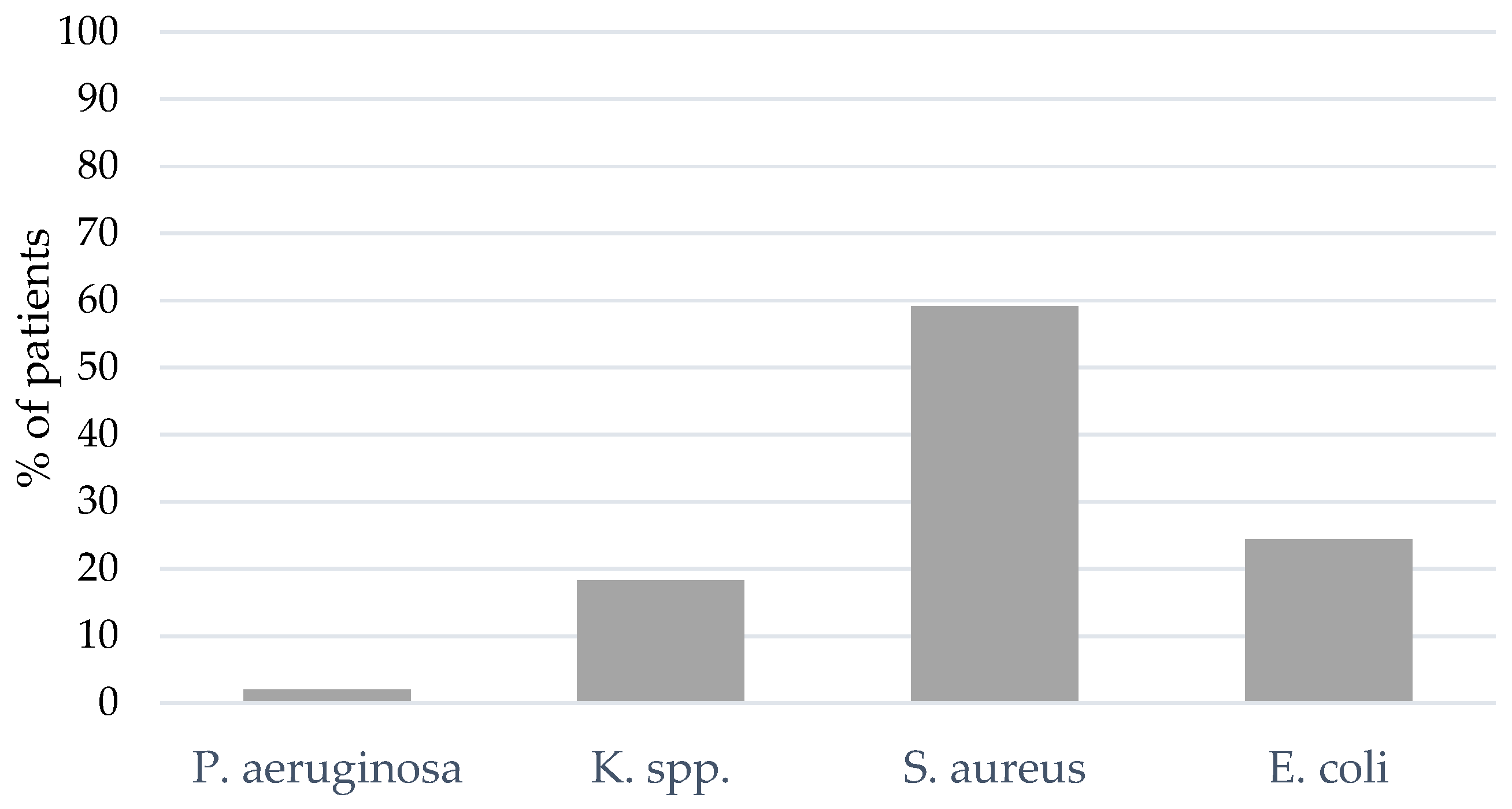
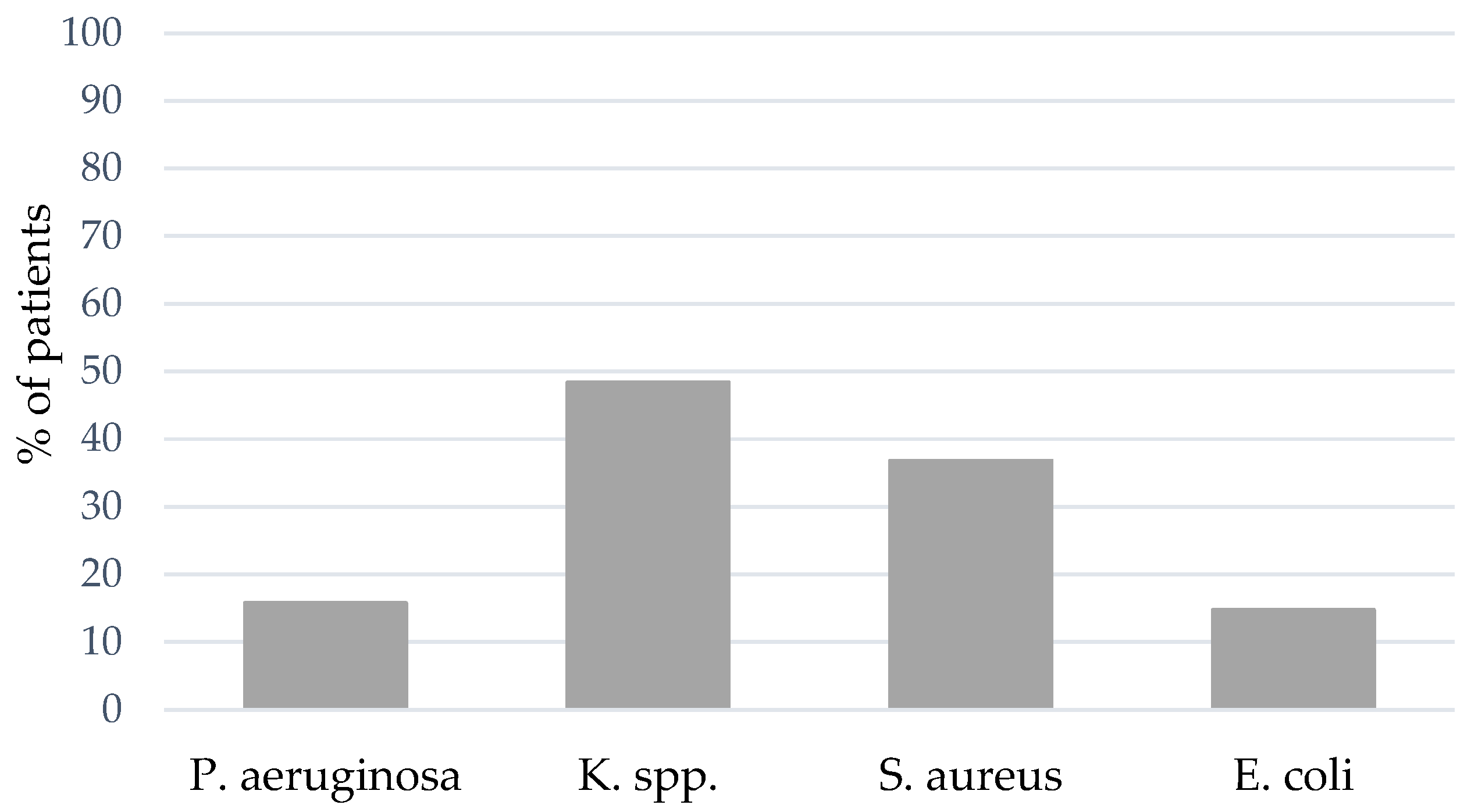
3.2. Etiology and Incidence of Coinfection and VAP
3.3. Bacterial Coinfection vs. Ventilator-Associated Pneumonia
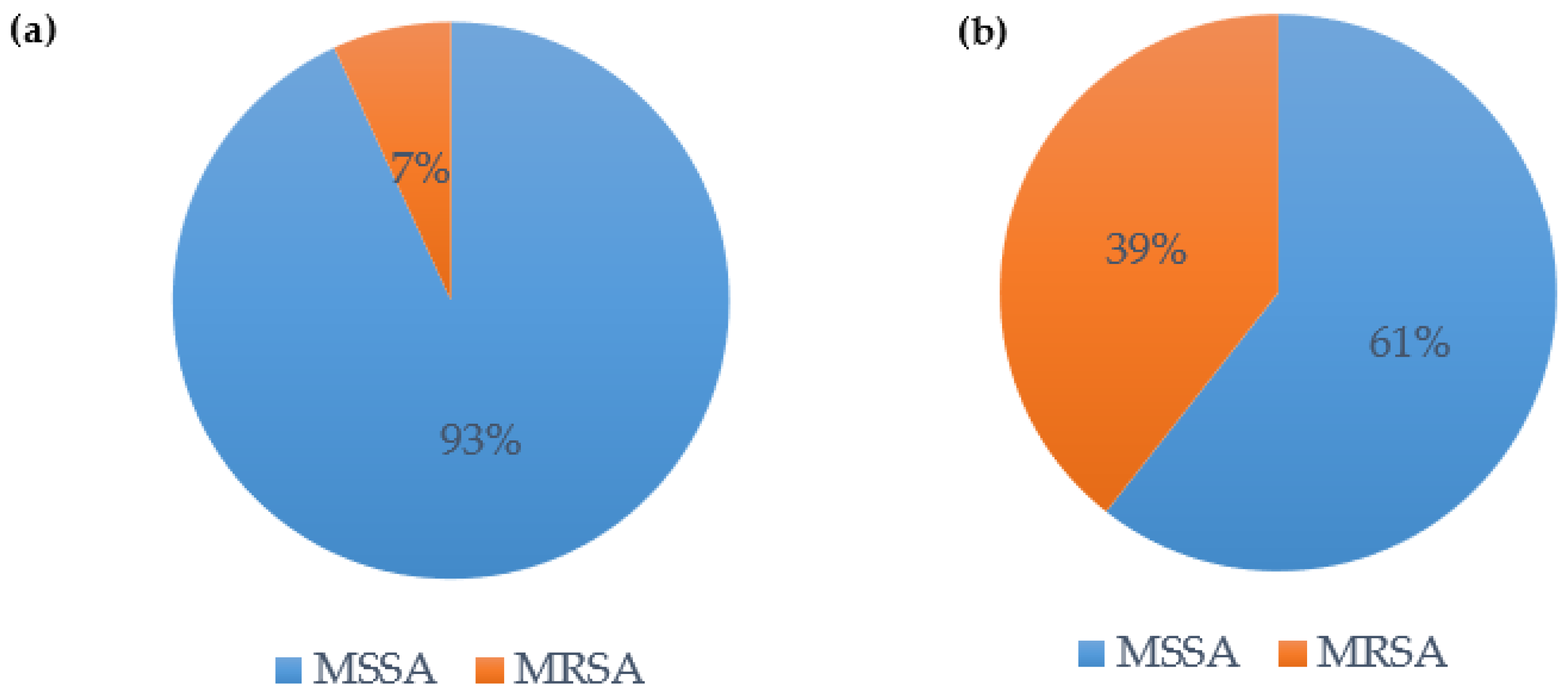
3.4. S. aureus Coinfection and Ventilator-Associated Pneumonia
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Warren, D.K.; Shukla, S.J.; Olsen, M.A.; Kollef, M.H.; Hollenbeak, C.S.; Cox, M.J.; Cohen, M.M.; Fraser, V.J. Outcome and Attributable Cost of Ventilator-Associated Pneumonia among Intensive Care Unit Patients in a Suburban Medical Center. Crit. Care Med. 2003, 31, 1312–1317. [Google Scholar] [CrossRef]
- Torres, A.; Niederman, M.S.; Chastre, J.; Ewig, S.; Fernandez-Vandellos, P.; Hanberger, H.; Kollef, M.; Bassi, G.L.; Luna, C.M.; Martin-Loeches, I.; et al. International ERS/ESICM/ESCMID/ALAT Guidelines for the Management of Hospital-Acquired Pneumonia and Ventilator-Associated Pneumonia. Eur. Respir. J. 2017, 50, 1700582. [Google Scholar] [CrossRef]
- Morens, D.M.; Taubenberger, J.K.; Fauci, A.S. Predominant Role of Bacterial Pneumonia as a Cause of Death in Pandemic Influenza: Implications for Pandemic Influenza Preparedness. J. Infect. Dis. 2008, 198, 962–970. [Google Scholar] [CrossRef] [PubMed]
- Pickens, C.O.; Gao, C.A.; Cuttica, M.J.; Smith, S.B.; Pesce, L.L.; Grant, R.A.; Kang, M.; Morales-Nebreda, L.; Bavishi, A.A.; Arnold, J.M.; et al. Bacterial Superinfection Pneumonia in Patients Mechanically Ventilated for COVID-19 Pneumonia. Am. J. Respir. Crit. Care Med. 2021, 204, 921–932. [Google Scholar] [CrossRef] [PubMed]
- Gill, J.R.; Sheng, Z.M.; Ely, S.F.; Guinee, D.G.; Beasley, M.B.; Suh, J.; Deshpande, C.; Mollura, D.J.; Morens, D.M.; Bray, M.; et al. Pulmonary Pathologic Findings of Fatal 2009 Pandemic Influenza A/H1N1 Viral Infections. Arch. Pathol. Lab. Med. 2010, 134, 235–243. [Google Scholar] [CrossRef]
- Rouzé, A.; Martin-Loeches, I.; Povoa, P.; Makris, D.; Artigas, A.; Bouchereau, M.; Lambiotte, F.; Metzelard, M.; Cuchet, P.; Boulle Geronimi, C.; et al. Relationship between SARS-CoV-2 Infection and the Incidence of Ventilator-Associated Lower Respiratory Tract Infections: A European Multicenter Cohort Study. Intensive Care Med. 2021, 47, 188–198. [Google Scholar] [CrossRef]
- Morens, D.M.; Fauci, A.S. The 1918 Influenza Pandemic: Insights for the 21st Century. J. Infect Dis. 2007, 195, 1018–1028. [Google Scholar] [CrossRef]
- Bakaletz, L.O. Viral–Bacterial Co-Infections in the Respiratory Tract. Curr. Opin. Microbiol. 2017, 35, 30–35. [Google Scholar] [CrossRef]
- Smith, A.M.; McCullers, J.A. Secondary Bacterial Infections in Influenza Virus Infection Pathogenesis. In Current Topics in Microbiology and Immunology; Springer: Berlin/Heidelberg, Germany, 2014; Volume 385, pp. 327–356. [Google Scholar]
- Bosch, A.A.T.M.; Biesbroek, G.; Trzcinski, K.; Sanders, E.A.M.; Bogaert, D. Viral and Bacterial Interactions in the Upper Respiratory Tract. PLoS Pathog. 2013, 9, e1003057. [Google Scholar] [CrossRef]
- Delhommeau, G.; Buetti, N.; Neuville, M.; Siami, S.; Cohen, Y.; Laurent, V.; Mourvillier, B.; Reignier, J.; Goldgran-Toledano, D.; Schwebel, C.; et al. Bacterial Pulmonary Co-Infections on ICU Admission: Comparison in Patients with SARS-CoV-2 and Influenza Acute Respiratory Failure: A Multicentre Cohort Study. Biomedicines 2022, 10, 2646. [Google Scholar] [CrossRef] [PubMed]
- Tetaj, N.; Capone, A.; Stazi, G.V.; Marini, M.C.; Garotto, G.; Busso, D.; Scarcia, S.; Caravella, I.; Macchione, M.; De Angelis, G.; et al. Epidemiology of Ventilator-Associated Pneumonia in ICU COVID-19 Patients: An Alarming High Rate of Multidrug-Resistant Bacteria. J. Anesth. Analg. Crit. Care 2022, 2, 36. [Google Scholar] [CrossRef] [PubMed]
- Maes, M.; Higginson, E.; Pereira-Dias, J.; Curran, M.D.; Parmar, S.; Khokhar, F.; Cuchet-Lourenço, D.; Lux, J.; Sharma-Hajela, S.; Ravenhill, B.; et al. Ventilator-Associated Pneumonia in Critically Ill Patients with COVID-19. Crit. Care 2021, 25, 25. [Google Scholar] [CrossRef]
- Kluge, S.; Strauß, R.; Kochanek, M.; Weigand, M.A.; Rohde, H.; Lahmer, T. Aspergillosis: Emerging Risk Groups in Critically Ill Patients. Med. Mycol. 2021, 60, myab064. [Google Scholar] [CrossRef] [PubMed]
- Lahmer, T.; Kriescher, S.; Herner, A.; Rothe, K.; Spinner, C.D.; Schneider, J.; Mayer, U.; Neuenhahn, M.; Hoffmann, D.; Geisler, F.; et al. Invasive Pulmonary Aspergillosis in Critically Ill Patients with Severe COVID-19 Pneumonia: Results from the Prospective AspCOVID-19 Study. PLoS ONE 2021, 16, e0238825. [Google Scholar] [CrossRef]
- Flanagan, P.G.; Barnes, R.A.; Magee, J.T.; Findlay, G.P.; Smithies, M.; Ionescu, A. The Diagnosis of Ventilator-Associated Pneumonia Using Non-Bronchoscopic, Non-Directed Lung Lavages. Intensive Care Med. 2000, 26, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Papazian, L.; Klompas, M.; Luyt, C.E. Ventilator-Associated Pneumonia in Adults: A Narrative Review. Intensive Care Med. 2020, 46, 888–906. [Google Scholar] [CrossRef] [PubMed]
- Klein, E.Y.; Monteforte, B.; Gupta, A.; Jiang, W.; May, L.; Hsieh, Y.H.; Dugas, A. The Frequency of Influenza and Bacterial Coinfection: A Systematic Review and Meta-analysis. Influenza Other Respir. Viruses 2016, 10, 394. [Google Scholar] [CrossRef]
- AWMF Leitlinienregister. Available online: https://register.awmf.org/de/leitlinien/detail/113-001LG (accessed on 8 August 2023).
- Russell, C.D.; Fairfield, C.J.; Drake, T.M.; Turtle, L.; Seaton, R.A.; Wootton, D.G.; Sigfrid, L.; Harrison, E.M.; Docherty, A.B.; de Silva, T.I.; et al. Co-Infections, Secondary Infections, and Antimicrobial Use in Patients Hospitalised with COVID-19 during the First Pandemic Wave from the ISARIC WHO CCP-UK Study: A Multicentre, Prospective Cohort Study. Lancet Microbe 2021, 2, e354–e365. [Google Scholar] [CrossRef]
- Jean, S.S.; Chang, Y.C.; Lin, W.C.; Lee, W.S.; Hsueh, P.R.; Hsu, C.W. Epidemiology, Treatment, and Prevention of Nosocomial Bacterial Pneumonia. J. Clin. Med. 2020, 9, 275. [Google Scholar] [CrossRef]
- Rothe, K.; Lahmer, T.; Rasch, S.; Schneider, J.; Spinner, C.D.; Wallnöfer, F.; Wurst, M.; Schmid, R.M.; Waschulzik, B.; Fuest, K.; et al. Dexamethasone Therapy and Rates of Secondary Pulmonary and Bloodstream Infections in Critically Ill COVID-19 Patients. Multidiscip. Respir. Med. 2021, 16, 162–169. [Google Scholar] [CrossRef]
- Rouzé, A.; Martin-Loeches, I.; Povoa, P.; Metzelard, M.; Cheyron, D.D.; Lambiotte, F.; Tamion, F.; Labruyere, M.; Geronimi, C.B.; Nieszkowska, A.; et al. Early Bacterial Identification among Intubated Patients with COVID-19 or Influenza Pneumonia: A European Multicenter Comparative Clinical Trial. Am. J. Respir. Crit. Care Med. 2021, 204, 546–556. [Google Scholar] [CrossRef] [PubMed]
- Martin-Loeches, I.; Póvoa, P.; Rodríguez, A.; Curcio, D.; Suarez, D.; Mira, J.P.; Cordero, M.L.; Lepecq, R.; Girault, C.; Candeias, C.; et al. Incidence and Prognosis of Ventilator-Associated Tracheobronchitis (TAVeM): A Multicentre, Prospective, Observational Study. Lancet Respir. Med. 2015, 3, 859–868. [Google Scholar] [CrossRef] [PubMed]
- Giacobbe, D.R.; Battaglini, D.; Enrile, E.M.; Dentone, C.; Vena, A.; Robba, C.; Ball, L.; Bartoletti, M.; Coloretti, I.; Di Bella, S.; et al. Incidence and Prognosis of Ventilator-Associated Pneumonia in Critically Ill Patients with COVID-19: A Multicenter Study. J. Clin. Med. 2021, 10, 555. [Google Scholar] [CrossRef]
- Razazi, K.; Arrestier, R.; Haudebourg, A.F.; Benelli, B.; Carteaux, G.; Decousser, J.-W.; Fourati, S.; Woerther, P.L.; Schlemmer, F.; Charles-Nelson, A.; et al. Risks of Ventilator-Associated Pneumonia and Invasive Pulmonary Aspergillosis in Patients with Viral Acute Respiratory Distress Syndrome Related or Not to Coronavirus 19 Disease. Crit. Care 2020, 24, 699. [Google Scholar] [CrossRef] [PubMed]
- Fumagalli, J.; Panigada, M.; Klompas, M.; Berra, L. Ventilator-Associated Pneumonia among SARS-CoV-2 Acute Respiratory Distress Syndrome Patients. Curr. Opin. Crit. Care 2022, 28, 74–82. [Google Scholar] [CrossRef]
- Wicky, P.H.; Niedermann, M.S.; Timsit, J.F. Ventilator-Associated Pneumonia in the Era of COVID-19 Pandemic: How Common and What Is the Impact? Crit. Care 2021, 25, 153. [Google Scholar] [CrossRef]
- Flinspach, A.N.; Booke, H.; Zacharowski, K.; Balaban, Ü.; Herrmann, E.; Adam, E.H. High Sedation Needs of Critically Ill COVID-19 ARDS Patients-A Monocentric Observational Study. PLoS ONE 2021, 16, e0253778. [Google Scholar] [CrossRef] [PubMed]
- Nseir, S.; Martin-Loeches, I.; Povoa, P.; Metzelard, M.; Du Cheyron, D.; Lambiotte, F.; Tamion, F.; Labruyere, M.; Makris, D.; Boulle Geronimi, C.; et al. Relationship between Ventilator-Associated Pneumonia and Mortality in COVID-19 Patients: A Planned Ancillary Analysis of the CoVAPid Cohort. Crit. Care 2021, 25, 177. [Google Scholar] [CrossRef]
- Luyt, C.E.; Sahnoun, T.; Gautier, M.; Vidal, P.; Burrel, S.; Pineton de Chambrun, M.; Chommeloux, J.; Desnos, C.; Arzoine, J.; Nieszkowska, A.; et al. Ventilator-Associated Pneumonia in Patients with SARS-CoV-2-Associated Acute Respiratory Distress Syndrome Requiring ECMO: A Retrospective Cohort Study. Ann. Intensive Care 2020, 10, 158. [Google Scholar] [CrossRef]
- Grasselli, G.; Scaravilli, V.; Mangioni, D.; Scudeller, L.; Alagna, L.; Bartoletti, M.; Bellani, G.; Biagioni, E.; Bonfanti, P.; Bottino, N.; et al. Hospital-Acquired Infections in Critically Ill Patients With COVID-19. Chest 2021, 160, 454–465. [Google Scholar] [CrossRef]
- Bonvento, B.V.; Rooney, J.A.; Columb, M.O.; McGrath, B.A.; Bentley, A.M.; Felton, T.W. Non-Directed Bronchial Lavage Is a Safe Method for Sampling the Respiratory Tract in Critically Ill Patient. J. Intensive Care Soc. 2019, 20, 237–241. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients | Total (169) | Coinfection (49) | VAP (95) | No Infection (45) | p-Value |
|---|---|---|---|---|---|
| Median age—years (IQR) | 63 (23) | 63 (22) | 63 (24) | 63 (19) | 0.633 |
| Male sex—% (n) | 74 (125) | 77.6 (38) | 76.8 (73) | 62.2 (28) | 0.105 |
| COVID-specific therapy—% (n) | |||||
| - Remdesivir | 11.8 (20) | 2 (1) | 15.8 (15) | 11.1 (5) | 0.607 |
| - Tocilizumab | 7.1 (12) | 14.3 (7) | 7.4 (7) | 2.2 (1) | 0.278 |
| - Monoclonal antibodies | 14.8 (25) | 20.4 (10) | 11.6 (11) | 15.6 (7) | 0.591 |
| - Corticosteroids | 81.1 (137) | 87.8 (43) | 88.4 (84) | 62.2 (28) | <0.001 (*) |
| ECMO—% (n) | 10.1 (17) | 8.2 (4) | 12.6 (12) | 8.9 (4) | 0.584 |
| Median duration of ICU stay (IQR) | 18 (21) | 17 (22) | 23 (23) | 13 (11) | <0.001 (*) |
| Median duration of hospital stay (IQR) | 26 (22) | 25 (28) | 33 (22.5) | 20 (23) | 0.002 (*) |
| Median number of ventilator days (IQR) | 15 (19) | 14 (18) | 19 (21.5) | 10 (14) | <0.001 (*) |
| Outcome | |||||
| Death—% (no.) | 43.8 (74) | 55.1 (27) | 37.9 (36) | 48.9 (22) | 0.271 |
| Coinfection | VAP | |
|---|---|---|
| Gram-negative bacteria | ||
| Pseudomonas aeruginosa | 1.1 | 8 |
| Stenotrophomonas maltophilia | 1.1 | 2.7 |
| Acinetobacter spp. (Acinetobacter pittii/dijkshoorniae + Acinetobacter baumanii) | 2.2 | 5.9 |
| Brevundimonas species (spp.) | 0 | 0.5 |
| Enterobacteriaceae | ||
| Escherichia spp. | 13.2 | 8 |
| Citrobacter spp. | 5.5 | 4.8 |
| Enterobacter spp. | 4.4 | 6.4 |
| Hafnia spp. | 1.1 | 0 |
| Morganella spp. | 14.3 | 8.5 |
| Proteus spp. | 3.3 | 4.3 |
| Serratia spp. | 5.5 | 5.3 |
| Klebsiella spp. | 9.9 | 25 |
| Haemophilus influenzae | 3.3 | 2.1 |
| Moraxella catarrhalis | 1.1 | 0 |
| Gram-positive bacteria | ||
| Staphylococcus aureus | 31.9 | 18.6 |
| Streptococcus agalactiae | 2.2 | 0 |
| Total (169) | + S. aureus (60) | − S. aureus (109) | p-Value | |
|---|---|---|---|---|
| Median age—years (IQR) | 63 (23) | 61 (20.3) | 63 (24) | 0.706 |
| Male sex—% (n) | 74 (125) | 78.3 (47) | 71.6 (78) | 0.366 |
| COVID-specific therapy—% (n) | ||||
| - Remdesivir | 11.8 (20) | 8.3 (5) | 13.8 (15) | 0.333 |
| - Tocilizumab | 7.1 (12) | 8.3 (5) | 6.4 (7) | 0.756 |
| - Monoclonal antibodies | 14.8 (25) | 16.7 (10) | 13.8 (15) | 0.654 |
| - Corticosteroids | 81.1 (137) | 88.3 (53) | 77.1 (84) | 0.1 |
| ECMO—% (n) | 10.1 (17) | 8.3 (5) | 11 (12) | 0.61 |
| Median duration of ICU stay (IQR) | 18 (21) | 22 (27.5) | 16 (18) | 0.001 (*) |
| Median duration of hospital stay (IQR) | 26 (22) | 27 (29.3) | 26 (21) | 0.171 |
| Median number of ventilator days (IQR) | 15 (19) | 15.5 (26.5) | 12 (16) | 0.025 (*) |
| Outcome | ||||
| Death—% (no.) | 43.8 (74) | 38.3 (23) | 46.8 (51) | 0.333 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dibos, M.; Haschka, S.J.; Abbassi, R.; Schneider, J.; Schmid, R.M.; Rasch, S.; Lahmer, T. Influence of a Structured Microbiological Endotracheal Monitoring Program on the Outcome of Critically Ill COVID-19 Patients: An Observational Study. J. Clin. Med. 2023, 12, 5622. https://doi.org/10.3390/jcm12175622
Dibos M, Haschka SJ, Abbassi R, Schneider J, Schmid RM, Rasch S, Lahmer T. Influence of a Structured Microbiological Endotracheal Monitoring Program on the Outcome of Critically Ill COVID-19 Patients: An Observational Study. Journal of Clinical Medicine. 2023; 12(17):5622. https://doi.org/10.3390/jcm12175622
Chicago/Turabian StyleDibos, Miriam, Stefanie Julia Haschka, Rami Abbassi, Jochen Schneider, Roland M. Schmid, Sebastian Rasch, and Tobias Lahmer. 2023. "Influence of a Structured Microbiological Endotracheal Monitoring Program on the Outcome of Critically Ill COVID-19 Patients: An Observational Study" Journal of Clinical Medicine 12, no. 17: 5622. https://doi.org/10.3390/jcm12175622
APA StyleDibos, M., Haschka, S. J., Abbassi, R., Schneider, J., Schmid, R. M., Rasch, S., & Lahmer, T. (2023). Influence of a Structured Microbiological Endotracheal Monitoring Program on the Outcome of Critically Ill COVID-19 Patients: An Observational Study. Journal of Clinical Medicine, 12(17), 5622. https://doi.org/10.3390/jcm12175622