Acceptance of Illness and Coping with Stress among Patients Undergoing Alcohol Addiction Therapy

 , , , ,
, , , ,  , , , , , , , ,
, , , , , , , ,  , and
, and  add
Show full author list
add
Show full author list
Abstract
1. Introduction
2. Materials and Methods
2.1. Material
2.2. Statistical Analysis
2.3. Descriptive Statistics
3. Results
3.1. Correlation Analysis
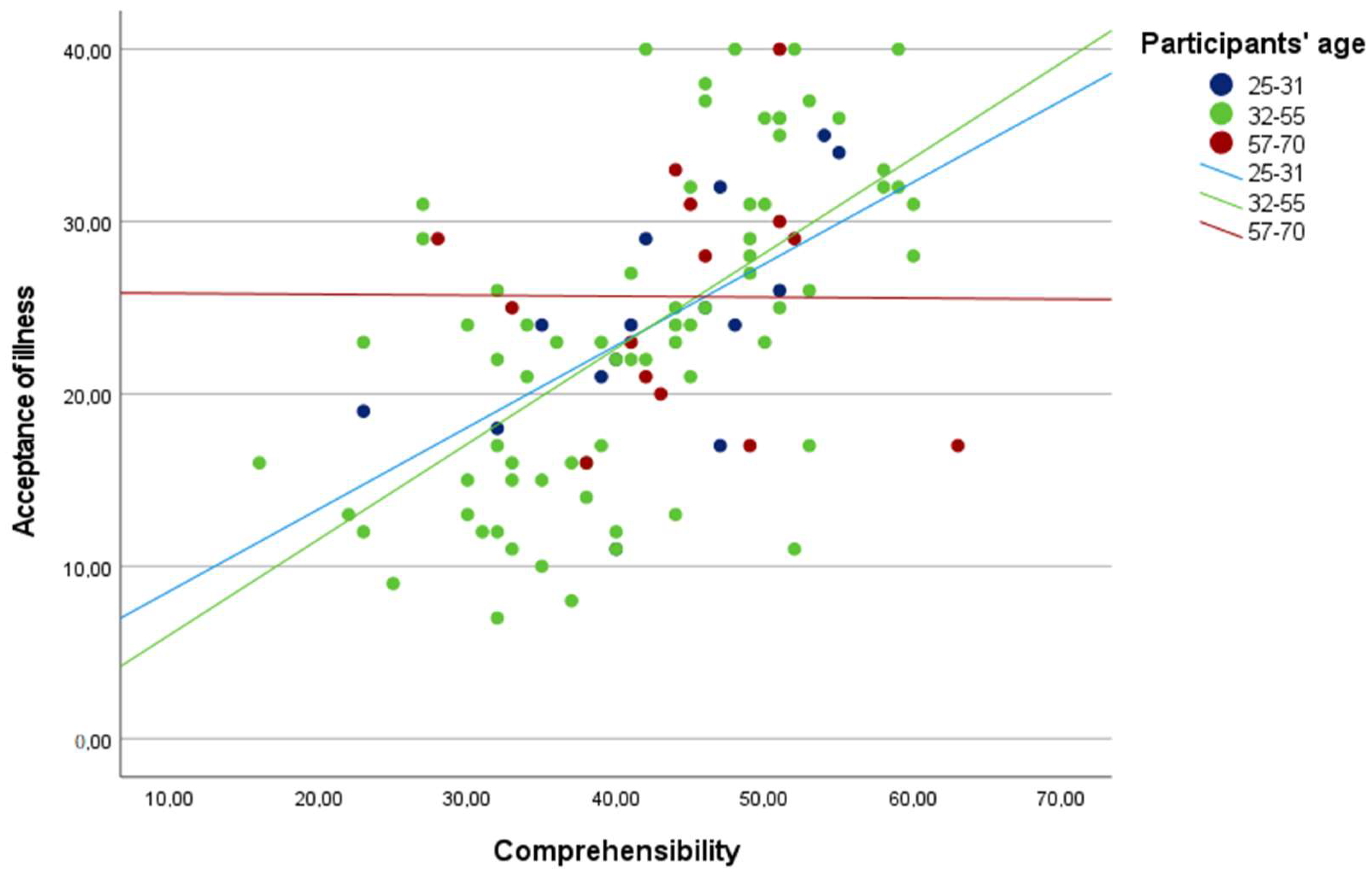
Perceived Stress and the Sense of Coherence as Predictors of Acceptance of Illness
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Alcohol. Key Facts. Available online: https://www.who.int/news-room/fact-sheets/detail/alcohol (accessed on 17 April 2023).
- Dawson, D.A.; Grant, B.F. The “gray area” of consumption between moderate and risk drinking. J. Stud. Alcohol Drugs 2011, 72, 453–458. [Google Scholar] [CrossRef] [PubMed]
- OECD. Available online: https://www.oecd-ilibrary.org/sites/33f1adaden/index.html?itemId=/content/component/33f1adad-en (accessed on 17 April 2023).
- Megari, K. Quality of Life in Chronic Disease Patients. Health Psychol. Res. 2013, 1, e27. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, S.; Bhatia, M.S. Quality of life as an outcome measure in the treatment of alcohol dependence. Ind. Psychiatry J. 2013, 22, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Kendler, K.S.; Gardner, C.; Dick, D.M. Predicting alcohol consumption in adolescence from alcohol-specific and general externalizing genetic risk factors, key environmental exposures and their interaction. Psychol. Med. 2011, 41, 1507–1516. [Google Scholar] [CrossRef] [PubMed]
- Peltzer, K.; Pengpid, S. Heavy drinking and social and health factors in university students from 24 low, middle income and emerging economy countries. Commun. Ment. Health J. 2016, 52, 239–244. [Google Scholar] [CrossRef]
- Smith, S.M.; Vale, W.W. The role of the hypothalamic-pituitary-adrenal axis in neuroendocrine responses to stress. Dialogues Clin. Neurosci. 2006, 8, 383–395. [Google Scholar] [CrossRef]
- Antonovsky, A.; Sagy, S. The development of a sense of coherence and its impact on responses to stress situations. J. Soc. Psychol. 1986, 126, 213–225. [Google Scholar]
- Quinto, R.M.; De Vincenzo, F.; Campitiello, L.; Innamorati, M.; Secinti, E.; Iani, L. Meaning in Life and the Acceptance of Cancer: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 5547. [Google Scholar] [CrossRef]
- Karademas, E.C.; Hondronikola, I. The impact of illness acceptance and helplessness to subjective health, and their stability over time: A prospective study in a sample of cardiac patients. Psychol. Health Med. 2010, 15, 336–346. [Google Scholar] [CrossRef]
- Obiegło, M.; Uchmanowicz, I.; Wleklik, M.; Jankowska-Polańska, B.; Kuśmierz, M. The effect of acceptance of illness on the quality of life in patients with chronic heart failure. Eur. J. Cardiovasc. Nurs. 2016, 15, 241–247. [Google Scholar] [CrossRef]
- Osaji, J.; Ojimba, C.; Ahmed, S. The Use of Acceptance and Commitment Therapy in Substance Use Disorders: A Review of Literature. J. Clin. Med. Res. 2020, 12, 629–633. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.F.; Urbanoski, K.A.; Hoeppner, B.B.; Slaymaker, V. Facilitating comprehensive assessment of 12-step experiences: A Multidimensional Measure of Mutual-Help Activity. Alcohol. Treat. Q. 2011, 29, 181–203. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Larm, P.; Aslund, C.; Starrin, B.; Nilsson, K.W. How are social capital and sense of coherence associated with hazardous alcohol use? Findings from a large population-based Swedish sample of adults. Scand. J. Public Health 2016, 44, 525–533. [Google Scholar] [CrossRef] [PubMed]
- Cohen, O.; Savaya, R. Sense of coherence and adjustment to divorce among Muslim Arab citizens of Israel. Eur. J. Pers. 2003, 17, 309–326. [Google Scholar] [CrossRef]
- Grevenstein, D.; Bluemke, M.; Nagy, E.; Wippermann, C.E.M.; Kroeninger-Jungaberle, H. Sense of coherence and substance use: Examining mutual influences. Personal. Individ. Differ. 2014, 64, 52–57. [Google Scholar] [CrossRef]
- Henje Blom, E.C.; Serlachius, E.; Larsson, J.O.; Theorell, T.; Ingvar, M. Low Sense of Coherence (SOC) is a mirror of general anxiety and persistent depressive symptoms in adolescent girls—A cross-sectional study of a clinical and a non-clinical cohort. Health Qual. Life Outcomes 2010, 8, 58. [Google Scholar] [CrossRef]
- Kuntsche, E.; Jordan, M.D. Adolescent alcohol and cannabis use in relation to peer and school factors: Results of multilevel analyses. Drug Alcohol Depend. 2006, 84, 167–174. [Google Scholar] [CrossRef]
- Kurpas, D.; Czech, T.; Mroczek, B. Illness acceptance in patients with diabetes and its influence on the quality of life and the subjective assessment of health. Fam. Med. Prim. Care Rev. 2012, 14, 383–388. [Google Scholar]
- Eriksson, M.; Mittelmark, M.B. The Sense of Coherence and Its Measurement. In The Handbook of Salutogenesis; Mittelmark, M.B., Sagy, S., Eriksson, M., Eds.; Springer: Cham, Switzerland, 2017. [Google Scholar]
- Golden-Kreutz, D.M.; Browne, M.W.; Frierson, G.M.; Andersen, B.L. Assessing stress in cancer patients: A second-order factor analysis model for the Perceived Stress Scale. Assessment 2004, 11, 216–223. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis, 2nd ed.; A Regression-Based Approach (Methodology in the Social Sciences); Guilford Publications: New York, NY, USA, 2018. [Google Scholar]
- Paul, A. When Can You Safely Ignore Multicollinearity? Available online: https://statisticalhorizons.com/multicollinearity (accessed on 28 June 2023).
- Mittelmark, M.B.; Sagy, S.; Eriksson, M.; Bauer, G.F.; Pelikan, J.M.; Lindström, B.; Espnes, G.A. (Eds.) The Handbook of Salutogenesis; Springer: Cham, Switzerland, 2017. [Google Scholar] [CrossRef]
- Chmielowiec, K.; Kasprzycki, A.; Grzywacz, A.; Masiak, J.; Chmielowiec, J. The level of the illness acceptance among patients of the Department of Alcohol Addiction Therapy. Pol. J. Public Health 2019, 129, 82–86. [Google Scholar] [CrossRef]
- Holgate, J.Y.; Bartlett, S.E. Early life stress, nicotinic acetylcholine receptors and alcohol use disorders. Brain Sci. 2015, 5, 258–274. [Google Scholar] [CrossRef]
- Büssing, A.; Matthiessen, P.F.; Mundle, G. Emotional and rational disease acceptance in patients with depression and alcohol addiction. Health Qual. Life Outcomes 2008, 6, 4. [Google Scholar] [CrossRef] [PubMed]
- Pompey, C.S.; Ridwan, M.N.; Zahra, A.N.; Yona, S. Illness acceptance and quality of life among end state renal disease patients undergoing hemodialysis. Enferm. Clín. 2019, 8621, 30112–30113. [Google Scholar] [CrossRef]
- Carver, C.S.; Scheier, M.F.; Weintraub, J.K. Assessing coping strategies: A theoretically based approach. J. Personal. Soc. Psychol. 1989, 56, 267–283. [Google Scholar] [CrossRef] [PubMed]
- Silverstein, M.; Heap, J. Sense of coherence changes with aging over the second half of life. Adv. Life Course Res. 2015, 23, 98–107. [Google Scholar] [CrossRef]
- Sierakowska, M.; Wysocka-Skurska, I.; Kułak, W. Identification of demographic factors and health problems that affect the acceptance of disease and health behaviors of patients with osteoarthritis. PeerJ 2017, 5, e3276. [Google Scholar] [CrossRef] [PubMed]
- Pankowski, D.; Wytrychiewicz-Pankowska, K.; Pisula, E.; Fal, A.; Kisiel, B.; Kamińska, E.; Tłustochowicz, W. Age, Cognitive Factors, and Acceptance of Living with the Disease in Rheumatoid Arthritis: The Short-Term Perspective. Int. J. Environ. Res. Public Health 2022, 19, 3136. [Google Scholar] [CrossRef]
- Amirkhan, J.; Greaves, H. Sense of Coherence and Stress: The Mechanics of a Healthy Disposition. Psychol. Health 2003, 18, 31–62. [Google Scholar] [CrossRef]
- Betke, K.; Basińska, M.A.; Andruszkiewicz, A. Sense of coherence and strategies for coping with stress among nurses. BMC Nurs. 2021, 20, 107. [Google Scholar] [CrossRef]
- Ramchandani, V.A.; Stangl, B.L.; Blaine, S.K.; Plawecki, M.H.; Schwandt, M.L.; Kwako, L.E.; Sinha, R.; Cyders, M.A.; O’Connor, S.; Zakhari, S. Stress vulnerability and alcohol use and consequences: From human laboratory studies to clinical outcomes. Alcohol 2018, 72, 75–88. [Google Scholar] [CrossRef]
- Becker, H.C. Influence of stress associated with chronic alcohol exposure on drinking. Neuropharmacology 2017, 122, 115–126. [Google Scholar] [CrossRef] [PubMed]
- Mattila, M.; Rautava, P.; Honkinen, P.; Ojanlatva, A.; Jaakkola, S.; Aromaa, M.; Suominen, S.; Helenius, H.; Sillanpää, M. Sense of coherence and health behaviour in adolescence. Acta Paediatr. 2011, 100, 1590–1595. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, C.A.; Ryan, P.; Foster, J.H. Thematic analysis of Antonovsky’s sense of coherence theory. Scand. J. Psychol 2011, 52, 168–173. [Google Scholar] [CrossRef]
- Dijkstra, A.; Buunk, A.P.; Tóth, G.; Jager, N. Psychological adjustment to chronic illness: The role of prototype evaluation in acceptance of illness. J. Appl. Biobehav. Res. 2008, 12, 119–140. [Google Scholar] [CrossRef]


{kind=link}
| Variables | M | SD | min | max | S | K | α |
|---|---|---|---|---|---|---|---|
| Perceived stress | 21.79 | 6.92 | 4 | 38 | −0.24 | −0.29 | 0.87 |
| Comprehensibility | 42.20 | 9.97 | 16 | 63 | −0.27 | −0.44 | 0.78 |
| Manageability | 45.39 | 9.06 | 26 | 65 | −0.05 | −0.40 | 0.75 |
| Meaningfulness | 39.90 | 8.42 | 13 | 56 | −0.69 | 0.41 | 0.79 |
| Sense of coherence | 127.50 | 23.13 | 63 | 176 | −0.25 | −0.30 | 0.89 |
| Acceptance of illness | 24.05 | 8.62 | 7 | 40 | 0.07 | −0.82 | 0.87 |
| Variables | Perceived Stress | Comprehensibility | Manageability | Meaningfulness | Sense of Coherence | Acceptance of Illness |
|---|---|---|---|---|---|---|
| Perceived stress | - | - | - | - | - | - |
| Comprehensibility | −0.576 ** | - | - | - | - | - |
| Manageability | −0.548 ** | 0.666 ** | - | - | - | - |
| Meaningfulness | −0.419 ** | 0.485 ** | 0.528 ** | - | - | - |
| Sense of coherence | −0.616 ** | 0.869 ** | 0.871 ** | 0.780 ** | - | - |
| Acceptance of illness | −0.439 ** | 0.502 ** | 0.479 ** | 0.346 ** | 0.530 ** | - |
| Age | −0.102 | 0.024 | 0.077 | 0.031 | 0.051 | 0.005 |
| Dependent Variable | Predictors | B | t | p | ΔR2 |
|---|---|---|---|---|---|
| Acceptance of illness | Sense of coherence | 0.58 | 6.83 | 0.001 | 0.33 |
| Interaction Effects | B | t | p |
|---|---|---|---|
| Perceived stress x Age | −0.02 | −0.16 | 0.874 |
| Comprehensibility x Age | −0.21 | −2.19 | 0.031 |
| Manageability x Age | −0.06 | −0.64 | 0.522 |
| Meaningfulness x Age | 0.01 | 0.02 | 0.985 |
| Sense of coherence x Age | −0.09 | −1.00 | 0.321 |
| z | B | t | p |
|---|---|---|---|
| −1.68 | 0.93 | 5.01 | 0.001 |
| −1.47 | 0.89 | 5.27 | 0.001 |
| −1.26 | 0.84 | 5.57 | 0.001 |
| −1.04 | 0.80 | 5.91 | 0.001 |
| −0.83 | 0.76 | 6.28 | 0.001 |
| −0.62 | 0.72 | 6.66 | 0.001 |
| −0.41 | 0.67 | 6.99 | 0.001 |
| −0.19 | 0.63 | 7.15 | 0.001 |
| 0.02 | 0.59 | 7.01 | 0.001 |
| 0.23 | 0.54 | 6.49 | 0.001 |
| 0.45 | 0.50 | 5.67 | 0.001 |
| 0.66 | 0.46 | 4.73 | 0.001 |
| 0.87 | 0.42 | 3.84 | 0.001 |
| 1.09 | 0.37 | 3.06 | 0.003 |
| 1.30 | 0.33 | 2.41 | 0.018 |
| 1.46 | 0.30 | 1.99 | 0.050 |
| 1.51 | 0.29 | 1.88 | 0.064 |
| 1.72 | 0.24 | 1.44 | 0.154 |
| 1.94 | 0.20 | 1.07 | 0.286 |
| 2.15 | 0.16 | 0.77 | 0.444 |
| 2.36 | 0.11 | 0.51 | 0.609 |
| 2.58 | 0.07 | 0.30 | 0.768 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Curyło, M.; Rynkiewicz-Andryśkiewicz, M.; Andryśkiewicz, P.; Mikos, M.; Lusina, D.; Raczkowski, J.W.; Partyka, O.; Pajewska, M.; Sygit, K.; Sygit, M.; et al. Acceptance of Illness and Coping with Stress among Patients Undergoing Alcohol Addiction Therapy. J. Clin. Med. 2023, 12, 4767. https://doi.org/10.3390/jcm12144767
Curyło M, Rynkiewicz-Andryśkiewicz M, Andryśkiewicz P, Mikos M, Lusina D, Raczkowski JW, Partyka O, Pajewska M, Sygit K, Sygit M, et al. Acceptance of Illness and Coping with Stress among Patients Undergoing Alcohol Addiction Therapy. Journal of Clinical Medicine. 2023; 12(14):4767. https://doi.org/10.3390/jcm12144767
Chicago/Turabian StyleCuryło, Mateusz, Marlena Rynkiewicz-Andryśkiewicz, Przemysław Andryśkiewicz, Marcin Mikos, Dariusz Lusina, Jan W. Raczkowski, Olga Partyka, Monika Pajewska, Katarzyna Sygit, Marian Sygit, and et al. 2023. "Acceptance of Illness and Coping with Stress among Patients Undergoing Alcohol Addiction Therapy" Journal of Clinical Medicine 12, no. 14: 4767. https://doi.org/10.3390/jcm12144767
APA StyleCuryło, M., Rynkiewicz-Andryśkiewicz, M., Andryśkiewicz, P., Mikos, M., Lusina, D., Raczkowski, J. W., Partyka, O., Pajewska, M., Sygit, K., Sygit, M., Cipora, E., Kaczmarski, M., Gawiński, Ł., Banaś, T., Strzępek, Ł., Juszczyk, G., Krzych-Fałta, E., Bandurska, E., Ciećko, W., ... Kozłowski, R. (2023). Acceptance of Illness and Coping with Stress among Patients Undergoing Alcohol Addiction Therapy. Journal of Clinical Medicine, 12(14), 4767. https://doi.org/10.3390/jcm12144767