
Unresolved Issues Associated with Transcranial Magnetic Stimulation (TMS) Treatment of Chronic Tinnitus

Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. rTMS Equipment
- Type/Brand of TMS System and Its Configuration.
- Coil Type
- Coil Orientation
3.2. Coil Placement/Scalp Target
- Temporal Lobe Stimulation
- Neuronavigation vs. Coil Placement via Scalp Landmarks
- Frontal/Dual Site Stimulation
- Laterality of rTMS Application
3.3. Stimulation Parameters
- Stimulation Frequency and Number of Pulses Per Session
- Number of Sessions
- Stimulation Intensity and Determination of Resting Motor Threshold (rMT).
- Placebo/Sham Control Condition and Blinding
3.4. Characteristics of the Study Population
- Study Population Size
- Etiology of Tinnitus
- Duration of Tinnitus
- Tinnitus Severity
- Responders in the Active rTMS group: 51.4 std dev 18.4 (n = 18 of 32)
- Responders in the Sham rTMS group: 55.0 std dev 22.2 (n = 7 of 32)
- Non-Responders in the Active rTMS group: 36.3 std dev 17.6 (n = 14 of 32)
- Non-Responders in the Sham rTMS group: 36.6 std dev 20.7 (n = 25 of 32)
- Age of Study Participants
- Co-Occurring Conditions
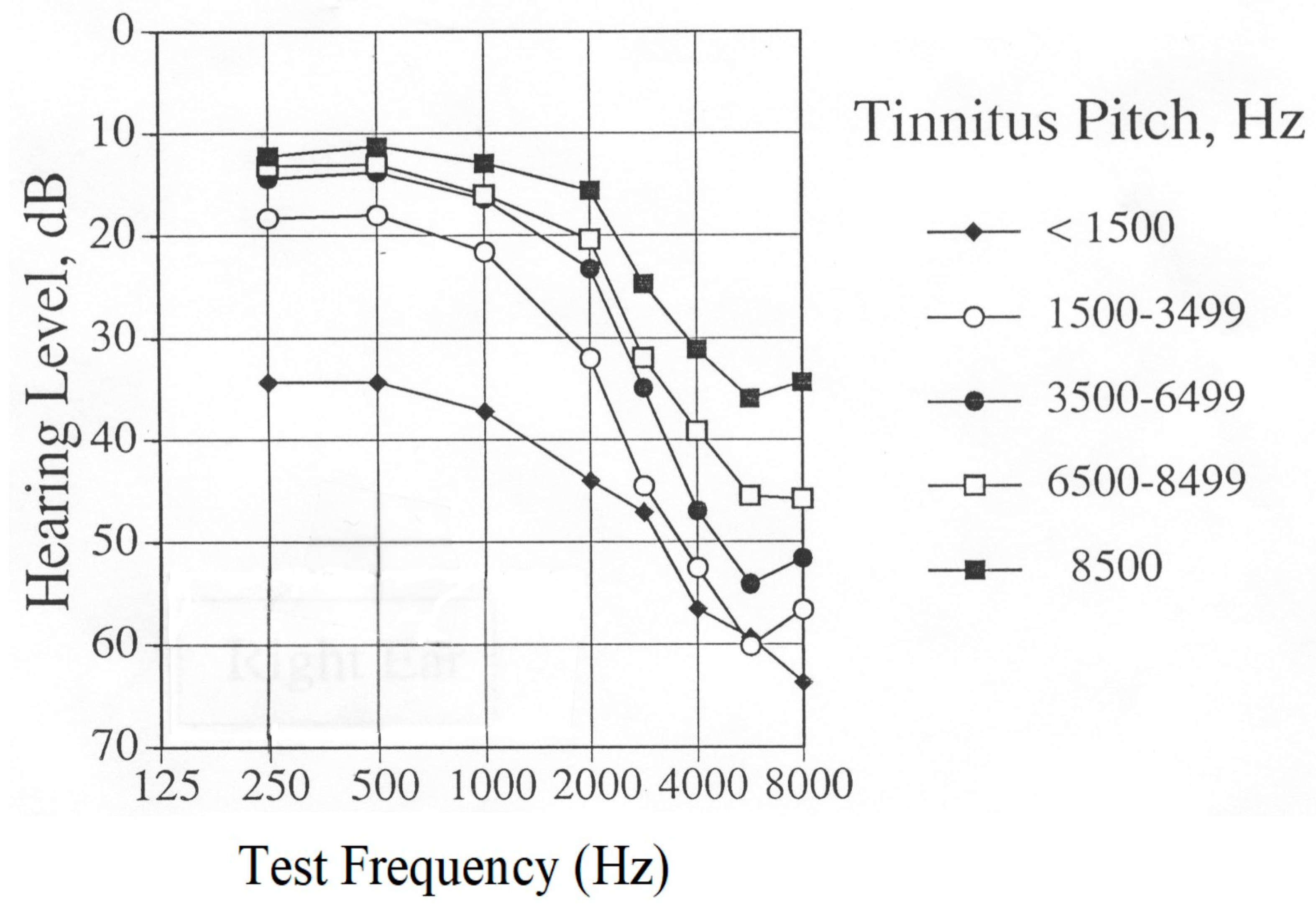
- Hearing Sensitivity of Participants
3.5. Outcome Measures and Follow Up
- Follow up
4. Discussion
Funding
Acknowledgments
Conflicts of Interest
References
- Folmer, R.L.; Griest, S.E.; Meikle, M.B.; Martin, W.H. Tinnitus severity, loudness and depression. Otolaryngol. Head Neck Surg. 1999, 121, 48–51. [Google Scholar] [CrossRef] [PubMed]
- Folmer, R.L.; Griest, S.E. Tinnitus and insomnia. Am. J. Otolaryngol. 2000, 21, 287–293. [Google Scholar] [CrossRef]
- Folmer, R.L.; Griest, S.E.; Martin, W.H. Chronic tinnitus as phantom auditory pain. Otolaryngol. Head Neck Surg. 2001, 124, 394–400. [Google Scholar] [CrossRef]
- Folmer, R.L.; Griest, S.E. Chronic tinnitus resulting from head or neck injuries. Laryngoscope 2003, 113, 821–827. [Google Scholar] [CrossRef] [PubMed]
- Folmer, R.L.; Martin, W.H.; Shi, Y. Tinnitus: Questions to reveal the cause, answers to provide relief. J. Fam. Pract. 2004, 53, 532–540. [Google Scholar]
- Folmer, R.L. Ringing-in-the-Ears: Hope and Help for Tinnitus Sufferers. Hear. Health 2006, 22, 42–45. [Google Scholar]
- Folmer, R.L.; Griest, S.E.; Martin, W.H. Obsessive-Compulsiveness in a Population of Tinnitus Patients. Int. Tinnitus J. 2008, 14, 127–130. [Google Scholar]
- Folmer, R.L.; McMillan, G.P.; Austin, D.F.; Henry, J.A. Audiometric thresholds and prevalence of tinnitus among male Veterans in the United States: Data from the National Health and Nutrition Examination Survey, 1999–2006. J. Rehabil. Res. Dev. 2011, 48, 503–516. [Google Scholar] [CrossRef]
- Folmer, R.L. Implants Can Improve Tinnitus, But Most Offer No Quick Fixes. Hear. J. 2012, 65, 42–48. [Google Scholar] [CrossRef]
- Folmer, R.L.; Theodoroff, S.M.; Martin, W.H.; Shi, Y.B. Experimental, Controversial and Futuristic Treatments for Chronic Tinnitus. J. Am. Acad. Audiol. 2014, 25, 106–125. [Google Scholar] [CrossRef]
- Theodoroff, S.M.; Lewis, M.S.; Folmer, R.L.; Henry, J.A.; Carlson, K.F. Hearing Impairment and Tinnitus: Prevalence, Risk Factors, and Outcomes in US Service Members and Veterans Deployed to Iraq and Afghanistan Wars. Epidemiol. Rev. 2015, 37, 71–85. [Google Scholar] [CrossRef] [PubMed]
- Folmer, R.L.; Carroll, J.R. Long-term effectiveness of ear-level devices for tinnitus. Otolaryngol. Head Neck Surg. 2006, 134, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Eichhammer, P.; Langguth, B.; Marienhagen, J.; Kleinjung, T.; Hajak, G. Neuronavigated repetitive transcranial magnetic stimulation in patients with tinnitus: A short case series. Biol. Psychiatry 2003, 54, 862–865. [Google Scholar] [CrossRef]
- Langguth, B.; Eichhammer, P.; Wiegand, R.; Marienhegen, J.; Maenner, P.; Jacob, P.; Hajak, G. Neuronavigated rTMS in a patient with chronic tinnitus. Effects of 4 weeks treatment. Neuroreport 2003, 14, 977–980. [Google Scholar] [CrossRef]
- Theodoroff, S.M.; Folmer, R.L. Repetitive Transcranial Magnetic Stimulation as a Treatment for Chronic Tinnitus: A Critical Review. Otol. Neurotol. 2013, 34, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Soleimani, R.; Jalali, M.M.; Hasandokht, T. Therapeutic impact of repetitive transcranial magnetic stimulation (rTMS) on tinnitus: A systematic review and meta-analysis. Eur. Arch. Otorhinolaryngol. 2016, 273, 1663–1675. [Google Scholar] [CrossRef] [PubMed]
- Liang, Z.; Yang, H.; Cheng, G.; Huang, L.; Zhang, T.; Jia, H. Repetitive transcranial magnetic stimulation on chronic tinnitus: A systematic review and meta-analysis. BMC Psychiatry 2020, 20, 547. [Google Scholar] [CrossRef]
- Chen, J.-J.; Zeng, B.-S.; Wu, C.-N.; Stubbs, B.; Carvalho, A.F.; Brunoni, A.R.; Su, K.-P.; Tu, Y.-K.; Wu, Y.-C.; Chen, T.-Y.; et al. Association of Central Noninvasive Brain Stimulation Interventions with Efficacy and Safety in Tinnitus Management: A Meta-analysis. JAMA Otolaryngol. Head Neck Surg. 2020, 146, 801–809. [Google Scholar] [CrossRef]
- Yin, L.; Chen, X.; Lu, X.; An, Y.; Zhang, T.; Yan, J. An updated meta-analysis: Repetitive transcranial magnetic stimulation for treating tinnitus. J. Int. Med. Res. 2021, 49, 300060521999549. [Google Scholar] [CrossRef]
- Arnold, W.; Bartenstein, P.; Oestreicher, E.; Romer, W.; Schwaiger, M. Focal metabolic activation in the predominant left auditory cortex in patients suffering from tinnitus: A PET study with [18F]deoxyglucose. ORL 1996, 58, 195–199. [Google Scholar] [CrossRef]
- Lockwood, A.H.; Salvi, R.J.; Coad, M.L.; Towsley, M.L.; Wach, D.S.; Murphy, B.W. The functional neuroanatomy of tinnitus: Evidence for limbic system links and neuroplasticity. Neurology 1998, 50, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Folmer, R.L. Lateralization of Neural Activity Associated with Tinnitus. Neuroradiology 2007, 49, 689–691. [Google Scholar] [CrossRef] [PubMed]
- Maudoux, A.; Lefebvre, P.; Cabay, J.E.; Demertzi, A.; Vanhaudenhuyse, A.; Laureys, S.; Soddu, A. Auditory resting-state network connectivity in tinnitus: A functional MRI study. PLoS ONE 2012, 7, e36222. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, S.A.; Akrofi, K.; Carpenter-Thompson, J.R.; Husain, F.T. Default mode, dorsal attention and auditory resting state networks exhibit differential functional connectivity in tinnitus and hearing loss. PLoS ONE 2013, 8, e76488. [Google Scholar] [CrossRef]
- Elgoyhen, A.B.; Langguth, B.; De Ridder, D.; Vanneste, S. Tinnitus: Perspectives from human neuroimaging. Nat. Rev. Neurosci. 2015, 16, 632–642. [Google Scholar] [CrossRef]
- Chen, Y.C.; Xia, W.; Chen, H.; Feng, Y.; Xu, J.J.; Gu, J.P.; Salvi, R.; Yin, X. Tinnitus distress is linked to enhanced resting-state functional connectivity from the limbic system to the auditory cortex. Hum. Brain Mapp. 2017, 38, 2384–2397. [Google Scholar] [CrossRef]
- Husain, F.T. Neural networks of tinnitus in humans: Elucidating severity and habituation. Hear Res. 2016, 334, 37–48. [Google Scholar] [CrossRef]
- Folmer, R.L.; Theodoroff, S.M.; Casiana, L.; Shi, Y.B.; Griest, S.E.; Vachhani, J. Repetitive Transcranial Magnetic Stimulation Treatment for Chronic Tinnitus: A Randomized Clinical Trial. JAMA Otolaryngol. Head Neck Surg. 2015, 141, 716–722. [Google Scholar] [CrossRef]
- Langguth, B.; de Ridder, D.; Dornhoffer, J.L.; Eichhammer, P.; Folmer, R.L.; Frank, E.; Fregni, F.; Gerloff, C.; Khedr, E.; Kleinjung, T.; et al. Controversy: Does repetitive transcranial magnetic stimulation/ transcranial direct current stimulation show efficacy in treating tinnitus patients? Brain Stimul. 2008, 1(3), 192–205. [Google Scholar] [CrossRef]
- Piccirillo, J.F. Transcranial Magnetic Stimulation for Chronic Tinnitus. JAMA 2016, 315, 506–507. [Google Scholar] [CrossRef]
- Mennemeier, M.; George, M. The Case for a Definitive Multisite, Randomized Clinical Trial of Repetitive Transcranial Magnetic Stimulation for Tinnitus. JAMA Otolaryngol. Head Neck Surg. 2017, 143, 441–442. [Google Scholar] [CrossRef] [PubMed]
- Piccirillo, J.F.; Kallogjeri, D.; Nicklaus, J.; Wineland, A.; Spitznagel, E.L.; Vlassenko, A.G.; Benzinger, T.; Mathews, J.; Garcia, K.S. Low-Frequency Repetitive Transcranial Magnetic Stimulation to the Temporoparietal Junction for Tinnitus: Four-Week Stimulation Trial. JAMA Otolaryngol. Head Neck Surg. 2013, 139, 388–395. [Google Scholar] [CrossRef]
- Landgrebe, M.; Hajak, G.; Wolf, S.; Padberg, F.; Klupp, P.; Fallgatter, A.J.; Polak, T.; Höppner, J.; Haker, R.; Cordes, J.; et al. 1-Hz rTMS in the treatment of tinnitus: A sham-controlled, randomized multicenter trial. Brain Stimul. 2017, 10, 1112–1120. [Google Scholar] [CrossRef] [PubMed]
- Schoisswohl, S.; Langguth, B.; Weber, F.C.; Abdelnaim, M.A.; Hebel, T.; Mack, W.; Schecklmann, M. One way or another: Treatment effects of 1 Hz rTMS using different current directions in a small sample of tinnitus patients. Neurosci. Lett. 2023, 797, 137026. [Google Scholar] [CrossRef]
- Pell, G.S.; Zangen, A.; Roth, Y.; Shachar, H.; Isserles, M.; Barnea-Ygael, N. Behavioral and Functional Brain Activity Alterations Induced by TMS Coils with Different Spatial Distributions. eNeuro 2023, 10, 1–11. [Google Scholar] [CrossRef]
- Ilmoniemi, R.J.; Deng, Z.-D.; Gomez, L.; Koponen, L.M.; Nieminen, J.O.; Peterchev, A.V.; Epstein, C.M. Transcranial magnetic stimulation coils. In The Oxford Handbook of Transcranial Stimulation, 2nd ed.; Wassermann, E.M., Peterchev, A.V., Ziemann, U., Lisanby, S.H., Siebner, H.R., Walsh, V., Eds.; Oxford University Press: Oxford, UK, 2021. [Google Scholar]
- Langguth, B.; Zowe, M.; Landgrebe, M.; Sand, P.; Kleinjung, T.; Binder, H.; Hajak, G.; Eichhammer, P. Transcranial Magnetic Stimulation for the treatment of tinnitus: A new coil positioning method and first results. Brain Topogr. 2006, 18, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Khedr, E.M.; Rothwell, J.C.; Ahmed, M.A.; El-Atar, A. Effect of daily repetitive transcranial magnetic stimulation for treatment of tinnitus: Comparison of different stimulus frequencies. J. Neurol. Neurosurg. Psychiatry 2008, 79, 212–215. [Google Scholar] [CrossRef]
- Noh, T.-S.; Rah, Y.-C.; Kyong, J.S.; Kim, J.S.; Park, M.K.; Lee, J.H.; Oh, S.H.; Chung, C.K.; Suh, M.-W. Comparison of treatment outcomes between 10 and 20 EEG electrode location system-guided and neuronavigation-guided repetitive transcranial magnetic stimulation in chronic tinnitus patients and target localization in the Asian brain. Acta Oto-Laryngol. 2017, 137, 945–951. [Google Scholar] [CrossRef]
- Langguth, B.; Landgrebe, M.; Frank, E.; Schecklmann, M.; Sand, P.G.; Vielsmeier, V.; Hajak, G.; Kleinjung, T. Efficacy of different protocols of transcranial magnetic stimulation for the treatment of tinnitus: Pooled analysis of two randomized controlled studies. World J. Biol. Psychiatry 2014, 15, 276–285. [Google Scholar] [CrossRef]
- Formanek, M.; Migalova, P.; Krulova, P.; Bar, M.; Jancatova, D.; Zakopcanova-Srovnalova, H.; Tomášková, H.; Zeleník, K.; Komínek, P. Combined transcranial magnetic stimulation in the treatment of chronic tinnitus. Ann. Clin. Transl. Neurol. 2018, 5, 857–864. [Google Scholar] [CrossRef]
- Noh, T.-S.; Kyong, J.-S.; Park, M.K.; Lee, J.H.; Oh, S.H.; Suh, M.-W. Dual-site rTMS is More Effective than Single-site rTMS in Tinnitus Patients: A Blinded Randomized Controlled Trial. Brain Topogr. 2020, 33, 767–775. [Google Scholar] [CrossRef]
- Poeppl, T.B.; Schecklmann, M.; Sakreida, K.; Landgrebe, M.; Langguth, B.; Eickhoff, S.B. Prediction of response to repetitive transcranial magnetic stimulation in phantom sounds based on individual brain anatomy. Brain Commun 2021, 3, fcab115. [Google Scholar] [CrossRef] [PubMed]
- Marder, K.G.; Cho, J.; Chincanchan, R.; Wilson, A.C.; Corlier, J.; Krantz, D.E.; Ginder, N.D.; Lee, J.C.; Wilke, S.A.; Tadayonnejad, R.; et al. Sequential Prefrontal and Temporoparietal Repetitive Transcranial Magnetic Stimulation (rTMS) for Treatment of Tinnitus with and Without Comorbid Depression: A Case Series and Systematic Review. Front. Neurol. 2022, 13, 831832. [Google Scholar] [CrossRef] [PubMed]
- Frank, G.; Kleinjung, T.; Landgrebe, M.; Vielsmeier, V.; Steffenhagen, C.; Burger, J.; Frank, E.; Vollberg, G.; Hajak, G.; Langguth, B. Left temporal low frequency rTMS for the treatment of tinnitus: Clinical predictors of treatment outcome—A retrospective study. Eur. J. Neurol. 2010, 17, 951–956. [Google Scholar] [CrossRef]
- Chen, R.; Classen, J.; Gerloff, C.; Celnik, P.; Wassermann, E.M.; Hallett, M.; Cohen, L.G. Depression of motor cortex excitability by low-frequency transcranial magnetic stimulation. Neurology 1997, 48, 1398–1403. [Google Scholar] [CrossRef]
- Ring, A.; Crowder, C.; Wyer, S.L.; Phillips, B. A Chart Review to Assess the Response of Veterans Suffering from Tinnitus to Alpha Burst Transcranial Magnetic Stimulation. Int. Tinnitus J. 2020, 24, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.-M.; Kim, S.-K.; Seo, M.-Y.; Kang, S.-Y. Multiple Daily Rounds of Theta-Burst Stimulation for Tinnitus: Preliminary Results. Medicina 2021, 57, 743. [Google Scholar] [CrossRef]
- Godbehere, J.; Sandhu, J.; Evans, A.; Twigg, V.; Scivill, I.; Ray, J.; Barker, A. Treatment of Tinnitus Using Theta Burst Based Repetitive Transcranial Magnetic Stimulation -- A Single Blinded Randomized Control Trial. Otol. Neurotol. 2019, 40, S38–S42. [Google Scholar] [CrossRef]
- Kleinjung, T.; Eichhammer, P.; Langguth, B.; Jacob, P.; Marienhagen, J.; Hajak, G.; Wolf, S.R.; Strutz, J. Long-term effects of repetitive transcranial magnetic stimulation (rTMS) in patients with chronic tinnitus. Otolaryngol. Head Neck Surg. 2005, 132, 566–569. [Google Scholar] [CrossRef]
- Rossi, S.; De Capua, A.; Ulivelli, M.; Bartalini, S.; Falzarano, V.; Filippone, G.; Passero, S. Effects of repetitive transcranial magnetic stimulation on chronic tinnitus: A randomised, cross over, double blind, placebo-controlled study. J. Neurol. Neurosurg. Psychiatry 2007, 78, 857–863. [Google Scholar] [CrossRef] [PubMed]
- Plewnia, C.; Bartels, M.; Gerloff, C. Transient suppression of tinnitus by transcranial magnetic stimulation. Ann Neurol. 2003, 53, 263–266. [Google Scholar] [CrossRef]
- Herbsman, T.; Avery, D.; Ramsey, D.; Holtzheimer, P.; Wadjik, C.; Hardaway, F.; Haynor, F.; George, M.S.; Nahas, Z. More lateral and anterior prefrontal coil location is associated with better repetitive transcranial magnetic stimulation antidepressant response. Biol. Psychiatry 2009, 66, 509–515. [Google Scholar] [CrossRef]
- Yesavage, J.A.; Fairchild, J.K.; Mi, Z.; Biswas, K.; Davis-Karim, A.; Phibbs, C.S.; Forman, S.D.; Thase, M.; Williams, L.M.; Etkin, A.; et al. Effect of repetitive transcranial magnetic stimulation on treatment-resistant major depression in US Veterans: A randomized clinical trial. JAMA Psychiatry 2018, 75, 884–893. [Google Scholar] [CrossRef]
- Cole, E.J.; Phillips, A.L.; Bentzley, B.S.; Stimpson, K.H.; Nejad, R.; Barmak, F.; Veerapal, C.; Khan, N.; Cherian, K.; Felber, E.; et al. Stanford Neuromodulation Therapy (SNT): A Double-Blind Randomized Controlled Trial. Am. J. Psychiatry 2022, 179, 132–141. [Google Scholar] [CrossRef]
- Dobie, R.A. A review of randomized clinical trials in tinnitus. Laryngoscope 1999, 109, 1202–1211. [Google Scholar] [CrossRef] [PubMed]
- Folmer, R.L.; Carroll, J.R.; Rahim, A.; Shi, Y.; Martin, W.H. Effects of Repetitive Transcranial Magnetic Stimulation (rTMS) on Chronic Tinnitus. Acta Otolaryngol. 2006, 126, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Anders, M.; Dvorakova, J.; Rathova, L.; Havrankova, P.; Pelcova, P.; Vaneckova, M.; Jech, R.; Holcat, M.; Seidl, Z.; Raboch, J. Efficacy of repetitive transcranial magnetic stimulation for the treatment of refractory chronic tinnitus: A randomized, placebo controlled study. Neuro Endocrinol. Lett. 2010, 31, 238–249. [Google Scholar] [PubMed]
- Khedr, E.M.; Rothwell, J.C.; El-Atar, A. One-year follow up of patients with chronic tinnitus treated with left temporoparietal rTMS. Eur. J. Neurol. 2009, 16, 404–408. [Google Scholar] [CrossRef] [PubMed]
- Vanneste, S.; Plazier, M.; van der Loo, E.; Ost, J.; Van de Heyning, P.; De Ridder, D. Burst transcranial magnetic stimulation: Which tinnitus characteristics influence the amount of transient tinnitus suppression? Eur. J. Neurol. 2010, 17, 1141–1147. [Google Scholar] [CrossRef]
- Keller, D.L. Assessment of Blinding in a Tinnitus Treatment Trial. JAMA Otolaryngol. Head Neck Surg. 2015, 141, 1031. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Bang, H.; Cañette, I. Blinding in clinical trials, time to do it better. Complement. Ther. Med. 2008, 16, 121–123. [Google Scholar] [CrossRef] [PubMed]
- Folmer, R.L. Long-term reductions in tinnitus severity. BMC Ear Nose Throat Disord. 2002, 2, 3. Available online: http://www.biomedcentral.com/content/pdf/1472-6815-2-3.pdf (accessed on 9 July 2023). [CrossRef] [PubMed]
- Theodoroff, S.M.; Folmer, R.L. Experimental Use of Transcranial Magnetic Stimulation (TMS) to Treat Tinnitus in a Deaf Patient. Clin. Med. Rev. Case Rep. 2015, 2, 1–4. Available online: https://clinmedjournals.org/articles/cmrcr/cmrcr-2-023.pdf (accessed on 9 July 2023). [CrossRef]
- Folmer, R.L.; Theodoroff, S.M. Hearing Protective Devices Should Be Used by Recipients of Repetitive Transcranial Magnetic Stimulation. J. Clin. Neurophysiol. 2017, 34, 552. [Google Scholar] [CrossRef]
- Newman, C.W.; Jacobson, G.P.; Spitzer, J.B. Development of the Tinnitus Handicap Inventory. Arch Otolaryngol. Head Neck Surg. 1996, 122, 143–148. [Google Scholar] [CrossRef]
- Meikle, M.B.; Henry, J.A.; Griest, S.E.; Stewart, B.J.; Abrams, H.B.; McArdle, R.; Myers, P.J.; Newman, C.W.; Sandridge, S.; Turk, S.C.; et al. The Tinnitus Functional Index: A new clinical measure for chronic, intrusive tinnitus. Ear Hear. 2012, 33, 153–176. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Was the Guess Correct? | ||
|---|---|---|
| Subjects’ Guess | YES | NO |
| They Received Active rTMS | 11 subjects | 11 subjects |
| They Received Placebo rTMS | 21 subjects | 21 subjects |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Folmer, R.L. Unresolved Issues Associated with Transcranial Magnetic Stimulation (TMS) Treatment of Chronic Tinnitus. J. Clin. Med. 2023, 12, 4648. https://doi.org/10.3390/jcm12144648
Folmer RL. Unresolved Issues Associated with Transcranial Magnetic Stimulation (TMS) Treatment of Chronic Tinnitus. Journal of Clinical Medicine. 2023; 12(14):4648. https://doi.org/10.3390/jcm12144648
Chicago/Turabian StyleFolmer, Robert L. 2023. "Unresolved Issues Associated with Transcranial Magnetic Stimulation (TMS) Treatment of Chronic Tinnitus" Journal of Clinical Medicine 12, no. 14: 4648. https://doi.org/10.3390/jcm12144648
APA StyleFolmer, R. L. (2023). Unresolved Issues Associated with Transcranial Magnetic Stimulation (TMS) Treatment of Chronic Tinnitus. Journal of Clinical Medicine, 12(14), 4648. https://doi.org/10.3390/jcm12144648