
Analysis of the Spinopelvic Parameters in Patients with Fragility Fractures of the Pelvis
 , ,
, ,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Baseline Characteristics
3.2. Distribution of FFP Types According to the FFP Classification System [9] and OF-Pelvis Classification System [10]
3.3. Spinopelvic Parameters
3.4. Spinopelvic Parameters in the Female and Male Subpopulation
3.5. Spinopelvic Parameters of FFP Patients Compared to Asymptomatic Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| LL [L1-S1] | PT | SS | PI | FFP Classification/ OF-Pelvis Classification |
|---|---|---|---|---|
| 66 | 19.8 | 46.15 | 67.75 | FFP II/OF3 |
| 32.15 | 22.65 | 23.05 | 47.85 | FFP I/OF2 |
| 55.85 | 30.9 | 41.85 | 71.6 | FFP II/OF3 |
| 51.35 | 34 | 38.3 | 74.1 | FFP II/OF3 |
| 43.15 | 27.2 | 23.7 | 53.15 | FFP II/OF3 |
| 75.3 | 45.5 | 44.05 | 100.9 | FFP II/OF3 |
| 22.05 | 42.35 | 30.7 | 72.8 | FFP II/OF3 |
| 38.2 | 39.65 | 25.75 | 66.65 | FFP II/OF3 |
| 42.2 | 20.8 | 27.9 | 51.05 | FFPII/OF3 |
| 42.35 | 46.35 | 31.55 | 75.55 | FFP IV/OF5 |
| 23.75 | 38.9 | 23.9 | 63.5 | FFP II/OF3 |
| 36.9 | 37.15 | 27.35 | 63.4 | FFP II/OF3 |
| 42.25 | 21.8 | 35.3 | 57.25 | FFP II/OF3 |
| 59.9 | 31.15 | 45.15 | 77.4 | FFP II/OF3 |
| 21.05 | 25.75 | 13.7 | 43.25 | FFP II/OF3 |
| 32.55 | 28.1 | 27 | 54.9 | FFP II/OF3 |
| 54.65 | 23.8 | 39.8 | 64.65 | FFP IV/OF5 |
| 53 | 20.1 | 27.1 | 50.2 | FFP II/OF3 |
| 82.9 | 35.7 | 64 | 99.55 | FFP II/OF3 |
| 36.05 | 24.65 | 33.3 | 58 | FFP II/OF3 |
| 45.85 | 28.55 | 29.55 | 58.55 | FFP II/OF3 |
| 49.85 | 28.15 | 41.15 | 68.85 | FFP II/OF3 |
| 21.95 | 38.3 | 13.3 | 49.7 | FFP II/OF3 |
| 31.2 | 23.65 | 29.95 | 53.35 | FFP II/OF3 |
| 45.9 | 30.15 | 30 | 61.4 | FFP I/OF2 |
| 44.7 | 37.9 | 22.9 | 63.15 | FFP II/OF3 |
| 33.5 | 19.6 | 30.25 | 50.5 | FFP II/OF3 |
| 63.35 | 30.25 | 47 | 77 | FFP I/OF2 |
| 50.75 | 18.05 | 39.2 | 55.5 | FFP II/OF3 |
| 53.3 | 25.8 | 49.75 | 75.8 | FFP II/OF3 |
| 64.95 | 35.25 | 45 | 81.8 | FFP II/OF3 |
| 50.6 | 20.2 | 30.65 | 51.35 | FFP II/OF3 |
| 68.55 | 21.2 | 46.1 | 67.65 | FFP I/OF2 |
| 57.5 | 35.55 | 34.8 | 71.65 | FFP II/OF3 |
| 49.05 | 36.85 | 20.5 | 59.55 | FFP I/OF2 |
| 54.2 | 12.1 | 41.05 | 53.95 | FFP II/OF3 |
| 40.5 | 31.1 | 25.35 | 58.05 | FFP II/OF3 |
| 53 | 24.2 | 36.65 | 60.65 | FFP II/OF3 |
| 31.95 | 34.55 | 34.4 | 70.4 | FFP I/OF2 |
| 40.5 | 35.95 | 28.15 | 64.05 | FFP IV/OF5 |
| 39.9 | 36.4 | 25.25 | 60.9 | FFP II/OF3 |
| 50.55 | 22.15 | 26.55 | 49.75 | FFP II/OF3 |
| 66.05 | 31.05 | 48.75 | 83.05 | FFP II/OF3 |
| 65.9 | 34.95 | 52.75 | 80.85 | FFP I/OF2 |
| 52.65 | 11 | 45.95 | 57.1 | FFP II/OF3 |
| 60.2 | 41.65 | 42.75 | 86.7 | FFP II/OF3 |
| 40.65 | 52.05 | 33.5 | 83.75 | FFP II/OF3 |
| 47.4 | 34.85 | 33.9 | 68.1 | FFPII/OF3 |
| 61.25 | 11.6 | 38.55 | 50.6 | FFP II/OF3 |
| 67.05 | 21.3 | 49.85 | 73.15 | FFP IV/OF5 |
| 57.95 | 37.8 | 41.25 | 79.35 | FFP II/OF3 |
| 50.3 | 24.95 | 33.65 | 60.65 | FFP II/OF3 |
| 6.75 | 28.65 | 11 | 40.35 | FFP II/OF3 |
| 53.55 | 27.7 | 33.65 | 61.75 | FFP II/OF3 |
| 49.05 | 19.45 | 28.2 | 51.95 | FFP II/OF3 |
| 49.65 | 31.05 | 27.15 | 60.95 | FFP I/OF2 |
| 49.1 | 26.95 | 29.45 | 56.7 | FFP III/OF4 |
References
- Rommens, P.M.; Arand, C.; Hofmann, A.; Wagner, D. When and How to Operate Fragility Fractures of the Pelvis? Indian J. Orthop. 2019, 53, 128–137. [Google Scholar] [CrossRef]
- Sullivan, M.P.; Baldwin, K.D.; Donegan, D.J.; Mehta, S.; Ahn, J. Geriatric fractures about the hip: Divergent patterns in the proximal femur, acetabulum, and pelvis. Orthopedics 2014, 37, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Lodde, M.F.; Katthagen, J.C.; Riesenbeck, O.; Raschke, M.J.; Hartensuer, R. Trends in der operativen Therapie von Frakturen des Beckenrings: Eine bundesweite Analyse von OPS-Daten zwischen 2005 und 2017. Unfallchirurg 2021, 124, 373–381. [Google Scholar] [CrossRef] [PubMed]
- Lourie, H. Spontaneous osteoporotic fracture of the sacrum. An unrecognized syndrome of the elderly. JAMA 1982, 248, 715–717. [Google Scholar] [CrossRef] [PubMed]
- Rommens, P.M.; Wagner, D.; Hofmann, A. Surgical management of osteoporotic pelvic fractures: A new challenge. Eur. J. Trauma Emerg. Surg. 2012, 38, 499–509. [Google Scholar] [CrossRef]
- Morris, R.O.; Sonibare, A.; Green, D.J.; Masud, T. Closed pelvic fractures: Characteristics and outcomes in older patients admitted to medical and geriatric wards. Postgrad. Med. J. 2000, 76, 646–650. [Google Scholar] [CrossRef]
- Koval, K.J.; Aharonoff, G.B.; Schwartz, M.C.; Alpert, S.; Cohen, G.; McShinawy, A.; Zuckerman, J.D. Pubic rami fracture: A benign pelvic injury? J. Orthop. Trauma 1997, 11, 7–9. [Google Scholar] [CrossRef]
- US Census Data. 2017 National Population Projections Tables: Main Series. Available online: https://www.census.gov/data/tables/2017/demo/popproj/2017-summary-tables.htm (accessed on 17 January 2023).
- Rommens, P.M.; Hofmann, A. Comprehensive classification of fragility fractures of the pelvic ring: Recommendations for surgical treatment. Injury 2013, 44, 1733–1744. [Google Scholar] [CrossRef]
- Ullrich, B.W.; Schnake, K.J.; Spiegl, U.J.A.; Schenk, P.; Mendel, T.; Behr, L.; Bula, P.; Flücht, L.B.; Franck, A.; Gercek, E.; et al. OF-Pelvis classification of osteoporotic sacral and pelvic ring fractures. BMC Musculoskelet. Disord. 2021, 22, 992. [Google Scholar] [CrossRef]
- Andrich, S.; Haastert, B.; Neuhaus, E.; Neidert, K.; Arend, W.; Ohmann, C.; Grebe, J.; Vogt, A.; Jungbluth, P.; Thelen, S.; et al. Excess Mortality After Pelvic Fractures Among Older People. J. Bone Miner. Res. 2017, 32, 1789–1801. [Google Scholar] [CrossRef]
- Rommens, P.M.; Wagner, D.; Hofmann, A. Minimal Invasive Surgical Treatment of Fragility Fractures of the Pelvis. Chirurgia 2017, 112, 524–537. [Google Scholar] [CrossRef] [PubMed]
- Schmerwitz, I.U.; Jungebluth, P.; Lehmann, W.; Hockertz, T.J. Minimally invasive posterior locked compression plate osteosynthesis shows excellent results in elderly patients with fragility fractures of the pelvis. Eur. J. Trauma Emerg. Surg. 2021, 47, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Hartensuer, R.; Lodde, M.F.; Keller, J.; Eveslage, M.; Stolberg-Stolberg, J.; Riesenbeck, O.; Raschke, M.J. Safety, Effect and Feasibility of Percutaneous SI-Screw with and without Augmentation-A 15-Year Retrospective Analysis on over 640 Screws. J. Clin. Med. 2020, 9, 2660. [Google Scholar] [CrossRef] [PubMed]
- Hartensuer, R.; Grüneweller, N.; Lodde, M.F.; Evers, J.; Riesenbeck, O.; Raschke, M. Die S2-Ala-Ilium-Schraube in der Beckentraumatologie. Z. Orthop. Unfall. 2021, 159, 522–532. [Google Scholar] [CrossRef]
- Lodde, M.F.; Katthagen, J.C.; Schopper, C.O.; Zderic, I.; Richards, G.; Gueorguiev, B.; Raschke, M.J.; Hartensuer, R. Biomechanical Comparison of Five Fixation Techniques for Unstable Fragility Fractures of the Pelvic Ring. J. Clin. Med. 2021, 10, 2326. [Google Scholar] [CrossRef]
- Lodde, M.F.; Katthagen, J.C.; Schopper, C.O.; Zderic, I.; Richards, R.G.; Gueorguiev, B.; Raschke, M.J.; Hartensuer, R. Does Cement Augmentation of the Sacroiliac Screw Lead to Superior Biomechanical Results for Fixation of the Posterior Pelvic Ring? A Biomechanical Study. Medicina 2021, 57, 1368. [Google Scholar] [CrossRef]
- Wilson, D.G.G.; Kelly, J.; Rickman, M. Operative management of fragility fractures of the pelvis—A systematic review. BMC Musculoskelet. Disord. 2021, 22, 717. [Google Scholar] [CrossRef]
- Heller, E.P. Avulsion of the anterior superior iliac spine, with symptomless sacralization of the fifth lumbar vertebra. JAMA 1925, 84, 508. [Google Scholar] [CrossRef]
- Splithoff, C.A. Lumbosacral junction; roentgenographic comparison of patients with and without backaches. J. Am. Med. Assoc. 1953, 152, 1610–1613. [Google Scholar] [CrossRef]
- Herbiniaux, G. Traité Sur Divers Accouchements Laborieux Et Sur Les Polypes Deia Matrice; Brux DeBoubers: Brussels, Belgium, 1782. [Google Scholar]
- Boissière, L.; Bourghli, A.; Vital, J.-M.; Gille, O.; Obeid, I. The lumbar lordosis index: A new ratio to detect spinal malalignment with a therapeutic impact for sagittal balance correction decisions in adult scoliosis surgery. Eur. Spine J. 2013, 22, 1339–1345. [Google Scholar] [CrossRef]
- Labelle, H.; Roussouly, P.; Berthonnaud, E.; Transfeldt, E.; O’Brien, M.; Chopin, D.; Hresko, T.; Dimnet, J. Spondylolisthesis, pelvic incidence, and spinopelvic balance: A correlation study. Spine 2004, 29, 2049–2054. [Google Scholar] [CrossRef]
- Labelle, H.; Roussouly, P.; Berthonnaud, E.; Dimnet, J.; O’Brien, M. The importance of spino-pelvic balance in L5-s1 developmental spondylolisthesis: A review of pertinent radiologic measurements. Spine 2005, 30, S27–S34. [Google Scholar] [CrossRef] [PubMed]
- Duval-Beaupère, G.; Schmidt, C.; Cosson, P. A Barycentremetric study of the sagittal shape of spine and pelvis: The conditions required for an economic standing position. Ann. Biomed. Eng. 1992, 20, 451–462. [Google Scholar] [CrossRef] [PubMed]
- Legaye, J.; Duval-Beaupère, G.; Hecquet, J.; Marty, C. Pelvic incidence: A fundamental pelvic parameter for three-dimensional regulation of spinal sagittal curves. Eur. Spine J. 1998, 7, 99–103. [Google Scholar] [CrossRef]
- Vaz, G.; Roussouly, P.; Berthonnaud, E.; Dimnet, J. Sagittal morphology and equilibrium of pelvis and spine. Eur. Spine J. 2002, 11, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Hanson, D.S.; Bridwell, K.H.; Rhee, J.M.; Lenke, L.G. Correlation of pelvic incidence with low- and high-grade isthmic spondylolisthesis. Spine 2002, 27, 2026–2029. [Google Scholar] [CrossRef]
- Sevrain, A.; Aubin, C.-E.; Gharbi, H.; Wang, X.; Labelle, H. Biomechanical evaluation of predictive parameters of progression in adolescent isthmic spondylolisthesis: A computer modeling and simulation study. Scoliosis 2012, 7, 2. [Google Scholar] [CrossRef] [PubMed]
- Boulay, C.; Tardieu, C.; Hecquet, J.; Benaim, C.; Mouilleseaux, B.; Marty, C.; Prat-Pradal, D.; Legaye, J.; Duval-Beaupère, G.; Pélissier, J. Sagittal alignment of spine and pelvis regulated by pelvic incidence: Standard values and prediction of lordosis. Eur. Spine J. 2006, 15, 415–422. [Google Scholar] [CrossRef]
- Hresko, M.T.; Labelle, H.; Roussouly, P.; Berthonnaud, E. Classification of high-grade spondylolistheses based on pelvic version and spine balance: Possible rationale for reduction. Spine 2007, 32, 2208–2213. [Google Scholar] [CrossRef] [PubMed]
- Schwab, F.; Lafage, V.; Patel, A.; Farcy, J.-P. Sagittal plane considerations and the pelvis in the adult patient. Spine 2009, 34, 1828–1833. [Google Scholar] [CrossRef]
- Schwab, F.; Lafage, V.; Boyce, R.; Skalli, W.; Farcy, J.-P. Gravity line analysis in adult volunteers: Age-related correlation with spinal parameters, pelvic parameters, and foot position. Spine 2006, 31, E959–E967. [Google Scholar] [CrossRef] [PubMed]
- Le Huec, J.C.; Hasegawa, K. Normative values for the spine shape parameters using 3D standing analysis from a database of 268 asymptomatic Caucasian and Japanese subjects. Eur. Spine J. 2016, 25, 3630–3637. [Google Scholar] [CrossRef] [PubMed]
- Barrey, C.; Jund, J.; Noseda, O.; Roussouly, P. Sagittal balance of the pelvis-spine complex and lumbar degenerative diseases. A comparative study about 85 cases. Eur. Spine J. 2007, 16, 1459–1467. [Google Scholar] [CrossRef]
- Nuber, S.; Ritter, B.; Fenwick, A.; Förch, S.; Wanzl, M.; Nuber, M.; Mayr, E. Midterm follow-up of elderly patients with fragility fractures of the pelvis: A prospective cohort-study comparing operative and non-operative treatment according to a therapeutic algorithm. Injury 2022, 53, 496–505. [Google Scholar] [CrossRef] [PubMed]
- Rommens, P.M.; Arand, C.; Hopf, J.C.; Mehling, I.; Dietz, S.O.; Wagner, D. Progress of instability in fragility fractures of the pelvis: An observational study. Injury 2019, 50, 1966–1973. [Google Scholar] [CrossRef]
- Jackson, R.P.; Kanemura, T.; Kawakami, N.; Hales, C. Lumbopelvic lordosis and pelvic balance on repeated standing lateral radiographs of adult volunteers and untreated patients with constant low back pain. Spine 2000, 25, 575–586. [Google Scholar] [CrossRef]
- Curylo, L.J.; Edwards, C.; DeWald, R.W. Radiographic markers in spondyloptosis: Implications for spondylolisthesis progression. Spine 2002, 27, 2021–2025. [Google Scholar] [CrossRef]
- Lee, J.S.; Lee, H.S.; Shin, J.K.; Goh, T.S.; Son, S.M. Prediction of sagittal balance in patients with osteoporosis using spinopelvic parameters. Eur. Spine J. 2013, 22, 1053–1058. [Google Scholar] [CrossRef]
- Lafage, V.; Schwab, F.; Vira, S.; Patel, A.; Ungar, B.; Farcy, J.-P. Spino-pelvic parameters after surgery can be predicted: A preliminary formula and validation of standing alignment. Spine 2011, 36, 1037–1045. [Google Scholar] [CrossRef]
- Kang, K.-B.; Ahn, Y.-J.; Kim, Y.J.; Kim, Y.-B.; Park, S.-C. Changes in Sagittal Spinopelvic Parameters according to Pelvic Incidence in Asymptomatic Old Korean Men. J. Korean Soc. Spine Surg. 2011, 18, 223. [Google Scholar] [CrossRef]
- Tanguay, F.; Mac-Thiong, J.-M.; de Guise, J.A.; Labelle, H. Relation between the sagittal pelvic and lumbar spine geometries following surgical correction of adolescent idiopathic scoliosis. Eur. Spine J. 2007, 16, 531–536. [Google Scholar] [CrossRef]
- Rose, P.S.; Bridwell, K.H.; Lenke, L.G.; Cronen, G.A.; Mulconrey, D.S.; Buchowski, J.M.; Kim, Y.J. Role of pelvic incidence, thoracic kyphosis, and patient factors on sagittal plane correction following pedicle subtraction osteotomy. Spine 2009, 34, 785–791. [Google Scholar] [CrossRef]
- Schwab, F.; Ungar, B.; Blondel, B.; Buchowski, J.; Coe, J.; Deinlein, D.; DeWald, C.; Mehdian, H.; Shaffrey, C.; Tribus, C.; et al. Scoliosis Research Society-Schwab adult spinal deformity classification: A validation study. Spine 2012, 37, 1077–1082. [Google Scholar] [CrossRef] [PubMed]
- Ha, K.-Y.; Jang, W.-H.; Kim, Y.-H.; Park, D.-C. Clinical Relevance of the SRS-Schwab Classification for Degenerative Lumbar Scoliosis. Spine 2016, 41, E282–E288. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.-Y.; Zhang, X.-N.; Hai, Y. Optimum pelvic incidence minus lumbar lordosis value after operation for patients with adult degenerative scoliosis. Spine J. 2017, 17, 983–989. [Google Scholar] [CrossRef] [PubMed]
- Yamada, K.; Abe, Y.; Yanagibashi, Y.; Hyakumachi, T.; Satoh, S. Mid- and long-term clinical outcomes of corrective fusion surgery which did not achieve sufficient pelvic incidence minus lumbar lordosis value for adult spinal deformity. Scoliosis 2015, 10, S17. [Google Scholar] [CrossRef]
- Rothenfluh, D.A.; Mueller, D.A.; Rothenfluh, E.; Min, K. Pelvic incidence-lumbar lordosis mismatch predisposes to adjacent segment disease after lumbar spinal fusion. Eur. Spine J. 2015, 24, 1251–1258. [Google Scholar] [CrossRef]
- Aoki, Y.; Nakajima, A.; Takahashi, H.; Sonobe, M.; Terajima, F.; Saito, M.; Takahashi, K.; Ohtori, S.; Watanabe, A.; Nakajima, T.; et al. Influence of pelvic incidence-lumbar lordosis mismatch on surgical outcomes of short-segment transforaminal lumbar interbody fusion. BMC Musculoskelet. Disord. 2015, 16, 213. [Google Scholar] [CrossRef]
- Cho, W.; Mason, J.R.; Smith, J.S.; Shimer, A.L.; Wilson, A.S.; Shaffrey, C.I.; Shen, F.H.; Novicoff, W.M.; Fu, K.-M.G.; Heller, J.E.; et al. Failure of lumbopelvic fixation after long construct fusions in patients with adult spinal deformity: Clinical and radiographic risk factors: Clinical article. J. Neurosurg. Spine 2013, 19, 445–453. [Google Scholar] [CrossRef]
- Hyun, S.-J.; Rhim, S.-C. Clinical outcomes and complications after pedicle subtraction osteotomy for fixed sagittal imbalance patients: A long-term follow-up data. J. Korean Neurosurg. Soc. 2010, 47, 95–101. [Google Scholar] [CrossRef]
- Hyun, S.-J.; Lee, B.H.; Park, J.-H.; Kim, K.-J.; Jahng, T.-A.; Kim, H.-J. Proximal Junctional Kyphosis and Proximal Junctional Failure Following Adult Spinal Deformity Surgery. Korean J. Spine 2017, 14, 126–132. [Google Scholar] [CrossRef]
- Odate, S.; Shikata, J.; Kimura, H.; Soeda, T. Sacral fracture after instrumented lumbosacral fusion: Analysis of risk factors from spinopelvic parameters. Spine 2013, 38, E223–E239. [Google Scholar] [CrossRef]
- Fei, H.; Li, W.-S.; Sun, Z.-R.; Ma, Q.-W.; Chen, Z.-Q. Analysis of Spino-pelvic Sagittal Alignment in Young Chinese Patients with Lumbar Disc Herniation. Orthop. Surg. 2017, 9, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Kao, F.-C.; Huang, Y.-J.; Chiu, P.-Y.; Hsieh, M.-K.; Tsai, T.-T. Factors Predicting the Surgical Risk of Osteoporotic Vertebral Compression Fractures. J. Clin. Med. 2019, 4, 501. [Google Scholar] [CrossRef] [PubMed]
- Sparrey, C.J.; Bailey, J.F.; Safaee, M.; Clark, A.J.; Lafage, V.; Schwab, F.; Smith, J.S.; Ames, C.P. Etiology of lumbar lordosis and its pathophysiology: A review of the evolution of lumbar lordosis, and the mechanics and biology of lumbar degeneration. Neurosurg. Focus 2014, 36, E1. [Google Scholar] [CrossRef] [PubMed]
- Katzman, W.B.; Wanek, L.; Shepherd, J.A.; Sellmeyer, D.E. Age-related hyperkyphosis: Its causes, consequences, and management. J. Orthop. Sports Phys. Ther. 2010, 40, 352–360. [Google Scholar] [CrossRef] [PubMed]
- Hsu, W.-L.; Chen, C.-Y.; Tsauo, J.-Y.; Yang, R.-S. Balance control in elderly people with osteoporosis. J. Formos. Med. Assoc. 2014, 113, 334–339. [Google Scholar] [CrossRef]
- Le Huec, J.-C.; Faundez, A.; Dominguez, D.; Hoffmeyer, P.; Aunoble, S. Evidence showing the relationship between sagittal balance and clinical outcomes in surgical treatment of degenerative spinal diseases: A literature review. Int. Orthop. 2015, 39, 87–95. [Google Scholar] [CrossRef]







| Patients | Mean Age (Years) | IQR (Years) |
|---|---|---|
| Study population | 81.0 | 77.1–84.8 |
| Female patients | 80.9 | 76.9–85.3 |
| Male patients | 81.5 | 79.1–84.9 |
| Parameters | Degree | SD (Degree) |
|---|---|---|
| LL | 47.9 | ±14.4 |
| PT | 29.4 | ±8.8 |
| SS | 34.2 | ±10.4 |
| PI | 64.4 | ±12.9 |
| LLI | 0.7 | ±0.2 |
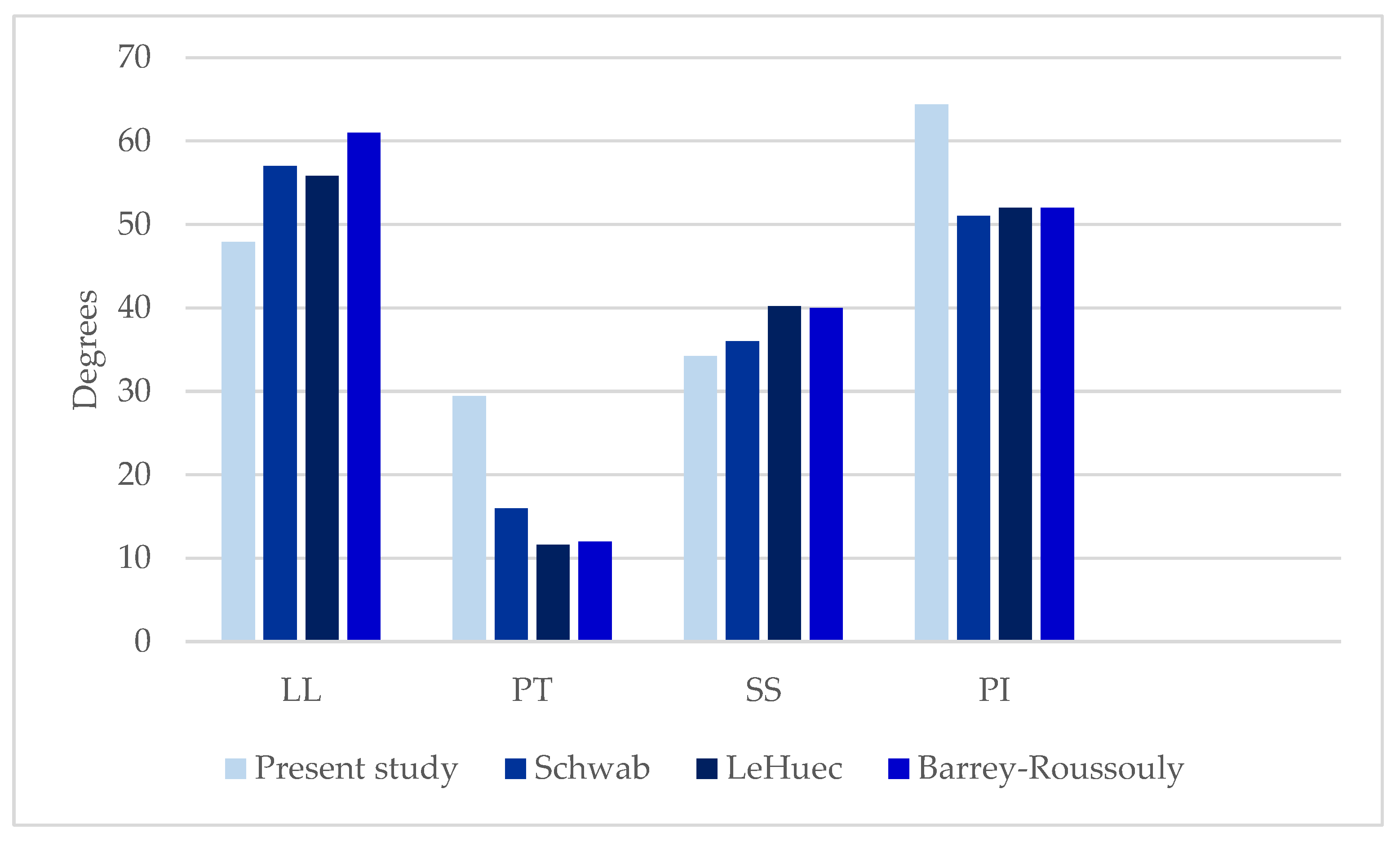
| Parameters | Present Study’s Degree | Schwab [33] Degree of Asymptomatic Patients > 60 Years | LeHuec [34] Degree of Asymptomatic Patient | Barrey-Roussouly [35] Degree of Asymptomatic Patients |
|---|---|---|---|---|
| LL | 47.9 ± 14.4 | 57 ± 11 | 55.8 ± 10.2 | 61 ± 9.7 |
| PT | 29.4 ± 8.8 | 16 ± 9 | 11.6 ± 7.0 | 12 ± 6.5 |
| SS | 34.2 ± 10.4 | 36 ± 9 | 40.2 ± 7.7 | 40 ± 8.2 |
| PI | 64.4 ± 12.9 | 51 ± 9 | 52.0 ± 10.5 | 52 ± 10.7 |
| LLI | 0.7 ± 0.2 | 1.1 | 1.1 | 1.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lodde, M.F.; Fischer, T.M.; Riesenbeck, O.; Roßlenbroich, S.; Katthagen, J.C.; Rometsch, D.; Günes, D.; Schneider, M.; Raschke, M.J.; Liljenqvist, U. Analysis of the Spinopelvic Parameters in Patients with Fragility Fractures of the Pelvis. J. Clin. Med. 2023, 12, 4445. https://doi.org/10.3390/jcm12134445
Lodde MF, Fischer TM, Riesenbeck O, Roßlenbroich S, Katthagen JC, Rometsch D, Günes D, Schneider M, Raschke MJ, Liljenqvist U. Analysis of the Spinopelvic Parameters in Patients with Fragility Fractures of the Pelvis. Journal of Clinical Medicine. 2023; 12(13):4445. https://doi.org/10.3390/jcm12134445
Chicago/Turabian StyleLodde, Moritz F., Thies M. Fischer, Oliver Riesenbeck, Steffen Roßlenbroich, J. Christoph Katthagen, Daria Rometsch, Dennis Günes, Marc Schneider, Michael J. Raschke, and Ulf Liljenqvist. 2023. "Analysis of the Spinopelvic Parameters in Patients with Fragility Fractures of the Pelvis" Journal of Clinical Medicine 12, no. 13: 4445. https://doi.org/10.3390/jcm12134445
APA StyleLodde, M. F., Fischer, T. M., Riesenbeck, O., Roßlenbroich, S., Katthagen, J. C., Rometsch, D., Günes, D., Schneider, M., Raschke, M. J., & Liljenqvist, U. (2023). Analysis of the Spinopelvic Parameters in Patients with Fragility Fractures of the Pelvis. Journal of Clinical Medicine, 12(13), 4445. https://doi.org/10.3390/jcm12134445