
Multi-Site Spinal Cord Transcutaneous Stimulation Facilitates Upper Limb Sensory and Motor Recovery in Severe Cervical Spinal Cord Injury: A Case Study

Abstract
1. Introduction
2. Materials and Methods
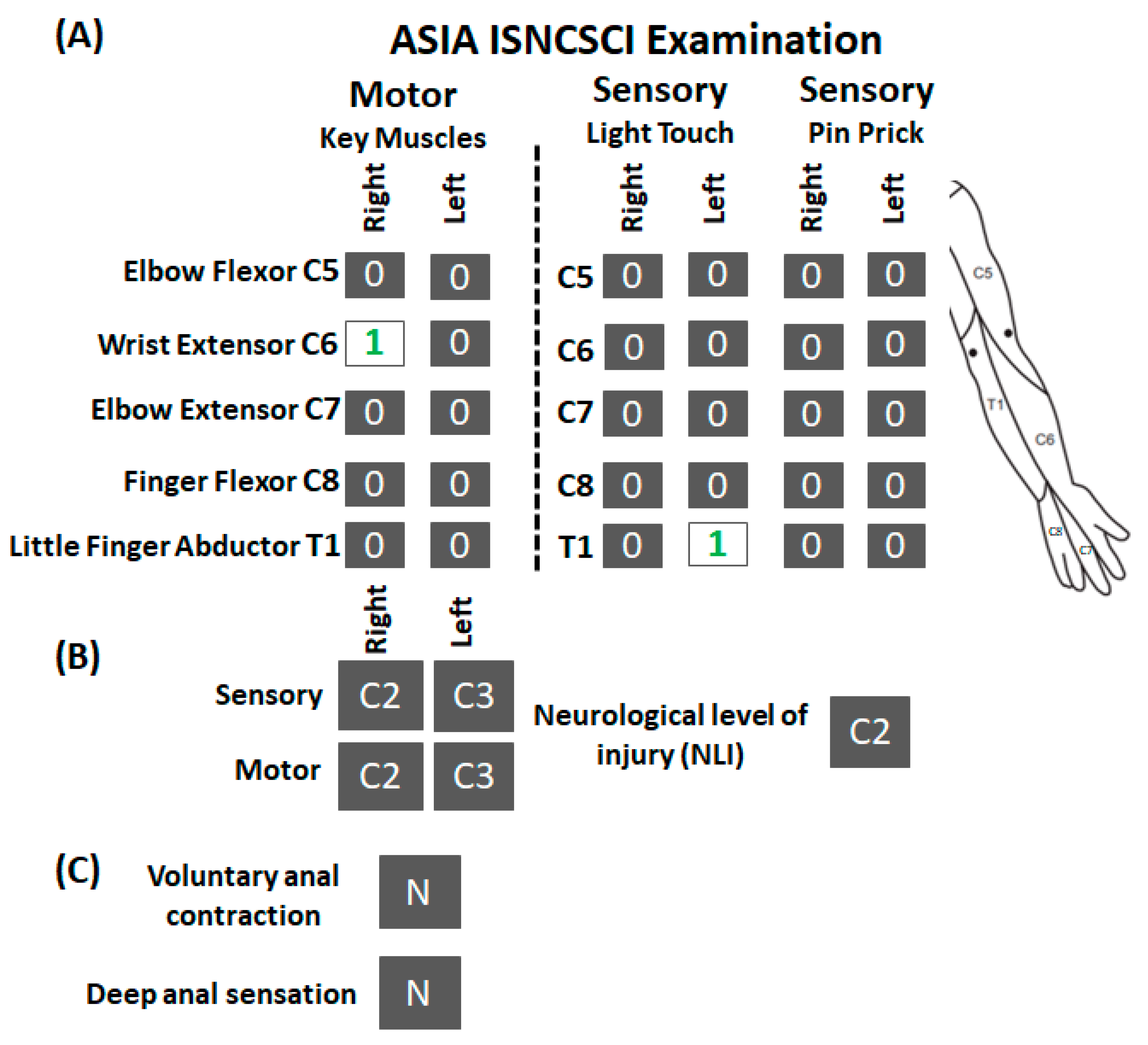
2.1. Clinical Characteristics of the Participant
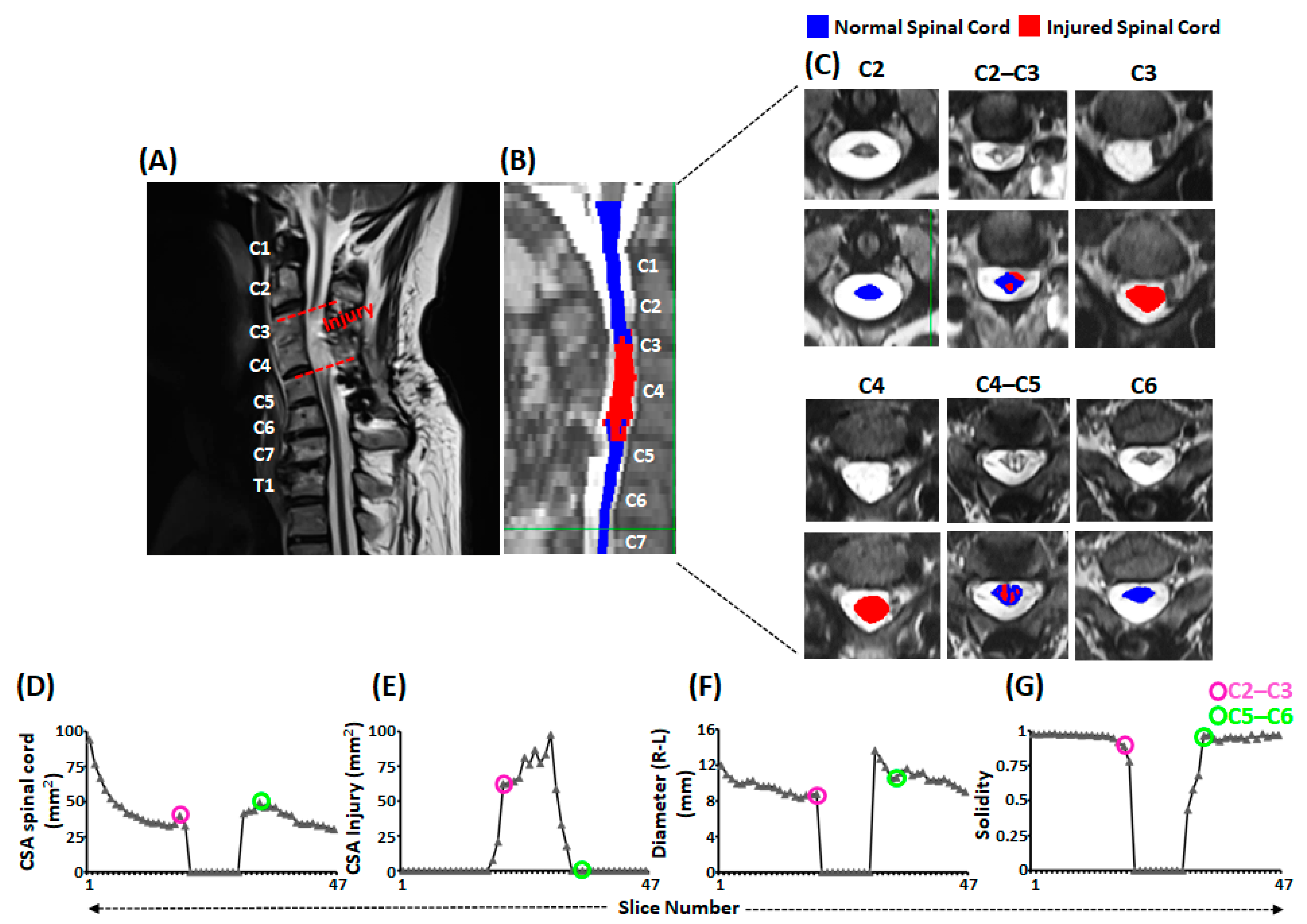
2.2. Magnetic Resonance Imaging (MRI) Data Acquisition
2.3. Functional Neurophysiological Assessment (FNPA)
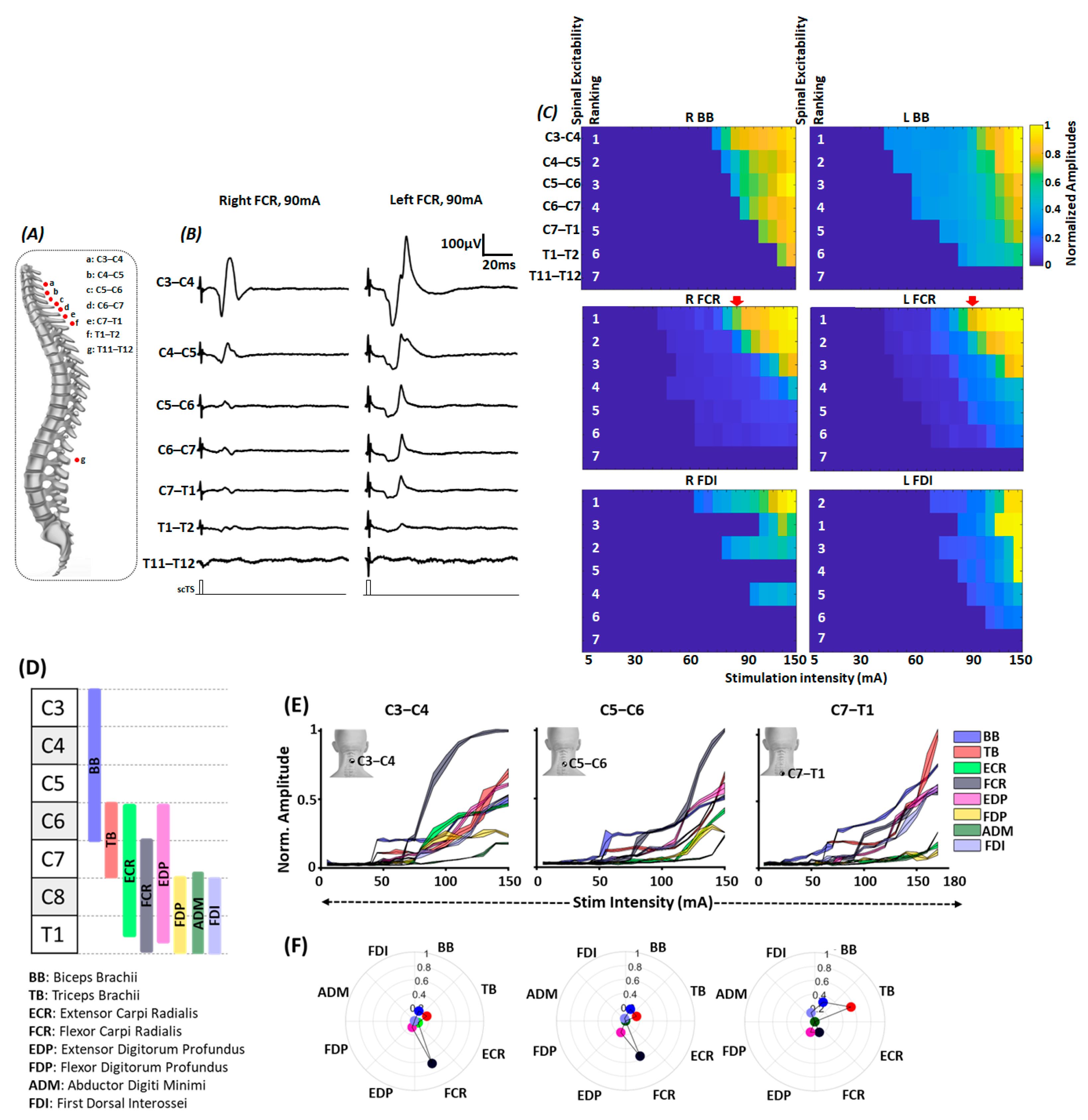
2.4. Multisegmental Motor Response (MMR) Mapping
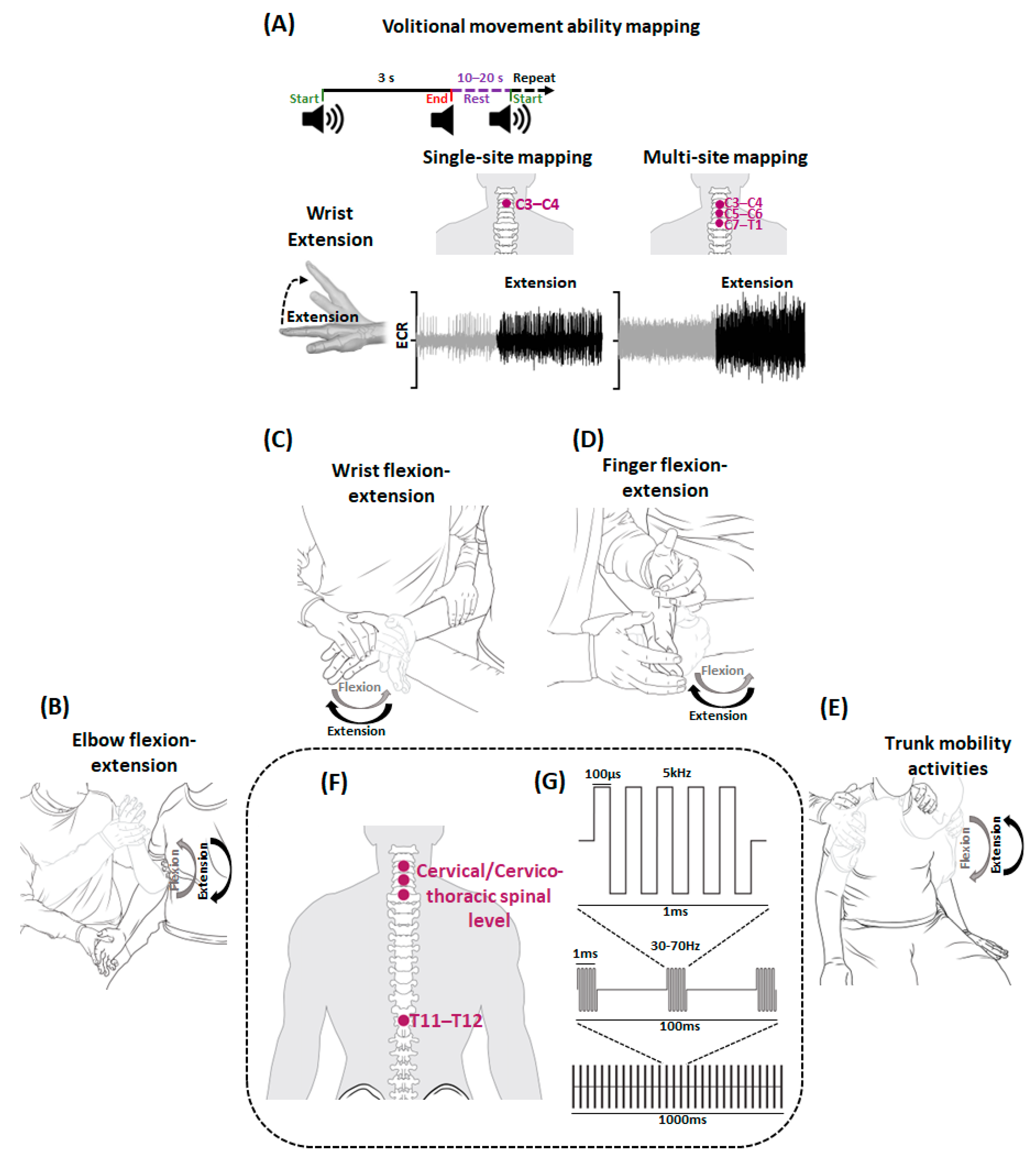
2.5. Upper Extremity Volitional Movement Ability Mapping
2.6. Activity-Based Recovery Training (ABRT)
2.7. Spinal Cord Transcutaneous Stimulation (scTS)
2.8. Upper Extremity Motor Assessment
2.9. Data Analysis
2.10. Statistical Analysis
3. Results
3.1. Severity of Injury
3.2. Activation of Upper Extremity Muscles via scTS
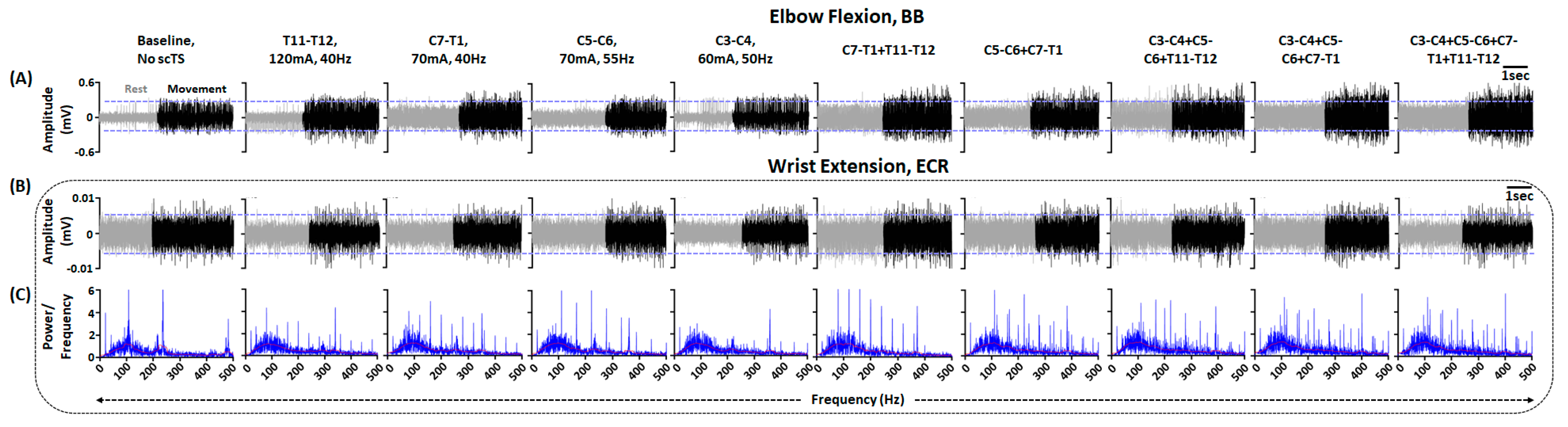
3.3. Greater Muscle Activation during Multi-Site Compared to Single-Site scTS
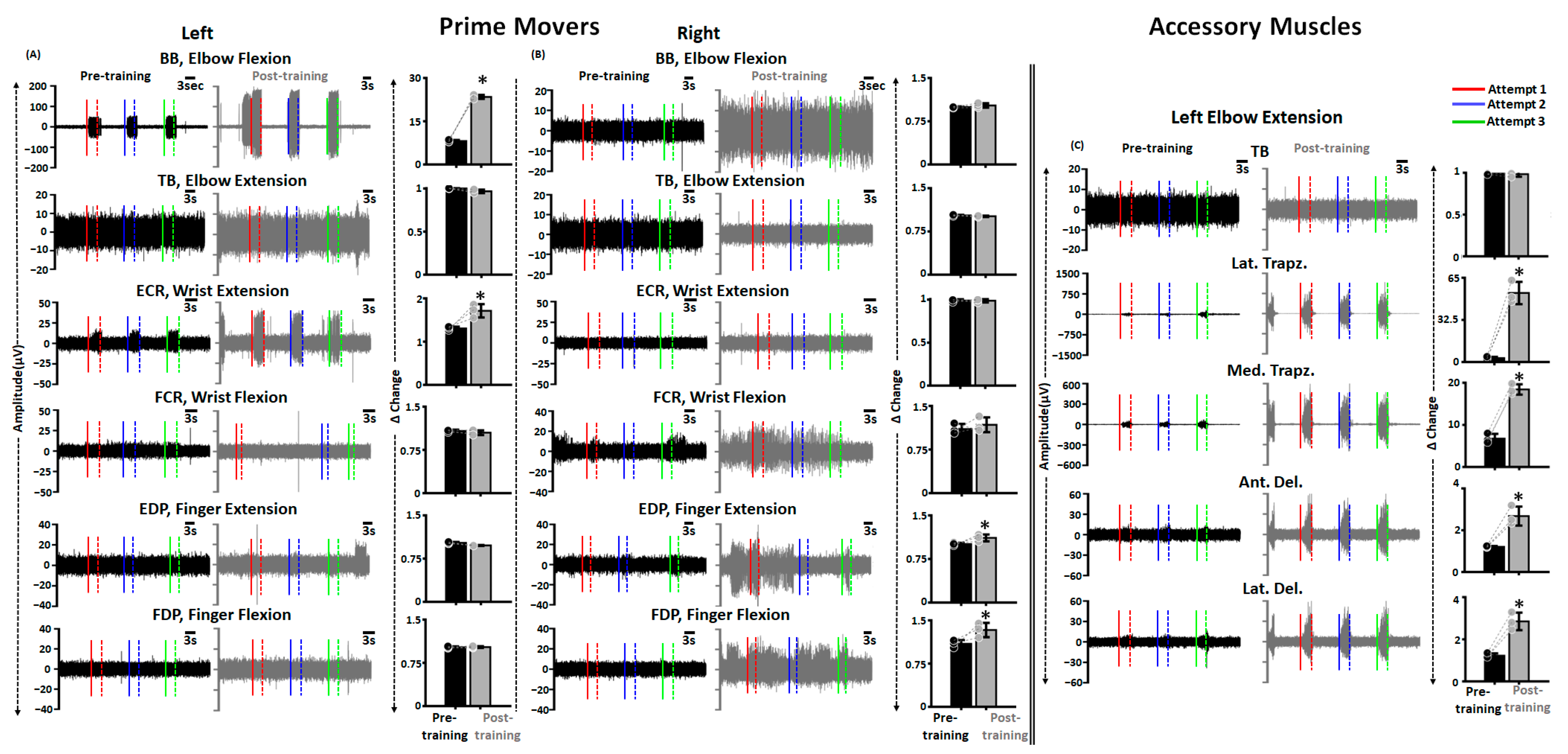
3.4. Improved Activation of Upper Extremity Muscles Post ABRT + scTS Training
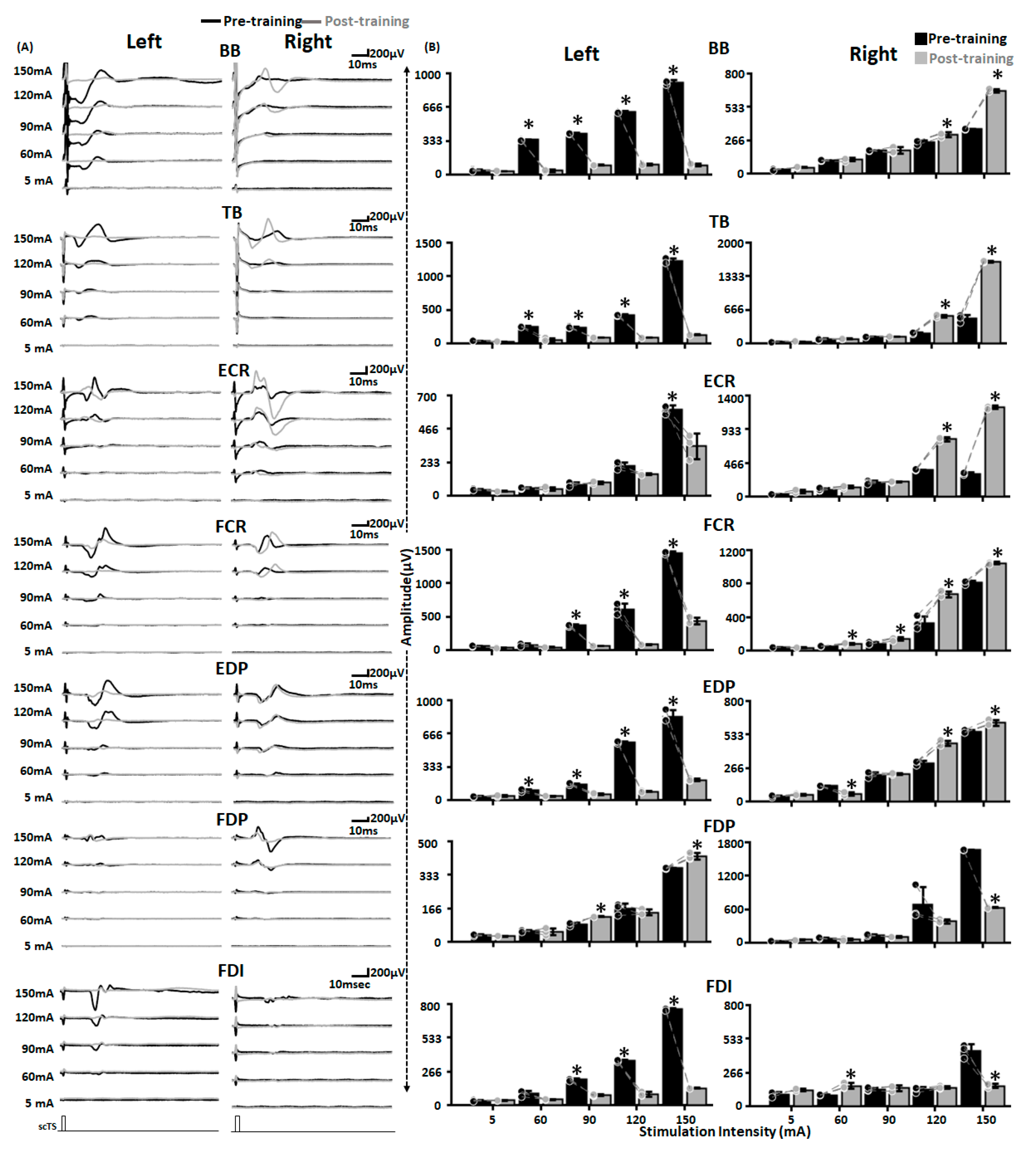
3.5. Altered Spinal Cord Excitability Post ABRT + scTS Training
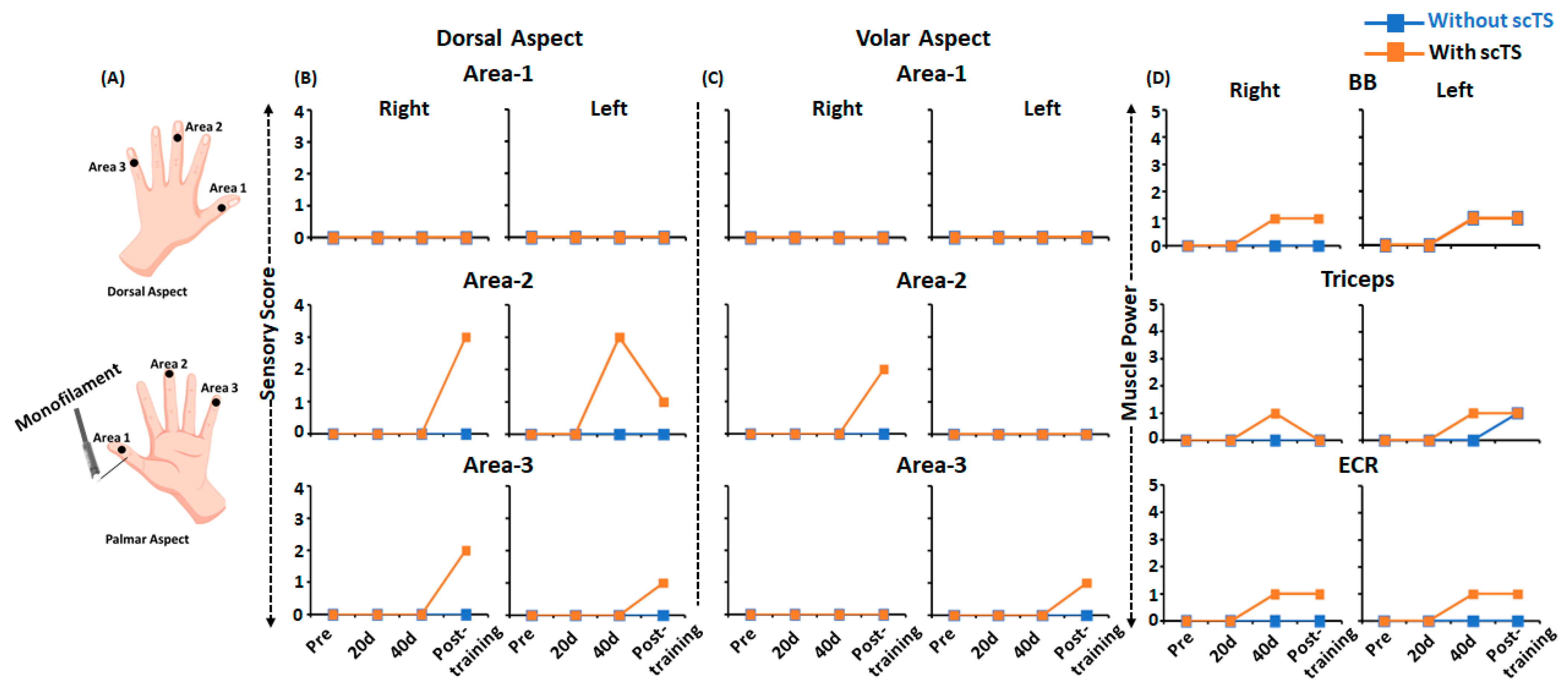
3.6. Improved Sensations and Muscle Strength Post ABRT + scTS Training
3.7. No Changes in the Visually Appreciable Functional Performance Post ABRT + scTS Training
3.8. Study-Related Adverse Effects
4. Discussion
4.1. Activation of Upper Extremity Muscles with Targeted scTS Post Severe Cervical SCI
4.2. Multi-Site scTS Induced Improved Sensory and Motor Activation Post Severe Cervical SCI
4.3. Neurophysiological Basis of Sensory and Motor Recovery
4.4. No Changes in the Visually Appreciable Motor Functions
4.5. Clinical Implications and Recommendations: Identifying Opportunities for Recovery following Severe Cervical SCI
4.6. Limitation
4.7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Birmingham, U. National Spinal Cord Injury Statistical Center, Facts and Figures at a Glance; University of Alabama: Birmingham, AL, USA, 2021. [Google Scholar]
- Lo, C.; Tran, Y.; Anderson, K.; Craig, A.; Middleton, J.; Sabre, L.; Harro, J.; Eensoo, D.; Vaht, M.; Kabel, V.; et al. Functional Priorities in Persons with Spinal Cord Injury: Using Discrete Choice Experiments To Determine Preferences. J. Neurotrauma 2016, 33, 1958–1968. [Google Scholar] [CrossRef]
- Anderson, K.D.; Walter, M.; Kran, S.L.; Ramirez, A.L.; Rapoport, D.; Nigro, M.K.; Stothers, L.; Kavanagh, A.; Krassioukov, A.V.; Hoey, R.F.; et al. Targeting Recovery: Priorities of the Spinal Cord-Injured Population. J. Neurotrauma 2004, 21, 1371–1383. [Google Scholar] [CrossRef] [PubMed]
- Peckham, P.; Keith, M.W.; Kilgore, K.; Grill, J.H.; Wuolle, K.S.; Thrope, G.B.; Gorman, P.; Hobby, J.; Mulcahey, M.; Carroll, S.; et al. Efficacy of an implanted neuroprosthesis for restoring hand grasp in tetraplegia: A multicenter study. Arch. Phys. Med. Rehabil. 2001, 82, 1380–1388. [Google Scholar] [CrossRef] [PubMed]
- Lu, D.C.; Edgerton, V.R.; Modaber, M.; AuYong, N.; Morikawa, E.; Zdunowski, S.; Sarino, M.E.; Sarrafzadeh, M.; Nuwer, M.R.; Roy, R.R.; et al. Engaging Cervical Spinal Cord Networks to Reenable Volitional Control of Hand Function in Tetraplegic Patients. Neurorehabilit. Neural Repair 2016, 30, 951–962. [Google Scholar] [CrossRef]
- Harkema, S.; Gerasimenko, Y.; Hodes, J.; Burdick, J.; Angeli, C.; Chen, Y.; Ferreira, C.; Willhite, A.; Rejc, E.; Grossman, R.G.; et al. Effect of epidural stimulation of the lumbosacral spinal cord on voluntary movement, standing, and assisted stepping after motor complete paraplegia: A case study. Lancet 2011, 377, 1938–1947. [Google Scholar] [CrossRef] [PubMed]
- Angeli, C.A.; Boakye, M.; Morton, R.A.; Vogt, J.; Benton, K.; Chen, Y.; Ferreira, C.K.; Harkema, S.J. Recovery of Over-Ground Walking after Chronic Motor Complete Spinal Cord Injury. N. Engl. J. Med. 2018, 379, 1244–1250. [Google Scholar] [CrossRef] [PubMed]
- Angeli, C.A.; Edgerton, V.R.; Gerasimenko, Y.P.; Harkema, S.J. Altering spinal cord excitability enables voluntary movements after chronic complete paralysis in humans. Brain 2014, 137 Pt 5, 1394–1409. [Google Scholar] [CrossRef]
- Rowald, A.; Komi, S.; Demesmaeker, R.; Baaklini, E.; Hernandez-Charpak, S.D.; Paoles, E.; Montanaro, H.; Cassara, A.; Becce, F.; Lloyd, B.; et al. Activity-dependent spinal cord neuromodulation rapidly restores trunk and leg motor functions after complete paralysis. Nat. Med. 2022, 28, 260–271. [Google Scholar] [CrossRef]
- Gill, M.; Linde, M.; Fautsch, K.; Hale, R.; Lopez, C.; Veith, D.; Calvert, J.; Beck, L.; Garlanger, K.; Edgerton, R.; et al. Epidural Electrical Stimulation of the Lumbosacral Spinal Cord Improves Trunk Stability During Seated Reaching in Two Humans with Severe Thoracic Spinal Cord Injury. Front. Syst. Neurosci. 2020, 14, 79. [Google Scholar] [CrossRef]
- Wagner, F.B.; Mignardot, J.-B.; Le Goff-Mignardot, C.G.; Demesmaeker, R.; Komi, S.; Capogrosso, M.; Rowald, A.; Seáñez, I.; Caban, M.; Pirondini, E.; et al. Targeted neurotechnology restores walking in humans with spinal cord injury. Nature 2018, 563, 65–71. [Google Scholar] [CrossRef]
- Gill, M.L.; Grahn, P.J.; Calvert, J.S.; Linde, M.B.; Lavrov, I.A.; Strommen, J.A.; Beck, L.A.; Sayenko, D.G.; Van Straaten, M.G.; Drubach, D.I.; et al. Neuromodulation of lumbosacral spinal networks enables independent stepping after complete paraplegia. Nat. Med. 2018, 24, 1677–1682. [Google Scholar] [CrossRef]
- Oh, J.; Steele, A.G.; Varghese, B.; Martin, C.A.; Scheffler, M.S.; Markley, R.L.; Lo, Y.-K.; Sayenko, D.G. Cervical transcutaneous spinal stimulation for spinal motor mapping. iScience 2022, 25, 105037. [Google Scholar] [CrossRef]
- Chandrasekaran, S.; Bhagat, N.; Ramdeo, R.; Ebrahimi, S.; Sharma, P.; Stein, A.; Griffin, D.; Harkema, S.; Bouton, C. Targeted transcutaneous cervical spinal cord stimulation promotes upper limb recovery in spinal cord and peripheral nerve injury. medRxiv 2022. [CrossRef]
- Hofstoetter, U.S.; Freundl, B.; Binder, H.; Minassian, K. Common neural structures activated by epidural and transcutaneous lumbar spinal cord stimulation: Elicitation of posterior root-muscle reflexes. PLoS ONE 2018, 13, e0192013. [Google Scholar] [CrossRef] [PubMed]
- Siu, R.; Brown, E.H.; Mesbah, S.; Gonnelli, F.; Pisolkar, T.; Edgerton, V.R.; Ovechkin, A.V.; Gerasimenko, Y.P. Novel Noninvasive Spinal Neuromodulation Strategy Facilitates Recovery of Stepping after Motor Complete Paraplegia. J. Clin. Med. 2022, 11, 3670. [Google Scholar] [CrossRef] [PubMed]
- Gerasimenko, Y.; Gorodnichev, R.; Moshonkina, T.; Sayenko, D.; Gad, P.; Edgerton, V.R. Transcutaneous electrical spinal-cord stimulation in humans. Ann. Phys. Rehabil. Med. 2015, 58, 225–231. [Google Scholar] [CrossRef]
- Singh, G.; Lucas, K.; Keller, A.; Martin, O.R.; Behrman, A.; Vissarionov, S.; Gerasimenko, Y.P. Transcutaneous Spinal Stimulation From Adults to Children: A Review. Top. Spinal Cord Inj. Rehabil. 2022, 29, 16–32. [Google Scholar] [CrossRef]
- Hofstoetter, U.S.; McKay, W.B.; Tansey, K.E.; Mayr, W.; Kern, H.; Minassian, K. Modification of spasticity by transcutaneous spinal cord stimulation in individuals with incomplete spinal cord injury. J. Spinal Cord Med. 2013, 37, 202–211. [Google Scholar] [CrossRef]
- Gad, P.; Lee, S.; Terrafranca, N.; Zhong, H.; Turner, A.; Gerasimenko, Y.; Edgerton, V.R. Non-Invasive Activation of Cervical Spinal Networks after Severe Paralysis. J. Neurotrauma 2018, 35, 2145–2158. [Google Scholar] [CrossRef]
- Freyvert, Y.; Yong, N.A.; Morikawa, E.; Zdunowski, S.; Sarino, M.E.; Gerasimenko, Y.; Edgerton, V.R.; Lu, D.C. Engaging cervical spinal circuitry with non-invasive spinal stimulation and buspirone to restore hand function in chronic motor complete patients. Sci. Rep. 2018, 8, 15546. [Google Scholar] [CrossRef]
- Inanici, F.; Brighton, L.N.; Samejima, S.; Hofstetter, C.P.; Moritz, C.T. Transcutaneous Spinal Cord Stimulation Restores Hand and Arm Function After Spinal Cord Injury. IEEE Trans. Neural Syst. Rehabil. Eng. 2021, 29, 310–319. [Google Scholar] [CrossRef] [PubMed]
- Inanici, F.; Samejima, S.; Gad, P.; Edgerton, V.R.; Hofstetter, C.P.; Moritz, C.T. Transcutaneous Electrical Spinal Stimulation Promotes Long-Term Recovery of Upper Extremity Function in Chronic Tetraplegia. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 26, 1272–1278. [Google Scholar] [CrossRef]
- Zhang, F.; Momeni, K.; Ramanujam, A.; Ravi, M.; Carnahan, J.; Kirshblum, S.; Forrest, G.F. Cervical Spinal Cord Transcutaneous Stimulation Improves Upper Extremity and Hand Function in People with Complete Tetraplegia: A Case Study. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 3167–3174. [Google Scholar] [CrossRef]
- Huang, R.; Nikooyan, A.A.; Moore, L.D.; Zdunowski, S.; Morikawa, E.; Sierro, T.; Sayenko, D.; Gad, P.; Homsey, T.; Le, T.; et al. Minimal handgrip force is needed for transcutaneous electrical stimulation to improve hand functions of patients with severe spinal cord injury. Sci. Rep. 2022, 12, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Kirshblum, S.C.; Burns, S.P.; Biering-Sørensen, F.; Donovan, W.; Graves, D.E.; Jha, A.; Johansen, M.; Jones, L.; Krassioukov, A.; Mulcahey, M.J.; et al. International standards for neurological classification of spinal cord injury (Revised 2011). J. Spinal Cord Med. 2011, 34, 535–546. [Google Scholar] [CrossRef] [PubMed]
- Rejc, E.; Smith, A.C.; Weber, K.A.I.; Ugiliweneza, B.; Bert, R.J.; Negahdar, M.; Boakye, M.; Harkema, S.J.; Angeli, C.A. Spinal Cord Imaging Markers and Recovery of Volitional Leg Movement With Spinal Cord Epidural Stimulation in Individuals With Clinically Motor Complete Spinal Cord Injury. Front. Syst. Neurosci. 2020, 14, 559313. [Google Scholar] [CrossRef]
- Smith, A.C.; Angeli, C.A.; Ugiliweneza, B.; Weber, K.A.; Bert, R.J.; Negahdar, M.; Mesbah, S.; Boakye, M.; Harkema, S.J.; Rejc, E. Spinal cord imaging markers and recovery of standing with epidural stimulation in individuals with clinically motor complete spinal cord injury. Exp. Brain Res. 2021, 240, 279–288. [Google Scholar] [CrossRef]
- Sharma, P.; Naglah, A.; Aslan, S.; Khalifa, F.; El-Baz, A.; Harkema, S.; D’Amico, J. Preservation of functional descending input to paralyzed upper extremity muscles in motor complete cervical spinal cord injury. Clin. Neurophysiol. 2023, 150, 56–68. [Google Scholar] [CrossRef]
- Li, K.; Atkinson, D.; Boakye, M.; Tolfo, C.Z.; Aslan, S.; Green, M.; McKay, B.; Ovechkin, A.; Harkema, S.J. Quantitative and sensitive assessment of neurophysiological status after human spinal cord injury. J. Neurosurg. Spine 2012, 17 (Suppl. S1), 77–86. [Google Scholar] [CrossRef]
- Hermens, H.J.; Freriks, B.; Disselhorst-Klug, C.; Rau, G. Development of recommendations for SEMG sensors and sensor placement procedures. J. Electromyogr. Kinesiol. 2000, 10, 361–374. [Google Scholar] [CrossRef]
- Geiringer, S.R. Anatomic Localization for Needle EMG, 2nd ed.; Elseiver: Amsterdam, The Netherlands, 1999. [Google Scholar]
- Parhizi, B.; Barss, T.S.; Mushahwar, V.K. Simultaneous Cervical and Lumbar Spinal Cord Stimulation Induces Facilitation of Both Spinal and Corticospinal Circuitry in Humans. Front. Neurosci. 2021, 15, 615103. [Google Scholar] [CrossRef] [PubMed]
- Barss, T.S.; Parhizi, B.; Porter, J.; Mushahwar, V.K. Neural Substrates of Transcutaneous Spinal Cord Stimulation: Neuromodulation across Multiple Segments of the Spinal Cord. J. Clin. Med. 2022, 11, 639. [Google Scholar] [CrossRef] [PubMed]
- Tharu, N.S.; Alam, M.; Ling, Y.T.; Wong, A.Y.; Zheng, Y.-P. Combined Transcutaneous Electrical Spinal Cord Stimulation and Task-Specific Rehabilitation Improves Trunk and Sitting Functions in People with Chronic Tetraplegia. Biomedicines 2022, 11, 34. [Google Scholar] [CrossRef] [PubMed]
- Keller, A.; Singh, G.; Sommerfeld, J.H.; King, M.; Parikh, P.; Ugiliweneza, B.; D’amico, J.; Gerasimenko, Y.; Behrman, A.L. Noninvasive spinal stimulation safely enables upright posture in children with spinal cord injury. Nat. Commun. 2021, 12, 5850. [Google Scholar] [CrossRef]
- Rath, M.; Vette, A.H.; Ramasubramaniam, S.; Li, K.; Burdick, J.; Edgerton, V.R.; Gerasimenko, Y.P.; Sayenko, D.G. Trunk Stability Enabled by Noninvasive Spinal Electrical Stimulation after Spinal Cord Injury. J. Neurotrauma 2018, 35, 2540–2553. [Google Scholar] [CrossRef]
- Benavides, F.D.; Jo, H.J.; Lundell, H.; Edgerton, V.R.; Gerasimenko, Y.; Perez, M.A. Cortical and Subcortical Effects of Transcutaneous Spinal Cord Stimulation in Humans with Tetraplegia. J. Neurosci. 2020, 40, 2633–2643. [Google Scholar] [CrossRef]
- Kalsi-Ryan, S.; Beaton, D.; Curt, A.; Duff, S.; Popovic, M.R.; Rudhe, C.; Fehlings, M.G.; Verrier, M.C. The Graded Redefined Assessment of Strength Sensibility and Prehension: Reliability and validity. J. Neurotrauma 2012, 29, 905–914. [Google Scholar] [CrossRef]
- Behrman, A.L.; Ardolino, E.; VanHiel, L.R.; Kern, M.; Atkinson, D.; Lorenz, D.J.; Harkema, S.J. Assessment of Functional Improvement Without Compensation Reduces Variability of Outcome Measures After Human Spinal Cord Injury. Arch. Phys. Med. Rehabil. 2012, 93, 1518–1529. [Google Scholar] [CrossRef]
- Harkema, S.J.; Shogren, C.; Ardolino, E.; Lorenz, D.J. Assessment of Functional Improvement without Compensation for Human Spinal Cord Injury: Extending the Neuromuscular Recovery Scale to the Upper Extremities. J. Neurotrauma 2016, 33, 2181–2190. [Google Scholar] [CrossRef]
- De Leener, B.; Lévy, S.; Dupont, S.M.; Fonov, V.S.; Stikov, N.; Collins, D.L.; Callot, V.; Cohen-Adad, J. SCT: Spinal Cord Toolbox, an open-source software for processing spinal cord MRI data. Neuroimage 2017, 145 Pt A, 24–43. [Google Scholar] [CrossRef]
- Smith, A.C.; O’Dell, D.R.; Albin, S.R.; Berliner, J.C.; Dungan, D.; Robinson, E.; Elliott, J.M.; Carballido-Gamio, J.; Stevens-Lapsley, J.; Weber, K.A. Lateral Corticospinal Tract and Dorsal Column Damage: Predictive Relationships With Motor and Sensory Scores at Discharge From Acute Rehabilitation After Spinal Cord Injury. Arch. Phys. Med. Rehabil. 2021, 103, 62–68. [Google Scholar] [CrossRef]
- Greiner, N.; Barra, B.; Schiavone, G.; Lorach, H.; James, N.; Conti, S.; Kaeser, M.; Fallegger, F.; Borgognon, S.; Lacour, S.; et al. Recruitment of upper-limb motoneurons with epidural electrical stimulation of the cervical spinal cord. Nat. Commun. 2021, 12, 435. [Google Scholar] [CrossRef]
- Mendez, A.; Islam, R.; Latypov, T.; Basa, P.; Joseph, O.J.; Knudsen, B.; Siddiqui, A.M.; Summer, P.; Staehnke, L.J.; Grahn, P.J.; et al. Segment-Specific Orientation of the Dorsal and Ventral Roots for Precise Therapeutic Targeting of Human Spinal Cord. Mayo Clin. Proc. 2021, 96, 1426–1437. [Google Scholar] [CrossRef]
- Atkinson, D.A.; Mendez, L.; Goodrich, N.; Aslan, S.C.; Ugiliweneza, B.; Behrman, A.L. Muscle Activation Patterns During Movement Attempts in Children With Acquired Spinal Cord Injury: Neurophysiological Assessment of Residual Motor Function Below the Level of Lesion. Front. Neurol. 2019, 10, 1295. [Google Scholar] [CrossRef]
- Gerasimenko, Y.; Gorodnichev, R.; Puhov, A.; Moshonkina, T.; Savochin, A.; Selionov, V.; Roy, R.R.; Lu, D.C.; Edgerton, V.R. Initiation and modulation of locomotor circuitry output with multisite transcutaneous electrical stimulation of the spinal cord in noninjured humans. J. Neurophysiol. 2015, 113, 834–842. [Google Scholar] [CrossRef] [PubMed]
- Sayenko, D.G.; Atkinson, D.A.; Dy, C.J.; Gurley, K.M.; Smith, V.L.; Angeli, C.; Harkema, S.J.; Edgerton, V.R.; Gerasimenko, Y.P. Spinal segment-specific transcutaneous stimulation differentially shapes activation pattern among motor pools in humans. J. Appl. Physiol. 2015, 118, 1364–1374. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Shah, P.K. In vivo electrophysiological mechanisms underlying cervical epidural stimulation in adult rats. J. Physiol. 2021, 599, 3121–3150. [Google Scholar] [CrossRef] [PubMed]
- Lü, X.-Y.; Wang, Z.-G.; Mao, G.-W.; Zhang, J.-J.; Su, H.; Zhou, Z.-J.; Zhu, L.-S. A flexible electrode array for determining regions of motor function activated by epidural spinal cord stimulation in rats with spinal cord injury. Neural Regen. Res. 2022, 17, 601–607. [Google Scholar] [CrossRef]
- Barra, B.; Conti, S.; Perich, M.G.; Zhuang, K.; Schiavone, G.; Fallegger, F.; Galan, K.; James, N.D.; Barraud, Q.; Delacombaz, M.; et al. Electrical Stimulation Of The Cervical Dorsal Roots Enables Functional Arm And Hand Movements In Monkeys With Cervical Spinal Cord Injury. bioRxiv 2020. [Google Scholar] [CrossRef]
- Sayenko, D.G.; Angeli, C.; Harkema, S.J.; Edgerton, V.R.; Gerasimenko, Y.P. Neuromodulation of evoked muscle potentials induced by epidural spinal-cord stimulation in paralyzed individuals. J. Neurophysiol. 2014, 111, 1088–1099. [Google Scholar] [CrossRef] [PubMed]
- Bareyre, F.M.; Kerschensteiner, M.; Raineteau, O.; Mettenleiter, T.C.; Weinmann, O.; Schwab, M. The injured spinal cord spontaneously forms a new intraspinal circuit in adult rats. Nat. Neurosci. 2004, 7, 269–277. [Google Scholar] [CrossRef]
- Bilchak, J.N.; Caron, G.; Côté, M.-P. Exercise-Induced Plasticity in Signaling Pathways Involved in Motor Recovery after Spinal Cord Injury. Int. J. Mol. Sci. 2021, 22, 4858. [Google Scholar] [CrossRef]
- Milosevic, M.; Masugi, Y.; Sasaki, A.; Sayenko, D.G.; Nakazawa, K. On the reflex mechanisms of cervical transcutaneous spinal cord stimulation in human subjects. J. Neurophysiol. 2019, 121, 1672–1679. [Google Scholar] [CrossRef]
- Hachmann, J.T.; Yousak, A.; Wallner, J.J.; Gad, P.N.; Edgerton, V.R.; Gorgey, A.S. Epidural spinal cord stimulation as an intervention for motor recovery after motor complete spinal cord injury. J. Neurophysiol. 2021, 126, 1843–1859. [Google Scholar] [CrossRef] [PubMed]
- Katoh, S.; El Masry, W.S. Neurological recovery after conservative treatment of cervical cord injuries. J. Bone Jt. Surg. 1994, 76, 225–228. [Google Scholar] [CrossRef]
- Poynton, A.R.; O’Farrell, D.; Shannon, F.; Murray, P.; McManus, F.; Walsh, M.G. Sparing of sensation to pin prick predicts recovery of a motor segment after injury to the spinal cord. J. Bone Jt. Surg. Br. 1997, 79, 952–954. [Google Scholar] [CrossRef]
- Meyer, C.; Hofstoetter, U.S.; Hubli, M.; Hassani, R.H.; Rinaldo, C.; Curt, A.; Bolliger, M. Immediate Effects of Transcutaneous Spinal Cord Stimulation on Motor Function in Chronic, Sensorimotor Incomplete Spinal Cord Injury. J. Clin. Med. 2020, 9, 3541. [Google Scholar] [CrossRef]
- Hofstoetter, U.S.; Freundl, B.; Danner, S.M.; Krenn, M.J.; Mayr, W.; Binder, H.; Minassian, K. Transcutaneous Spinal Cord Stimulation Induces Temporary Attenuation of Spasticity in Individuals with Spinal Cord Injury. J. Neurotrauma 2019, 37, 481–493. [Google Scholar] [CrossRef] [PubMed]
- Knikou, M.; Murray, L.M. Repeated transspinal stimulation decreases soleus H-reflex excitability and restores spinal inhibition in human spinal cord injury. PLoS ONE 2019, 14, e0223135. [Google Scholar] [CrossRef]
- Angeli, C.A.; Gerasimenko, Y. Combined cervical transcutaneous with lumbosacral epidural stimulation improves voluntary control of stepping movements in spinal cord injured individuals. Front. Bioeng. Biotechnol. 2023, 11, 1073716. [Google Scholar] [CrossRef] [PubMed]
- Calvert, J.S.; Gill, M.L.; Linde, M.B.; Veith, D.D.; Thoreson, A.R.; Lopez, C.; Lee, K.H.; Gerasimenko, Y.P.; Edgerton, V.R.; Lavrov, I.A.; et al. Voluntary Modulation of Evoked Responses Generated by Epidural and Transcutaneous Spinal Stimulation in Humans with Spinal Cord Injury. J. Clin. Med. 2021, 10, 4898. [Google Scholar] [CrossRef] [PubMed]
- Barss, T.S.; Parhizi, B.; Mushahwar, V.K. Transcutaneous spinal cord stimulation of the cervical cord modulates lumbar networks. J. Neurophysiol. 2020, 123, 158–166. [Google Scholar] [CrossRef] [PubMed]
- Balbinot, G.; Li, G.; Kalsi-Ryan, S.; Abel, R.; Maier, D.; Kalke, Y.-B.; Weidner, N.; Rupp, R.; Schubert, M.; Curt, A.; et al. Segmental motor recovery after cervical spinal cord injury relates to density and integrity of corticospinal tract projections. Nat. Commun. 2023, 14, 723. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.C.; Weber, K.; Parrish, T.; Hornby, T.G.; Tysseling, V.M.; McPherson, J.G.; Wasielewski, M.; Elliott, J.M. Ambulatory function in motor incomplete spinal cord injury: A magnetic resonance imaging study of spinal cord edema and lower extremity muscle morphometry. Spinal Cord 2017, 55, 672–678. [Google Scholar] [CrossRef]
- Flanders, A.; Spettell, C.M.; Tartaglino, L.M.; Friedman, D.P.; Herbison, G.J. Forecasting motor recovery after cervical spinal cord injury: Value of MR imaging. Radiology 1996, 201, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Al-Habib, A.F.; Attabib, N.; Ball, J.; Bajammal, S.; Casha, S.; Hurlbert, R.J.; Badhiwala, J.H.; Wilson, J.R.; Kulkarni, A.V.; Kiss, A.; et al. Clinical Predictors of Recovery after Blunt Spinal Cord Trauma: Systematic Review. J. Neurotrauma 2011, 28, 1431–1443. [Google Scholar] [CrossRef]
- Dietz, V.; Fouad, K. Restoration of sensorimotor functions after spinal cord injury. Brain 2013, 137 Pt 3, 654–667. [Google Scholar] [CrossRef]
- Kloosterman, M.G.M.; Snoek, G.J.; Jannink, M.J. Systematic review of the effects of exercise therapy on the upper extremity of patients with spinal-cord injury. Spinal Cord 2009, 47, 196–203. [Google Scholar] [CrossRef]
- Rejc, E.; Angeli, C.A.; Atkinson, D.; Harkema, S.J. Motor recovery after activity-based training with spinal cord epidural stimulation in a chronic motor complete paraplegic. Sci. Rep. 2017, 7, 13476. [Google Scholar] [CrossRef]
- Burns, A.S.; O’Connell, C. The challenge of spinal cord injury care in the developing world. J. Spinal Cord Med. 2012, 35, 3–8. [Google Scholar] [CrossRef]
- Khorasanizadeh, M.; Yousefifard, M.; Eskian, M.; Lu, Y.; Chalangari, M.; Harrop, J.S.; Jazayeri, S.B.; Seyedpour, S.; Khodaei, B.; Hosseini, M.; et al. Neurological recovery following traumatic spinal cord injury: A systematic review and meta-analysis. J. Neurosurg. Spine 2019, 30, 683–699. [Google Scholar] [CrossRef] [PubMed]
- Eldabe, S.; Buchser, E.; Duarte, R.V. Complications of Spinal Cord Stimulation and Peripheral Nerve Stimulation Techniques: A Review of the Literature. Pain Med. 2016, 17, 325–336. [Google Scholar] [CrossRef] [PubMed]
- Tolmacheva, A.; Savolainen, S.; Kirveskari, E.; Brandstack, N.; Mäkelä, J.P.; Shulga, A. Paired associative stimulation improves hand function after non-traumatic spinal cord injury: A case series. Clin. Neurophysiol. Pract. 2019, 4, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Francisco, G.E.; Yozbatiran, N.; Berliner, J.; O’Malley, M.K.; Pehlivan, A.U.; Kadivar, Z.; Fitle, K.; Boake, C. Robot-Assisted Training of Arm and Hand Movement Shows Functional Improvements for Incomplete Cervical Spinal Cord Injury. Am. J. Phys. Med. Rehabil. 2017, 96 (Suppl. S1), S171–S177. [Google Scholar] [CrossRef]
- McGeady, C.; Vučković, A.; Tharu, N.S.; Zheng, Y.-P.; Alam, M. Brain-Computer Interface Priming for Cervical Transcutaneous Spinal Cord Stimulation Therapy: An Exploratory Case Study. Front. Rehabil. Sci. 2022, 3, 896766. [Google Scholar] [CrossRef]
- Jovanovic, L.I.; Kapadia, N.; Zivanovic, V.; Rademeyer, H.J.; Alavinia, M.; McGillivray, C.; Kalsi-Ryan, S.; Popovic, M.R.; Marquez-Chin, C. Brain–computer interface-triggered functional electrical stimulation therapy for rehabilitation of reaching and grasping after spinal cord injury: A feasibility study. Spinal Cord Ser. Cases 2021, 7, 24. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Left | ||||||||
| Muscle | BB | TB | ECR | FCR | EDP | FDP | FDI | |
| Stimulation intensity (mA) | 5 | Pre: 47.37 ± 9.59 | Pre: 44.90 ± 2.62 | Pre: 44.47 ± 5.30 | Pre: 61.91 ± 6.85 | Pre: 38.22 ± 2.90 | Pre: 35.60 ± 4.54 | Pre: 36.91 ± 5.85 |
| Post: 37.20 ± 2.90 | Post: 40.42 ± 2.19 | Post: 33.28 ± 2.55 | Post: 38.80 ± 7.44 | Post: 46.94 ± 9.94 | Post: 59.50 ± 1.10 | Post: 39.82 ± 3.39 | ||
| t = 1.637 p = 0.243 | t = 2.825 p = 0.085 | t = 6.676 p = 0.021 | t = 2.956 p = 0.097 | t = −1.22 p = 0.344 | t = 2.102 p = 0.170 | t = −1.643 p = 0.241 | ||
| 60 | Pre: 344.27 ± 8.09 | Pre: 254.8.10 ± 8.10 | Pre: 54.21 ± 3.96 | Pre: 82.11 ± 20.28 | Pre: 99.98 ± 12.71 | Pre: 55.80 ± 4.95 | Pre: 93.01 ± 21.65 | |
| Post: 43.16 ± 1071 | Post: 59.00 ± 24.43 | Post: 51.01 ± 11.31 | Post: 83.71 ± 8.58 | Post: 41.71 ± 3.66 | Post: 51.30 ± 17.67 | Post: 47.67 ± 2.40 | ||
| t = 29.891 p = 0.001 | t = 20.575 p = 0.002 | t = 0.746 p = 0.533 | t = 3.465 p = 0.074 | t = 11.134 p = 0.007 | t = 0.348 p = 0.760 | t = 3.541 p = 0.071 | ||
| 90 | Pre: 406.76 ± 5.46 | Pre: 244.00 ± 11.38 | Pre: 79.78 ± 14.84 | Pre: 371.44 ± 17.42 | Pre: 162.03 ± 9.21 | Pre: 88.21 ± 8.07 | Pre: 203.74 ± 10.04 | |
| Post: 97.22 ± 3.72 | Post: 90.97 ± 2.63 | Post: 92.13 ± 7.66 | Post: 66.99 ± 3.15 | Post: 62.05 ± 8.00 | Post: 125.85 ± 1.65 | Post: 79.64 ± 5.62 | ||
| t = 127.519 p < 0.001 | t = 21.243 p = 0.002 | t = −0.952 p = 0.441 | t = 25.779 p = 0.001 | t = 84.052 p < 0.001 | t = −6.712 p = 0.021 | t = 13.726 p = 0.005 | ||
| 120 | Pre: 616.89 ± 6.60 | Pre: 424.19 ± 12.43 | Pre: 208.54 ± 24.42 | Pre: 610.79 ± 78.94 | Pre: 578.09 ± 11.05 | Pre: 164.21 ± 28.19 | Pre: 347.90 ± 6.58 | |
| Post: 103.32 ± 5.99 | Post: 90.83 ± 4.70 | Post: 151.86 ± 7.25 | Post: 89.23 ± 5.45 | Post: 89.37 ± 6.77 | Post: 146.63 ± 14.98 | Post: 88.50 ± 16.70 | ||
| t = 154.236 p < 0.001 | t = 41.959 p < 0.001 | t = 3.483 p = 0.073 | t = 11.011 p = 0.008 | t = 60.323 p < 0.001 | t = 1.371 p = 0.303 | t = 27.120 p = 0.001 | ||
| 150 | Pre: 9.7.39 ± 20.44 | Pre: 1225.64 ± 35.14 | Pre: 598.14 ± 28.18 | Pre: 1447.70 ± 18.76 | Pre: 835.31 ± 59.45 | Pre: 365.05 ± 2.40 | Pre: 754.95 ± 9.89 | |
| Post: 97.80 ± 8.94 | Post: 131.08 ± 6.54 | Post: 344.85 ± 87.60 | Post: 439.89 ± 47.40 | Post: 204.90 ± 12.36 | Post: 423.32 ± 16.07 | Post: 135.44 ± 3.21 | ||
| t = 73.577 p < 0.001 | t = 51.915 p < 0.001 | t = 4.721 p = 0.042 | t = 38.843 p < 0.001 | t = 16.119 p = 0.003 | t = −6.966 p = 0.019 | t = 123.062 p < 0.001 | ||
| Right | ||||||||
| Stimulation intensity (mA) | 5 | Pre: 33.13 ± 5.72 | Pre: 34.01 ± 5.23 | Pre: 38.66 ± 2.52 | Pre: 41.85 ± 0.76 | Pre: 40.84 ± 7.50 | Pre: 34.73 ± 2.97 | Pre: 47.52 ± 9.64 |
| Post: 51.59 ± 3.39 | Post: 44.61 ± 2.97 | Post: 71.35 ± 21.66 | Post: 39.24 ± 1.90 | Post: 55.95 ± 6.76 | Post: 59.87 ± 8.85 | Post: 64.96 ± 4.29 | ||
| t = −3.692 p = 0.066 | t = −2.392 p = 0.139 | t = −2.342 p = 0.143 | t = 3.927 p = 0.060 | t = −2.442 p = 0.134 | t = −3.872 p = 0.060 | t = −2.168 p = 0.162 | ||
| 60 | Pre: 106.23 ± 3.50 | Pre: 88.21 ± 14.94 | Pre: 102.60 ± 18.93 | Pre: 55.51 ± 2.90 | Pre: 126.72 ± 3.50 | Pre: 82.69 ± 12.59 | Pre: 45.34 ± 1.15 | |
| Post: 112.77 ± 13.91 | Post: 94.90 ± 4.58 | Post: 135.15 ± 17.50 | Post: 83.71 ± 8.58 | Post: 60.60 ± 13.59 | Post: 66.59 ± 16.81 | Post: 80.94 ± 11.15 | ||
| t = −0.991 p = 0.426 | t = −1.097 p = 0.386 | t = −5.142 p = 0.035 | t = −5.698 p = 0.029 | t = 8.022 p = 0.015 | t = 0.987 p = 0.439 | t = −5.3983 p = 0.032 | ||
| 90 | Pre: 184.56 ± 2.48 | Pre: 135.59 ± 5.57 | Pre: 196.91 ± 22.99 | Pre: 87.63 ± 15.16 | Pre: 210.86 ± 20.75 | Pre: 144.45 ± 16.45 | Pre: 68.01 ± 6.29 | |
| Post: 184.12 ± 26.10 | Post: 140.53 ± 2.06 | Post: 208.25 ± 9.41 | Post: 140.09 ± 19.50 | Post: 221.91 ± 6.80 | Post: 110.15 ± 11.47 | Post: 72.95 ± 10.70 | ||
| t = 0.026 p = 0.981 | t = −1.123 p = 0.378 | t = −0.654 p = 0.579 | t = −5.232 p = 0.034 | t = −0.893 p = 0.465 | t = 2.145 p = 0.165 | t = −1.114 p = 0.381 | ||
| 120 | Pre: 250.24 ± 16.99 | Pre: 202.87 ± 13.14 | Pre: 371.30 ± 6.93 | Pre: 333.66 ± 76.91 | Pre: 307.06 ± 16.37 | Pre: 687.95 ± 304.14 | Pre: 66.12 ± 10.11 | |
| Post: 311.13 ± 18.37 | Post: 546.70 ± 22.62 | Post: 794.18 ± 27.13 | Post: 671.82 ± 33.78 | Post: 462.70 ± 21.52 | Post: 385.10 ± 34.10 | Post: 75.28 ± 5.62 | ||
| t = −29.052 p < 0.001 | t = −52.371 p < 0.001 | t = −29.667 p < 0.001 | t = −13.450 p = 0.005 | t = −11.514 p = 0.007 | t = 1.661 p = 0.238 | t = −2.055 p = 0.176 | ||
| 150 | Pre: 355.89 ± 3.15 | Pre: 495.84 ± 73.21 | Pre: 320.73 ± 13.61 | Pre: 808.43 ± 20.18 | Pre: 554.84 ± 11.29 | Pre: 1655.22 ± 3.76 | Pre: 217.69 ± 26.67 | |
| Post: 660.49 ± 12.84 | Post: 1615.98 ± 11.07 | Post: 1230.59 ± 20.60 | Post: 1040.21 ± 14.99 | Post: 624.01 ± 22.71 | Post: 631.28 ± 10.42 | Post: 81.67 ± 7.33 | ||
| t = −45.088 p < 0.001 | t = −26.140 p = 0.001 | t = −49.095 p < 0.001 | t = −14.543 p = 0.004 | t = −10.444 p = 0.009 | t = 125.105 p < 0.001 | t = 7.710 p = 0.016 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sharma, P.; Panta, T.; Ugiliweneza, B.; Bert, R.J.; Gerasimenko, Y.; Forrest, G.; Harkema, S. Multi-Site Spinal Cord Transcutaneous Stimulation Facilitates Upper Limb Sensory and Motor Recovery in Severe Cervical Spinal Cord Injury: A Case Study. J. Clin. Med. 2023, 12, 4416. https://doi.org/10.3390/jcm12134416
Sharma P, Panta T, Ugiliweneza B, Bert RJ, Gerasimenko Y, Forrest G, Harkema S. Multi-Site Spinal Cord Transcutaneous Stimulation Facilitates Upper Limb Sensory and Motor Recovery in Severe Cervical Spinal Cord Injury: A Case Study. Journal of Clinical Medicine. 2023; 12(13):4416. https://doi.org/10.3390/jcm12134416
Chicago/Turabian StyleSharma, Pawan, Tudor Panta, Beatrice Ugiliweneza, Robert J. Bert, Yury Gerasimenko, Gail Forrest, and Susan Harkema. 2023. "Multi-Site Spinal Cord Transcutaneous Stimulation Facilitates Upper Limb Sensory and Motor Recovery in Severe Cervical Spinal Cord Injury: A Case Study" Journal of Clinical Medicine 12, no. 13: 4416. https://doi.org/10.3390/jcm12134416
APA StyleSharma, P., Panta, T., Ugiliweneza, B., Bert, R. J., Gerasimenko, Y., Forrest, G., & Harkema, S. (2023). Multi-Site Spinal Cord Transcutaneous Stimulation Facilitates Upper Limb Sensory and Motor Recovery in Severe Cervical Spinal Cord Injury: A Case Study. Journal of Clinical Medicine, 12(13), 4416. https://doi.org/10.3390/jcm12134416