
Helicobacter pylori Diagnostic Tests Used in Europe: Results of over 34,000 Patients from the European Registry on Helicobacter pylori Management

 , ,
, ,  , ,
, ,  , , , , , , ,
, , , , , , ,  ,
,  ,
,  , , ,
, , ,  , , , ,
, , , ,  , , , , , , and add
Show full author list
, , , , , , and add
Show full author list
Abstract
1. Introduction
2. Methods
2.1. European Registry on H. pylori Management
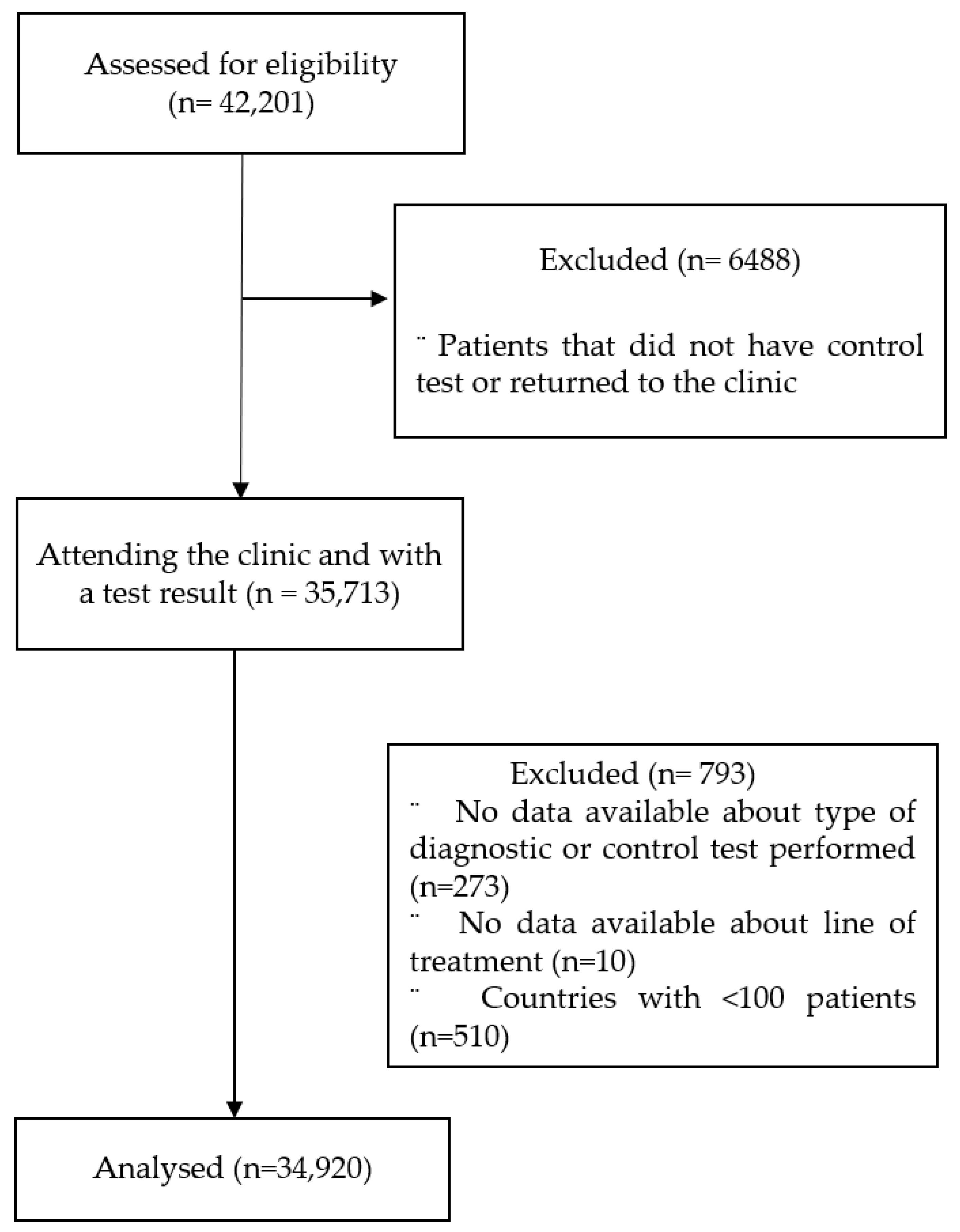
2.2. Patients
2.3. Data Management
2.4. Statistical Analyses
3. Results
3.1. Patients’ Characteristics
3.2. Initial Diagnosis in Treatment-naïve Patients
3.3. Evolution of the Initial Diagnostic Tests Used in Treatment-naïve Patients
3.4. Control Tests to Confirm the Eradication in Treatment-naïve and Rescue Treatment Patients
3.5. Evolution of the Control Tests
3.6. Use of Culture in Treatment-naïve and Rescue Treatment Patients
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Eusebi, L.H.; Zagari, R.M.; Bazzoli, F. Epidemiology of Helicobacter pylori infection. Helicobacter 2014, 19, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Burucoa, C.; Axon, A. Epidemiology of Helicobacter pylori infection. Helicobacter 2017, 22 (Suppl. S1). [Google Scholar] [CrossRef] [PubMed]
- Peleteiro, B.; Bastos, A.; Ferro, A.; Lunet, N. Prevalence of Helicobacter pylori Infection Worldwide: A Systematic Review of Studies with National Coverage. Dig. Dis. Sci. 2014, 59, 1698–1709. [Google Scholar] [CrossRef] [PubMed]
- De Brito, B.B.; Da Silva, F.A.F.; Soares, A.S.; Pereira, V.A.; Cordeiro Santos, M.L.; Sampaio, M.M.; Neves, P.H.M.; de Melo, F.F. Pathogenesis and clinical management of Helicobacter pylori gastric infection. World J. Gastroenterol. 2019, 25, 5578–5589. [Google Scholar] [CrossRef] [PubMed]
- Gisbert, J.P.; Alcedo, J.; Amador, J.; Bujanda, L.; Calvet, X.; Castro-Fernández, M.; Fernández-Salazar, L.; Gené, E.; Lanas, Á.; Lucendo, A.J.; et al. V Spanish Consensus Conference on Helicobacter pylori infection treatment. Gastroenterol. Hepatol. 2022, 45, 392–417. [Google Scholar] [CrossRef]
- Malfertheiner, P.; Megraud, F.; O’Morain, C.; Gisbert, J.P.; Kuipers, E.J.; Axon, A.; Bazzoli, F.; Gasbarrini, A.; Atherton, J.; Graham, D.Y.; et al. Management of Helicobacter pylori infection-the Maastricht V/Florence consensus report. Gut 2017, 66, 6–30. [Google Scholar] [CrossRef]
- Gisbert, J.P.; Pajares, J.M. Review article: 13 C-urea breath test in the diagnosis of Helicobacter pylori infection—A critical review. Aliment. Pharmacol. Ther. 2004, 20, 1001–1017. [Google Scholar] [CrossRef]
- Gisbert, J.P.; de la Morena, F.; Abraira, V. Accuracy of Monoclonal Stool Antigen Test for the Diagnosis of H. pylori Infection: A Systematic Review and Meta-Analysis. Am. J. Gastroenterol. 2006, 101, 1921–1930. [Google Scholar] [CrossRef]
- Gisbert, J.P.; Calvet, X.; Ferrándiz, J.; Mascort, J.; Alonso-Coello, P.; Marzo, M. Clinical practice guideline on the management of patients with dyspepsia. Update 2012. Gastroenterol. Hepatol. 2012, 35, 725.e1-38. [Google Scholar]
- Gisbert, J.P. Empirical or susceptibility-guided treatment for Helicobacter pylori infection? A comprehensive review. Ther. Adv. Gastroenterol. 2020, 13, 1756284820968736. [Google Scholar] [CrossRef]
- López-Góngora, S.; Puig, I.; Calvet, X.; Villoria, A.; Baylina, M.; Muñoz, N.; Sanchez-Delgado, J.; Suarez, D.; García-Hernando, V.; Gisbert, J.P. Systematic review and meta-analysis: Susceptibility-guided versus empirical antibiotic treatment for Helicobacter pylori infection. J. Antimicrob. Chemother. 2015, 70, 2447–2455. [Google Scholar] [CrossRef] [PubMed]
- Bujanda, L.; Nyssen, O.P.; Vaira, D.; Saracino, I.M.; Fiorini, G.; Lerang, F.; Georgopoulos, S.; Tepes, B.; Heluwaert, F.; Gasbarrini, A.; et al. Antibiotic Resistance Prevalence and Trends in Patients Infected with Helicobacter pylori in the Period 2013-2020: Results of the European Registry on H. pylori Management (Hp-EuReg). Antibiotics 2021, 10, 1058. [Google Scholar] [PubMed]
- Gisbert, J.P.; Calvet, X. Helicobacter pylori “test-and-treat” strategy for management of dyspepsia: A comprehensive review. Clin. Transl. Gastroenterol. 2013, 4, e32. [Google Scholar] [CrossRef] [PubMed]
- Black, C.J.; Houghton, L.A.; Ford, A.C. Insights into the evaluation and management of dyspepsia: Recent developments and new guidelines. Ther. Adv. Gastroenterol. 2018, 11, 1756284818805597. [Google Scholar] [CrossRef] [PubMed]
- McNicholl, A.G.; O’Morain, C.A.; Megraud, F.; Gisbert, J.P. Protocol of the European Registry on the management of Helicobacter pylori infection (Hp-EuReg). Helicobacter 2019, 24, e12630. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Nyssen, O.P.; Vaira, D.; Tepes, B.; Kupcinskas, L.; Bordin, D.; Pérez-Aisa, Á.; Gasbarrini, A.; Castro-Fernández, M.; Bujanda, L.; Garre, A.; et al. Room for Improvement in the Treatment of Helicobacter pylori Infection Lessons from the European Registry on H. pylori Management (Hp-EuReg). J. Clin. Gastroenterol. 2022, 56, e98–e108. [Google Scholar] [CrossRef]
- Mahachai, V.; Vilaichone, R.; Pittayanon, R.; Rojborwonwitaya, J.; Leelakusolvong, S.; Maneerattanaporn, M.; Chotivitayatarakorn, P.; Treeprasertsuk, S.; Kositchaiwat, C.; Pisespongsa, P.; et al. Helicobacter pylori management in ASEAN: The Bangkok consensus report. J. Gastroenterol. Hepatol. 2018, 33, 37–56. [Google Scholar] [CrossRef]
- Liou, J.-M.; Malfertheiner, P.; Lee, Y.-C.; Sheu, B.-S.; Sugano, K.; Cheng, H.-C.; Yeoh, K.-G.; Hsu, P.-I.; Goh, K.-L.; Mahachai, V.; et al. Screening and eradication of Helicobacter pylori for gastric cancer prevention: The Taipei global consensus. Gut 2020, 69, 2093–2112. [Google Scholar] [CrossRef]
- El-Serag, H.B.; Kao, J.Y.; Kanwal, F.; Gilger, M.; LoVecchio, F.; Moss, S.F.; Crowe, S.; Elfant, A.; Haas, T.; Hapke, R.J.; et al. Houston Consensus Conference on Testing for Helicobacter pylori Infection in the United States. Clin. Gastroenterol. Hepatol. 2018, 16, 992–1002. [Google Scholar] [CrossRef] [PubMed]
- Moayyedi, P.; Talley, N.J.; Fennerty, M.B.; Vakil, N. Can the Clinical History Distinguish Between Organic and Functional Dyspepsia? JAMA 2006, 295, 1566. [Google Scholar] [CrossRef] [PubMed]
- Savoldi, A.; Carrara, E.; Graham, D.Y.; Conti, M.; Tacconelli, E. Prevalence of Antibiotic Resistance in Helicobacter pylori: A Systematic Review and Meta-analysis in World Health Organization Regions. Gastroenterology 2018, 155, 1372–1382. [Google Scholar] [CrossRef] [PubMed]
- Romano, M.; Marmo, R.; Cuomo, A.; De Simone, T.; Mucherino, C.; Iovene, M.R.; Montella, F.; Tufano, M.A.; Blanco, C.D.V.; Nardone, G. Pretreatment antimicrobial susceptibility testing is cost saving in the eradication of Helicobacter pylori. Clin. Gastroenterol. Hepatol. 2003, 1, 273–278. [Google Scholar] [CrossRef]
- Cosme, A.; Montes, M.; Martos, M.; Gil, I.; Mendarte, U.; Salicio, Y.; Piñeiro, L.; Recasens, M.; Ibarra, B.; Sarasqueta, C.; et al. Usefulness of antimicrobial susceptibility in the eradication of Helicobacter pylori. Clin. Microbiol. Infect. 2013, 19, 379–383. [Google Scholar] [CrossRef] [PubMed]
- Baylina, M.; Muñoz, N.; Sánchez-Delgado, J.; López-Góngora, S.; Calvet, X.; Puig, I. Systematic review: Would susceptibility-guided treatment achieve acceptable cure rates for second-line Helicobacter pylori therapy as currently practiced? Helicobacter 2019, 24, e12584. [Google Scholar] [CrossRef]


{kind=link}
| Overall n (%) N = 34,920 | Treatment-naïve n (%) N = 27,776 | Rescue Treatments n (%) N = 7144 | ||
|---|---|---|---|---|
| Age; years (Mean (±SD)) | 51.0 (13.7) | 50.3 (15.1) | 50.4 (14.2) | |
| Age | <50 years 50 years | 16,467 (47.2) 18,400 (52.8) | 13,179 (47.5) 14,554 (52.5) | 3288 (46.1) 3846 (53.9) |
| Gender | Female Male | 21,350 (61.2) 13,545 (38.8) | 16,677 (60.1) 11,079 (39.9) | 4673 (65.5) 2466 (34.5) |
| Ethnicity | Caucasian | 31,058 (89.1) | 24,611 (88.8) | 6447 (90.5) |
| Black | 272 (0.8) | 193 (0.7) | 79 (1.1) | |
| Asian | 420 (1.2) | 330 (1.2) | 90 (1.3) | |
| Other | 2299 (6.6) | 1973 (7.1) | 326 (4.6) | |
| Not available | 796 (2.3) | 615 (2.2) | 181 (2.5) |
| n (% *) | |
|---|---|
| Non-invasive test | 11,369 (40.9) |
| 13C-urea breath test | 7472 (26.9) |
| 14C-urea breath test | 115 (0.4) |
| Serology | 1824 (6.6) |
| Monoclonal stool antigen test | 1915 (6.9) |
| Polyclonal stool antigen test | 282 (1) |
| Invasive test | 19,801 (71.3) |
| Histology | 11,885 (42.8) |
| Rapid urease test | 10,636 (38.3) |
| Culture | 2927 (10.5) |
| Biochemical methods (PCR, FISH) | 265 (1) |
| Patients with Invasive Diagnostic Test, n/N (%) | Patients <50 yo with Invasive Diagnostic Test, n/N <50 yo (%) | Patients ≥50 yo with Invasive Diagnostic Test, n/N ≥50 yo (%) | p-Value | |
|---|---|---|---|---|
| Azerbaijan | 565/570 (99.1) | 382/386 (99.0) | 183/184 (99.5) | 1.000 |
| Croatia | 277/338 (82.0) | 70/99 (70.7) | 207/239 (86.6) | 0.001 * |
| France | 101/107 (94.4) | 46/49 (93.9) | 55/58 (94.8) | 1.000 |
| Germany | 101/132 (76.5) | 40/55 (72.7) | 61/77 (79.2) | 0.386 |
| Greece | 497/541 (91.9) | 184/211 (87.2) | 313/330 (94.8) | 0.002 * |
| Hungary | 194/233 (83.3) | 77/95 (81.1) | 117/138 (84.8) | 0.454 |
| Ireland | 221/313 (70.6) | 90/164 (54.9) | 131/149 (87.9) | <0.001 * |
| Israel | 59/103 (57.3) | 21/52 (40.4) | 38/51 (74.5) | <0.001 * |
| Italy | 2213/2629 (84.2) | 904/1117 (80.9) | 1300/1485 (87.5) | <0.001 * |
| Latvia | 426/528 (80.7) | 250/326 (76.7) | 176/202 (87.1) | 0.003 * |
| Lithuania | 397/512 (77.5) | 149/203 (73.4) | 248/309 (80.3) | 0.069 |
| Norway | 598/740, (80.8) | 215/261 (82.4) | 383/479 (80.0) | 0.425 |
| Portugal | 337/347 (97.1) | 103/107 (96.3) | 233/239 (97.5) | 0.506 |
| Russia | 3520/5245 (67.1) | 1871/2879 (65.0) | 1648/2364 (69.7) | <0.001 * |
| Serbia | 67/92 (72.8) | 16/31 (51.6) | 51/61 (83.6) | 0.001 * |
| Slovenia | 2304/2411 (95.6) | 952/983 (96.8) | 1352/1428 (94.7) | 0.011 * |
| Spain | 7482/12,331 (60.7) | 3027/5876 (51.5) | 4447/6442 (69.0) | <0.001 * |
| Turkey | 247/264 (93.6) | 137/150 (91.3) | 110/114 (96.5) | 0.091 |
| United Kingdom | 98/195 (50.3) | 18/62 (29.0) | 80/133 (60.2) | <0.001 * |
| Ukraine | 97/145 (66.9) | 51/73 (69.9) | 46/72 (63.9) | 0.445 |
| TOTAL | 19,801/27,776 (71.3) | 8603/13,179 (65.3) | 11,179/14,554 (76.8) | <0.001 * |
| Non-Invasive Diagnostic Test | Invasive Diagnostic Test | p-Value | ||
|---|---|---|---|---|
| Age, mean (25–75th percentiles) (continuous) * | 46 [(35–58) | 53 (41–63) | <0.001 ** | |
| Age, n (%) (categorical) | <50 years | 4576 (39.7) | 6955 (60.3) | <0.001 ** |
| ≥50 years | 3375 (26.3) | 9435 (73.7) | ||
| Gender, n (%) | Female | 5028 (34.3) | 9627 (65.7) | <0.001 ** |
| Male | 2943 (30.3) | 6768 (69.7) | ||
| Ethnic background, n (%) | Caucasian | 6776 (30.9) | 15,137 (69.1) | 0.509 |
| Black | 45 (31.7) | 97 (68.3) | ||
| Asian | 72 (34.6) | 136 (65.4) | ||
| Azerbaijan | 5 (0.9) | 564 (99.1) | ||
| Country, n (%) | Croatia | 61 (18.3) | 273 (81.7) | <0.001 ** |
| France | 6 (5.9) | 96 (94.1) | ||
| Germany | 31 (25.6) | 90 (74.4%) | ||
| Greece | 44 (8.5) | 474 (91.5) | ||
| Hungary | 39 (27.5) | 103 (72.5) | ||
| Ireland | 92 (29.7) | 218 (70.3) | ||
| Israel | 44 (44.4) | 55 (55.6) | ||
| Italy | 416 (49.8) | 420 (50.2) | ||
| Latvia | 102 (19.7) | 416 (80.3) | ||
| Lithuania | 115 (22.9) | 387 (77.1) | ||
| Norway | 142 (21.8) | 510 (78.2) | ||
| Portugal | 10 (2.9) | 336 (97.1) | ||
| Russia | 1725 (40) | 2585 (60) | ||
| Serbia | 25 (29.1) | 61 (70.9) | ||
| Slovenia | 107 (4.7) | 2170 (95.3) | ||
| Spain | 4849 (40.2) | 7218 (59.8) | ||
| Turkey | 17 (6.5) | 245 (93.5) | ||
| United Kingdom | 97 (51.1) | 93 (48.9) | ||
| Ukraine | 48 (34) | 93 (66) | ||
| Overall, n (%) N = 34,920 | First-Line, n (%) N = 27,776 | Rescue Treatments, n (%) N = 7144 | |
|---|---|---|---|
| Non-invasive test | 32,540 (93.2) | 25,772 (92.8) | 6768 (94.7) |
| 13C-urea breath test | 27,320 (78.2) | 21,297 (76.7) | 6023 (84.3) |
| 14C-urea breath test | 389 (1.1) | 322 (1.2) | 67 (0.9) |
| Serology | 388 (1.1) | 302 (1.1) | 86 (1.2) |
| Monoclonal stool antigen test | 3673 (10.5) | 3117 (11.2) | 556 (7.8) |
| Polyclonal stool antigen test | 1259 (3.6) | 1172 (4.2) | 87 (1.2) |
| Invasive test | 2983 (8.5) | 2458 (8.8) | 525 (7.3) |
| Histology | 1887 (5.4) | 1533 (5.5) | 354 (5.0) |
| Rapid Urease Test | 1223 (3.5) | 1040 (3.7) | 183 (2.6) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Morales, N.; Pérez-Aísa, Á.; Fiorini, G.; Tepes, B.; Castro-Fernández, M.; Lucendo, A.; Voynovan, I.; Bujanda, L.; Garre, A.; Rodrigo, L.; et al. Helicobacter pylori Diagnostic Tests Used in Europe: Results of over 34,000 Patients from the European Registry on Helicobacter pylori Management. J. Clin. Med. 2023, 12, 4363. https://doi.org/10.3390/jcm12134363
García-Morales N, Pérez-Aísa Á, Fiorini G, Tepes B, Castro-Fernández M, Lucendo A, Voynovan I, Bujanda L, Garre A, Rodrigo L, et al. Helicobacter pylori Diagnostic Tests Used in Europe: Results of over 34,000 Patients from the European Registry on Helicobacter pylori Management. Journal of Clinical Medicine. 2023; 12(13):4363. https://doi.org/10.3390/jcm12134363
Chicago/Turabian StyleGarcía-Morales, Natalia, Ángeles Pérez-Aísa, Giulia Fiorini, Bojan Tepes, Manuel Castro-Fernández, Alfredo Lucendo, Irina Voynovan, Luis Bujanda, Ana Garre, Luis Rodrigo, and et al. 2023. "Helicobacter pylori Diagnostic Tests Used in Europe: Results of over 34,000 Patients from the European Registry on Helicobacter pylori Management" Journal of Clinical Medicine 12, no. 13: 4363. https://doi.org/10.3390/jcm12134363
APA StyleGarcía-Morales, N., Pérez-Aísa, Á., Fiorini, G., Tepes, B., Castro-Fernández, M., Lucendo, A., Voynovan, I., Bujanda, L., Garre, A., Rodrigo, L., Martínez Domínguez, S. J., Denkovski, M., Huguet Malavés, J. M., Jonaitis, L., Bumane, R., Zaytsev, O., Mata Romero, P., Barrio, J., Fernández-Salazar, L., ... on behalf of Hp-EuReg Investigators. (2023). Helicobacter pylori Diagnostic Tests Used in Europe: Results of over 34,000 Patients from the European Registry on Helicobacter pylori Management. Journal of Clinical Medicine, 12(13), 4363. https://doi.org/10.3390/jcm12134363