
Total Globulin Fraction at Diagnosis Could Forecast All-Cause Mortality during the Disease Course in Patients with Antineutrophil Cytoplasmic Antibody-Associated Vasculitis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Clinical Data
2.3. Calculation of TGF
2.4. Statistical Analyses
3. Results
3.1. Characteristics of AAV Patients
3.2. Correlation Analysis
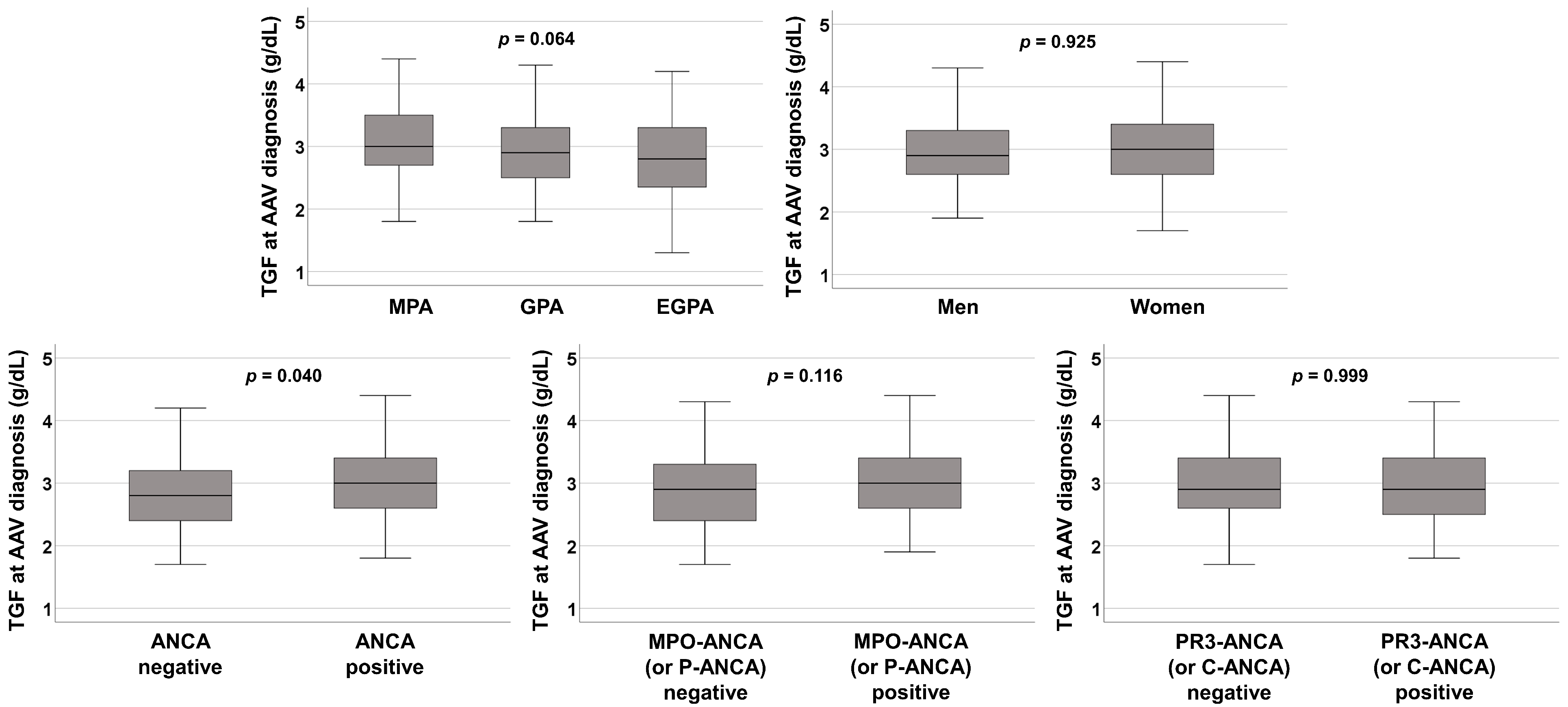
3.3. Comparison of TGF at AAV Diagnosis among the Groups
3.4. Optimal Cut-Off of TGF at AAV Diagnosis for All-Cause Mortality during Follow-Up
3.5. Comparison of Cumulative Patients’ Survival Rate according to the Cut-Off of TGF at AAV Diagnosis
3.6. Cox Hazards Model Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jennette, J.C.; Falk, R.J.; Bacon, P.A.; Basu, N.; Cid, M.C.; Ferrario, F.; Flores-Suarez, L.F.; Gross, W.L.; Guillevin, L.; Hagen, E.C.; et al. 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum. 2013, 65, 1–11. [Google Scholar] [CrossRef]
- Watts, R.; Lane, S.; Hanslik, T.; Hauser, T.; Hellmich, B.; Koldingsnes, W.; Mahr, A.; Segelmark, M.; Cohen-Tervaert, J.W.; Scott, D. Development and validation of a consensus methodology for the classification of the ANCA-associated vasculitides and polyarteritis nodosa for epidemiological studies. Ann. Rheum. Dis. 2007, 66, 222–227. [Google Scholar] [CrossRef] [Green Version]
- Wallace, Z.S.; Fu, X.; Harkness, T.; Stone, J.H.; Zhang, Y.; Choi, H. All-cause and cause-specific mortality in ANCA-associated vasculitis: Overall and according to ANCA type. Rheumatology 2020, 59, 2308–2315. [Google Scholar] [CrossRef] [PubMed]
- Scherlinger, M.; Mertz, P.; Sagez, F.; Meyer, A.; Felten, R.; Chatelus, E.; Javier, R.M.; Sordet, C.; Martin, T.; Korganow, A.S.; et al. Worldwide trends in all-cause mortality of auto-immune systemic diseases between 2001 and 2014. Autoimmun. Rev. 2020, 19, 102531. [Google Scholar] [CrossRef] [PubMed]
- Dagostin, M.A.; Nunes, S.L.O.; Shinjo, S.K.; Pereira, R.M.R. Mortality predictors in ANCA-associated vasculitis: Experience of a Brazilian monocentric cohort of a rheumatology center. Medicine 2021, 100, e28305. [Google Scholar] [CrossRef] [PubMed]
- Floyd, L.; Morris, A.; Joshi, M.; Dhaygude, A. Glucocorticoid Therapy in ANCA Vasculitis: Using the Glucocorticoid Toxicity Index as an Outcome Measure. Kidney360 2021, 2, 1002–1010. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.A.; Dehghan, N.; Chen, W.; Xie, H.; Esdaile, J.M.; Avina-Zubieta, J.A. Mortality in ANCA-associated vasculitis: A meta-analysis of observational studies. Ann. Rheum. Dis. 2017, 76, 1566–1574. [Google Scholar] [CrossRef]
- Murray, C.J.; Atkinson, C.; Bhalla, K.; Birbeck, G.; Burstein, R.; Chou, D.; Dellavalle, R.; Danaei, G.; Ezzati, M.; Fahimi, A.; et al. The state of US health, 1990–2010: Burden of diseases, injuries, and risk factors. JAMA 2013, 310, 591–608. [Google Scholar] [CrossRef] [Green Version]
- Laudin, G.E.; Levay, P.F.; Coetzer, B. Globulin fraction and albumin: Globulin ratio as a predictor of mortality in a South African multiple myeloma cohort. Int. J. Hematol. Oncol. 2020, 9, IJH27. [Google Scholar] [CrossRef]
- Hashash, J.G.; Koutroumpakis, F.; Anderson, A.M.; Rivers, C.R.; Hosni, M.; Koutroubakis, I.E.; Ahsan, M.; Gkiaouraki, E.; Dunn, M.A.; Schwartz, M.; et al. Elevated serum globulin fraction as a biomarker of multiyear disease severity in inflammatory bowel disease. Ann. Gastroenterol. 2022, 35, 609–617. [Google Scholar] [CrossRef]
- Pyo, J.Y.; Lee, L.E.; Park, Y.B.; Lee, S.W. Comparison of the 2022 ACR/EULAR Classification Criteria for Antineutrophil Cytoplasmic Antibody-Associated Vasculitis with Previous Criteria. Yonsei Med. J. 2023, 64, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Suppiah, R.; Robson, J.C.; Grayson, P.C.; Ponte, C.; Craven, A.; Khalid, S.; Judge, A.; Hutchings, A.; Merkel, P.A.; Luqmani, R.A.; et al. 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology Classification Criteria for Microscopic Polyangiitis. Ann. Rheum. Dis. 2022, 81, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Robson, J.C.; Grayson, P.C.; Ponte, C.; Suppiah, R.; Craven, A.; Judge, A.; Khalid, S.; Hutchings, A.; Watts, R.A.; Merkel, P.A.; et al. 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology Classification Criteria for Granulomatosis with Polyangiitis. Ann. Rheum. Dis. 2022, 81, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Grayson, P.C.; Ponte, C.; Suppiah, R.; Robson, J.C.; Craven, A.; Judge, A.; Khalid, S.; Hutchings, A.; Luqmani, R.A.; Watts, R.A.; et al. 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology Classification Criteria for Eosinophilic Granulomatosis with Polyangiitis. Ann. Rheum. Dis. 2022, 81, 309–314. [Google Scholar] [CrossRef] [PubMed]
- Mukhtyar, C.; Lee, R.; Brown, D.; Carruthers, D.; Dasgupta, B.; Dubey, S.; Flossmann, O.; Hall, C.; Hollywood, J.; Jayne, D.; et al. Modification and validation of the Birmingham Vasculitis Activity Score (version 3). Ann. Rheum. Dis. 2009, 68, 1827–1832. [Google Scholar] [CrossRef] [PubMed]
- Guillevin, L.; Pagnoux, C.; Seror, R.; Mahr, A.; Mouthon, L.; Toumelin, P.L.; French Vasculitis Study Group (FVSG). The Five-Factor Score revisited: Assessment of prognoses of systemic necrotizing vasculitides based on the French Vasculitis Study Group (FVSG) cohort. Medicine 2011, 90, 19–27. [Google Scholar] [CrossRef]
- Kronbichler, A.; Leierer, J.; Gauckler, P.; Shin, J.I. Comorbidities in ANCA-associated vasculitis. Rheumatology 2020, 59, iii79–iii83. [Google Scholar] [CrossRef]
- Nelveg-Kristensen, K.E.; Szpirt, W.; Carlson, N.; McClure, M.; Jayne, D.; Dieperink, H.; Gregersen, J.W.; Krarup, E.; Ivarsen, P.; Torp-Pedersen, C.; et al. Increasing incidence and improved survival in ANCA-associated vasculitis-a Danish nationwide study. Nephrol. Dial. Transpl. 2021, 37, 63–71. [Google Scholar] [CrossRef]
- Cohen Tervaert, J.W. Cardiovascular disease due to accelerated atherosclerosis in systemic vasculitides. Best. Pract. Res. Clin. Rheumatol. 2013, 27, 33–44. [Google Scholar] [CrossRef]
- Monach, P.A.; Warner, R.L.; Tomasson, G.; Specks, U.; Stone, J.H.; Ding, L.; Fervenza, F.C.; Fessler, B.J.; Hoffman, G.S.; Iklé, D.; et al. Serum proteins reflecting inflammation, injury and repair as biomarkers of disease activity in ANCA-associated vasculitis. Ann. Rheum. Dis. 2013, 72, 1342–1350. [Google Scholar] [CrossRef] [Green Version]
- Ahn, S.S.; Park, Y.B.; Lee, S.W. Serological Biomarkers and Indices for the Current Activity and Prognosis of ANCA-Associated Vasculitis: Experience in a Single Centre in Korea. Yonsei Med. J. 2021, 62, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Holding, S.; Khan, S.; Sewell, W.A.; Jolles, S.; Dore, P.C. Using calculated globulin fraction to reduce diagnostic delay in primary and secondary hypogammaglobulinaemias: Results of a demonstration project. Ann. Clin. Biochem. 2015, 52, 319–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, C.B.; Park, Y.B.; Lee, S.W. Antineutrophil Cytoplasmic Antibody-Associated Vasculitis in Korea: A Narrative Review. Yonsei Med. J. 2019, 60, 10–21. [Google Scholar] [CrossRef] [PubMed]
- Kitching, A.R.; Anders, H.J.; Basu, N.; Brouwer, E.; Gordon, J.; Jayne, D.R.; Kullman, J.; Lyons, P.A.; Merkel, P.A.; Savage, C.O.S.; et al. ANCA-associated vasculitis. Nat. Rev. Dis. Prim. 2020, 6, 71. [Google Scholar] [CrossRef]
- Vega, L.E.; Espinoza, L.R. Predictors of Poor Outcome in ANCA-Associated Vasculitis (AAV). Curr. Rheumatol. Rep. 2016, 18, 70. [Google Scholar] [CrossRef]
- Arques, S. Human serum albumin in cardiovascular diseases. Eur. J. Intern. Med. 2018, 52, 8–12. [Google Scholar] [CrossRef]
- Ma, L.; Zhao, S. Risk factors for mortality in patients undergoing hemodialysis: A systematic review and meta-analysis. Int. J. Cardiol. 2017, 238, 151–158. [Google Scholar] [CrossRef]
- Ahn, S.S.; Yoo, J.; Jung, S.M.; Song, J.J.; Park, Y.B.; Lee, S.W. Clinical role of albumin to globulin ratio in microscopic polyangiitis: A retrospective monocentric study. Clin. Rheumatol. 2019, 38, 487–494. [Google Scholar] [CrossRef]
- Xu, P.C.; Tong, Z.Y.; Chen, T.; Gao, S.; Hu, S.Y.; Yang, X.W.; Yan, T.K.; Lin, S. Hypoalbuminaemia in antineutrophil cytoplasmic antibody-associated vasculitis: Incidence and significance. Clin. Exp. Rheumatol. 2018, 36, 603–611. [Google Scholar]
- O’Connell, T.X.; Horita, T.J.; Kasravi, B. Understanding and interpreting serum protein electrophoresis. Am. Fam. Physician 2005, 71, 105–112. [Google Scholar]
- Kim, J.H. Multicollinearity and misleading statistical results. Korean J. Anesth. 2019, 72, 558–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Values |
|---|---|
| Variables at diagnosis | |
| Demographic data | |
| Age (years) | 60.0 (49.0–69.0) |
| Male sex (N, (%)) | 101 (35.7) |
| BMI (kg/m2) | 22.7 (20.3–24.6) |
| Ex-smoker (N, (%)) | 9 (3.2) |
| AAV subtype (N, (%)) | |
| MPA | 155 (54.8) |
| GPA | 72 (25.4) |
| EGPA | 56 (19.8) |
| ANCA type and positivity (N, (%)) | |
| MPO-ANCA (or P-ANCA) positivity | 195 (68.9) |
| PR3-ANCA (or C-ANCA) positivity | 45 (15.9) |
| ANCA negativity | 55 (19.4) |
| AAV-specific indices | |
| BVAS | 12.0 (7.0–18.0) |
| FFS | 1.0 (0–2.0) |
| Laboratory results | |
| White blood cell count (/mm3) | 9280.0 (6420.0–13,010.0) |
| Haemoglobin (g/dL) | 11.4 (9.5–13.2) |
| Platelet count (×1000/mm3) | 294.0 (227.0–389.0) |
| Blood urea nitrogen (mg/dL) | 17.7 (12.5–31.0) |
| Serum creatinine (mg/dL) | 0.9 (0.7–1.8) |
| Serum total protein (g/dL) | 6.6 (6.0–7.2) |
| Serum albumin (g/dL) | 3.7 (3.1–4.2) |
| ESR (mm/h) | 56.0 (21.5–95.0) |
| CRP (mg/L) | 13.2 (1.6–64.9) |
| Total globulin fraction (g/dL) | 2.9 (2.6–3.4) |
| Comorbidities (N, (%)) | |
| T2DM | 75 (26.5) |
| Hypertension | 114 (40.3) |
| Dyslipidaemia | 58 (20.5) |
| Variables during the disease course | |
| All-cause mortality (N, (%)) | 39 (13.8) |
| Follow-up duration based on all-cause mortality (months) | 46.9 (16.8–79.0) |
| Medications (N, (%)) | |
| Glucocorticoids | 267 (94.3) |
| Cyclophosphamide | 157 (55.5) |
| Rituximab | 50 (17.7) |
| Mycophenolate mofetil | 54 (19.1) |
| Azathioprine | 149 (52.7) |
| Tacrolimus | 24 (8.5) |
| Methotrexate | 23 (8.1) |
| Variables | Univariable | Multivariable | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p Value | HR | 95% CI | p Value | |
| Age (years) | 1.063 | 1.031, 1.095 | <0.001 | 1.037 | 1.002, 1.072 | 0.036 |
| Male sex (N, (%)) | 2.702 | 1.430, 5.103 | 0.002 | 3.136 | 1.495, 6.580 | 0.002 |
| BMI (kg/m2) | 1.122 | 1.029, 1.225 | 0.010 | 1.114 | 1.001, 1.238 | 0.047 |
| Ex-smoker (N, (%)) | 1.619 | 0.389, 6.732 | 0.508 | |||
| MPO-ANCA (or P-ANCA) positivity | 1.409 | 0.699, 2.843 | 0.338 | |||
| PR3-ANCA (or C-ANCA) positivity | 0.693 | 0.271, 1.772 | 0.444 | |||
| BVAS | 1.082 | 1.038, 1.128 | <0.001 | 1.043 | 0.984, 1.107 | 0.156 |
| FFS | 1.927 | 1.423, 2.609 | <0.001 | 1.359 | 0.951, 2.046 | 0.089 |
| T2DM | 1.083 | 0.547, 2.143 | 0.819 | |||
| Hypertension | 1.129 | 0.600, 2.125 | 0.706 | |||
| Dyslipidaemia | 1.808 | 0.915, 3.574 | 0.088 | |||
| White blood cell count (/mm3) | 1.000 | 1.000, 1.000 | 0.047 | 1.000 | 1.000, 1.000 | 0.804 |
| Haemoglobin (g/dL) | 0.787 | 0.680, 0.911 | 0.001 | 0.932 | 0.740, 1.173 | 0.547 |
| Platelet count (×1000/mm3) | 1.000 | 0.998, 1.002 | 0.765 | |||
| Fasting glucose (mg/dL) | 1.005 | 0.999, 1.010 | 0.112 | |||
| Blood urea nitrogen (mg/dL) | 1.011 | 1.003, 1.019 | 0.005 | 1.000 | 0.985, 1.016 | 0.961 |
| Serum creatinine (mg/dL) | 1.139 | 1.014, 1.279 | 0.028 | 1.078 | 0.863, 1.347 | 0.508 |
| ESR (mm/h) | 1.010 | 1.002, 1.019 | 0.013 | 0.993 | 0.981, 1.006 | 0.295 |
| CRP (mg/L) | 1.008 | 1.004, 1.013 | <0.001 | 1.004 | 0.997, 1.011 | 0.295 |
| TGF ≥ 3.1 g/dL | 2.197 | 1.152, 4.192 | 0.017 | 2.611 | 1.223, 5.572 | 0.013 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ha, J.-W.; Ahn, S.-S.; Song, J.-J.; Park, Y.-B.; Lee, S.-W. Total Globulin Fraction at Diagnosis Could Forecast All-Cause Mortality during the Disease Course in Patients with Antineutrophil Cytoplasmic Antibody-Associated Vasculitis. J. Clin. Med. 2023, 12, 4170. https://doi.org/10.3390/jcm12124170
Ha J-W, Ahn S-S, Song J-J, Park Y-B, Lee S-W. Total Globulin Fraction at Diagnosis Could Forecast All-Cause Mortality during the Disease Course in Patients with Antineutrophil Cytoplasmic Antibody-Associated Vasculitis. Journal of Clinical Medicine. 2023; 12(12):4170. https://doi.org/10.3390/jcm12124170
Chicago/Turabian StyleHa, Jang-Woo, Sung-Soo Ahn, Jason-Jungsik Song, Yong-Beom Park, and Sang-Won Lee. 2023. "Total Globulin Fraction at Diagnosis Could Forecast All-Cause Mortality during the Disease Course in Patients with Antineutrophil Cytoplasmic Antibody-Associated Vasculitis" Journal of Clinical Medicine 12, no. 12: 4170. https://doi.org/10.3390/jcm12124170
APA StyleHa, J.-W., Ahn, S.-S., Song, J.-J., Park, Y.-B., & Lee, S.-W. (2023). Total Globulin Fraction at Diagnosis Could Forecast All-Cause Mortality during the Disease Course in Patients with Antineutrophil Cytoplasmic Antibody-Associated Vasculitis. Journal of Clinical Medicine, 12(12), 4170. https://doi.org/10.3390/jcm12124170