
Correlation of Clinical Outcomes with the Prominent Indication of Transcatheter Paravalvular Leak Closure: A Multicenter Experience
 ,
,  , ,
, ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Endpoints and Definitions
2.3. Transcatheter PVL Closure Techniques
2.4. Device Selection
2.5. Statistical Analysis
3. Results
3.1. Patient and Procedural Characteristics
3.2. Outcome
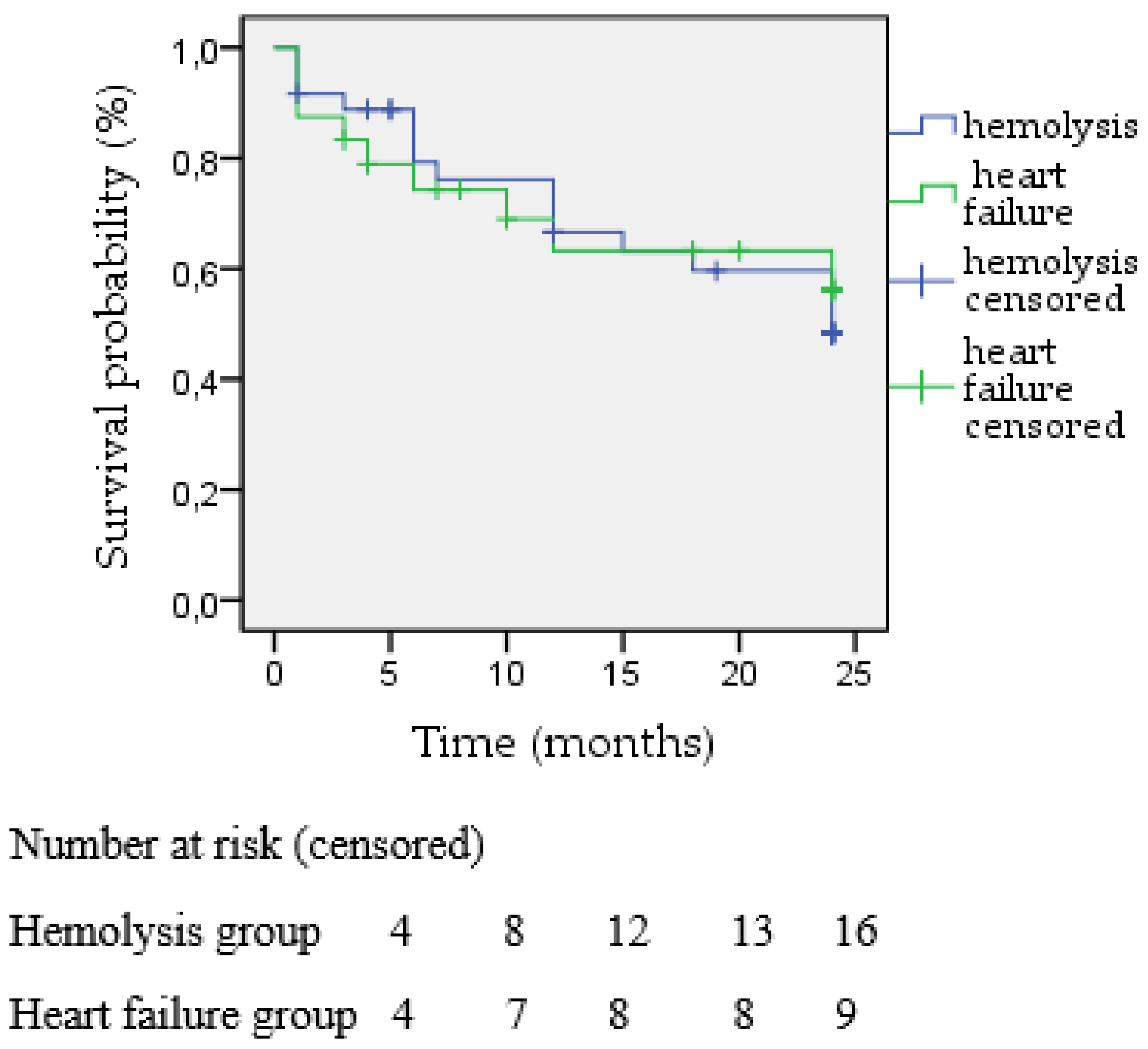
3.3. Survival
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Leon, M.B.; Smith, C.R.; Mack, M.J.; Makkar, R.R.; Svensson, L.G.; Kodali, S.K.; Thourani, V.H.; Tuzcu, E.M.; Miller, D.C.; Herrmann, H.C.; et al. Transcatheter or Surgical Aortic-Valve Replacement in Intermediate-Risk Patients. N. Engl. J. Med. 2016, 374, 1609–1620. [Google Scholar] [CrossRef]
- Ruiz, C.E.; Hahn, R.T.; Berrebi, A.; Borer, J.S.; Cutlip, D.E.; Fontana, G.; Gerosa, G.; Ibrahim, R.; Jelnin, V.; Jilaihawi, H.; et al. Clinical Trial Principles and Endpoint Definitions for Paravalvular Leaks in Surgical Prosthesis: An Expert Statement. J. Am. Coll. Cardiol. 2017, 69, 2067–2087. [Google Scholar] [CrossRef]
- Jilaihawi, H.; Kashif, M.; Fontana, G.; Furugen, A.; Shiota, T.; Friede, G.; Makhija, R.; Doctor, N.; Leon, M.B.; Makkar, R.R. Cross-Sectional Computed Tomographic Assessment Improves Accuracy of Aortic Annular Sizing for Transcatheter Aortic Valve Replacement and Reduces the Incidence of Paravalvular Aortic Regurgitation. J. Am. Coll. Cardiol. 2012, 59, 1275–1286. [Google Scholar] [CrossRef] [PubMed]
- Giblett, J.P.; Rana, B.S.; Shapiro, L.M.; Calvert, P.A. Percutaneous management of paravalvular leaks. Nat. Rev. Cardiol. 2019, 16, 275–285. [Google Scholar] [CrossRef]
- Baumgartner, H.; Falk, V.; Bax, J.J.; De Bonis, M.; Hamm, C.; Holm, P.J.; Iung, B.; Lancellotti, P.; Lansac, E.; Rodriguez Muñoz, D.; et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2017, 38, 2739–2791. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, R.A.; Otto, C.M.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., III; Fleisher, L.A.; Jneid, H.; Mack, M.J.; McLeod, C.J.; O’Gara, P.T.; et al. 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients with Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2017, 70, 252–289. [Google Scholar] [CrossRef]
- Joseph, T.A.; Lane, C.E.; Fender, E.A.; Zack, C.J.; Rihal, C.S. Catheter-based closure of aortic and mitral paravalvular leaks: Existing techniques and new frontiers. Expert Rev. Med. Devices 2018, 15, 653–663. [Google Scholar] [CrossRef]
- Alkhouli, M.; Sarraf, M.; Maor, E.; Sanon, S.; Cabalka, A.; Eleid, M.F.; Hagler, D.J.; Pollak, P.; Reeder, G.; Rihal, C.S. Techniques and Outcomes of Percutaneous Aortic Paravalvular Leak Closure. JACC Cardiovasc. Interv. 2016, 9, 2416–2426. [Google Scholar] [CrossRef] [PubMed]
- Zamorano, J.; Gonçalves, A.; Lancellotti, P.; Andersen, K.A.; González-Gómez, A.; Monaghan, M.; Brochet, E.; Wunderlich, N.; Gafoor, S.; Gillam, L.D.; et al. The use of imaging in new transcatheter interventions: An EACVI review paper. Eur. Hear. J. Cardiovasc. Imaging 2016, 17, 835–835af. [Google Scholar] [CrossRef]
- Vavuranakis, M.; Kalogeras, K.; Lozos, V.; Aznaouridis, K.; Aggeli, K.; Moldovan, C.; Kalantzis, C.; Siasos, G.; Koufakis, N.; Tousoulis, D. Transapical closure of multiple mitral paravalvular leaks with dual device deployment through a single sheath: A Heart Team job. Hell. J. Cardiol. 2018, 59, 367–369. [Google Scholar] [CrossRef]
- Goktekin, O.; Vatankulu, M.A.; Ozhan, H.; Ay, Y.; Ergelen, M.; Tasal, A.; Aydin, C.; Ismail, Z.; Ates, I.; Hijazi, Z. Early experience of percutaneous paravalvular leak closure using a novel Occlutech occluder. Eurointervention 2016, 11, 1195–1200. [Google Scholar] [CrossRef]
- Onorato, E.M.; Muratori, M.; Smolka, G.; Malczewska, M.; Zorinas, A.; Zakarkaite, D.; Mussayev, A.; Christos, C.P.; Bauer, F.; Gandet, T.; et al. Midterm procedural and clinical outcomes of percutaneous paravalvular leak closure with the Occlutech Paravalvular Leak Device. Eurointervention 2020, 15, 1251–1259. [Google Scholar] [CrossRef]
- Kalogeras, K.; Ntalekou, K.; Aggeli, K.; Moldovan, C.; Katsianos, E.; Kalantzis, C.; Bei, E.; Mourmouris, C.; Spargias, K.; Chrissoheris, M.; et al. Transcatheter closure of paravalvular leak: Multicenter experience and follow-up. Hell. J. Cardiol. 2021, 62, 416–422. [Google Scholar] [CrossRef]
- Hourihan, M.; Perry, S.B.; Mandell, V.S.; Keane, J.F.; Rome, J.J.; Bittl, J.; Lock, J.E. Transcatheter umbrella closure of valvular and paravalvular leaks. J. Am. Coll. Cardiol. 1992, 20, 1371–1377. [Google Scholar] [CrossRef]
- Alkhouli, M.; Rihal, C.S.; Zack, C.J.; Eleid, M.F.; Maor, E.; Sarraf, M.; Cabalka, A.K.; Reeder, G.S.; Hagler, D.J.; Maalouf, J.F.; et al. Transcatheter and Surgical Management of Mitral Paravalvular Leak: Long-Term Outcomes. JACC Cardiovasc. Interv. 2017, 10, 1946–1956. [Google Scholar] [CrossRef]
- Ruiz, C.E.; Jelnin, V.; Kronzon, I.; Dudiy, Y.; Del Valle-Fernandez, R.; Einhorn, B.N.; Chiam, P.T.; Martinez, C.; Eiros, R.; Roubin, G.; et al. Clinical Outcomes in Patients Undergoing Percutaneous Closure of Periprosthetic Paravalvular Leaks. J. Am. Coll. Cardiol. 2011, 58, 2210–2217. [Google Scholar] [CrossRef]
- Alkhouli, M.; Zack, C.J.; Sarraf, M.; Eleid, M.F.; Cabalka, A.K.; Reeder, G.S.; Hagler, D.J.; Maalouf, J.F.; Nkomo, V.T.; Rihal, C.S. Successful Percutaneous Mitral Paravalvular Leak Closure Is Associated with Improved Midterm Survival. Circ. Cardiovasc. Interv. 2017, 10, e005730. [Google Scholar] [CrossRef]
- Yang, C.; Liu, Y.; Tang, J.; Jin, P.; Li, L.; Yu, S.; Yang, J. Prognosis of Transcatheter Closure Compared with Surgical Repair of Paravalvular Leak after Prosthetic Valve Replacement: A Retrospective Comparison. Thorac. Cardiovasc. Surg. 2020, 68, 148–157. [Google Scholar] [CrossRef] [PubMed]
- García, E.; Arzamendi, D.; Jimenez-Quevedo, P.; Sarnago, F.; Martí, G.; Sanchez-Recalde, A.; Lasa-Larraya, G.; Sancho, M.; Iñiguez, A.; Goicolea, J.; et al. Outcomes and predictors of success and complications for paravalvular leak closure: An analysis of the SpanisH real-wOrld paravalvular LEaks closure (HOLE) registry. Eurointervention 2017, 12, 1962–1968. [Google Scholar] [CrossRef] [PubMed]
- Calvert, P.A.; Northridge, D.B.; Malik, I.S.; Shapiro, L.; Ludman, P.; Qureshi, S.A.; Mullen, M.; Henderson, R.; Turner, M.; Been, M.; et al. Percutaneous Device Closure of Paravalvular Leak: Combined Experience From the United Kingdom and Ireland. Circulation 2016, 134, 934–944. [Google Scholar] [CrossRef] [PubMed]
- Hascoët, S.; Smolka, G.; Blanchard, D.; Kloëckner, M.; Brochet, E.; Bouisset, F.; Leurent, G.; Thambo, J.-B.; Combes, N.; Dumonteil, N.; et al. Predictors of Clinical Success After Transcatheter Paravalvular Leak Closure: An International Prospective Multicenter Registry. Circ. Cardiovasc. Interv. 2022, 15, e012193. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 60) | Heart Failure (n = 24) | Hemolysis (n = 36) | p Value | |
|---|---|---|---|---|
| Demographics Age (years) | 69.5 ± 11 | 68.5 ± 11.8 | 70.22 ± 10.8 | 0.281 |
| Male (%) | 39 (65%) | 16 (66.7%) | 23 (63.9%) | |
| Female (%) | 21 (35%) | 8 (33.3%) | 13 (36.1%) | |
| Male versus female | 1.000 | |||
| Body mass index | 25.9 ± 2.9 | 26.6 ± 2.8 | 25.4 ± 2.9 | 0.285 |
| Cardiovascular risk factors/medical history | ||||
| Diabetes mellitus | 11 (18.3%) | 4 (16.7%) | 7 (19.4%) | 0.905 |
| Smoking | 10 (16.7%) | 6 (25%) | 4 (11.1%) | 0.254 |
| Chronic kidney disease | 21 (35%) | 5 (20.8%) | 16 (44.4%) | 0.011 |
| Previous permanent pacemaker | 14 (23.3%) | 5 (20.8%) | 9 (25%) | 0.431 |
| Previous coronary artery disease | 14 (23.3%) | 7 (29.2%) | 7 (19.4%) | 0.397 |
| Previous coronary artery bypass | 12 (20%) | 6 (25%) | 6 (16.7%) | 0.391 |
| Previous stroke | 4 (6.7%) | 2 (8.3%) | 2 (5.6%) | 0.801 |
| Pulmonary hypertension | 29 (48.3%) | 10 (41.7%) | 19 (52.8%) | 0.254 |
| Previous Endocarditis | 10 (16.7%) | 2 (8.3%) | 8 (22.2%) | 0.149 |
| Atrial fibrillation | 30 (50%) | 11 (45.8%) | 19 (67.9%) | 0.201 |
| Logistic EuroSCORE | 24.5 ± 13.5 | 21.02 ± 10.2 | 27.36 ± 15.3 | 0.391 |
| Mitral Valve (n = 41) | Aortic Valve (n = 19) | p Value | |
|---|---|---|---|
| Gender | |||
| Male | 21 (51.2%) | 17 (89.5%) | |
| Female | 20 (48.8%) | 2 (10.5%) | |
| Male versus female | 0.003 | ||
| Cardiovascular risk factors/medical history | |||
| Diabetes mellitus | 8 (19.5%) | 2 (10.5%) | 0.764 |
| Smoking | 8 (19.5%) | 2 (10.5%) | 0.363 |
| Chronic kidney disease | 18 (43.9%) | 3 (15.8%) | 0.016 |
| Previous permanent pacemaker | 12 (29.2%) | 2 (10.5%) | 0.159 |
| Previous coronary artery disease | 11 (26.8%) | 3 (15.8%) | 0.277 |
| Previous coronary artery bypass | 11 (26.8%) | 1 (5.3%) | 0.046 |
| Previous stroke | 2 (4.9%) | 2 (10.5%) | 0.421 |
| Pulmonary hypertension | 24 (58.5%) | 4 (21.1%) | 0.005 |
| Previous Endocarditis | 4 (9.8%) | 6 (31.6%) | 0.049 |
| Atrial fibrillation | 23 (56.1%) | 7 (36.8%) | 0.108 |
| Prominent indication for PVL closure | |||
| Hemolysis | 30 (73.2%) | 6 (31.6%) | 0.034 |
| Heart failure symptoms | 11 (26.8%) | 13 (68.4%) | 0.030 |
| Hemoglobin baseline | 9.7 ± 1.3 | 11.2 ± 1.9 | 0.006 |
| Risk scores | |||
| Logistic EuroSCORE | 26.8 ± 14.5 | 17.7 ± 8.7 | 0.024 |
| Total (n = 60) | Mitral Valve (n = 41) | Aortic Valve (n = 19) | ||
|---|---|---|---|---|
| Number of devices used | ||||
| One (1) | 38 (63.3%) | 27 (65.8%) | 12 (63.1%) | |
| Two (2) | 11 (18.3%) | 7 (17.1%) | 4 (21.1%) | |
| Three (3) | 4 (6.7%) | 3 (7.3%) | 1 (5.2%) | |
| None | 4 (6.7%) | 2 (4.8%) | 2 (10.5%) | |
| Type of device implanted | ||||
| Amplatzer vascular plug II | 9 | 5 | 4 | |
| Amplatzer vascular plug III | 53 | 37 | 16 | |
| Occlutech paravalvular leak device | 4 | 2 | 2 | |
| Amplatzer duct occluder | 7 | 7 | 0 | |
| Total number of devices | 73 | 51 | 22 | |
| Fluoroscopy time (minute) | 48 ± 25 | 46 ± 21 | 53 ± 35 | |
| Access site | ||||
| Transarterial retrograde | 30 | 15 | 15 | |
| Transeptal anterograde | 12 | 10 | 2 | |
| Transapical retrograde | 12 | 11 | 1 | |
| Transarterial and transeptal | 6 | 5 | 1 | |
| Valve type | ||||
| Bioprosthesis | 6 (14.6%) | 6 (31.6%) | ||
| Mechanical prosthesis | 35 (85.4%) | 13 (68.4%) | ||
| TAVI | 0 (0%) | 0 (0%) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lytra, T.; Kalogeras, K.; Pesiridis, T.; Moldovan, C.; Vavuranakis, M.A.; Vogiatzi, G.; Oikonomou, E.; Dardas, P.; Chrissoheris, M.; Ninios, V.; et al. Correlation of Clinical Outcomes with the Prominent Indication of Transcatheter Paravalvular Leak Closure: A Multicenter Experience. J. Clin. Med. 2023, 12, 4047. https://doi.org/10.3390/jcm12124047
Lytra T, Kalogeras K, Pesiridis T, Moldovan C, Vavuranakis MA, Vogiatzi G, Oikonomou E, Dardas P, Chrissoheris M, Ninios V, et al. Correlation of Clinical Outcomes with the Prominent Indication of Transcatheter Paravalvular Leak Closure: A Multicenter Experience. Journal of Clinical Medicine. 2023; 12(12):4047. https://doi.org/10.3390/jcm12124047
Chicago/Turabian StyleLytra, Thekla, Konstantinos Kalogeras, Theodoros Pesiridis, Carmen Moldovan, Michael Andrew Vavuranakis, Georgia Vogiatzi, Evaggelos Oikonomou, Petros Dardas, Michail Chrissoheris, Vlasis Ninios, and et al. 2023. "Correlation of Clinical Outcomes with the Prominent Indication of Transcatheter Paravalvular Leak Closure: A Multicenter Experience" Journal of Clinical Medicine 12, no. 12: 4047. https://doi.org/10.3390/jcm12124047
APA StyleLytra, T., Kalogeras, K., Pesiridis, T., Moldovan, C., Vavuranakis, M. A., Vogiatzi, G., Oikonomou, E., Dardas, P., Chrissoheris, M., Ninios, V., & Vavuranakis, M. (2023). Correlation of Clinical Outcomes with the Prominent Indication of Transcatheter Paravalvular Leak Closure: A Multicenter Experience. Journal of Clinical Medicine, 12(12), 4047. https://doi.org/10.3390/jcm12124047