
Association between HbA1c Levels and Fetal Macrosomia and Large for Gestational Age Babies in Women with Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis of 17,711 Women

 , , ,
, , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Search Strategy and Selection Criteria
- Any study design addressing the research question,
- Including women with GDM diagnoses at any point in pregnancy (singleton pregnancy),
- Including women who received HbA1c during their pregnancy and reported the time of testing,
- Reported on fetal macrosomia or birth weight,
- If birth weight is reported as a dichotomous outcome (primary or secondary), a threshold of 4 kg was used to define fetal macrosomia.
- Women with type 1 or type 2 diabetes,
- GDM being diagnosed on OGTT only with no HbA1c,
- Large for gestational age reported with no clear definition of fetal macrosomia or birth weight thresholds,
- Studies with no primary data and/or case report and case series,
- Studies in animals.
2.2. Outcome Measures
2.3. Data Collection
2.4. Data Analysis
2.5. Assessment of the Risk of Bias
3. Results
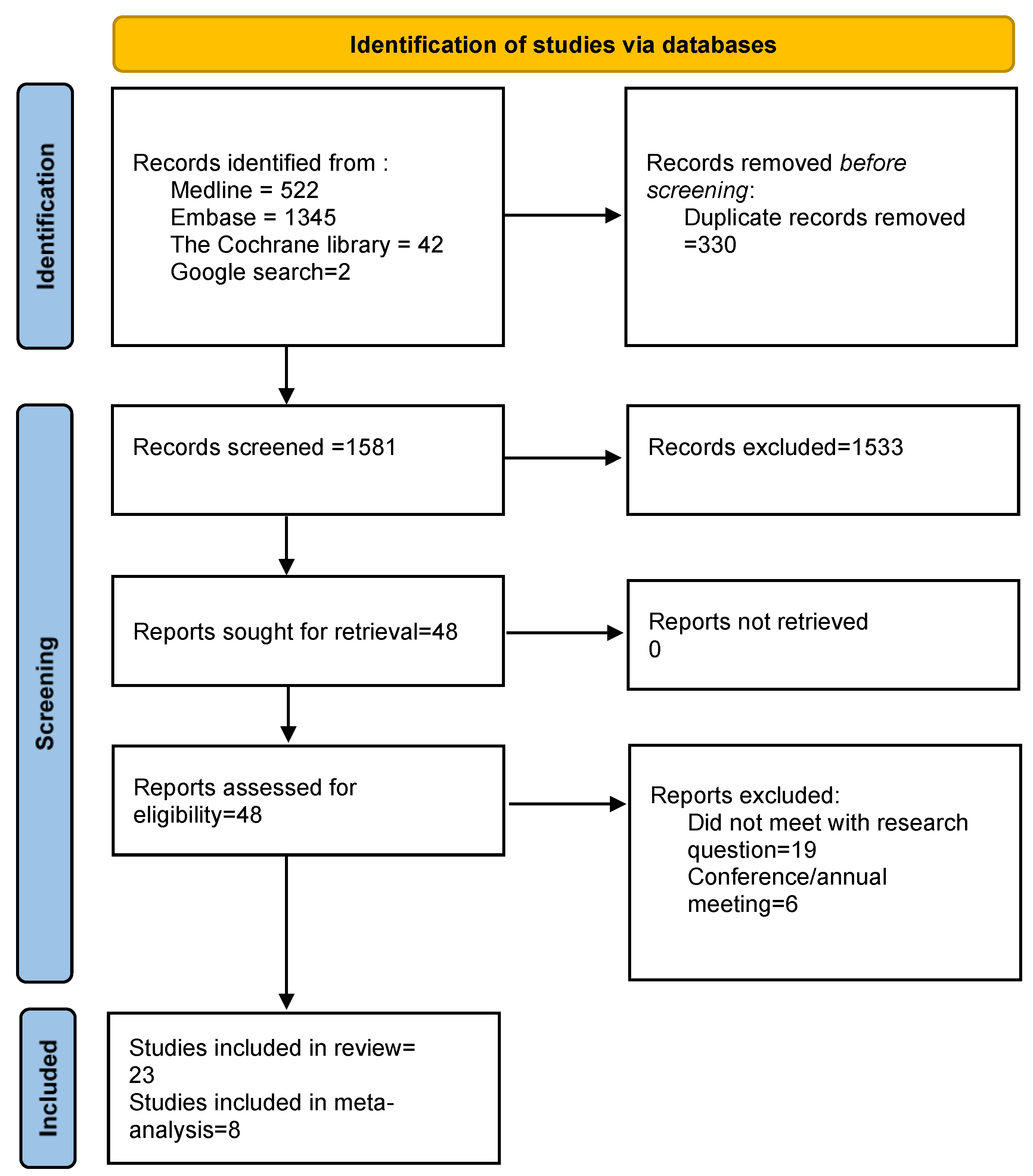
3.1. Search Results and Characteristics of Included Studies
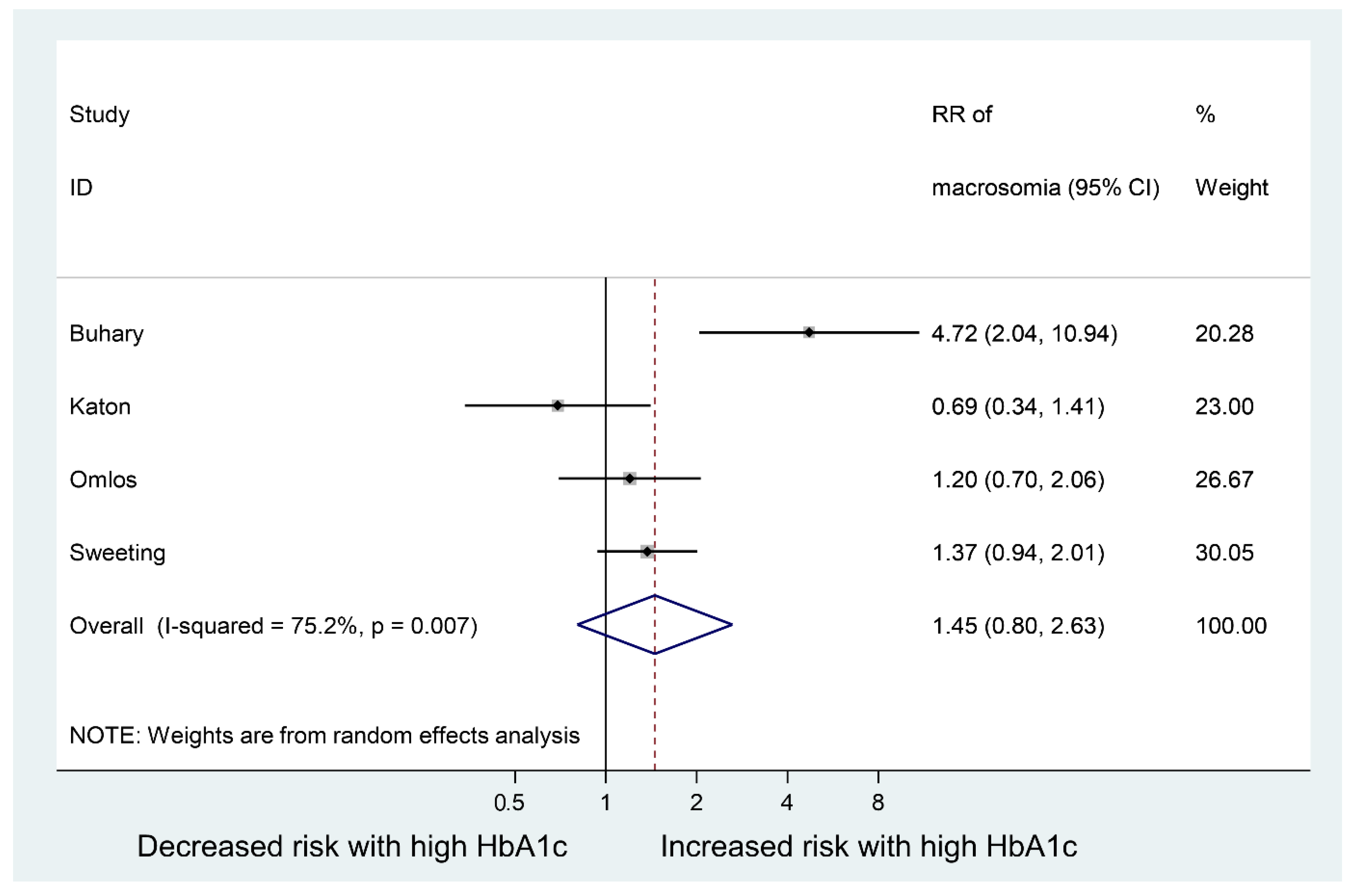
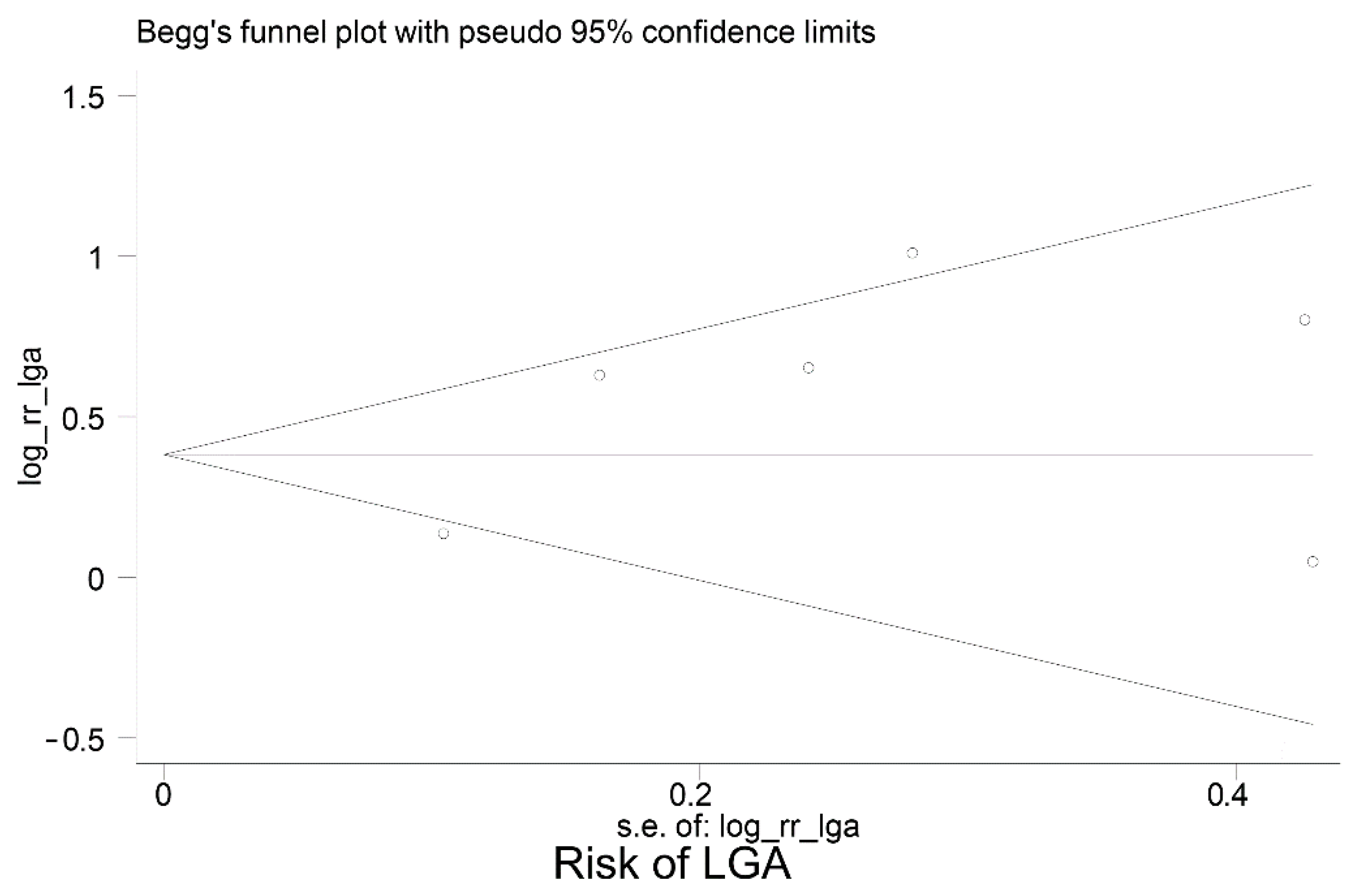
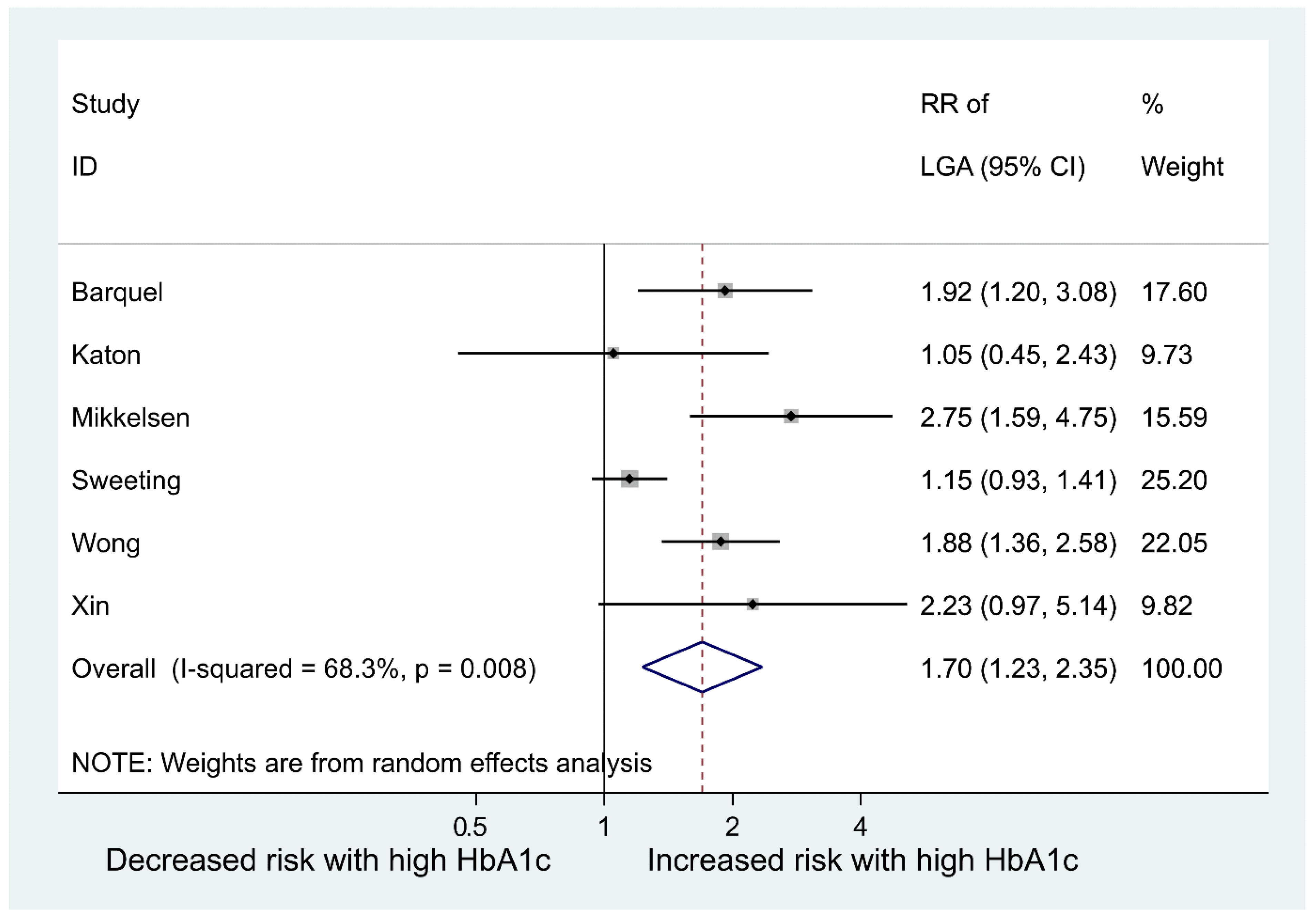
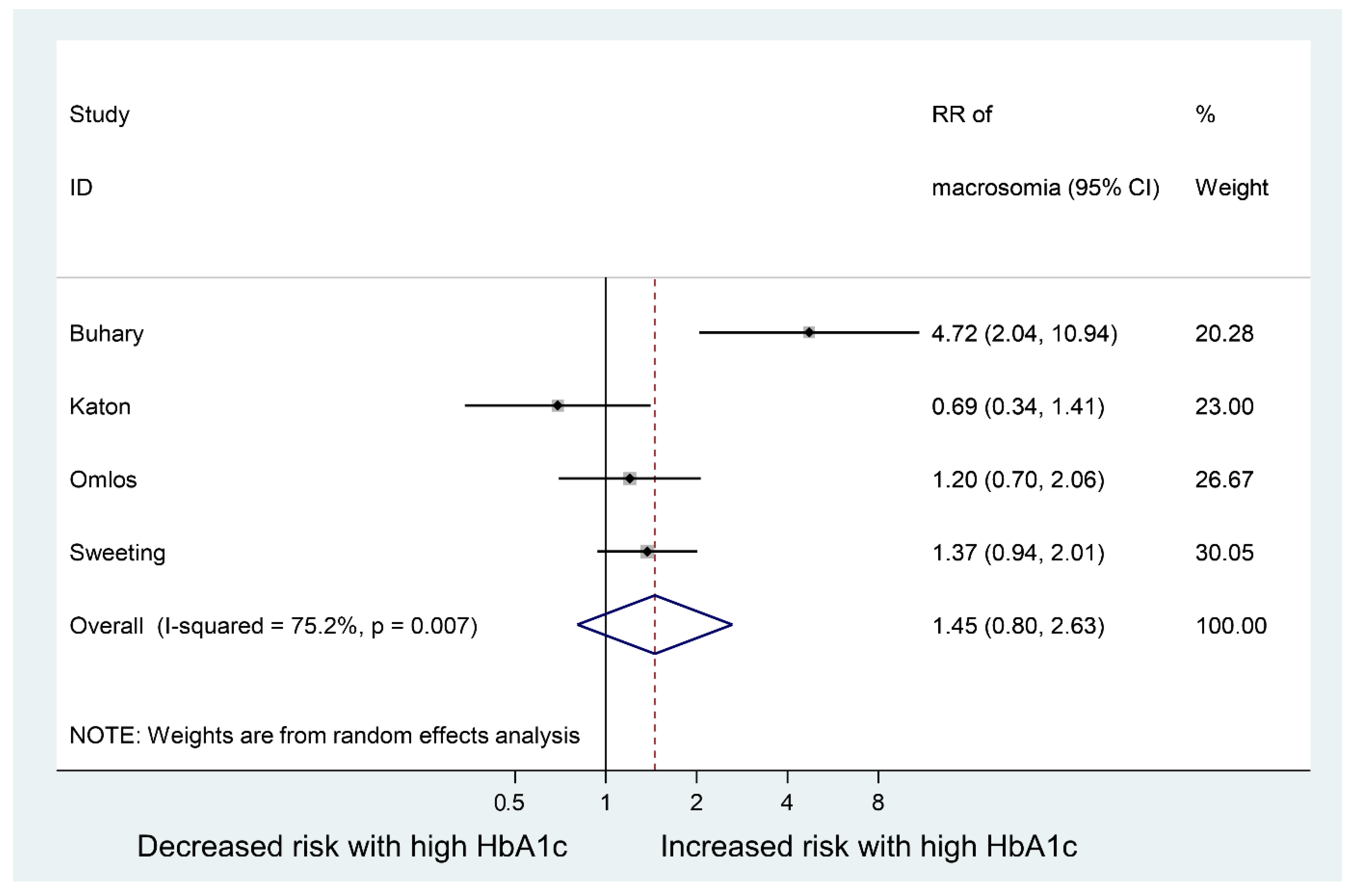
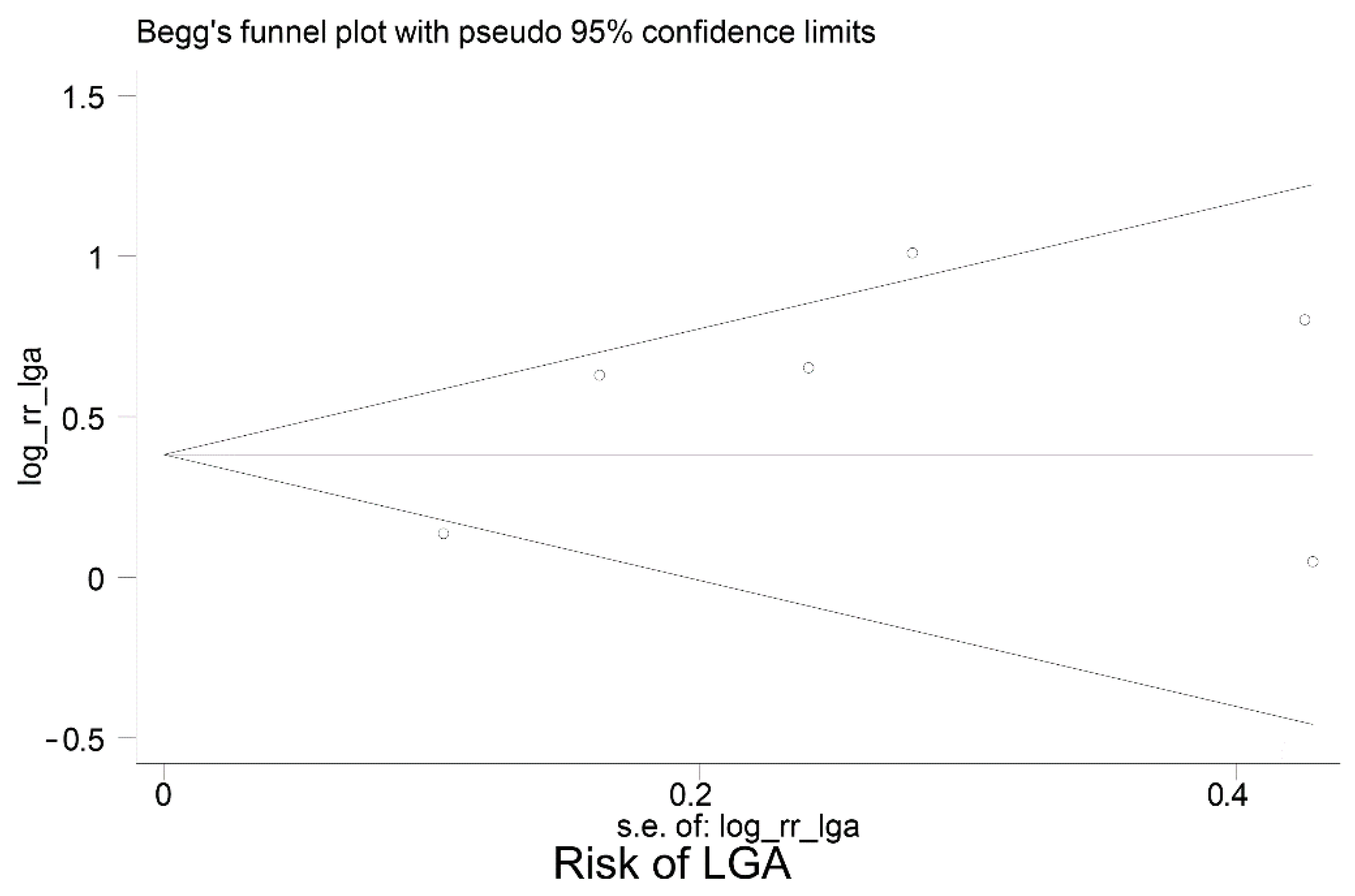
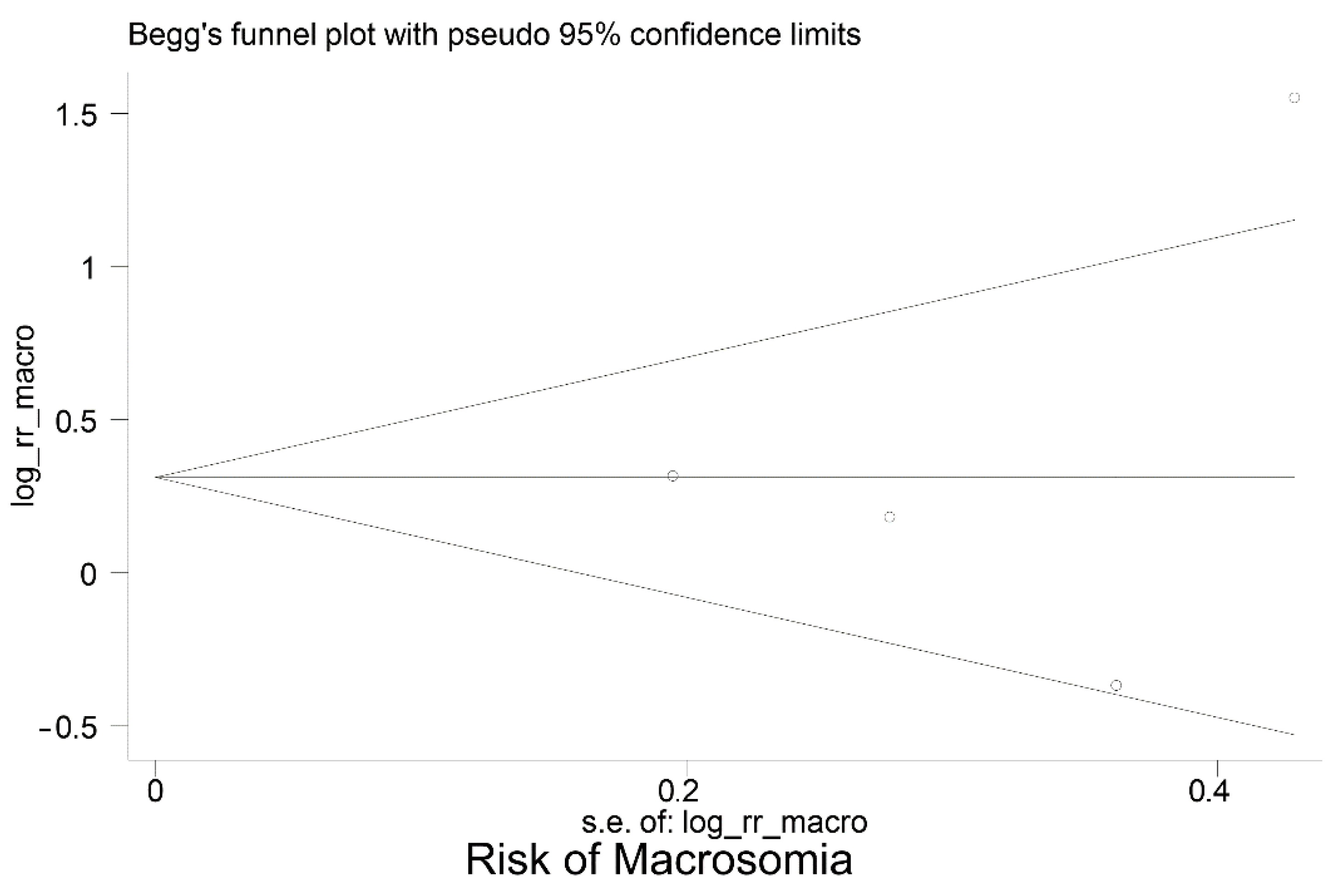
3.2. Meta-Analysis
3.3. Study Quality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferrara, A. Increasing prevalence of gestational diabetes mellitus: A public health perspective. Diabetes Care 2007, 30, S141–S146. [Google Scholar] [CrossRef] [Green Version]
- Guariguata, L.; Linnenkamp, U.; Beagley, J.; Whiting, D.R.; Cho, N.H. Global estimates of the prevalence of hyperglycaemia in pregnancy. Diabetes Res. Clin. Pract. 2014, 103, 176–185. [Google Scholar] [CrossRef]
- Svare, J.A.; Hansen, B.B.; M⊘lsted-Pedersen, L. Perinatal complications in women with gestational diabetes mellitus. Acta Obstet. Et Gynecol. Scand. 2001, 80, 899. [Google Scholar] [CrossRef]
- Kc, K.; Shakya, S.; Zhang, H. Gestational diabetes mellitus and macrosomia: A literature review. Ann. Nutr. Metab. 2015, 66, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Beta, J.; Khan, N.; Khalil, A.; Fiolna, M.; Ramadan, G.; Akolekar, R. Maternal and neonatal complications of fetal macrosomia: A systematic review and meta-analysis. Ultrasound Obstet. Gynecol. 2019, 54, 308–318. [Google Scholar] [CrossRef] [Green Version]
- Munda, A.; Starcic Erjavec, M.; Molan, K.; Ambrozic Avgustin, J.; Zgur-Bertok, D.; Pongrac Barlovic, D. Association between pre-pregnancy body weight and dietary pattern with large-for-gestational-age infants in gestational diabetes. Diabetol. Metab. Syndr. 2019, 11, 68. [Google Scholar] [CrossRef] [Green Version]
- Koning, S.H.; Hoogenberg, K.; Scheuneman, K.A.; Baas, M.G.; Korteweg, F.J.; Sollie, K.M.; Schering, B.J.; van Loon, A.J.; Wolffenbuttel, B.H.R.; van den Berg, P.P.; et al. Neonatal and obstetric outcomes in diet- and insulin-treated women with gestational diabetes mellitus: A retrospective study. BMC Endocr. Disord. 2016, 16, 52. [Google Scholar] [CrossRef] [Green Version]
- Reader, D.; Splett, P.; Gunderson, E.P.; Diabetes, C.; Education Dietetic Practice, G. Impact of gestational diabetes mellitus nutrition practice guidelines implemented by registered dietitians on pregnancy outcomes. J. Am. Diet. Assoc. 2006, 106, 1426–1433. [Google Scholar] [CrossRef]
- Hunt, K.J.; Schuller, K.L. The increasing prevalence of diabetes in pregnancy. Obs. Gynecol. Clin. North Am. 2007, 34, 173-vii. [Google Scholar] [CrossRef] [Green Version]
- Glucose Tolerance Tests: What Exactly do They Involve? Available online: https://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0072515/ (accessed on 16 January 2018).
- Sherwin, S.R. Limitations of the oral glucose tolerance test in diagnosis of early diabetes. Prim. Care Clin. Off. Pract. 1977, 4, 255–266. [Google Scholar] [CrossRef]
- Farah, N.; McGoldrick, A.; Fattah, C.; O'Connor, N.; Kennelly, M.M.; Turner, M.J. Body Mass Index (BMI) and Glucose Intolerance during Pregnancy in White European Women. J. Reprod. Infertil. 2012, 13, 95–99. [Google Scholar]
- Kwon, S.S.; Kwon, J.Y.; Park, Y.W.; Kim, Y.H.; Lim, J.B. HbA1c for diagnosis and prognosis of gestational diabetes mellitus. Diabetes Res. Clin. Pract. 2015, 110, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Brooke, B.S.; Schwartz, T.A.; Pawlik, T.M. MOOSE Reporting Guidelines for Meta-analyses of Observational Studies. JAMA Surg. 2021, 156, 787–788. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Quality Assesment Tool for Observational Chorot and Cross-Sectional Studies. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 25 July 2021).
- Barquel, B.; Herranz, L.; Hillman, N.; Burgos, M.A.; Grande, C.; Tukia, K.M.; Bartha, J.L.; Pallardo, L.F. HbA1c and gestational weight gain are factors that influence neonatal outcome in mothers with gestational diabetes. J. Women's Health 2016, 25, 579–585. [Google Scholar] [CrossRef]
- Olmos, P.R.; Borzone, G.R.; Olmos, R.I.; Valencia, C.N.; Bravo, F.A.; Hodgson, M.I.; Belmar, C.G.; Poblete, J.A.; Escalona, M.O.; Gomez, B. Gestational diabetes and pre-pregnancy overweight: Possible factors involved in newborn macrosomia. J. Obstet. Gynaecol. Res. 2012, 38, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Sweeting, A.N.; Ross, G.P.; Hyett, J.; Wong, J. Gestational diabetes in the first trimester: Is early testing justified? Lancet Diabetes Endocrinol. 2017, 5, 571–573. [Google Scholar] [CrossRef]
- Wong, V.W.; Chong, S.; Mediratta, S.; Jalaludin, B. Measuring glycated haemoglobin in women with gestational diabetes mellitus: How useful is it? Aust. N. Z. J. Obstet. Gynaecol. 2017, 57, 260–265. [Google Scholar] [CrossRef] [PubMed]
- Katon, J.; Reiber, G.; Williams, M.A.; Yanez, D.; Miller, E. Antenatal haemoglobin A1c and risk of large-for-gestational-age infants in a multi-ethnic cohort of women with gestational diabetes. Paediatr. Perinat. Epidemiol. 2012, 26, 208–217. [Google Scholar] [CrossRef]
- Xin, S.; Pravin, R.; Rajadurai, V.; Chandran, S. Elevated glycated hemoglobin during pregnancy in diabetic women as a predictor of large-for-gestational age infants in an Asian cohort. J. Clin. Neonatol. 2018, 7, 136–140. [Google Scholar] [CrossRef]
- Mikkelsen, M.R.; Nielsen, S.B.; Stage, E.; Mathiesen, E.R.; Damm, P. High maternal HbA1c is associated with overweight in neonates. Dan. Med. Bull. 2011, 58, A4309. [Google Scholar]
- Hu, J.; Ge, Z.; Xu, Q.; Shen, S.; Wang, Y.; Zhu, D.; Bi, Y. Influence of fetal sex on perinatal outcomes in women with gestational diabetes mellitus. Diabetes Metab. Res. Rev. 2020, 36, e3245. [Google Scholar] [CrossRef]
- Liu, B.; Cai, J.; Xu, Y.; Long, Y.; Deng, L.; Lin, S.; Zhang, J.; Yang, J.; Zhong, L.; Luo, Y.; et al. Early Diagnosed Gestational Diabetes Mellitus Is Associated with Adverse Pregnancy Outcomes: A Prospective Cohort Study. J. Clin. Endocrinol. Metab. 2020, 105, e4264–e4274. [Google Scholar] [CrossRef]
- Xu, Q.; Ge, Z.; Hu, J.; Shen, S.; Bi, Y.; Zhu, D. The association of gestational weight gain and adverse pregnancy outcomes in women with gestational diabetes mellitus. Endocr. Pract. 2019, 25, 1137–1150. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Zhang, Y.; Gu, Z.; Li, Y. Effects of effective blood glucose control on pregnancy outcomes and neonatal complications in pregnant women with gestational diabetes. Int. J. Clin. Exp. Med. 2019, 12, 4387–4391. [Google Scholar]
- Dalfra, M.G.; Ragazzi, E.; Masin, M.; Bonsembiante, B.; Cosma, C.; Barison, A.; Toniato, R.; Fedele, D.; Lapolla, A. Pregnancy outcome in immigrant women with gestational diabetes mellitus. Gynecol. Endocrinol. 2011, 27, 379–383. [Google Scholar] [CrossRef]
- Pintaudi, B.; Fresa, R.; Dalfra, M.; Dodesini, A.; Vitacolonna, E.; Tumminia, A.; Lencioni, C.; Marcone, T.; Bonomo, M.; Napoli, A. The risk stratification of adverse neonatal outcomes in women with gestational diabetes (strong) study: A preliminary report. Diabetes 2017, 66, A396. [Google Scholar] [CrossRef]
- Capula, C.; Mazza, T.; Vero, R.; Costante, G. HbA1c levels in patients with gestational diabetes mellitus: Relationship with pre-pregnancy BMI and pregnancy outcome. J. Endocrinol. Investig. 2013, 36, 1038–1045. [Google Scholar] [CrossRef]
- Alfadhil, E.M.; Osman, E.N.; Basri, T.H.; Mansuri, N.S.; Youssef, M.H.; Assaaedi, S.A.; Aljohani, B.A. Gestational diabetes among Saudi women: Prevalence, risk factors and pregnancy outcomes. Ann. Saudi Med. 2015, 35, 222–230. [Google Scholar] [CrossRef]
- Buhary, B.M.; Almohareb, O.; Aljohani, N.; Alzahrani, S.H.; Elkaissi, S.; Sherbeeni, S.; Almaghamsi, A.; Almalki, M. Glycemic control and pregnancy outcomes in patients with diabetes in pregnancy: A retrospective study. Indian J. Endocrinol. Metab. 2016, 20, 481–490. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Quintero, V.H.; Istwan, N.B.; Rhea, D.J.; Rodriguez, L.I.; Cotter, A.; Carter, J.; Mueller, A.; Stanziano, G.J. The impact of glycemic control on neonatal outcome in singleton pregnancies complicated by gestational diabetes. Diabetes Care 2007, 30, 467–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mane, L.; Flores-Le Roux, J.A.; Benaiges, D.; Rodriguez, M.; Marcelo, I.; Chillaron, J.J.; Pedro-Botet, J.; Llaurado, G.; Gortazar, L.; Carreras, R.; et al. Role of first-trimester HbA1c as a predictor of adverse obstetric outcomes in a multiethnic cohort. J. Clin. Endocrinol. Metab. 2017, 102, 390–397. [Google Scholar] [CrossRef]
- Braga, F.O.; Negrato, C.A.; da Matta, M.F.B.; Carneiro, J.R.I.; Gomes, M.B. Relationship between inflammatory markers, glycated hemoglobin and placental weight on fetal outcomes in women with gestational diabetes. Arch. Endocrinol. Metab. 2019, 63, 22–29. [Google Scholar] [CrossRef] [Green Version]
- Kansu Çelik, H.; Seval Ozgu-Erdinc, A.; Kisa Karakaya, B.; Eldem, S.; Hançerlioğulları, N.; Engin-Ustun, Y.; Kansu-Celik, H.; Ozgu-Erdinc, A.S.; Kisa, B.; Hancerliogullari, N. Maternal serum glycosylated hemoglobin and fasting plasma glucose predicts gestational diabetes at the first trimester in Turkish women with a low-risk pregnancy and its relationship with fetal birth weight; a retrospective cohort study. J. Matern. Fetal Neonatal Med. 2019, 32, 1–211. [Google Scholar] [CrossRef] [PubMed]
- Vereş, M.; Crəiuţ, D.I.; Trutz, J.; Babeş, A. The utility of glycated hemoglobin, determined in the second trimester of pregnancy, in diagnosing gestational diabetes. Rom. J. Diabetes Nutr. Metab. Dis. 2015, 22, 233–240. [Google Scholar] [CrossRef] [Green Version]
- Antoniou, M.C.; Gilbert, L.; Gross, J.; Rossel, J.B.; Fumeaux, C.J.F.; Vial, Y.; Puder, J.J. Main fetal predictors of adverse neonatal outcomes in pregnancies with gestational diabetes mellitus. J. Clin. Med. 2020, 9, 2409. [Google Scholar] [CrossRef]
- Krstevska, B.; Mishevska, S.; Janevska, E.; Simeonova, S.; Livrinova, V.; Pemovska, G.; Velkoska Nakova, V.; Serafimoski, V. Gestational Diabetes Mellitus—the impact of maternal body mass index and glycaemic control on baby's birth weight. Prilozi 2009, 30, 115–124. [Google Scholar]
- Homko, C.J.; Deeb, L.C.; Rohrbacher, K.; Mulla, W.; Mastrogiannis, D.; Gaughan, J.; Santamore, W.P.; Bove, A.A.; Homko, C.J.; Deeb, L.C.; et al. Impact of a telemedicine system with automated reminders on outcomes in women with gestational diabetes mellitus. Diabetes Technol. Ther. 2012, 14, 624–629. [Google Scholar] [CrossRef] [Green Version]
- Huang, N.; Chen, S.; Zhou, Y.; Xing, W.; Wang, K.; Zhong, J.; Li, L. Efficacy and safety of telemedicine for blood glucose and pregnancy outcomes in gestational diabetes mellitus: A systematic review. Chin. J. Evid. Based Med. 2019, 19, 960–967. [Google Scholar] [CrossRef]
- Calle-Pascual, A.L.; Perez-Ferre, N.; Galindo, M.; Fernandez, M.D.; Velasco, V.; Runkle, I.; De La Cruz, M.J.; Martin Rojas-Marcos, P.; Del Valle, L. The outcomes of gestational diabetes mellitus after a telecare approach are not inferior to traditional outpatient clinic visits. Int. J. Endocrinol. 2010, 2010, 386941. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Country | Total GDM | Macrosomia | LGA | Mean HBA1C | DX Criteria | Duration | Mean Age | BMI |
|---|---|---|---|---|---|---|---|---|---|---|
| Alfadhil [31] | 2015 | Saudi Arabia | 292 | 10 | - | 5.77 (±0.82) | IADPSG | 2011–2014 | 32.69 (±6.08) | 32.30 (±6.66) |
| Antoniou [38] | 2020 | Switzerland | 740 | 45 | 95 | 5.50 (±0.4) | IADPSG | 2012–2017 | 32.80 (±5.5) | 26.10 (±5.4) |
| Barquel [17] | 2016 | Spain | 2037 | - | 126 | 5.20 (±0.4) | NDDG | 1987–2008 | 33.00 (±4.0) | 24.70 (±4.7) |
| Braga [35] | 2019 | Brazil | 78 | 9 | - | 5.68 | Carpenter & Coustan | 2004–2005 | 31.00 | 27.80 |
| Buhary [32] | 2016 | Saudi Arabia | 177 | 31 | - | 6.58 | WHO | 2012–2013 | 31.88 | 31.31 |
| Capula [30] | 2013 | Italy | 148 | 3 | 10 | 5.28 (±0.29) | Two step procedure IWCGDM | 2009–2010 | 33.4 (±4.8) | 26.40 (±5.2) |
| Dalfra [28] | 2011 | Italy | 1300 | - | 269 | 5.20 | Carpenter & Coustan | 2001–2007 | 33.48 | 24.90 |
| Gonzalez-quintero [33] | 2007 | Miami, USA | 3218 | 376 | 462 | 5.10–5.50 | - | 2001–2005 | 31.11 | 29.47 |
| Hu [24] | 2020 | China | 1155 | 108 | 112 | 5.36 | ADP | 2012–2017 | 31.30 | 22.62 |
| Kansu-celik [36] | 2019 | Turkey | 69 | 12 | 5.31 (±0.58) | Carpenter & Coustan | 2010–2018 | 31.11 (±6.93) | 27.43 (±5.49) | |
| Katon [21] | 2012 | USA | 502 | 210 | 210 | 5.70 | - | 2000–2010 | 31.00 (±5.4) | 25.00 |
| Krstevska [39] | 2009 | North Macedonia | 180 | 37 | - | 6.23 (±1.2) | ADA | 2006–2009 | 31.29 | 28.20 (±6.2) |
| Liu [25] | 2020 | China | 81 | 3 | - | 4.98 | WHO 13 | - | 31.95 | 22.02 |
| Mane [34] | 2017 | Spain | 22 | 3 | 4 | 5.90 | ADA | 2013–2015 | 33.81 (±4.87) | 30.41 (±5.46) |
| Mikkelsen [23] | 2011 | Denmark | 148 | - | 38 | 5.37 | 2-h 75 g OGTT | 2007 | 32.57 | 28.86 |
| Olmos [18] | 2012 | Chile | 251 | 21 | 44 | 5.56 | WHO | 1998–2009 | 32.75 | 26.31 |
| Pintaudi [29] | 2018 | Italy | 2736 | 132 | 163 | 5.10 (±0.8) | Italian recommendation | 2012–2015 | 36.60 (±5.10) | 24.80 |
| Sweeting [19] | 2017 | Australia | 1805 | 161 | 411 | 5.30 (±0.5) | ADP | 1991–2011 | 33.20 (±5.0) | 24.00 (±5.1) |
| Veres [37] | 2015 | Romania | 26 | 6 | - | 6.50 | Carpenter & Coustan | 2009–2011 | 31.31 (±4.47) | 27.84 (±4.45) |
| Wong [20] | 2017 | Australia | 1244 | - | 142 | 5.40 (±0.4) | ADIPS | 2010–2014 | 31.60 (±5.2) | 27.50 (6.9) |
| Xin [22] | 2018 | Singapore | 202 | - | 21 | 5.99 | WHO-2011 | 2012–2013 | 33.07 (±4.6) | - |
| Xu [26] | 2019 | China | 1200 | 142 | 260 | 5.40 (±0.62) | IADPSG | 2016–2017 | 30.90 (±4.2) | 23.50 (±3.4) |
| Zhao [27] | 2019 | China | 100 | 8 | - | 6.10–6.30 | 75 g OGTT | 2014–2017 | 31.90 | 26.40 |
| Study, Year | Source of Funding | Type of Study |
|---|---|---|
| Alfadhil 2015 [31] | Supported by grant from King Abdulaziz City for Science and Technology, Riyadh, Saudi Arabia. | Prospective descriptive study |
| Antoniou 2020 [38] | This study was sponsored by an unrestricted educational grant from NovoNordisk. | Prospective study |
| Barquel 2016 [17] | None | Observational study |
| Braga 2019 [35] | Supported by “Fundação do Amparo à Pesquisa do Estado do Rio de Janeiro” (Faperj) | Prospective, longitudinal and observational study |
| Buhary 2016 [32] | None | Retrospective study |
| Capula 2013 [30] | Not mentioned | Observational study |
| Dalfra 2011 [28] | Not mentioned | Observational study |
| Gonzalez-quintero 2007 [33] | Not mentioned | Retrospective cohort study |
| Hu 2020 [24] | Supported by the National Natural Science Foundation of China under by Foundation for Innovative Research Groups of the National Natural Science Foundation of China; the National Key Research and Development Program of China; the Project of National Key Clinical Division of China, the Medical Scientific Research Foundation of Jiangsu Province of China; the Key Research and Development Program of Jiangsu Province of China; the Key Provincial Talents Program of Jiangsu Province of China; the Six talent peaks project of Jiangsu Province of China | Retrospective cohort study |
| Kansu-Celik 2019 [36] | Not mentioned | Retrospective cohort |
| Katon 2012 [21] | Funded by the University of Washington Department of Epidemiology. | Observational study |
| Krstevska 2009 [39] | Nothing mentioned | Observational study |
| Liu 2020 [25] | This study was funded by Sun Yat-Sen University Clinical Research 5010 Program and National Natural Science Foundation of China | Cohort study |
| Mane 2017 [34] | Received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. | Prospective cohort study |
| Mikkelsen 2011 [23] | Not mentioned | Cohort study |
| Olmos 2012 [18] | Not mentioned | Observational study |
| Pintaudi 2017 [29] | Not mentioned | Observational, retrospective, multicentre study |
| Sweeting 2017 [19] | Not mentioned | Retrospective cohort |
| Veres 2015 [37] | Not mentioned | Prospective cohort |
| Wong 2017 [20] | None | Retrospective review |
| Xin 2018 [22] | None | Retrospective study |
| Xu 2019 [26] | Supported by grants from the National Natural Science Foundation of China Grant Award, National Key Research and Development Program of China, the Project of National Key Clinical Division of China, and the Medical Scientific Research Foundation of Jiangsu Province of China. | Retrospective Cchort study |
| Zhao 2019 [27] | Not mentioned | Observational study |
| Author | Year | Total GDM | Number of LGA for Low HbA1c | Number of LGA for High HbA1c | Number of Low HbA1c | Number of High HbA1c | Cut-off HbA1c Value | Number of Macro Low HbA1c | Number of Macro High HbA1c |
|---|---|---|---|---|---|---|---|---|---|
| Barquel [17] | 2016 | 2037 | 20 | 95 | 526 | 1301 | 5 | - | - |
| Xin [22] | 2018 | 202 | 14 | 7 | 165 | 37 | 6.5 | - | - |
| Sweeting [19] | 2017 | 2254 | 89 | 410 | 449 | 1805 | 5 | 29 | 160 |
| Wong [20] | 2017 | 1244 | 55 | 87 | 675 | 569 | 5.4 | - | - |
| Buhary [32] | 2019 | 177 | - | - | 94 | 83 | 6.5 | 6 | 25 |
| Olmos [18] | 2012 | 251 | - | - | 202 | 49 | 6 | 30 | 14 |
| Mikkelsen [23] | 2011 | 148 | 18 | 20 | 97 | 51 | 5.6 | - | 3 |
| Katon [21] | 2012 | 502 | 8 | 14 | 292 | 210 | 5.7 | 13 | 15 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mou, S.S.; Gillies, C.; Hu, J.; Danielli, M.; Al Wattar, B.H.; Khunti, K.; Tan, B.K. Association between HbA1c Levels and Fetal Macrosomia and Large for Gestational Age Babies in Women with Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis of 17,711 Women. J. Clin. Med. 2023, 12, 3852. https://doi.org/10.3390/jcm12113852
Mou SS, Gillies C, Hu J, Danielli M, Al Wattar BH, Khunti K, Tan BK. Association between HbA1c Levels and Fetal Macrosomia and Large for Gestational Age Babies in Women with Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis of 17,711 Women. Journal of Clinical Medicine. 2023; 12(11):3852. https://doi.org/10.3390/jcm12113852
Chicago/Turabian StyleMou, Sudipta Sarker, Clare Gillies, Jiamiao Hu, Marianna Danielli, Bassel Hamameeh Al Wattar, Kamlesh Khunti, and Bee Kang Tan. 2023. "Association between HbA1c Levels and Fetal Macrosomia and Large for Gestational Age Babies in Women with Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis of 17,711 Women" Journal of Clinical Medicine 12, no. 11: 3852. https://doi.org/10.3390/jcm12113852
APA StyleMou, S. S., Gillies, C., Hu, J., Danielli, M., Al Wattar, B. H., Khunti, K., & Tan, B. K. (2023). Association between HbA1c Levels and Fetal Macrosomia and Large for Gestational Age Babies in Women with Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis of 17,711 Women. Journal of Clinical Medicine, 12(11), 3852. https://doi.org/10.3390/jcm12113852