
Characteristics of Chemosensory Perception in Long COVID and COVID Reinfection


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Statistical Analysis
3. Results
3.1. Participant Characteristics
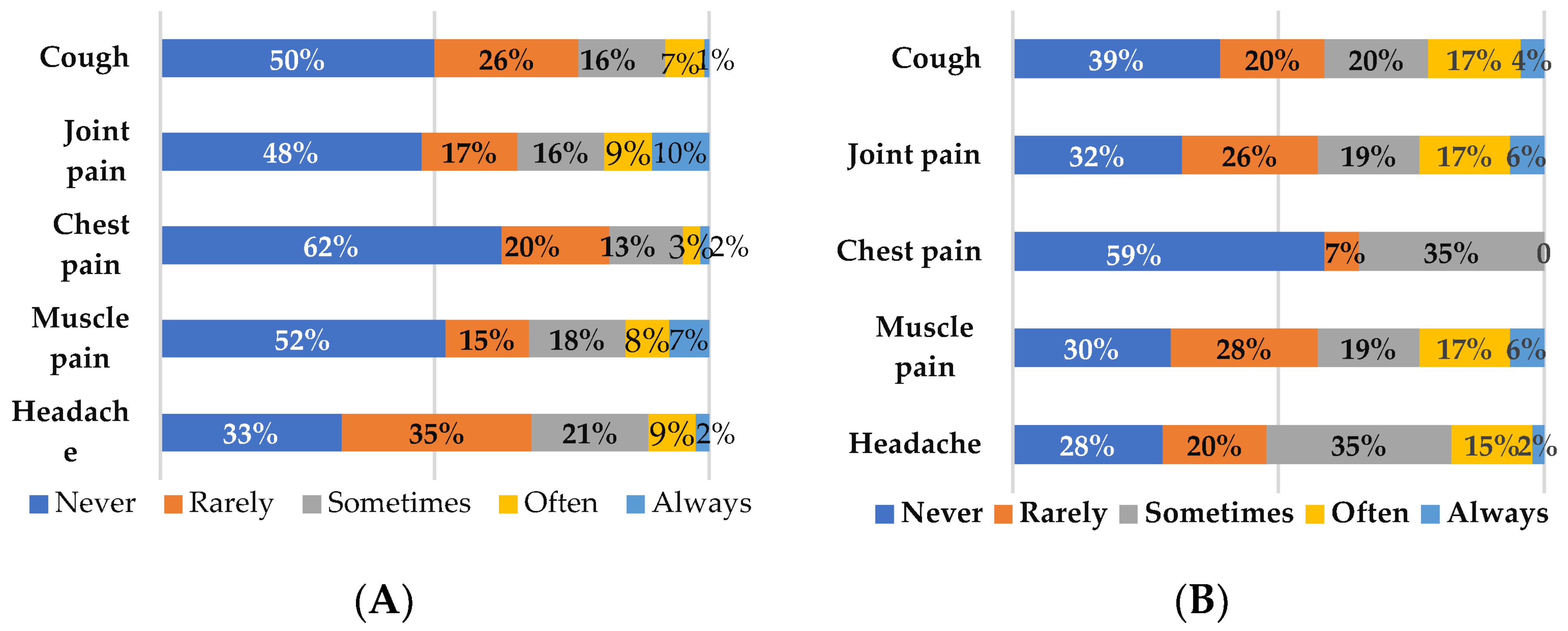
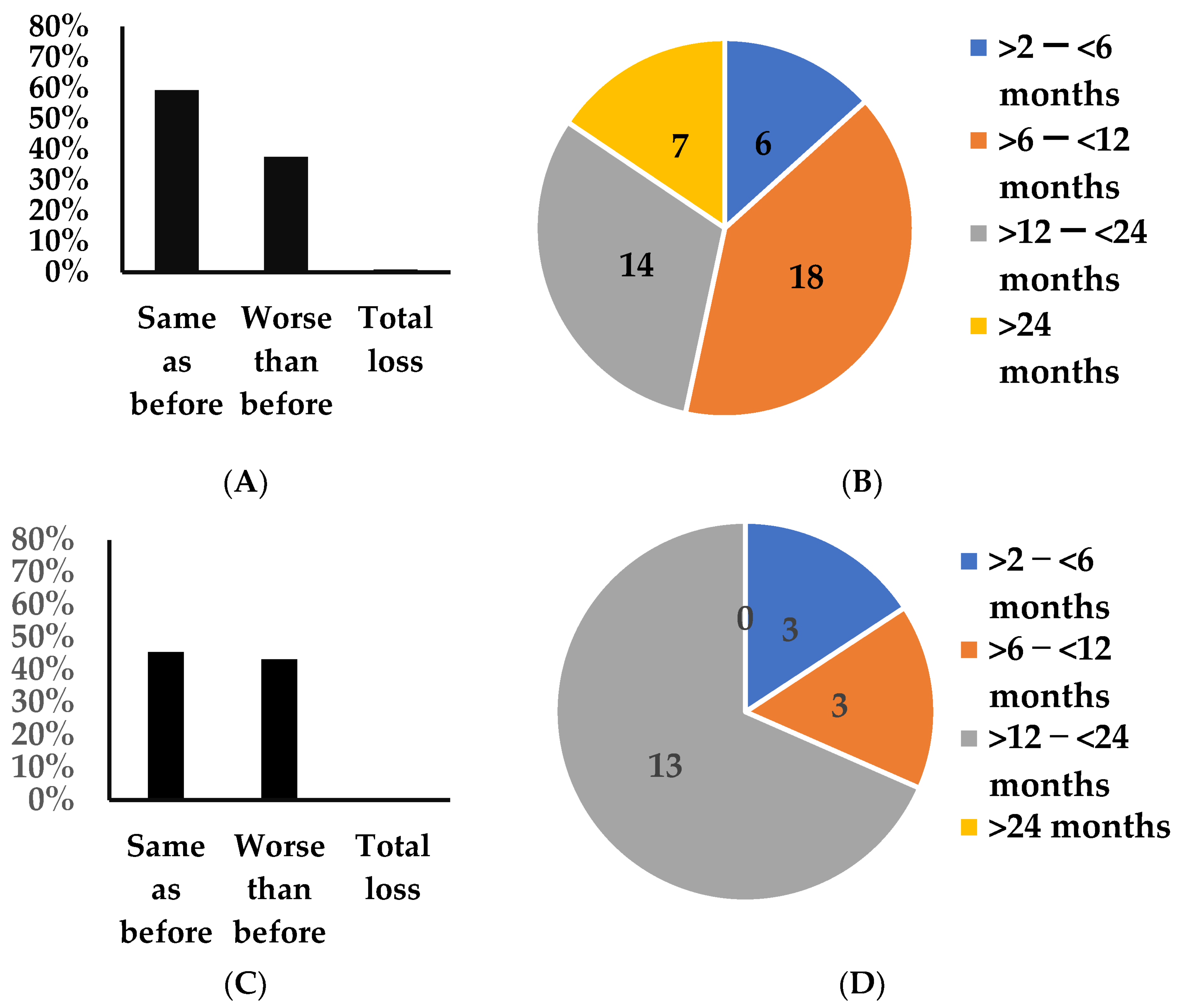
3.2. Incidence of Long COVID Symptomatology
3.3. Chemosensory Symptoms in Long COVID and COVID Reinfection
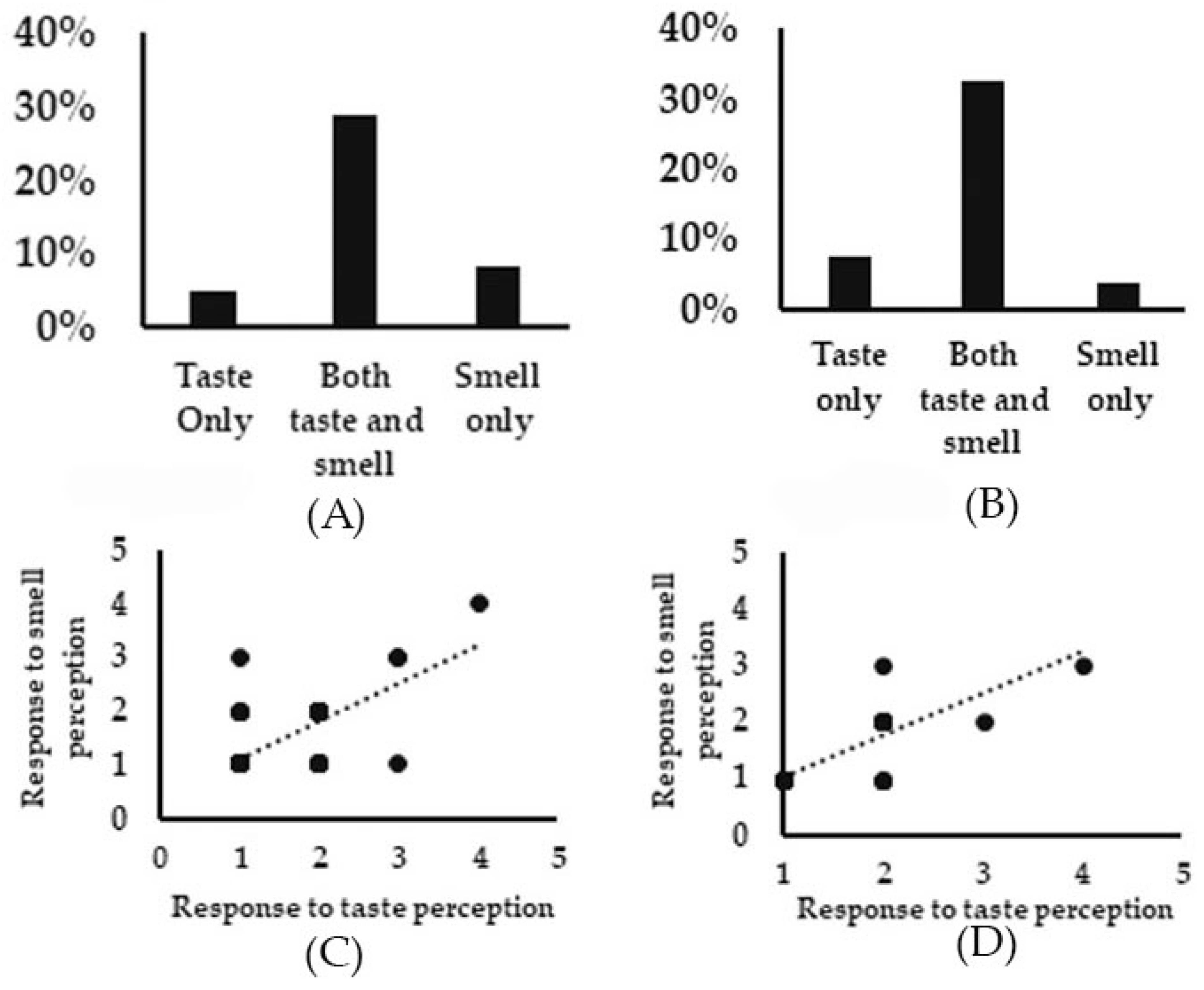
3.3.1. Changes in Taste Perception
3.3.2. Changes in Smell Perception
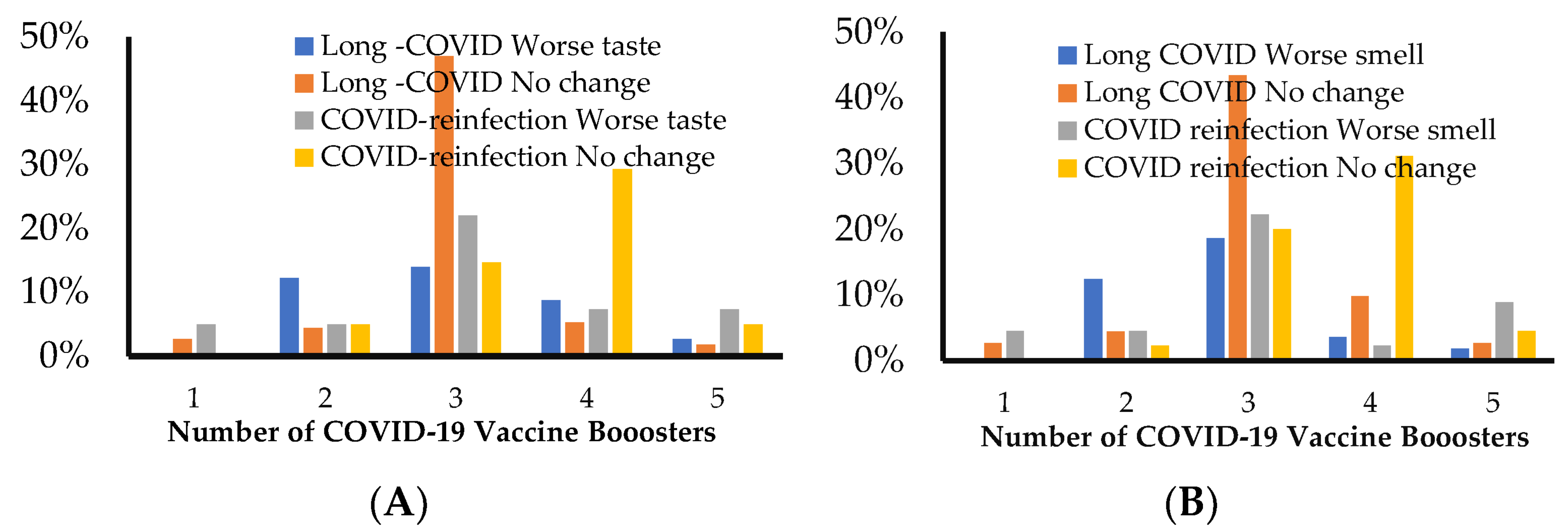
3.3.3. Correlation between Vaccination and Smell/Taste Perception in Long COVID and COVID Reinfection
3.3.4. Correlation between Taste and Smell Perception and with Other Neurological Symptoms
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/WHO (accessed on 18 April 2023).
- Fernandez-de-Las-Penas, C.; Palacios-Cena, D.; Gomez-Mayordomo, V.; Cuadrado, M.L.; Florencio, L.L. Defining Post-COVID Symptoms (Post-Acute COVID, Long COVID, Persistent Post-COVID): An Integrative Classification. Int. J. Environ. Res. Public Health 2021, 18, 2621. [Google Scholar] [CrossRef]
- Ma, Y.; Deng, J.; Liu, Q.; Du, M.; Liu, M.; Liu, J. Long-Term Consequences of Asymptomatic SARS-CoV-2 Infection: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2023, 20, 1613. [Google Scholar] [CrossRef]
- Binmadi, N.O.; Aljohani, S.; Alsharif, M.T.; Almazrooa, S.A.; Sindi, A.M. Oral Manifestations of COVID-19: A Cross-Sectional Study of Their Prevalence and Association with Disease Severity. J. Clin. Med. 2022, 11, 4461. [Google Scholar] [CrossRef]
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J.V. Condition WHOCCDWGoP-C-: A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect Dis. 2022, 22, e102–e107. [Google Scholar] [CrossRef]
- Deng, J.; Ma, Y.; Liu, Q.; Du, M.; Liu, M.; Liu, J. Severity and Outcomes of SARS-CoV-2 Reinfection Compared with Primary Infection: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2023, 20, 3335. [Google Scholar] [CrossRef] [PubMed]
- Brindisi, G.; Spalice, A.; Anania, C.; Bonci, F.; Gori, A.; Capponi, M.; Cinicola, B.; De Castro, G.; Martinelli, I.; Pulvirenti, F.; et al. COVID-19, Anosmia, and Allergies: Is There a Relationship? A Pediatric Perspective. J. Clin. Med. 2022, 11, 5019. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-de-Las-Penas, C.; Notarte, K.I.; Peligro, P.J.; Velasco, J.V.; Ocampo, M.J.; Henry, B.M.; Arendt-Nielsen, L.; Torres-Macho, J.; Plaza-Manzano, G. Long-COVID Symptoms in Individuals Infected with Different SARS-CoV-2 Variants of Concern: A Systematic Review of the Literature. Viruses 2022, 14, 2629. [Google Scholar] [CrossRef]
- Brindisi, G.; De Vittori, V.; De Nola, R.; Pignataro, E.; Anania, C.; De Castro, G.; Cinicola, B.; Gori, A.; Cicinelli, E.; Zicari, A.M. Updates on Children with Allergic Rhinitis and Asthma during the COVID-19 Outbreak. J. Clin. Med. 2021, 10, 2278. [Google Scholar] [CrossRef] [PubMed]
- Agyeman, A.A.; Chin, K.L.; Landersdorfer, C.B.; Liew, D.; Ofori-Asenso, R. Smell and Taste Dysfunction in Patients with COVID-19: A Systematic Review and Meta-analysis. Mayo Clin. Proc. 2020, 95, 1621–1631. [Google Scholar] [CrossRef]
- Schwab, J.; Jensen, C.D.; Fjaeldstad, A.W. Sustained Chemosensory Dysfunction during the COVID-19 Pandemic. ORL J. Otorhinolaryngol. Relat. Spec. 2021, 83, 209–218. [Google Scholar] [CrossRef]
- von Bartheld, C.S.; Hagen, M.M.; Butowt, R. Prevalence of Chemosensory Dysfunction in COVID-19 Patients: A Systematic Review and Meta-analysis Reveals Significant Ethnic Differences. ACS Chem. Neurosci. 2020, 11, 2944–2961. [Google Scholar] [CrossRef] [PubMed]
- Printza, A.; Constantinidis, J. The role of self-reported smell and taste disorders in suspected COVID-19. Eur. Arch. Otorhinolaryngol. 2020, 277, 2625–2630. [Google Scholar] [CrossRef] [PubMed]
- Schambeck, S.E.; Mateyka, L.M.; Burrell, T.; Graf, N.; Brill, I.; Stark, T.; Protzer, U.; Busch, D.H.; Gerhard, M.; Riehl, H.; et al. Two-Year Follow-Up on Chemosensory Dysfunction and Adaptive Immune Response after Infection with SARS-CoV-2 in a Cohort of 44 Healthcare Workers. Life 2022, 12, 1556. [Google Scholar] [CrossRef] [PubMed]
- Tan, B.K.J.; Han, R.; Zhao, J.J.; Tan, N.K.W.; Quah, E.S.H.; Tan, C.J.; Chan, Y.H.; Teo, N.W.Y.; Charn, T.C.; See, A.; et al. Prognosis and persistence of smell and taste dysfunction in patients with covid-19: Meta-analysis with parametric cure modelling of recovery curves. BMJ 2022, 378, e069503. [Google Scholar] [CrossRef] [PubMed]
- Printza, A.; Katotomichelakis, M.; Valsamidis, K.; Metallidis, S.; Panagopoulos, P.; Panopoulou, M.; Petrakis, V.; Constantinidis, J. Smell and Taste Loss Recovery Time in COVID-19 Patients and Disease Severity. J. Clin. Med. 2021, 10, 966. [Google Scholar] [CrossRef] [PubMed]
- Ercoli, T.; Masala, C.; Pinna, I.; Orofino, G.; Solla, P.; Rocchi, L.; Defazio, G. Qualitative smell/taste disorders as sequelae of acute COVID-19. Neurol. Sci. 2021, 42, 4921–4926. [Google Scholar] [CrossRef]
- Gurrola, J.G., 2nd; Chang, J.L.; Roland, L.T.; Loftus, P.A.; Cheung, S.W. Short-term chemosensory distortions and phantoms in COVID-19. Laryngoscope Investig. Otolaryngol. 2021, 6, 172–176. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- Bai, F.; Tomasoni, D.; Falcinella, C.; Barbanotti, D.; Castoldi, R.; Mule, G.; Augello, M.; Mondatore, D.; Allegrini, M.; Cona, A.; et al. Female gender is associated with long COVID syndrome: A prospective cohort study. Clin. Microbiol. Infect. 2022, 28, 611.E9–611.E16. [Google Scholar] [CrossRef]
- Notarte, K.I.; de Oliveira, M.H.S.; Peligro, P.J.; Velasco, J.V.; Macaranas, I.; Ver, A.T.; Pangilinan, F.C.; Pastrana, A.; Goldrich, N.; Kavteladze, D.; et al. Age, Sex and Previous Comorbidities as Risk Factors Not Associated with SARS-CoV-2 Infection for Long COVID-19: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 7314. [Google Scholar] [CrossRef]
- Nikolic Turnic, T.; Vasiljevic, I.; Stanic, M.; Jakovljevic, B.; Mikerova, M.; Ekkert, N.; Reshetnikov, V.; Jakovljevic, V. Post-COVID-19 Status and Its Physical, Nutritional, Psychological, and Social Effects in Working-Age Adults-A Prospective Questionnaire Study. J. Clin. Med. 2022, 11, 6668. [Google Scholar] [CrossRef]
- Jain, A.; Kaur, J.; Rai, A.K.; Pandey, A.K. Anosmia: A Clinical Indicator of COVID-19 Reinfection. Ear. Nose Throat J. 2021, 100 (Suppl. 2), 180S–181S. [Google Scholar] [CrossRef]
- Graham, C.S.; Graham, B.G.; Bartlett, J.A.; Heald, A.E.; Schiffman, S.S. Taste and smell losses in HIV infected patients. Physiol. Behav. 1995, 58, 287–293. [Google Scholar] [CrossRef]
- Henin, D.; Pellegrini, G.; Carmagnola, D.; Lanza Attisano, G.C.; Lopez, G.; Ferrero, S.; Amendola, A.; De Angelis, D.; Tanzi, E.; Dellavia, C. Morphological and Immunopathological Aspects of Lingual Tissues in COVID-19. Cells 2022, 11, 1248. [Google Scholar] [CrossRef] [PubMed]
- Henkin, R.I.; Larson, A.L.; Powell, R.D. Hypogeusia, dysgeusia, hyposmia, and dysosmia following influenza-like infection. Ann. Otol. Rhinol. Laryngol. 1975, 84, 672–682. [Google Scholar] [CrossRef]
- Henkin, R.I.; Levy, L.M.; Fordyce, A. Taste and smell function in chronic disease: A review of clinical and biochemical evalu-ations of taste and smell dysfunction in over 5000 patients at The Taste and Smell Clinic in Washington, DC. Am. J. Otolaryngol. 2013, 34, 477–489. [Google Scholar] [CrossRef] [PubMed]
- Huart, C.; Philpott, C.; Konstantinidis, I.; Altundag, A.; Whitcroft, K.L.; Trecca, E.M.C.; Cassano, M.; Rombaux, P.; Hummel, T. Comparison of COVID-19 and common cold chemosensory dysfunction. Rhinology 2020, 58, 623–625. [Google Scholar] [CrossRef] [PubMed]
- Cooper, K.W.; Brann, D.H.; Farruggia, M.C.; Bhutani, S.; Pellegrino, R.; Tsukahara, T.; Weinreb, C.; Joseph, P.V.; Larson, E.D.; Parma, V.; et al. COVID-19 and the Chemical Senses: Supporting Players Take Center Stage. Neuron 2020, 107, 219–233. [Google Scholar] [CrossRef]
- Saniasiaya, J.; Islam, M.A.; Abdullah, B. Prevalence and Characteristics of Taste Disorders in Cases of COVID-19: A Meta-analysis of 29,349 Patients. Otolaryngol. Head Neck Surg. 2021, 165, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Bowe, B.; Xie, Y.; Al-Aly, Z. Acute and postacute sequelae associated with SARS-CoV-2 reinfection. Nat. Med. 2022, 28, 2398–2405. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; Jing, Q.; Zhu, E.; Liu, Q.; Fei, M.; Zhang, H.; An, G.; Cao, S.; Tang, J.; Xu, G.; et al. Alterations in smell or taste in individuals infected with SARS-CoV-2 during periods of Omicron variant dominance. Int. J. Infect Dis. 2023, 128, 278–284. [Google Scholar] [CrossRef] [PubMed]
- Vihta, K.D.; Pouwels, K.B.; Peto, T.E.; Pritchard, E.; House, T.; Studley, R.; Rourke, E.; Cook, D.; Diamond, I.; Crook, D.; et al. Omicron-associated changes in SARS-CoV-2 symptoms in the United Kingdom. Clin. Infect Dis. 2022, 76, e133–e141. [Google Scholar] [PubMed]
- Notarte, K.I.; Catahay, J.A.; Velasco, J.V.; Pastrana, A.; Ver, A.T.; Pangilinan, F.C.; Peligro, P.J.; Casimiro, M.; Guerrero, J.J.; Gellaco, M.M.L.; et al. Impact of COVID-19 vaccination on the risk of developing long-COVID and on existing long-COVID symptoms: A systematic review. eClinicalMedicine 2022, 53, 101624. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, M. Taste Dysfunction and Long COVID-19. Front. Cell. Infect. Microbiol. 2021, 11, 716563. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| (A) | |||
| Long COVID (N = 127) | COVID reinfection (N = 47) | p value | |
| Age | 46.7 ± 17.8 yrs | 45.8 ± 13.9 yrs | 0.37 |
| Sex | 29 M:92 F * | 11 M:36 F | |
| Mean duration | 352.4 ± 250 days | 488 ± 228.5 days | 0.0007 |
| Vaccination: % N (V + booster) | 2% (1 + 0) | 6% (1 + 0) | 0.54 |
| 19% (1 + 1) | 15% (1 + 1) | ||
| 57% (1 + 2) | 55% (1 + 2) | ||
| 13% (1 + 3) | 13% (1 + 3) | ||
| 6% (1 + 4) | 11% (1 + 4) | ||
| 2% (1 + 5) | 0% (1 + 5) | ||
| (B) | |||
| Number of individuals | |||
| Duration (days) | Long COVID | COVID reinfection | |
| 60–119 | 25 | 4 | |
| 120–179 | 9 | 1 | |
| 180–239 | 31 | 5 | |
| 240–299 | 13 | 6 | |
| 300–359 | 7 | 1 | |
| 360–419 | 2 | 0 | |
| 420–479 | 0 | 0 | |
| 480–539 | 0 | 4 | |
| 540–599 | 8 | 4 | |
| 600–659 | 9 | 8 | |
| 660–719 | 10 | 9 | |
| 720–779 | 4 | 3 | |
| 780–839 | 2 | 0 | |
| 840–899 | 6 | 2 | |
| 900–959 | 1 | 4 | |
| Total | 127 | 47 | |
| History of hospitalization | 6 | 4 | |
| (A) | ||||
| Taste | Long COVID | COVID Reinfection | ||
| Duration | No Changes (82) | Worse @ (35) | No changes (23) | Worse @ (18) |
| 2 to 6 months | 27 (23%) | 4 (3%) | 3 (7%) | 1 (2%) |
| >6 to 12 months | 36 (31%) | 13 (11%) | 8 (20%) | 4 (10%) |
| >12 to 24 months | 16 (14%) | 11 (9%) | 9 (22%) | 12 (29%) |
| >24 months | 3 (3%) | 7 (6%) | 3 (7%) | 1 (2%) |
| Chi-square | 13.72 | 3.2 | ||
| p value | 0.003 | 0.36 | ||
| (B) | ||||
| Smell | Long COVID | COVID reinfection | ||
| No changes (71) | Worse @ (45) | No changes (22) | Worse @ (19) | |
| 2 to 6 months | 25 (22%) | 6 (5%) | 4 (7%) | 3 (7%) |
| >6 to 12 months | 30 (26%) | 18 (16%) | 3 (10%) | 3 (7%) |
| >12 to 24 months | 13 (11%) | 14 (12%) | 11 (27%) | 13 (32%) |
| >24 months | 3 (3%) | 7 (6%) | 4 (10%) | 0 |
| Chi-square | 11.1 | 4.1 | ||
| p value | 0.012 | 0.25 | ||
| Worse than Pre COVID | <12 Months | 12–24 Months | >24 Months | Chi-Square | p-Value | |
|---|---|---|---|---|---|---|
| Taste | Long COVID (35) | 17 (49%) | 11 (31%) | 7 (20%) | 6.23 | 0.043 |
| COVID reinfection (18) | 5 (28%) | 12 (67%) | 1 (6%) | |||
| Smell | Long COVID (45) | 24 (53%) | 14 (31%) | 7 (16%) | 17.56 | 0.0002 |
| COVID reinfection (19) | 6 (32%) | 13 (68%) | 0 | |||
| Change from Pre COVID | ||||||
|---|---|---|---|---|---|---|
| Chi-Square | p-Value | |||||
| Long COVID | Headache | 78 (69%) (Never and rarely) | 27 (20%) Sometimes | 17 (10%) Often and always | 17.16 | 0.0002 |
| Taste | 81 (66%) (No change) | 41 (33%) Worse | 1 (1%) Total loss | |||
| COVID reinfection | Headache | 23 (50%) | 18 (39%) | 11 (24%) | 9.25 | 0.0098 |
| Taste | 27 (59%) | 23 (50%) | 1 (2%) | |||
| Long COVID | Joint pain | 82 (65%) | 20 (15%) | 24(19%) | 28.36 | 0.0000007 |
| Taste | 81 (66%) | 41 (33%) | 1 (1%) | |||
| COVID reinfection | Joint pain | 29 (63%) | 10 (22%) | 13 (28%) | 15.5 | 0.00044 |
| Taste | 27 (59%) | 23 (50%) | 1 (2%) | |||
| Long COVID | Headache | 78 (69%) | 27 (20%) | 17 (10%) | 18.71 | 0.000087 |
| Smell | 78 (63%) | 45 (34%) | 1 (1%) | |||
| COVID reinfection | Headache | 23 (50%) | 18 (39%) | 11 (24%) | 10.04 | 0.0066 |
| Smell | 25 (54%) | 19 (41%) | 0 | |||
| Long COVID | Joint pain | 82 (65%) | 20 (15%) | 24 (19%) | 30.86 | 0.0000002 |
| Smell | 78 (63%) | 45 (34%) | 1 (1%) | |||
| COVID reinfection | Joint pain | 29 (63%) | 10 (22%) | 13 (28%) | 15.5 | 0.00044 |
| Smell | 25 (54%) | 19 (41%) | 0 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jaramillo, M.; Thyvalikakath, T.P.; Eckert, G.; Srinivasan, M. Characteristics of Chemosensory Perception in Long COVID and COVID Reinfection. J. Clin. Med. 2023, 12, 3598. https://doi.org/10.3390/jcm12103598
Jaramillo M, Thyvalikakath TP, Eckert G, Srinivasan M. Characteristics of Chemosensory Perception in Long COVID and COVID Reinfection. Journal of Clinical Medicine. 2023; 12(10):3598. https://doi.org/10.3390/jcm12103598
Chicago/Turabian StyleJaramillo, Mikki, Thankam P. Thyvalikakath, George Eckert, and Mythily Srinivasan. 2023. "Characteristics of Chemosensory Perception in Long COVID and COVID Reinfection" Journal of Clinical Medicine 12, no. 10: 3598. https://doi.org/10.3390/jcm12103598
APA StyleJaramillo, M., Thyvalikakath, T. P., Eckert, G., & Srinivasan, M. (2023). Characteristics of Chemosensory Perception in Long COVID and COVID Reinfection. Journal of Clinical Medicine, 12(10), 3598. https://doi.org/10.3390/jcm12103598