
Prevalence of Clinical Signs and Symptoms of Temporomandibular Joint Disorders Registered in the EUROTMJ Database: A Prospective Study in a Portuguese Center

 ,
,
Abstract
1. Introduction
2. Materials and Methods
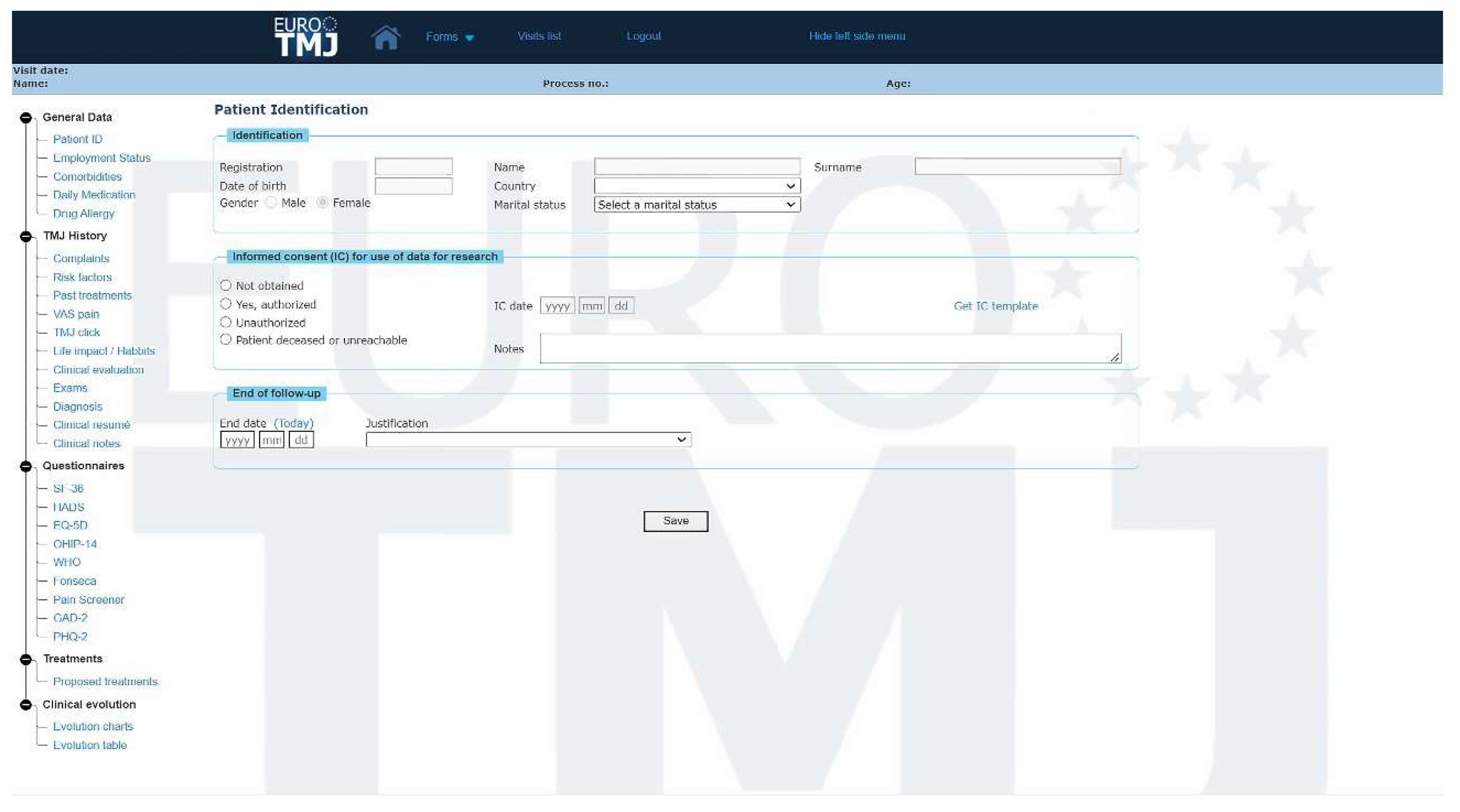
2.1. Database Description
2.2. Study Design and Data Collection
2.3. Statistical Analysis
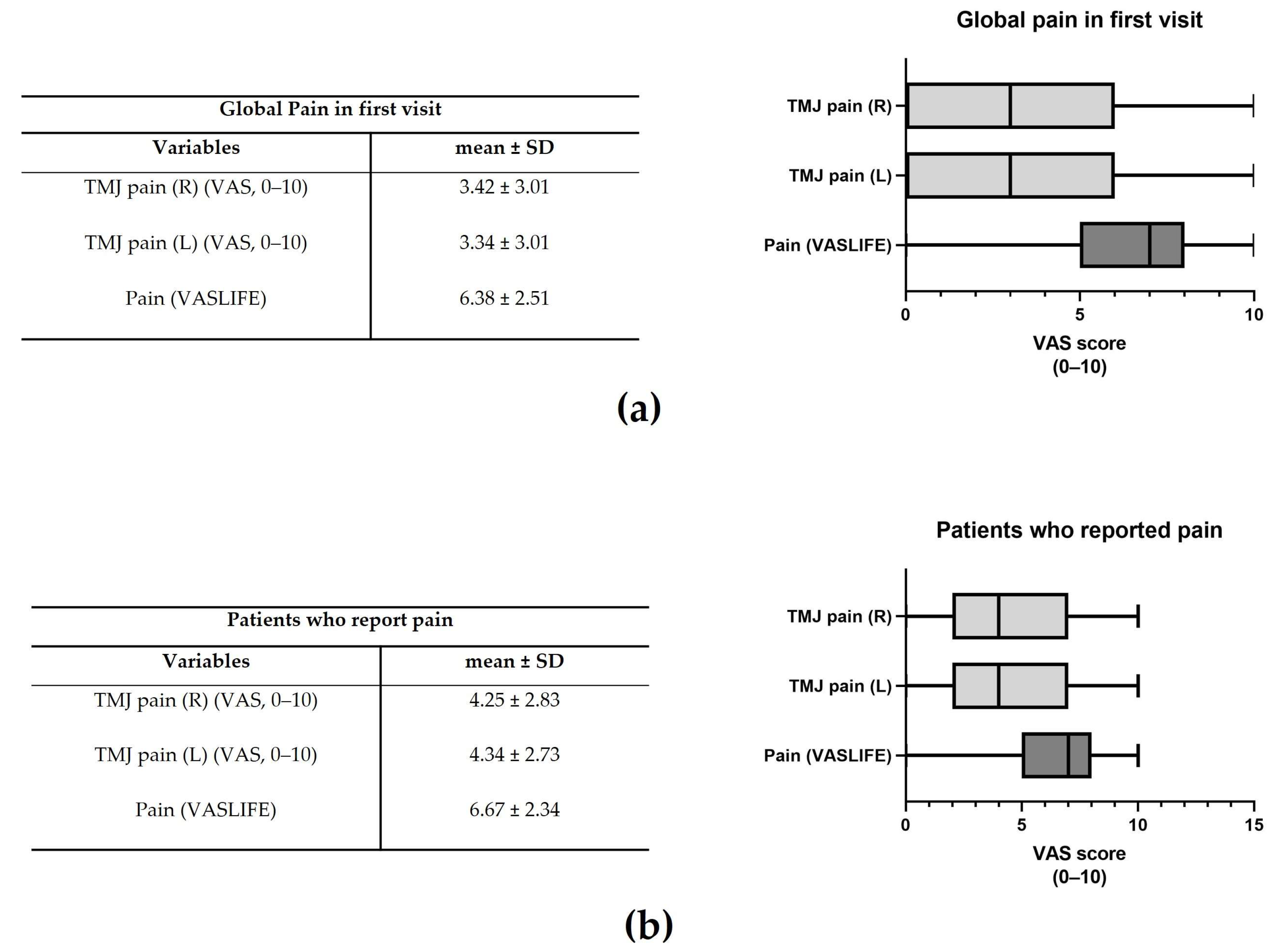
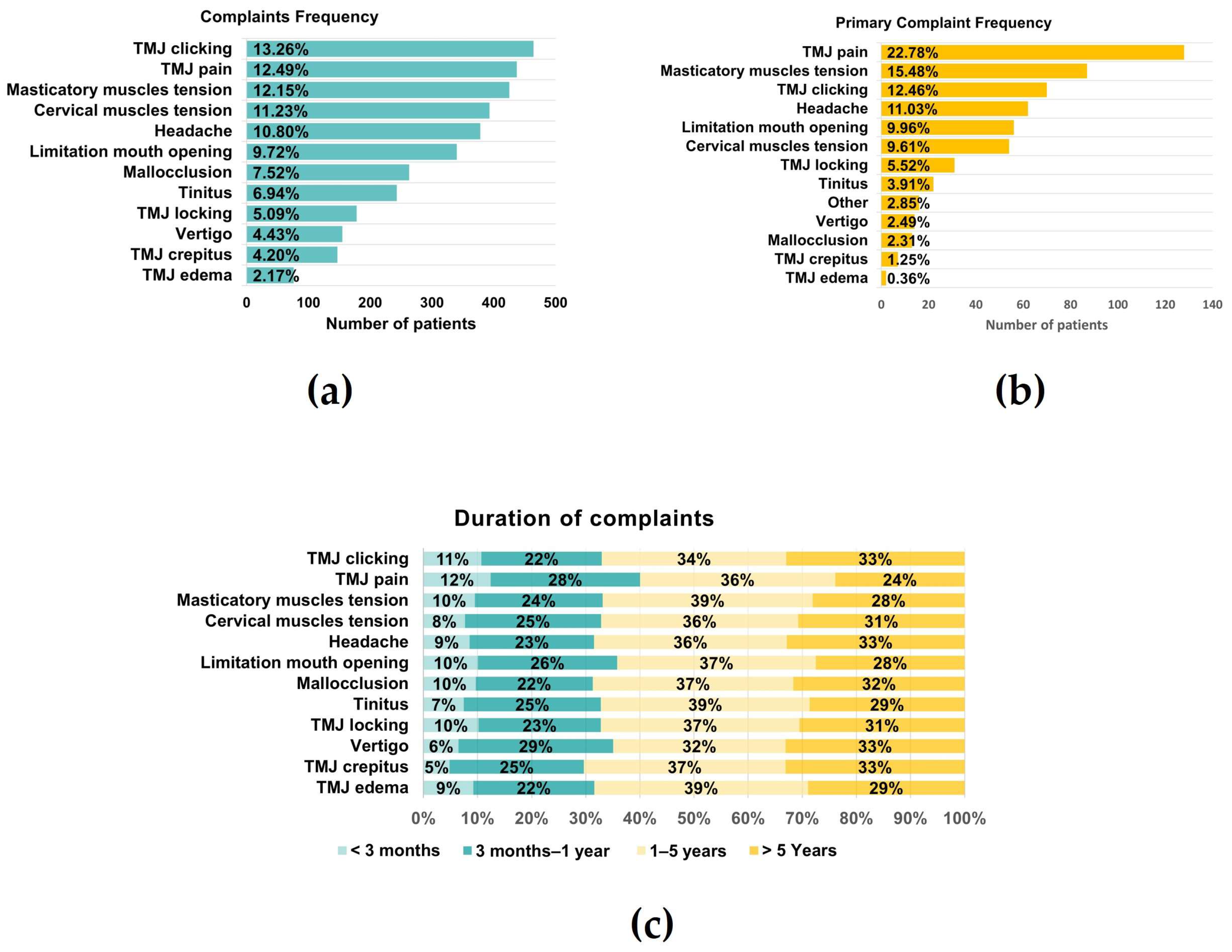
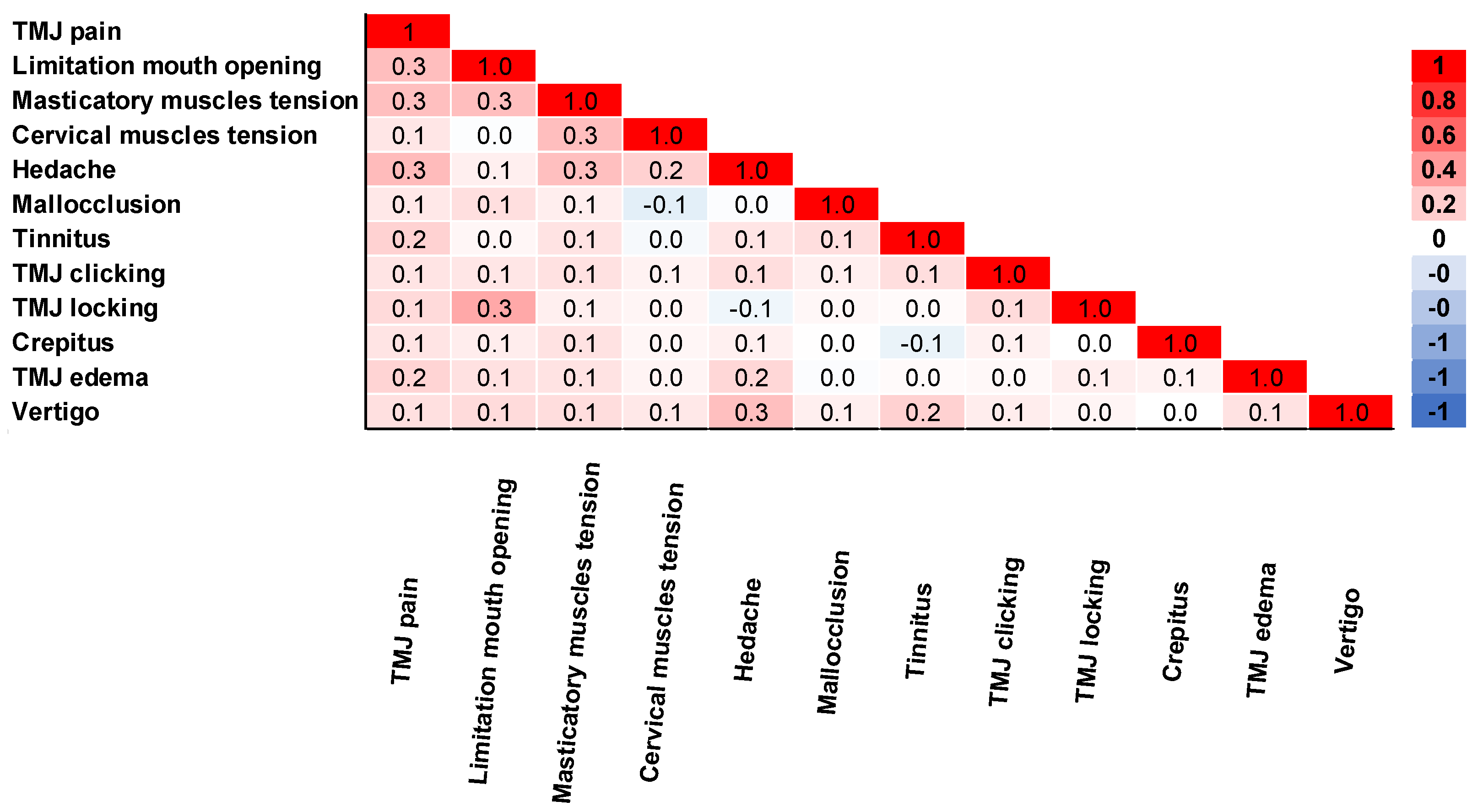
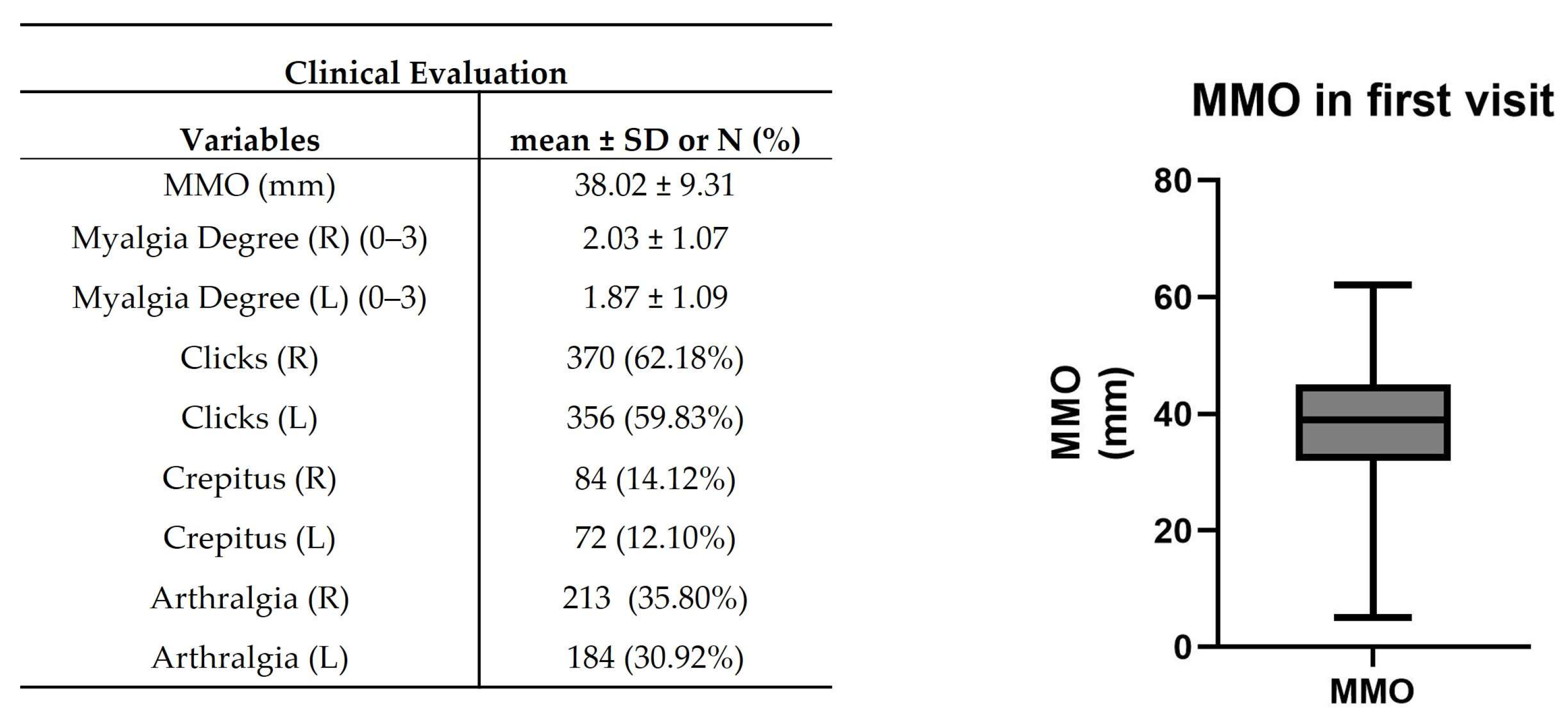
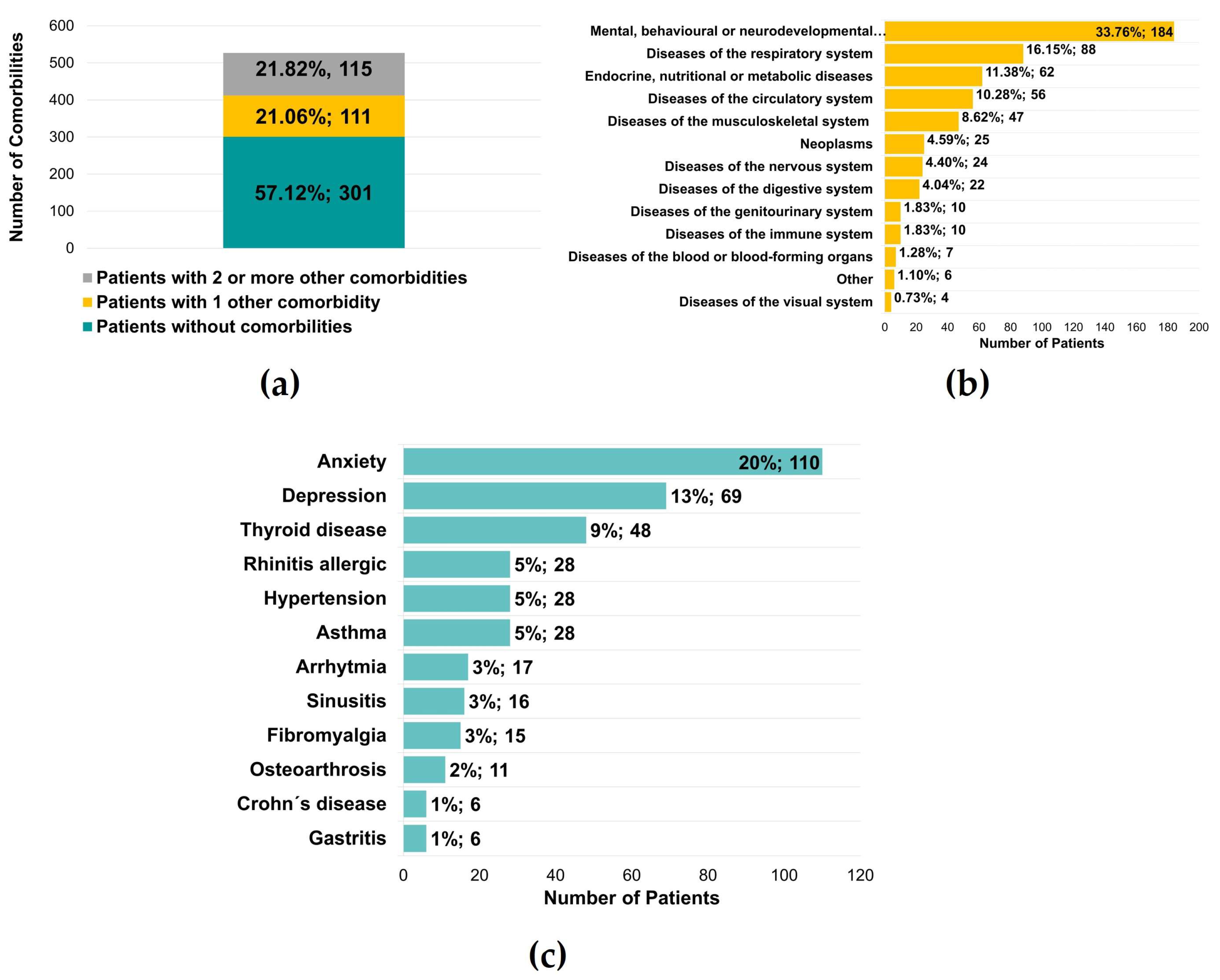
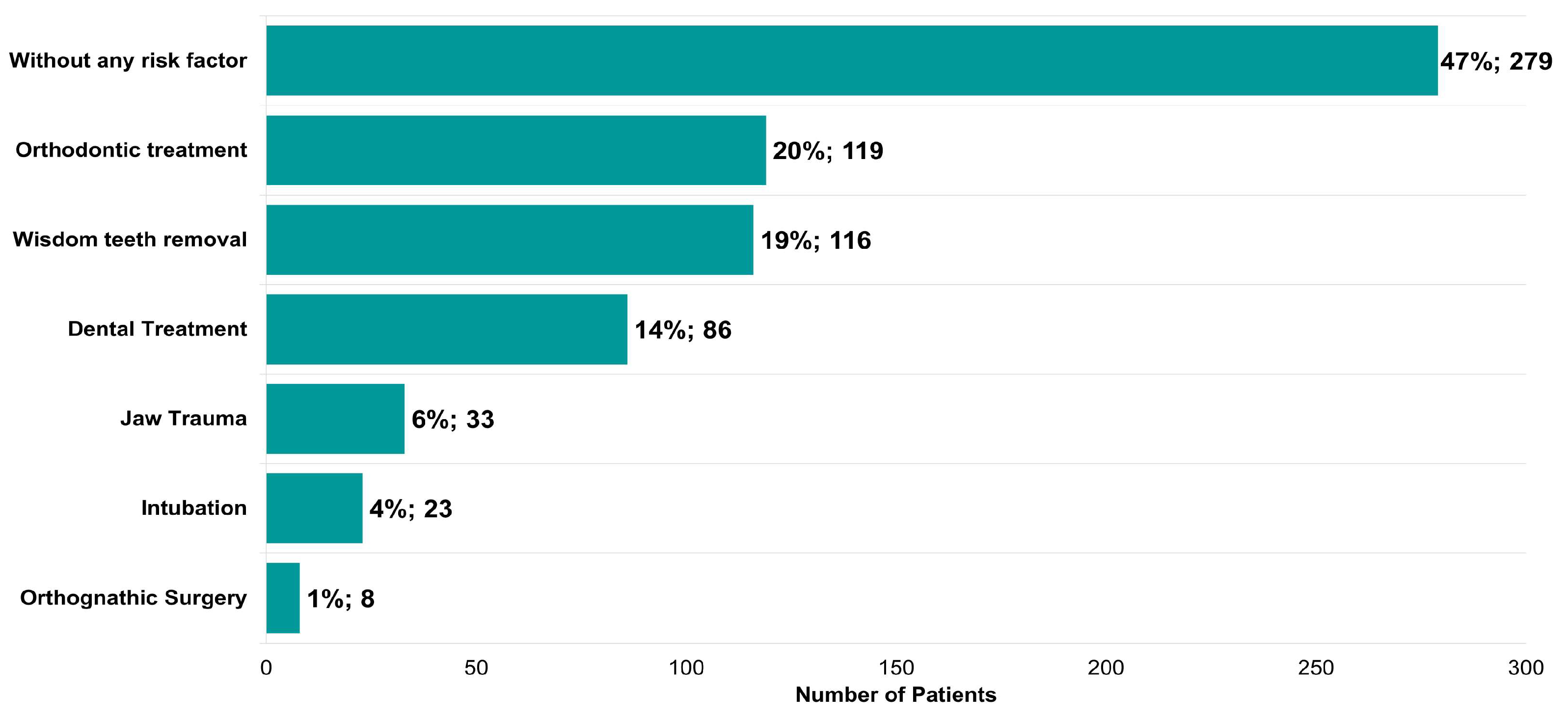
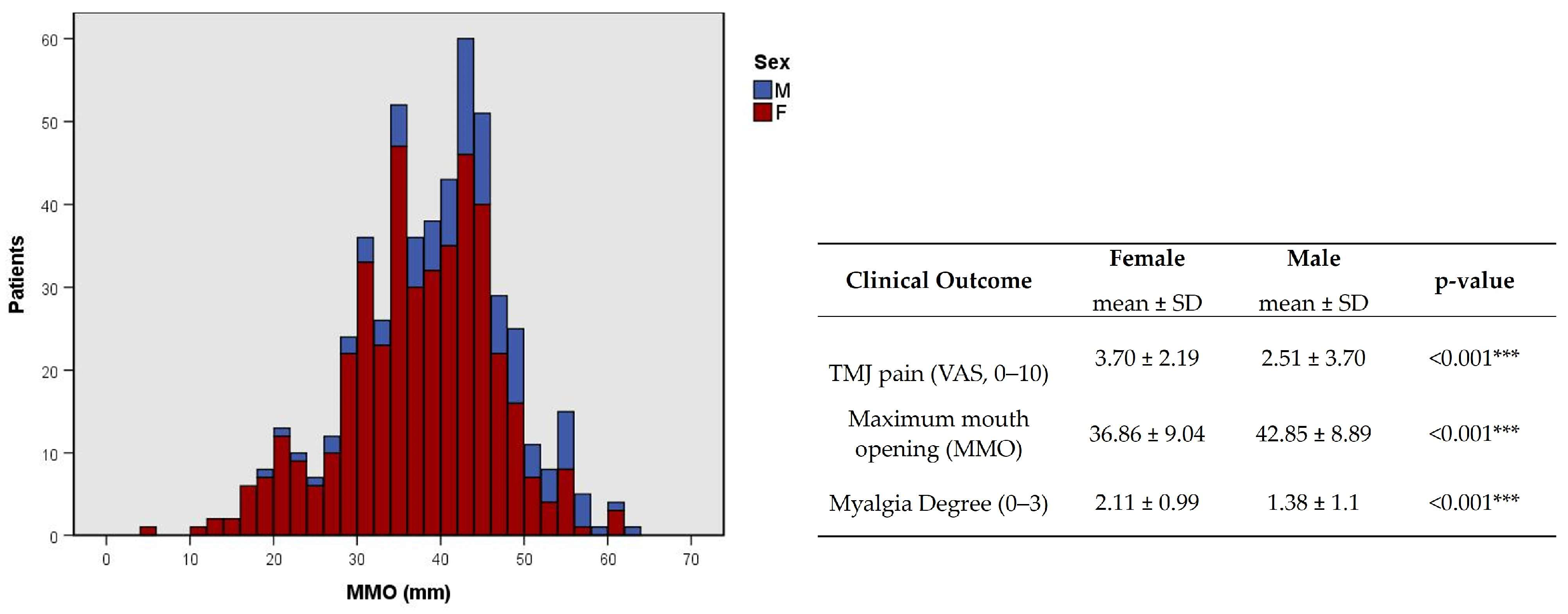
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chaurasia, A.; Ishrat, S.; Katheriya, G.; Chaudhary, P.K.; Dhingra, K.; Nagar, A. Temporomandibular disorders in North Indian population visiting a tertiary care dental hospital. Natl. J. Maxillofac. Surg. 2020, 11, 106–109. [Google Scholar] [CrossRef] [PubMed]
- Qvintus, V.; Sipilä, K.; Le Bell, Y.; Suominen, A.L. Prevalence of clinical signs and pain symptoms of temporomandibular disorders and associated factors in adult Finns. Acta Odontol. Scand. 2020, 78, 515–521. [Google Scholar] [CrossRef] [PubMed]
- Iodice, G.; Cimino, R.; Vollaro, S.; Lobbezoo, F.; Michelotti, A. Prevalence of temporomandibular disorder pain, jaw noises and oral behaviours in an adult Italian population sample. J. Oral. Rehabil. 2019, 46, 691–698. [Google Scholar] [CrossRef]
- Kmeid, E.; Nacouzi, M.; Hallit, S.; Rohayem, Z. Prevalence of temporomandibular joint disorder in the Lebanese population, and its association with depression, anxiety, and stress. Head Face Med. 2020, 16, 19. [Google Scholar] [CrossRef] [PubMed]
- Valesan, L.F.; Da-Cas, C.D.; Réus, J.C.; Denardin, A.C.S.; Garanhani, R.R.; Bonotto, D.; Januzzi, E.; de Souza, B.D.M. Prevalence of temporomandibular joint disorders: A systematic review and meta-analysis. Clin. Oral Investig. 2021, 25, 441–453. [Google Scholar] [CrossRef] [PubMed]
- Manfredini, D.; Piccotti, F.; Ferronato, G.; Guarda-Nardini, L. Age peaks of different RDC/TMD diagnoses in a patient population. J. Dent. 2010, 38, 392–399. [Google Scholar] [CrossRef]
- Johansson, A.; Unell, L.; Carlsson, G.E.; Söderfeldt, B.; Halling, A. Risk factors associated with symptoms of temporomandibular disorders in a population of 50- and 60-year-old subjects. J. Oral. Rehabil. 2006, 33, 473–481. [Google Scholar] [CrossRef]
- de Boer, A.G.; van Lanschot, J.J.; Stalmeier, P.F.; van Sandick, J.W.; Hulscher, J.B.; de Haes, J.C.; Sprangers, M.A. Is a single-item visual analogue scale as valid, reliable and responsive as multi-item scales in measuring quality of life? Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 2004, 13, 311–320. [Google Scholar] [CrossRef]
- Schiffman, E.L.; Ohrbach, R.; Truelove, E.L.; Tai, F.; Anderson, G.C.; Pan, W.; Gonzalez, Y.M.; John, M.T.; Sommers, E.; List, T.; et al. The Research Diagnostic Criteria for Temporomandibular Disorders. V: Methods used to establish and validate revised Axis I diagnostic algorithms. J. Orofac. Pain 2010, 24, 63–78. [Google Scholar]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.-P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Group. J. Oral Facial Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef]
- Goiato, M.C.; Zuim, P.R.J.; Moreno, A.; Dos Santos, D.M.; da Silva, E.V.F.; de Caxias, F.P.; Turcio, K.H.L. Does pain in the masseter and anterior temporal muscles influence maximal bite force? Arch. Oral Biol. 2017, 83, 1–6. [Google Scholar] [CrossRef]
- Kothari, K.; Jayakumar, N.; Razzaque, A. Multidisciplinary management of temporomandibular joint ankylosis in an adult: Journey from arthroplasty to oral rehabilitation. BMJ Case Rep. 2021, 14, e245120. [Google Scholar] [CrossRef]
- Gesch, D.; Bernhardt, O.; Alte, D.; Schwahn, C.; Kocher, T.; John, U.; Hensel, E. Prevalence of signs and symptoms of temporomandibular disorders in an urban and rural German population: Results of a population-based Study of Health in Pomerania. Quintessence Int. 2004, 35, 143–150. [Google Scholar]
- Feteih, R.M. Signs and symptoms of temporomandibular disorders and oral parafunctions in urban Saudi Arabian adolescents: A research report. Head Face Med. 2006, 2, 25. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, D.A.; Dal Fabbro, A.L.; Campos, J.A.; Bigal, M.E.; Speciali, J.G. Symptoms of temporomandibular disorders in the population: An epidemiological study. J. Orofac. Pain 2010, 24, 270–278. [Google Scholar] [PubMed]
- Mobilio, N.; Casetta, I.; Cesnik, E.; Catapano, S. Prevalence of self-reported symptoms related to temporomandibular disorders in an Italian population. J. Oral. Rehabil. 2011, 38, 884–890. [Google Scholar] [CrossRef] [PubMed]
- Könönen, M.; Waltimo, A.; Nyström, M. Does clicking in adolescence lead to painful temporomandibular joint locking? Lancet 1996, 347, 1080–1081. [Google Scholar] [CrossRef] [PubMed]
- Lamot, U.; Strojan, P.; Šurlan Popovič, K. Magnetic resonance imaging of temporomandibular joint dysfunction-correlation with clinical symptoms, age, and gender. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 116, 258–263. [Google Scholar] [CrossRef]
- Abrahamsson, A.K.; Kristensen, M.; Arvidsson, L.Z.; Kvien, T.K.; Larheim, T.A.; Haugen, I.K. Frequency of temporomandibular joint osteoarthritis and related symptoms in a hand osteoarthritis cohort. Osteoarthr. Cartil. 2017, 25, 654–657. [Google Scholar] [CrossRef]
- Almoznino, G.; Zini, A.; Zakuto, A.; Zlutzky, H.; Bekker, S.; Shay, B.; Haviv, Y.; Sharav, Y.; Benoliel, R. Cervical Muscle Tenderness in Temporomandibular Disorders and Its Associations with Diagnosis, Disease-Related Outcomes, and Comorbid Pain Conditions. J. Oral Facial Pain Headache 2020, 34, 67–76. [Google Scholar] [CrossRef]
- Zieliński, G.; Byś, A.; Szkutnik, J.; Majcher, P.; Ginszt, M. Electromyographic Patterns of Masticatory Muscles in Relation to Active Myofascial Trigger Points of the Upper Trapezius and Temporomandibular Disorders. Diagnostics 2021, 11, 580. [Google Scholar] [CrossRef] [PubMed]
- Al-Baghdadi, M.; Durham, J.; Araujo-Soares, V.; Robalino, S.; Errington, L.; Steele, J. TMJ Disc Displacement without Reduction Management: A Systematic Review. J. Dent. Res. 2014, 93, 37s–51s. [Google Scholar] [CrossRef]
- Ângelo, D.F.; Sousa, R.; Pinto, I.; Sanz, D.; Gil, F.M.; Salvado, F. Early magnetic resonance imaging control after temporomandibular joint arthrocentesis. Ann. Maxillofac. Surg. 2015, 5, 255–257. [Google Scholar] [CrossRef] [PubMed]
- Marklund, S.; Wänman, A. Risk factors associated with incidence and persistence of signs and symptoms of temporomandibular disorders. Acta Odontol. Scand. 2010, 68, 289–299. [Google Scholar] [CrossRef]
- Johansson, A.; Unell, L.; Carlsson, G.; Söderfeldt, B.; Halling, A.; Widar, F. Associations between social and general health factors and symptoms related to temporomandibular disorders and bruxism in a population of 50-year-old subjects. Acta Odontol. Scand. 2004, 62, 231–237. [Google Scholar] [CrossRef] [PubMed]
- De La Torre Canales, G.; Câmara-Souza, M.B.; Muñoz Lora, V.R.M.; Guarda-Nardini, L.; Conti, P.C.R.; Rodrigues Garcia, R.M.; Del Bel Cury, A.A.; Manfredini, D. Prevalence of psychosocial impairment in temporomandibular disorder patients: A systematic review. J. Oral. Rehabil. 2018, 45, 881–889. [Google Scholar] [CrossRef]
- Rauch, A.; Hahnel, S.; Kloss-Brandstätter, A.; Schierz, O. Patients referred to a German TMD-specialized consultation hour-a retrospective on patients without a diagnosis according to RDC/TMD decision trees. Clin. Oral Investig. 2021, 25, 5641–5647. [Google Scholar] [CrossRef]
- Zieliński, G.; Ginszt, M.; Zawadka, M.; Rutkowska, K.; Podstawka, Z.; Szkutnik, J.; Majcher, P.; Gawda, P. The Relationship between Stress and Masticatory Muscle Activity in Female Students. J. Clin. Med. 2021, 10, 3459. [Google Scholar] [CrossRef]
- Stocka, A.; Sierpinska, T.; Kuc, J.; Golebiewska, M. Relationship between depression and masticatory muscles function in a group of adolescents. Cranio J. Craniomandib. Pract. 2018, 36, 390–395. [Google Scholar] [CrossRef]
- Huang, F.; Zhang, M.; Chen, Y.-J.; Li, Q.; Wu, A.-Z. Psychological Stress Induces Temporary Masticatory Muscle Mechanical Sensitivity in Rats. J. Biomed. Biotechnol. 2011, 2011, 720603. [Google Scholar] [CrossRef]
- Dworkin, S.F.; Huggins, K.H.; LeResche, L.; Von Korff, M.; Howard, J.; Truelove, E.; Sommers, E. Epidemiology of signs and symptoms in temporomandibular disorders: Clinical signs in cases and controls. J. Am. Dent. Assoc. 1990, 120, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, R.G.; Kotchen, J.M.; Kotchen, T.A.; Cowley, T.; Dasgupta, M.; Cowley, A.W., Jr. Temporomandibular disorders and associated clinical comorbidities. Clin. J. Pain 2011, 27, 268–274. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | n (%), or Mean ± SD | |
|---|---|---|
| Number of patients | 595 | |
| Sex | Female | 479 (80.50%) |
| Male | 116 (19.50%) | |
| Age | 38.20 ± 15.73 | |
| Side of the joint with symptoms | Only Right | 41 (6.89%) |
| Only Left | 40 (6.72%) | |
| Bilateral | 514 (86.39%) | |
| Parafunctional Habits | ||
|---|---|---|
| Variables | n (%) | |
| Bruxism | Day | 7 (1%) |
| Night | 138 (23%) | |
| Day and Night | 35 (6%) | |
| No | 212 (36%) | |
| Does not know | 203 (34%) | |
| Clenching | Yes | 359 (60%) |
| No | 159 (27%) | |
| Does not know | 77 (13%) | |
| TMJ Pain and Clinical Variables | ||||||
|---|---|---|---|---|---|---|
| Demographic Data | TMJ Pain | Limitation of Mouth Opening | Myalgia Degree | TMJ Clicks | TMJ Crepitus | Arthralgia |
| p-Value, Cramer’s V | ||||||
| Sex | <0.001, 0.189 | <0.001, 0.154 | <0.001, 0.277 | 0.698, 0.016 | 0.179, 0.060 | 0.143, 0.064 |
| Age | 0.889, 0.060 | 0.543, 0.072 | 0.456, 0.088 | 0.002, 0.177 | <0.001, 0.229 | 0.032, 0.142 |
| TMJ Pain and Clinical Variables | ||||||
|---|---|---|---|---|---|---|
| Parafunctional Habits | TMJ Pain | Limitation of Mouth Opening | Myalgia Degree | TMJ Clicks | TMJ Crepitus | Arthralgia |
| p-Value, Cramer’s V | ||||||
| Clenching | 0.203, 0.094 | 0.340, 0.042 | 0.008, 0.159 | 0.760, 0.013 | 0.571, 0.026 | 0.677, 0.020 |
| Bruxism | 0.035, 0.148 | 0.732, 0.017 | 0.006, 0.186 | 0.890, 0.012 | 0.496, 0.036 | 0.364, 0.048 |
| Global Pain and Clinical Variables | ||||||
|---|---|---|---|---|---|---|
| Risk Factors | TMJ Pain | Open Mouth Limitation | Myalgia Degree | TMJ Clicks | TMJ Crepitus | Arthralgia |
| p-Value, Cramer’s V | ||||||
| Dental treatment | 0.343, 0.075 | 0.168, 0.057 | 0.891, 0.035 | 0.698, 0.016 | 0.270, 0.049 | 0.065, 0.080 |
| Orthodontic treatment | 0.419, 0.069 | 0.116, 0.064 | 0.386, 0.077 | 0.026, 0.094 | 0.238, 0.053 | 0.523, 0.028 |
| Intubation | 0.489, 0.064 | 0.047, 0.082 | 0.323, 0.082 | 0.169, 0.058 | 0.135, 0.067 | 0.731, 0.015 |
| Orthognathic surgery | 0.011, 0.137 | 0.234, 0.049 | 0.286, 0.086 | 0.858, 0.008 | 0.313, 0.045 | 0.524, 0.028 |
| Wisdom teeth removal | 0.537, 0.060 | 0.115, 0.065 | 0.879, 0.036 | 0.038, 0.088 | 0.824, 0.010 | 0.729, 0.015 |
| Jaw trauma | 0.216, 0.087 | 0.326, 0.040 | 0.179, 0.098 | 0.732, 0.014 | 0.037, 0.093 | 0.201, 0.056 |
| TMJ Pain and Clinical Variables | ||||||
|---|---|---|---|---|---|---|
| Other Comorbidities | TMJ Pain | Limitation of Mouth Opening | Myalgia Degree | TMJ Clicks | TMJ Crepitus | Arthralgia |
| p-Value, Cramer’s V | ||||||
| n (no, 1, ≥2) | 0.002, 0.131 | 0.354, 0.059 | <0.001, 0.185 | 0.125, 0.086 | 0.490, 0.054 | 0.786, 0.030 |
| Group of other Comorbidities | ||||||
| Mental, behavioral, or neurodevelopmental disorders | 0.008, 0.142 | 0.678, 0.017 | <0.001, 0.202 | 0.708, 0.016 | 0.677, 0.019 | 0.645, 0.020 |
| Diseases of the respiratory system | 0.492, 0.064 | 0.475, 0.029 | 0.138, 0.103 | 0.381, 0.037 | 0.236, 0.053 | 0.835, 0.009 |
| Endocrine, nutritional, or metabolic diseases | 0.154, 0.094 | 0.798, 0.011 | 0.195, 0.096 | 0.264, 0.047 | 0.370, 0.040 | 0.487, 0.030 |
| Diseases of the circulatory system | 0.990, 0.014 | 0.679, 0.017 | 0.956, 0.025 | 0.003, 0.125 | 0.066, 0.083 | 0.416, 0.035 |
| Diseases of the musculoskeletal system | 0.228, 0.085 | 0.584, 0.022 | 0.719, 0.051 | 0.979, 0.001 | 0.125, 0.069 | 0.253, 0.050 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ângelo, D.F.; Mota, B.; João, R.S.; Sanz, D.; Cardoso, H.J. Prevalence of Clinical Signs and Symptoms of Temporomandibular Joint Disorders Registered in the EUROTMJ Database: A Prospective Study in a Portuguese Center. J. Clin. Med. 2023, 12, 3553. https://doi.org/10.3390/jcm12103553
Ângelo DF, Mota B, João RS, Sanz D, Cardoso HJ. Prevalence of Clinical Signs and Symptoms of Temporomandibular Joint Disorders Registered in the EUROTMJ Database: A Prospective Study in a Portuguese Center. Journal of Clinical Medicine. 2023; 12(10):3553. https://doi.org/10.3390/jcm12103553
Chicago/Turabian StyleÂngelo, David Faustino, Beatriz Mota, Ricardo São João, David Sanz, and Henrique José Cardoso. 2023. "Prevalence of Clinical Signs and Symptoms of Temporomandibular Joint Disorders Registered in the EUROTMJ Database: A Prospective Study in a Portuguese Center" Journal of Clinical Medicine 12, no. 10: 3553. https://doi.org/10.3390/jcm12103553
APA StyleÂngelo, D. F., Mota, B., João, R. S., Sanz, D., & Cardoso, H. J. (2023). Prevalence of Clinical Signs and Symptoms of Temporomandibular Joint Disorders Registered in the EUROTMJ Database: A Prospective Study in a Portuguese Center. Journal of Clinical Medicine, 12(10), 3553. https://doi.org/10.3390/jcm12103553