
Postoperative Delirium and Cognitive Dysfunction after General and Regional Anesthesia: A Systematic Review and Meta-Analysis

 , , ,
, , ,  and
and
Abstract
1. Introduction
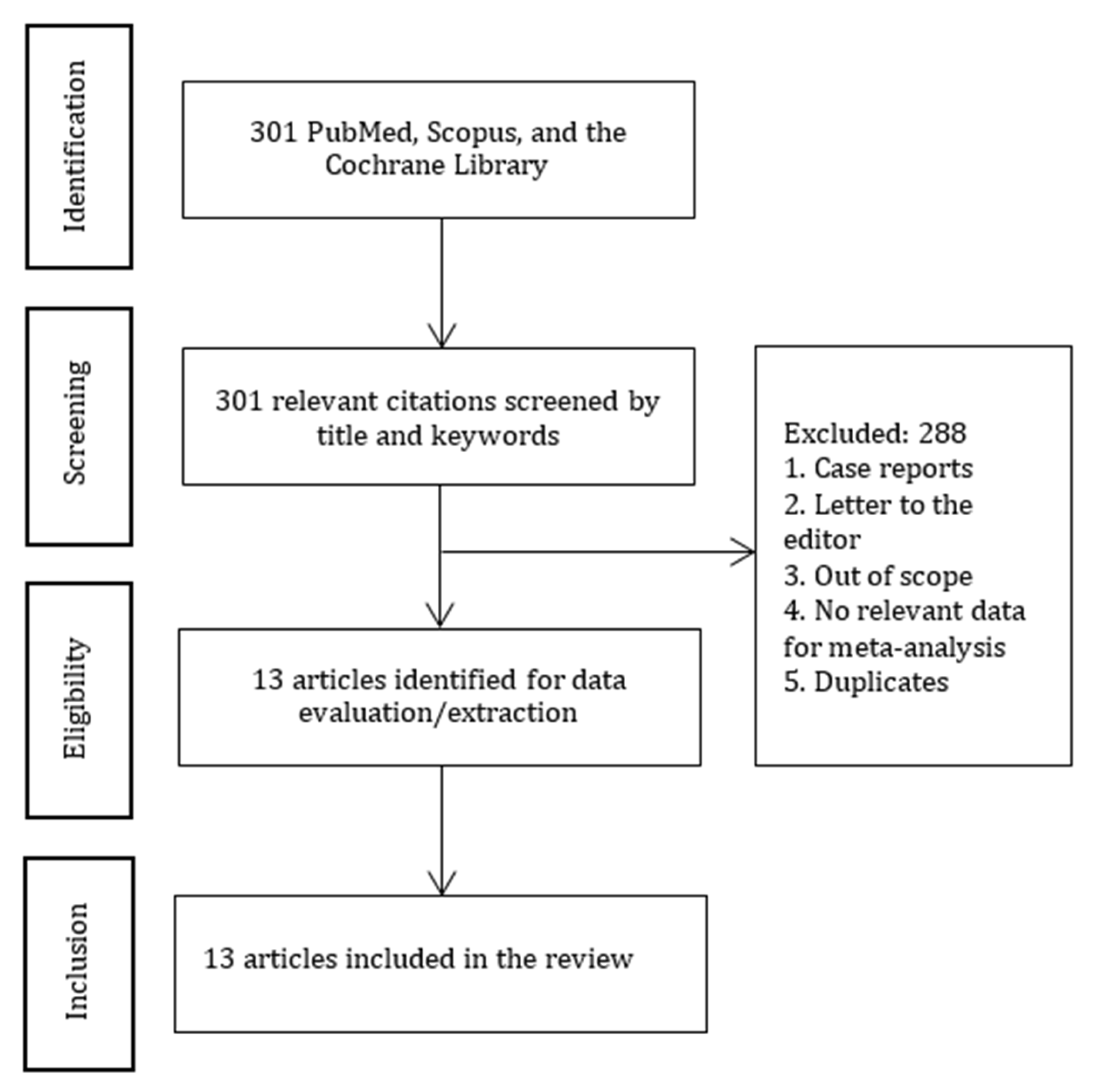
2. Material and Methods
2.1. Protocol
2.2. Participants and Population
2.2.1. Inclusion Criteria
2.2.2. Exclusion Criteria
2.2.3. Outcomes
2.3. Data Extraction and Statistical Methods
2.4. Assessment of Methodological Quality
3. Results
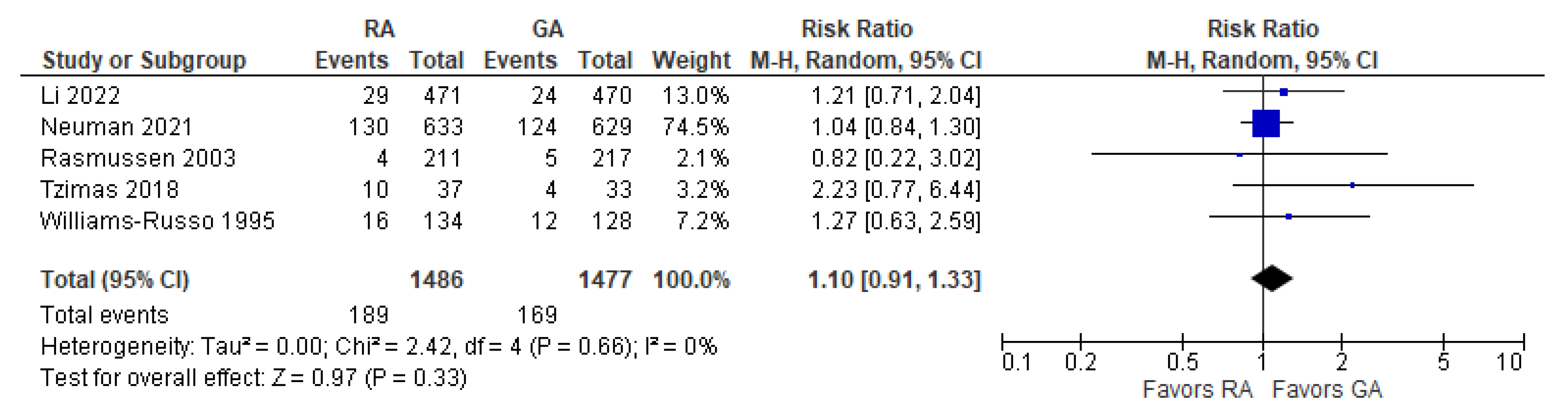
3.1. Incidence of Post-operative Delirium
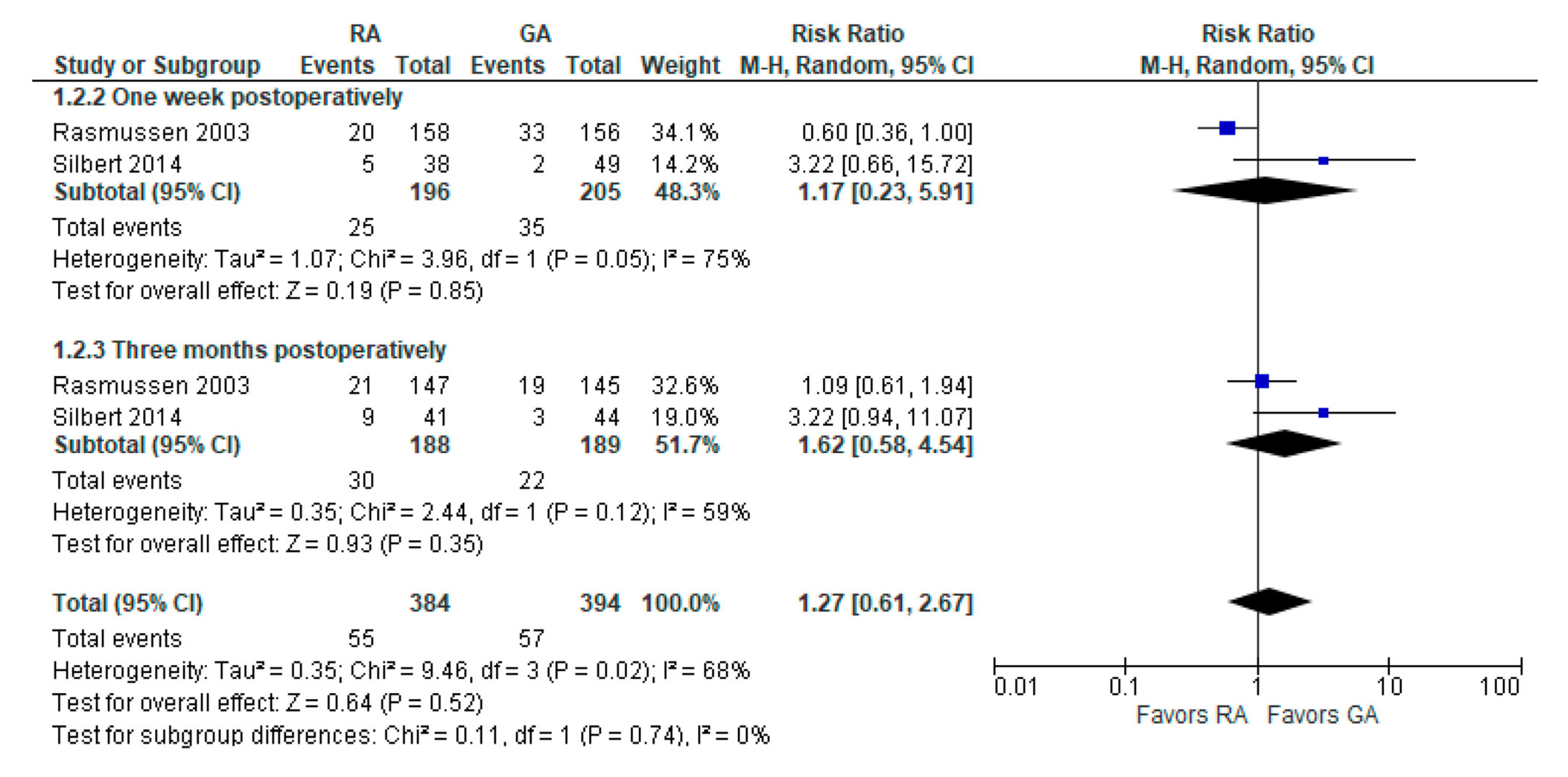
3.2. Incidence of POCD Per-Protocol Analysis
3.3. Psychomotor/Attention Tests (Preoperatively/Baseline)
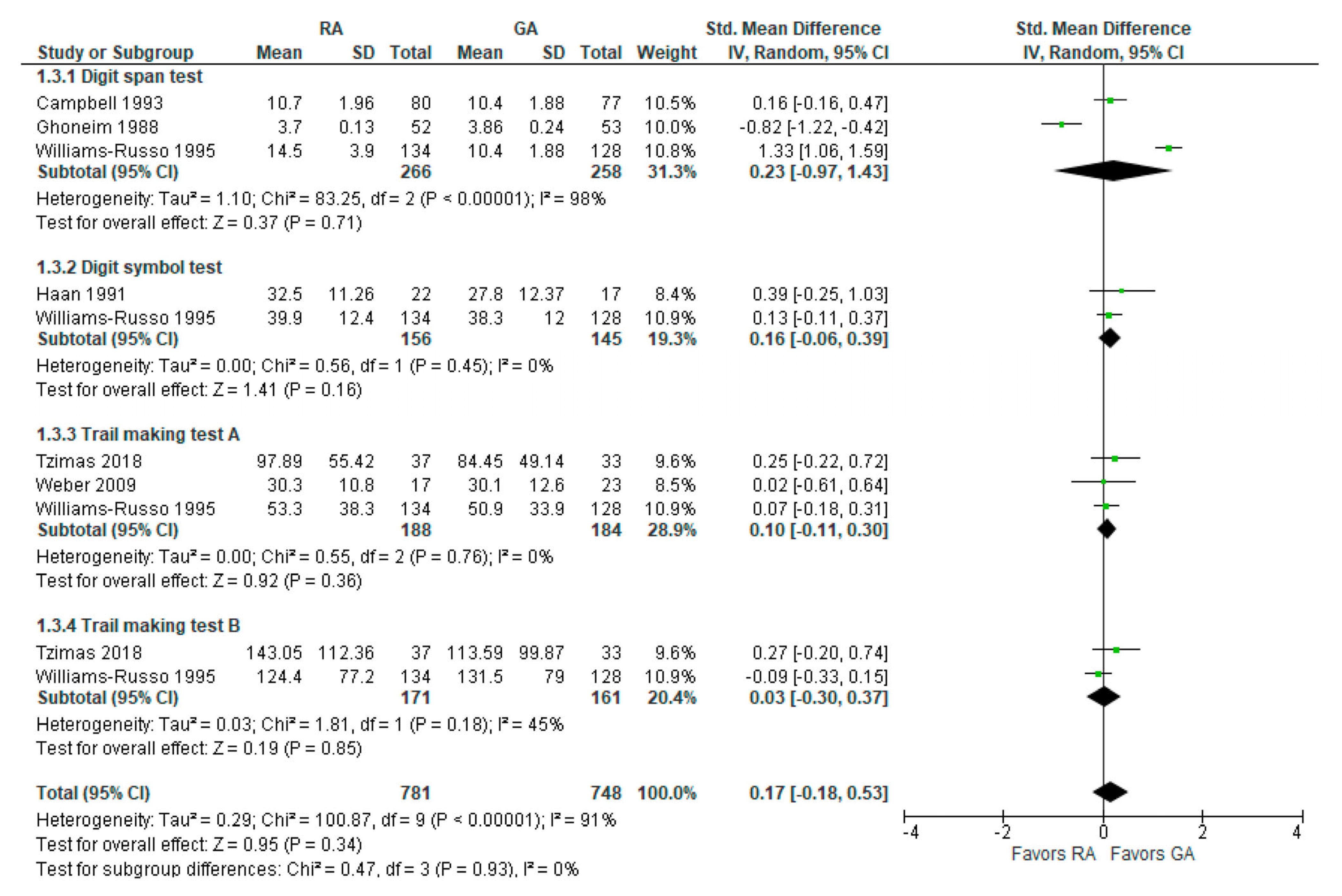
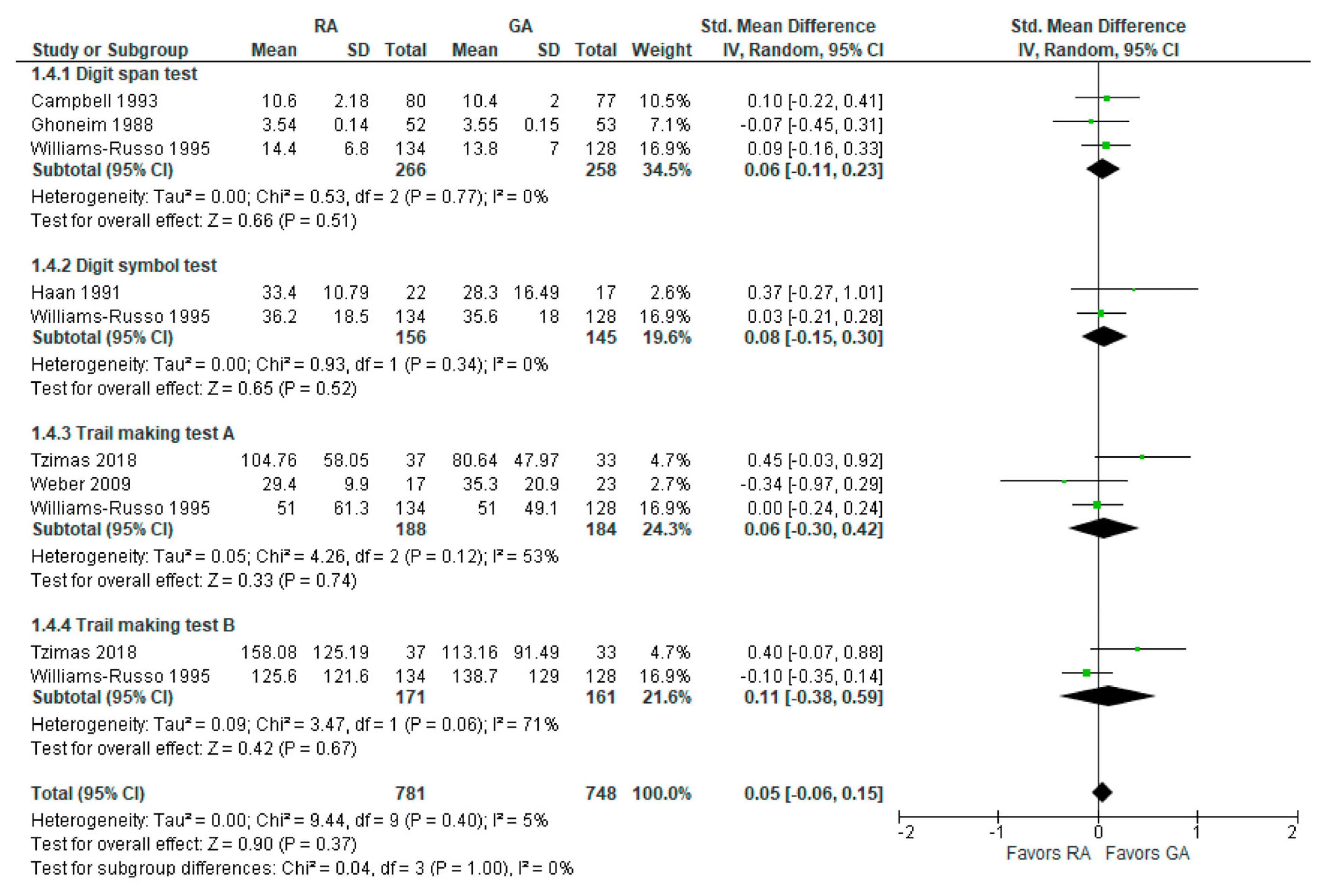
3.4. Psychomotor/Attention Tests (Postoperatively)
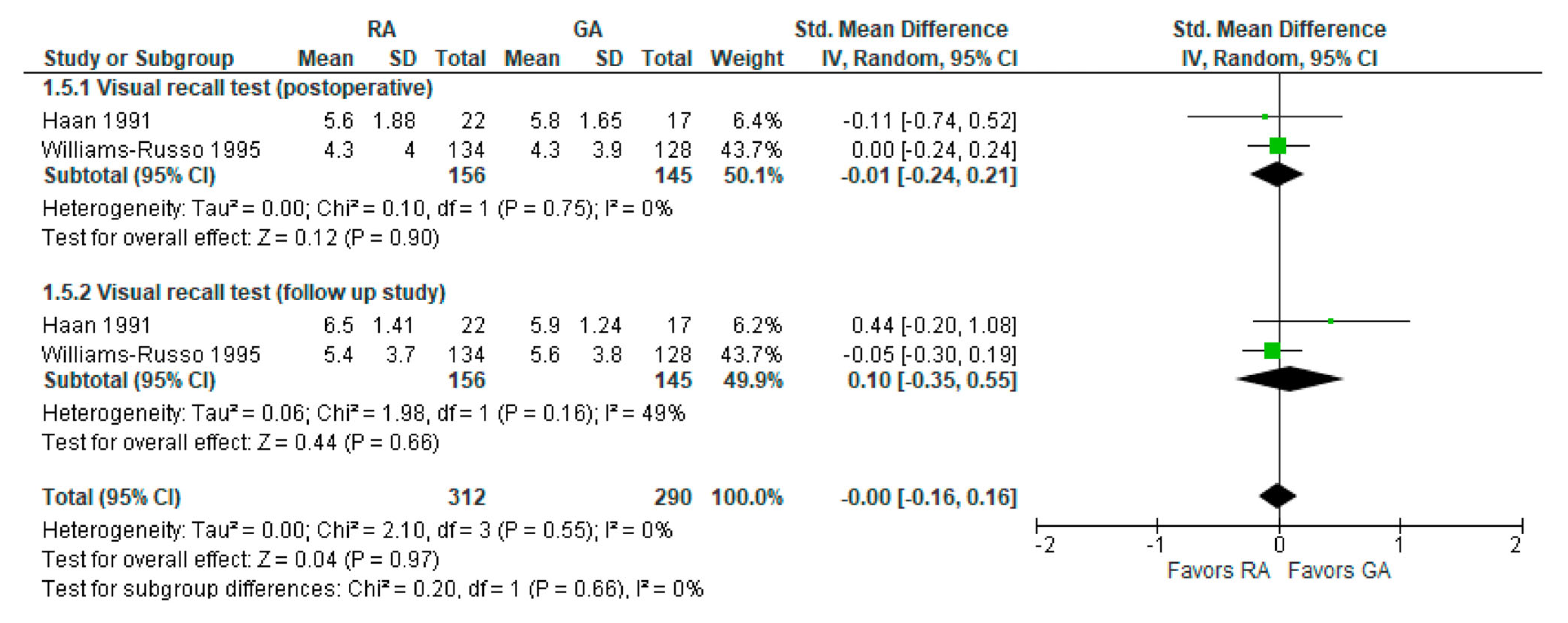
3.5. Visual Recall Test (Memory Test Postoperatively and Follow-up Study)
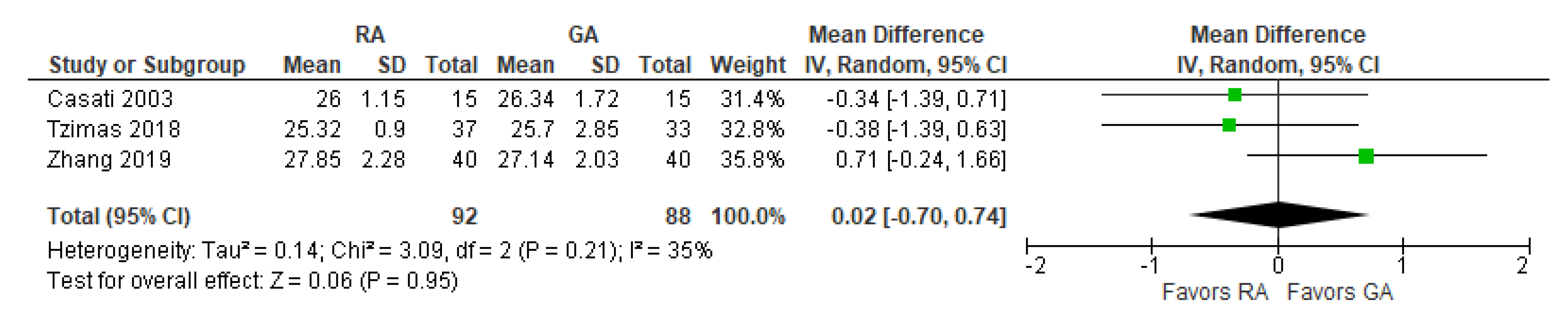
3.6. MMSE Score 24 h Postoperatively
3.7. Reaction Time Three Months Postoperatively (ms)
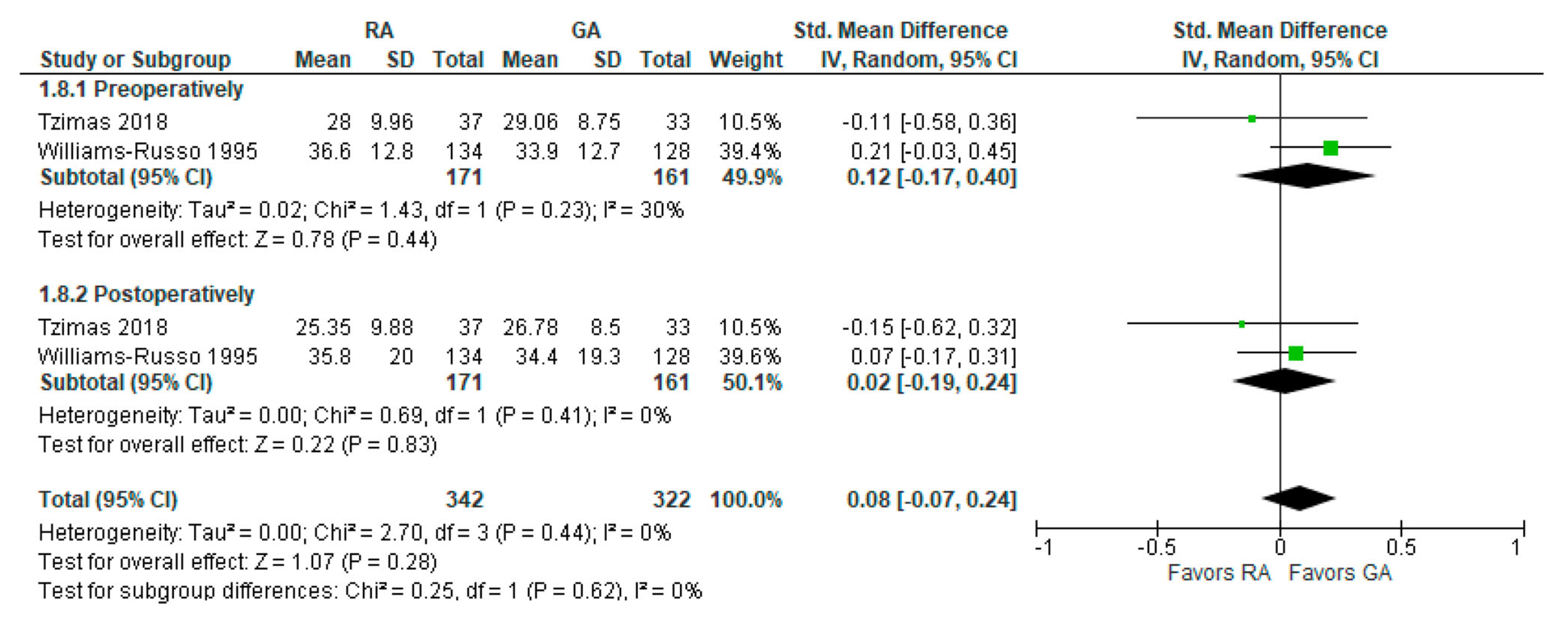
3.8. Controlled Oral Word Association Test
3.9. Digit Copying Test, PO Three Months
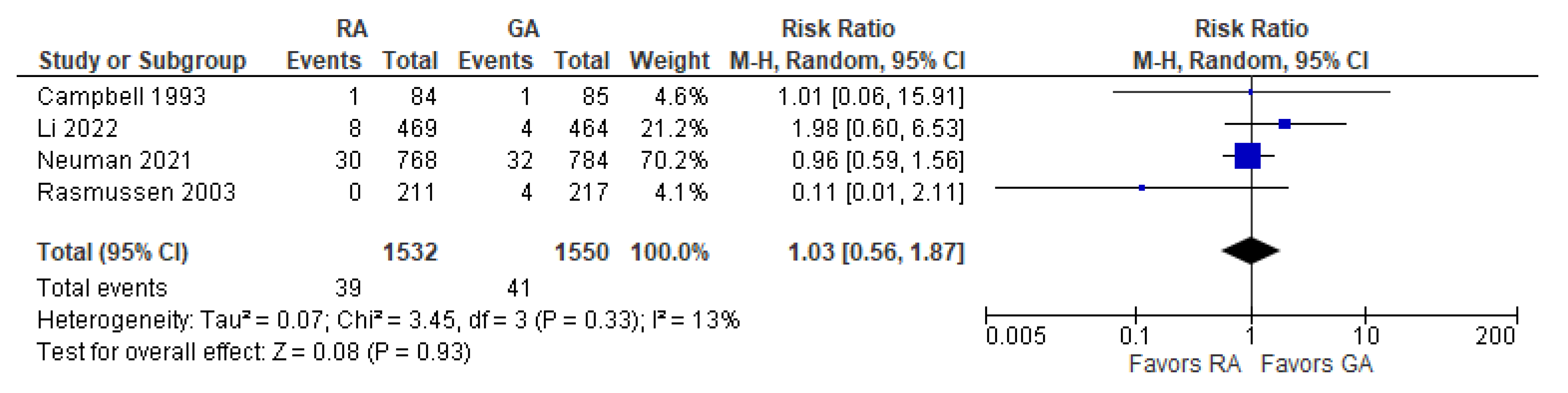
3.10. Post-operative Death
3.11. Assessment of Methodological Quality (and Cochrane Risk of Bias Tool)
Quality Assessment
4. Discussion
- Preoperative factors: advanced age, history of alcoholism, cognitive impairment, neurocognitive disorders (e.g., psychosis, depression, dementia), hypertension, diabetes mellitus, chronic renal failure, anemia, chronic renal failure, electrolyte disorders, anemia, chronic steroid, and antipsychotic agents [29,30,31];
- Intraoperative factors: duration of anesthesia and/or surgery, anesthetic drugs, intraoperative hypoxemia or/or hypotension, blood loss;
- Post-operative risk factors: quality of sleep, the use of sedative agents, and post-operative pain intensity [32].
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Registration
References
- Safavynia, S.A.; Goldstein, P.A. The Role of Neuroinflammation in Postoperative Cognitive Dysfunction: Moving From Hypothesis to Treatment. Front. Psychiatry 2018, 9, 752. [Google Scholar] [CrossRef] [PubMed]
- Rundshagen, I. Postoperative Cognitive Dysfunction. Dtsch. Arztebl. Int. 2014, 111, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Newman, M.F.; Kirchner, J.L.; Phillips-Bute, B.; Gaver, V.; Grocott, H.; Jones, R.H.; Mark, D.B.; Reves, J.G.; Blumenthal, J.A. Longitudinal Assessment of Neurocognitive Function after Coronary-Artery Bypass Surgery. N. Engl. J. Med. 2001, 344, 395–402. [Google Scholar] [CrossRef]
- Moller, J.T.; Cluitmans, P.; Rasmussen, L.S.; Houx, P.; Rasmussen, H.; Canet, J.; Rabbitt, P.; Jolles, J.; Larsen, K.; Hanning, C.D.; et al. Long-Term Postoperative Cognitive Dysfunction in the Elderly ISPOCD1 Study. ISPOCD Investigators. International Study of Post-Operative Cognitive Dysfunction. Lancet 1998, 351, 857–861. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, L.S. Postoperative Cognitive Dysfunction: Incidence and Prevention. Best Pract. Res. Clin. Anaesthesiol. 2006, 20, 315–330. [Google Scholar] [CrossRef]
- Krenk, L.; Rasmussen, L.S.; Kehlet, H. New Insights into the Pathophysiology of Postoperative Cognitive Dysfunction. Acta Anaesthesiol. Scand. 2010, 54, 951–956. [Google Scholar] [CrossRef]
- Posner, M.I.; Petersen, S.E. The Attention System of the Human Brain. Annu. Rev. Neurosci. 1990, 13, 25–42. [Google Scholar] [CrossRef]
- Zhang, H.; Lu, Y.; Liu, M.; Zou, Z.; Wang, L.; Xu, F.-Y.; Shi, X.-Y. Strategies for Prevention of Postoperative Delirium: A Systematic Review and Meta-Analysis of Randomized Trials. Crit. Care 2013, 17, R47. [Google Scholar] [CrossRef]
- Nielson, W.R.; Gelb, A.W.; Casey, J.E.; Penny, F.J.; Merchant, R.N.; Manninen, P.H. Long-Term Cognitive and Social Sequelae of General versus Regional Anesthesia during Arthroplasty in the Elderly. Anesthesiology 1990, 73, 1103–1109. [Google Scholar] [CrossRef]
- Rasmussen, L.S.; Johnson, T.; Kuipers, H.M.; Kristensen, D.; Siersma, V.D.; Vila, P.; Jolles, J.; Papaioannou, A.; Abildstrom, H.; Silverstein, J.H.; et al. Does Anaesthesia Cause Postoperative Cognitive Dysfunction? A Randomised Study of Regional versus General Anaesthesia in 438 Elderly Patients. Acta Anaesthesiol. Scand. 2003, 47, 260–266. [Google Scholar] [CrossRef]
- Kukreja, D.; Günther, U.; Popp, J. Delirium in the Elderly: Current Problems with Increasing Geriatric Age. Indian J. Med. Res. 2015, 142, 655–662. [Google Scholar] [CrossRef] [PubMed]
- Michaud, L.; Stiefel, F.A.; Caraceni, L. Grassi: Delirium—Acute Confusional States in Palliative Medicine. Support. Care Cancer 2003, 11, 745. [Google Scholar] [CrossRef]
- Viderman, D.; Brotfain, E.; Bilotta, F.; Zhumadilov, A. Risk Factors and Mechanisms of Postoperative Delirium after Intracranial Neurosurgical Procedures. Asian J. Anesthesiol. 2020, 58, 5–13. [Google Scholar] [CrossRef]
- Kat, M.G.; Vreeswijk, R.; de Jonghe, J.F.M.; van der Ploeg, T.; van Gool, W.A.; Eikelenboom, P.; Kalisvaart, K.J. Long-Term Cognitive Outcome of Delirium in Elderly Hip Surgery Patients. A Prospective Matched Controlled Study over Two and a Half Years. Dement. Geriatr. Cogn. Disord. 2008, 26, 1–8. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Campbell, D.N.; Lim, M.; Muir, M.K.; O’Sullivan, G.; Falcon, M.; Fison, P.; Woods, R. A Prospective Randomised Study of Local versus General Anaesthesia for Cataract Surgery. Anaesthesia 1993, 48, 422–428. [Google Scholar] [CrossRef]
- Casati, A.; Aldegheri, G.; Vinciguerra, E.; Marsan, A.; Fraschini, G.; Torri, G. Randomized Comparison between Sevoflurane Anaesthesia and Unilateral Spinal Anaesthesia in Elderly Patients Undergoing Orthopaedic Surgery. Eur. J. Anaesthesiol. 2003, 20, 640–646. [Google Scholar] [CrossRef]
- Ghoneim, M.M.; Hinrichs, J.V.; O’Hara, M.W.; Mehta, M.P.; Pathak, D.; Kumar, V.; Clark, C.R. Comparison of Psychologic and Cognitive Functions after General or Regional Anesthesia. Anesthesiology 1988, 69, 507–515. [Google Scholar] [CrossRef]
- Haan, J.; van Kleef, J.W.; Bloem, B.R.; Zwartendijk, J.; Lanser, J.B.; Brand, R.; van der Does, I.G.; Krul, E.J.; Elshove, H.M.; Moll, A.C. Cognitive Function after Spinal or General Anesthesia for Transurethral Prostatectomy in Elderly Men. J. Am. Geriatr. Soc. 1991, 39, 596–600. [Google Scholar] [CrossRef]
- Jones, M.J.; Piggott, S.E.; Vaughan, R.S.; Bayer, A.J.; Newcombe, R.G.; Twining, T.C.; Pathy, J.; Rosen, M. Cognitive and Functional Competence after Anaesthesia in Patients Aged over 60: Controlled Trial of General and Regional Anaesthesia for Elective Hip or Knee Replacement. BMJ 1990, 300, 1683–1687. [Google Scholar] [CrossRef]
- Li, T.; Li, J.; Yuan, L.; Wu, J.; Jiang, C.; Daniels, J.; Mehta, R.L.; Wang, M.; Yeung, J.; Jackson, T.; et al. Effect of Regional vs General Anesthesia on Incidence of Postoperative Delirium in Older Patients Undergoing Hip Fracture Surgery: The RAGA Randomized Trial. JAMA 2022, 327, 50. [Google Scholar] [CrossRef] [PubMed]
- Neuman, M.D.; Feng, R.; Carson, J.L.; Gaskins, L.J.; Dillane, D.; Sessler, D.I.; Sieber, F.; Magaziner, J.; Marcantonio, E.R.; Mehta, S.; et al. Spinal Anesthesia or General Anesthesia for Hip Surgery in Older Adults. N. Engl. J. Med. 2021, 385, 2025–2035. [Google Scholar] [CrossRef] [PubMed]
- Silbert, B.S.; Evered, L.A.; Scott, D.A. Incidence of Postoperative Cognitive Dysfunction after General or Spinal Anaesthesia for Extracorporeal Shock Wave Lithotripsy. Br. J. Anaesth. 2014, 113, 784–791. [Google Scholar] [CrossRef] [PubMed]
- Tzimas, P.; Samara, E.; Petrou, A.; Korompilias, A.; Chalkias, A.; Papadopoulos, G. The Influence of Anesthetic Techniques on Postoperative Cognitive Function in Elderly Patients Undergoing Hip Fracture Surgery: General vs Spinal Anesthesia. Injury 2018, 49, 2221–2226. [Google Scholar] [CrossRef]
- Weber, C.F.; Friedl, H.; Hueppe, M.; Hintereder, G.; Schmitz-Rixen, T.; Zwissler, B.; Meininger, D. Impact of General versus Local Anesthesia on Early Postoperative Cognitive Dysfunction Following Carotid Endarterectomy: GALA Study Subgroup Analysis. World J. Surg. 2009, 33, 1526–1532. [Google Scholar] [CrossRef]
- Williams-Russo, P.; Sharrock, N.E.; Mattis, S.; Szatrowski, T.P.; Charlson, M.E. Cognitive Effects after Epidural vs General Anesthesia in Older Adults. A Randomized Trial. JAMA 1995, 274, 44–50. [Google Scholar] [CrossRef]
- Zhang, X.; Dong, Q.; Fang, J. Impacts of General and Spinal Anaesthesia on Short-Term Cognitive Function and Mental Status in Elderly Patients Undergoing Orthopaedic Surgery. J. Coll. Physicians Surg—Pak. JCPSP 2019, 29, 101–104. [Google Scholar] [CrossRef]
- Jevtovic-Todorovic, V.; Absalom, A.R.; Blomgren, K.; Brambrink, A.; Crosby, G.; Culley, D.J.; Fiskum, G.; Giffard, R.G.; Herold, K.F.; Loepke, A.W.; et al. Anaesthetic Neurotoxicity and Neuroplasticity: An Expert Group Report and Statement Based on the BJA Salzburg Seminar. Br. J. Anaesth. 2013, 111, 143–151. [Google Scholar] [CrossRef]
- Robinson, T.N.; Raeburn, C.D.; Tran, Z.V.; Angles, E.M.; Brenner, L.A.; Moss, M. Postoperative Delirium in the Elderly: Risk Factors and Outcomes. Ann. Surg. 2009, 249, 173–178. [Google Scholar] [CrossRef]
- Yang, F.M.; Marcantonio, E.R.; Inouye, S.K.; Kiely, D.K.; Rudolph, J.L.; Fearing, M.A.; Jones, R.N. Phenomenological Subtypes of Delirium in Older Persons: Patterns, Prevalence, and Prognosis. Psychosomatics 2009, 50, 248–254. [Google Scholar] [CrossRef]
- Echigoya, Y.; Kato, H. Causes of postoperative delirium after abdominal surgery in elderly patients. Masui. Jpn. J. Anesthesiol. 2007, 56, 932–936. [Google Scholar]
- Vaurio, L.E.; Sands, L.P.; Wang, Y.; Mullen, E.A.; Leung, J.M. Postoperative Delirium: The Importance of Pain and Pain Management. Anesth. Analg. 2006, 102, 1267. [Google Scholar] [CrossRef] [PubMed]
- Boyko, Y.; Ording, H.; Jennum, P. Sleep Disturbances in Critically Ill Patients in ICU: How Much Do We Know? Acta Anaesthesiol. Scand. 2012, 56, 950–958. [Google Scholar] [CrossRef] [PubMed]
- Avidan, M.S.; Evers, A.S. The Fallacy of Persistent Postoperative Cognitive Decline. Anesthesiology 2016, 124, 255–258. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | D1 | D2 | D3 | D4 | D5 | Overall | ||
|---|---|---|---|---|---|---|---|---|
| Zhang et al., 2019 [27] |  |  |  | | |  | | Low risk |
| Tzimas et al., 2018 [24] | | | | | |  | | Some concerns |
| Silbert et al., 2014 [23] | | | | | |  | | High risk |
| Rasmussen et al., 2003 [10] | | | | | | | D1 | Randomization process |
| Williams-Russo et al., 1995 [26] | | | | | | | D2 | Deviations from the intended interventions |
| Campbell et al., 1993 [16] | | | | | | | D3 | Missing outcome data |
| Haan et al., 1991 [19] | | | | | | | D4 | Measurement of the outcome |
| Jones et al., 1990 [20] | | | | | | | D5 | Selection of the reported result |
| Ghoneim et al., 1988 [18] | | | | | | | ||
| Weber et al., 2009 [25] | | | | | | | ||
| Casati et al., 2003 [17] | | | | | | | ||
| Neuman et al., 2021 [22] | | | | | | | ||
| Li et al., 2022 [21] | | | | | | |
| Outcomes | Standardized Mean Difference [95% CI] | Number of Patients (Studies) | Certainty of the Evidence (GRADE) |
|---|---|---|---|
| Incidence of PO delirium | 1.10 [0.91, 1.33] | 2963 (5) | ⊕⊕⊕◯ Moderate a |
| Incidence of POCD | 1.14 [0.60, 2.13] | 885 (2) | ⊕⊕⊕◯ Moderate a |
| Death | 1.03 [0.56, 1.87] | 3082 (4) | ⊕⊕⊕⊕ High |
| Psychomotor/attention tests PO | 0.05 [−0.06, 0.15] | 1529 (6) | ⊕⊕⊕⊕ High |
| Visual recall (PO and follow-up) | 0.00 [−0.16, 0.16] | 602 (2) | ⊕⊕⊕⊕ High |
| Controlled oral word association test | 0.08 [−0.07, 0.24] | 664 (2) | ⊕⊕⊕⊕ High |
| MMSE 24 h | 0.02 [−0.70, 0.74] | 180 (3) | ⊕⊕◯◯ Low |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Viderman, D.; Nabidollayeva, F.; Aubakirova, M.; Yessimova, D.; Badenes, R.; Abdildin, Y. Postoperative Delirium and Cognitive Dysfunction after General and Regional Anesthesia: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 3549. https://doi.org/10.3390/jcm12103549
Viderman D, Nabidollayeva F, Aubakirova M, Yessimova D, Badenes R, Abdildin Y. Postoperative Delirium and Cognitive Dysfunction after General and Regional Anesthesia: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2023; 12(10):3549. https://doi.org/10.3390/jcm12103549
Chicago/Turabian StyleViderman, Dmitriy, Fatima Nabidollayeva, Mina Aubakirova, Dinara Yessimova, Rafael Badenes, and Yerkin Abdildin. 2023. "Postoperative Delirium and Cognitive Dysfunction after General and Regional Anesthesia: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 12, no. 10: 3549. https://doi.org/10.3390/jcm12103549
APA StyleViderman, D., Nabidollayeva, F., Aubakirova, M., Yessimova, D., Badenes, R., & Abdildin, Y. (2023). Postoperative Delirium and Cognitive Dysfunction after General and Regional Anesthesia: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 12(10), 3549. https://doi.org/10.3390/jcm12103549