
Central Retinal Artery Occlusion Is Related to Vascular Endothelial Injury and Left Ventricular Diastolic Dysfunction


 , ,
, , 

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Laboratory Analysis
2.3. Ultrasound Examinations
2.4. Flow-Mediated Dilatation of the Brachial Artery (FMD)
2.5. Intima-Media Thickness (IMT) of the Common Carotid Artery
2.6. Transthoracic Echocardiogram
2.7. Statistics
3. Results
3.1. Characteristics of Patients and Controls
3.2. Ophthalmic Examination
3.3. Basic Laboratory Tests
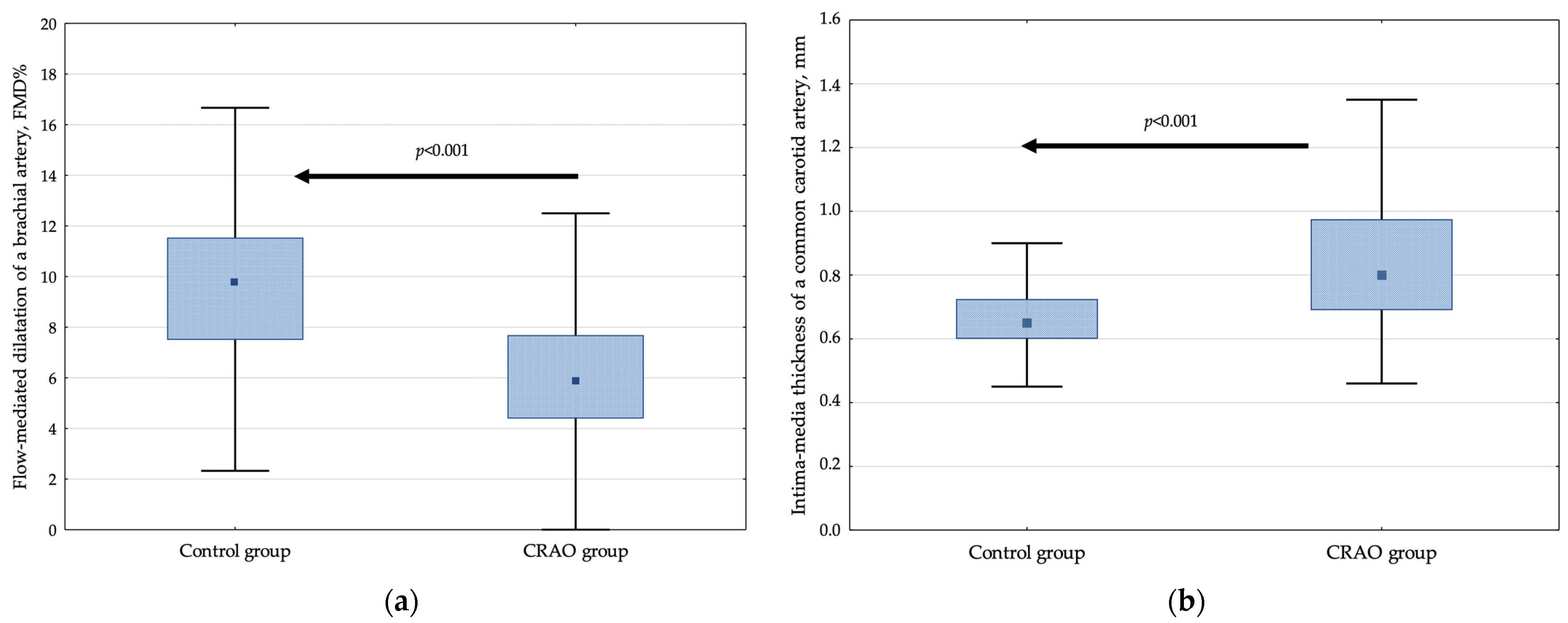
3.4. Flow-Mediated Dilatation of the Brachial Artery (FMD) and Intima-Media Thickness of the Common Carotid Artery (IMT)
3.5. Basic Transthoracic Echocardiographic Parameters
3.6. Associations of the Flow-Mediated Dilatation of the Brachial Artery (FMD) and Intima-Media Thickness of the Common Carotid Artery (IMT) with Basic Transthoracic Echocardiographic Parameters
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hayreh, S.S. Central retinal artery occlusion. Indian J. Ophthalmol. 2018, 66, 1684. [Google Scholar] [CrossRef]
- Leavitt, J.A.; Larson, T.A.; Hodge, D.O.; Gullerud, R.E. The incidence of central retinal artery occlusion in Olmsted County, Minnesota. Am. J. Ophthalmol. 2011, 152, 820–823.e2. [Google Scholar] [CrossRef]
- Park, S.J.; Choi, N.K.; Seo, K.H.; Park, K.H.; Woo, S.J. Nationwide incidence of clinically diagnosed central retinal artery occlusion in Korea, 2008 to 2011. Ophthalmology 2014, 121, 1933–1938. [Google Scholar] [CrossRef]
- Dattilo, M.; Biousse, V.; Newman, N.J. Update on the Management of Central Retinal Artery Occlusion. Neurol. Clin. 2017, 35, 83–100. [Google Scholar] [CrossRef]
- Chronopoulos, A.; Schutz, J.S. Central retinal artery occlusion—A new, provisional treatment approach. Surv. Ophthalmol. 2019, 64, 443–451. [Google Scholar] [CrossRef]
- Fallico, M.; Lotery, A.J.; Longo, A.; Avitabile, T.; Bonfiglio, V.; Russo, A.; Murabito, P.; Palmucci, S.; Pulvirenti, A.; Reibaldi, M. Risk of acute stroke in patients with retinal artery occlusion: A systematic review and meta-analysis. Eye 2020, 34, 683–689. [Google Scholar] [CrossRef]
- Shaikh, I.S.; Elsamna, S.T.; Zarbin, M.A.; Bhagat, N. Assessing the risk of stroke development following retinal artery occlusion. J. Stroke Cerebrovasc. Dis. 2020, 29, 105002. [Google Scholar] [CrossRef]
- Kim, Y.D.; Kim, Y.K.; Yoon, Y.E.; Yoon, C.H.; Park, K.H.; Woo, S.J. Association of Retinal Artery Occlusion with Subclinical Coronary Artery Disease. J. Korean Med. Sci. 2019, 34, e286. [Google Scholar] [CrossRef]
- Mac Grory, B.; Landman, S.R.; Ziegler, P.D.; Boisvert, C.J.; Flood, S.P.; Stretz, C.; Madsen, T.E.; Reznik, M.E.; Cutting, S.; Moore, E.E.; et al. Detection of Atrial Fibrillation After Central Retinal Artery Occlusion. Stroke 2021, 9, 2773–2781. [Google Scholar] [CrossRef]
- Callizo, J.; Feltgen, N.; Pantenburg, S.; Wolf, A.; Neubauer, A.S.; Jurklies, B.; Wachter, R.; Schmoor, C.; Schumacher, M.; Junker, B.; et al. Cardiovascular Risk Factors in Central Retinal Artery Occlusion: Results of a Prospective and Standardized Medical Examination. Ophthalmology 2015, 9, 1881–1888. [Google Scholar] [CrossRef]
- Woo, S.C.; Lip, G.Y.; Lip, P.L. Associations of retinal artery occlusion and retinal vein occlusion to mortality, stroke, and myocardial infarction: A systematic review. Eye 2016, 30, 1031–1038. [Google Scholar] [CrossRef]
- Lavin, P.; Patrylo, M.; Hollar, M.; Espaillat, K.B.; Kirshner, H.; Schrag, M. Stroke Risk and Risk Factors in Patients with Central Retinal Artery Occlusion. Am. J. Ophthalmol. 2018, 196, 96–100. [Google Scholar] [CrossRef]
- Mac Grory, B.; Schrag, M.; Biousse, V.; Furie, K.L.; Gerhard-Herman, M.; Lavin, P.J.; Sobrin, L.; Tjoumakaris, S.I.; Weyand, C.M.; Yaghi, S.; et al. Management of Central Retinal Artery Occlusion: A Scientific Statement from the American Heart Association. Stroke 2021, 52, e282–e294. [Google Scholar] [CrossRef]
- Hayreh, S.S.; Zimmerman, M.B.; Kimura, A.; Sanon, A. Central retinal artery occlusion. Retinal survival time. Exp. Eye Res. 2004, 78, 723–736. [Google Scholar] [CrossRef]
- Ochakovski, G.A.; Wenzel, D.A.; Spitzer, M.S.; Poli, S.; Härtig, F.; Fischer, M.D.; Dimopoulos, S.; Schultheiss, M. Retinal oedema in central retinal artery occlusion develops as a function of time. Acta Ophthalmol. 2020, 98, e680–e684. [Google Scholar] [CrossRef]
- Kramer, M.; Goldenberg-Cohen, N.; Axer-Siegel, R.; Weinberger, D.; Cohen, Y.; Monselise, Y. Inflammatory reaction in acute retinal artery occlusion: Cytokine levels in aqueous humor and serum. Ocul. Immunol. Inflamm. 2005, 13, 305–310. [Google Scholar] [CrossRef]
- Weger, M.; Steinbrugger, I.; Haas, A.; März, W.; El-Shabrawi, Y.; Weger, W.; Schmut, O.; Renner, W. Role of the interleukin-6-174 G>C gene polymorphism in retinal artery occlusion. Stroke 2005, 36, 249–252. [Google Scholar] [CrossRef]
- Weger, M.; Steinbrugger, I.; El-Shabrawi, Y.; Wegscheider, B.J.; Weger, W.; Renner, W.; Schmut, O.; Haas, A. Haplotype-tagging interleukin-10 promoter polymorphism is associated with reduced risk of retinal artery occlusion. Mol. Vis. 2007, 13, 549–552. [Google Scholar] [PubMed]
- Rudkin, A.K.; Lee, A.W.; Chen, C.S. Vascular risk factors for central retinal artery occlusion. Eye 2010, 24, 678–681. [Google Scholar] [CrossRef]
- Widlansky, M.E.; Gokce, N.; Keaney, J.F., Jr.; Vita, J.A. The clinical implications of endothelial dysfunction. J. Am. Coll. Cardiol. 2003, 42, 1149–1160. [Google Scholar] [CrossRef]
- Grover-Páez, F.; Zavalza-Gómez, A.B. Endothelial dysfunction and cardiovascular risk factors. Diabetes Res. Clin. Pract. 2009, 84, 1–10. [Google Scholar] [CrossRef]
- Rajendran, P.; Rengarajan, T.; Thangavel, J.; Nishigaki, Y.; Sakthisekaran, D.; Sethi, G.; Nishigaki, I. The vascular endothelium and human diseases. Int. J. Biol. Sci. 2013, 9, 1057–1069. [Google Scholar] [CrossRef]
- Chia, P.Y.; Teo, A.; Yeo, T.W. Overview of the Assessment of Endothelial Function in Humans. Front. Med. 2020, 7, 542567. [Google Scholar] [CrossRef]
- Corretti, M.C.; Anderson, T.J.; Benjamin, E.J.; Celermajer, D.; Charbonneau, F.; Creager, M.A.; Deanfield, J.; Drexler, H.; Gerhard-Herman, M.; Herrington, D.; et al. International Brachial Artery Reactivity Task Force. Guidelines for the ultrasound assessment of endothelial-dependent flow-mediated vasodilation of the brachial artery: A report of the International Brachial Artery Reactivity Task Force. J. Am. Coll. Cardiol. 2002, 39, 257–265. [Google Scholar] [CrossRef]
- Stein, J.H.; Korcarz, C.E.; Hurst, R.T.; Lonn, E.; Kendall, C.B.; Mohler, E.R.; Najjar, S.S.; Rembold, C.M.; Post, W.S. American Society of Echocardiography Carotid Intima-Media Thickness Task Force. Use of carotid ultrasound to identify subclinical vascular disease and evaluate cardiovascular disease risk: A consensus statement from the American Society of Echocardiography Carotid Intima-Media Thickness Task Force. Endorsed by the Society for Vascular Medicine. J. Am. Soc. Echocardiogr. 2008, 21, 93–111. [Google Scholar] [CrossRef]
- Hillis, G.S.; Bloomfield, P. Basic transthoracic echocardiography. BMJ 2005, 330, 1432–1436. [Google Scholar] [CrossRef]
- Su, W.W.; Cheng, S.T.; Ho, W.J.; Tsay, P.K.; Wu, S.C.; Chang, S.H. Glaucoma is associated with peripheral vascular endothelial dysfunction. Ophthalmology 2008, 115, 1173–1178.e1. [Google Scholar] [CrossRef]
- Malecki, M.T.; Osmenda, G.; Walus-Miarka, M.; Skupien, J.; Cyganek, K.; Mirkiewicz-Sieradzka, B.; Damek-Guzik, T.A.; Guzik, T.J.; Sieradzki, J. Retinopathy in type 2 diabetes mellitus is associated with increased intima-media thickness and endothelial dysfunction. Eur. J. Clin. Investig. 2008, 38, 925–930. [Google Scholar] [CrossRef]
- Baltu, F.; Sarici, A.M.; Yildirim, O.; Mergen, B.; Bolat, E. Investigation of vascular endothelial dysfunction in the patients with age-related macular degeneration. Cutan. Ocul. Toxicol. 2019, 38, 29–35. [Google Scholar] [CrossRef]
- Hayreh, S.S.; Zimmerman, M.B. Central retinal artery occlusion: Visual outcome. Am. J. Ophthalmol. 2005, 140, 376–391. [Google Scholar] [CrossRef]
- Harris, R.A.; Nishiyama, S.K.; Wray, D.W.; Richardson, R.S. Ultrasound assessment of flow-mediated dilation. Hypertension 2010, 55, 1075–1085. [Google Scholar] [CrossRef]
- Tanano, I.; Nagaoka, T.; Sogawa, K.; Tani, T.; Omae, T.; Nakabayashi, S.; Ishibazawa, A.; Yoshida, A. Impaired systemic vascular endothelial function in patients with branch retinal vein occlusion. Curr. Eye Res. 2013, 38, 114–118. [Google Scholar] [CrossRef]
- Gouliopoulos, N.; Siasos, G.; Moschos, M.M.; Oikonomou, E.; Rouvas, A.; Bletsa, E.; Stampouloglou, P.; Siasou, G.; Paraskevopoulos, T.; Vlasis, K.; et al. Endothelial dysfunction and impaired arterial wall properties in patients with retinal vein occlusion. Vasc. Med. 2020, 25, 302–308. [Google Scholar] [CrossRef]
- Pacholczak-Madej, R.; Kuszmiersz, P.; Iwaniec, T.; Zaręba, L.; Zarychta, J.; Walocha, J.A.; Dropiński, J.; Bazan-Socha, S. Endothelial Dysfunction and Pentraxin-3 in Clinically Stable Adult Asthma Patients. J. Investig. Allergol. Clin. Immunol. 2021, 31, 417–425. [Google Scholar] [CrossRef]
- Ergül, E.; Yılmaz, A.S.; Öğütveren, M.M.; Emlek, N.; Kostakoğlu, U.; Çetin, M. COVID-19 disease independently predicted endothelial dysfunction measured by flow-mediated dilatation. Int. J. Cardiovasc. Imaging 2021, 38, 25–32. [Google Scholar] [CrossRef]
- Gimbrone, M.A., Jr.; García-Cardeña, G. Endothelial Cell Dysfunction and the Pathobiology of Atherosclerosis. Circ. Res. 2016, 118, 620–636. [Google Scholar] [CrossRef]
- Dropiński, J.; Szczeklik, W.; Wegrzyn, W. Increased carotid artery intima-media thickness as an indicator of the onset of atherosclerosis in patients with connective tissue systemic diseases. Kardiol. Pol. 2003, 59, 475–483. [Google Scholar] [PubMed]
- Smrzova, A.; Horak, P.; Skacelova, M.; Hermanova, Z.; Langova, K.; Zadrazil, J.; Novotny, D. Intima media thickness measurement as a marker of subclinical atherosclerosis in SLE patient. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc. Czech Repub. 2014, 158, 404–411. [Google Scholar] [CrossRef]
- Goldenberg-Cohen, N.; Cohen, Y.; Monselise, Y.; Eldar, I.; Axer-Siegel, R.; Weinberger, D.; Kramer, M. C-reactive protein levels do not correlate with retinal artery occlusion but with atherosclerosis. Eye 2009, 23, 785–790. [Google Scholar] [CrossRef]
- Huang, X.; Yang, Y.; Duan, Y.; Kuang, Y.Q.; Lin, D. Homocysteine in retinal artery occlusive disease: A meta-analysis of cohort studies. Sci. Rep. 2017, 7, 15708. [Google Scholar] [CrossRef]
- Marin-Sanabria, E.A.; Kondoh, T.; Yamanaka, A.; Kohmura, E. Ultrasonographic screening of carotid artery in patients with vascular retinopathies. Kobe J. Med. Sci. 2005, 51, 7–16. [Google Scholar] [PubMed]
- Song, Y.J.; Cho, K.I.; Kim, S.M.; Jang, H.D.; Park, J.M.; Kim, S.S.; Kim, D.J.; Lee, H.G.; Kim, T.I. The predictive value of retinal vascular findings for carotid artery atherosclerosis: Are further recommendations with regard to carotid atherosclerosis screening needed? Heart Vessel 2013, 28, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Hodis, H.N.; Mack, W.J.; LaBree, L.; Selzer, R.H.; Liu, C.; Liu, C.; Alaupovic, P.; Kwong-Fu, H.; Azen, S.P. Reduction in carotid arterial wall thickness using lovastatin and dietary therapy: A randomized controlled clinical trial. Ann. Intern. Med. 1996, 124, 548–556. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.; Kang, S.W.; Choi, K.J.; Son, K.Y.; Lim, D.H.; Shin, D.W.; Kim, K.; Kim, S.J. High-density Lipoprotein Cholesterol and the Risk of Future Retinal Artery Occlusion Development: A Nationwide Cohort Study. Am. J. Ophthalmol. 2022, 235, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Chien, C.-C.; Chen, P.-H.; Chung, C.-H.; Sun, C.-A.; Chien, W.-C.; Chien, K.-H. Association between Statins and Retinal Vascular Occlusion: A Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2021, 18, 9864. [Google Scholar] [CrossRef]
- Kim, S.M.; Cho, K.I. Impact of cilostazol on the progression of carotid atherosclerosis in patients with retinal vascular occlusion. Cardiovasc. Ther. 2013, 31, e94–e101. [Google Scholar] [CrossRef]
- Lan, N.S.H.; Massam, B.D.; Kulkarni, S.S.; Lang, C.C. Pulmonary Arterial Hypertension: Pathophysiology and Treatment. Diseases 2018, 6, 38. [Google Scholar] [CrossRef]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F., 3rd; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef]
- Paulus, W.J.; Tschöpe, C. A novel paradigm for heart failure with preserved ejection fraction: Comorbidities drive myocardial dysfunction and remodeling through coronary microvascular endothelial inflammation. J. Am. Coll. Cardiol. 2013, 62, 263–271. [Google Scholar] [CrossRef]
- Kai, H.; Kuwahara, F.; Tokuda, K.; Imaizumi, T. Diastolic dysfunction in hypertensive hearts: Roles of perivascular inflammation and reactive myocardial fibrosis. Hypertens. Res. 2005, 28, 483–490. [Google Scholar] [CrossRef]


{kind=link}
| Parameter | Patients n = 126 | Controls n = 107 | p-Value |
|---|---|---|---|
| Demographic parameters | |||
| Age, years | 55.7 (53.7–57.7) | 53.7 (51.9–55.5) | 0.1 |
| Sex, male, n (%) | 66 (52.4%) | 56 (52.3%) | 0.9 |
| Body mass index, kg/m2 | 26.6 (25.5–28.3) | 26.4 (24.2–27.9) | 0.1 |
| Clinical characteristics | |||
| Systolic blood pressure, mmHg | 140 (130–145) | 130 (120–135) | <0.001 * |
| Diastolic blood pressure, mmHg | 85 (80–90) | 80 (70–85) | <0.001 * |
| Hypertension, n (%) | 49 (38.9%) | 27 (25.2%) | 0.038 * |
| Diabetes mellitus, n (%) | 24 (19.0%) | 9 (8.4%) | 0.012 * |
| Hypercholesterolemia, n (%) | 85 (67.5%) | 46 (43.0%) | <0.001 * |
| Smoking habit, n (%) | 47 (37.3%) | 23 (21.5%) | 0.02 * |
| Positive family history of CVD, n (%) | 46 (36.5%) | 20 (18.7%) | 0.004 * |
| Basic laboratory tests | |||
| Blood platelets, 103/μL | 228 (190–276) | 228 (198–278) | 0.86 |
| Hemoglobin, g/dL | 14.5 (13.6–15.4) | 13.9 (12.8–14.8) | <0.001 * |
| White blood cells, 103/μL | 6.8 (5.3–7.9) | 6.1 (5.0–7.1) | 0.01 * |
| Total cholesterol, mmol/L | 5.4 (4.9–5.9) | 5.0 (4.6–5.5) | <0.001 * |
| HDL cholesterol, mmol/L | 1.2 (1.1–1.4) | 1.4 (1.2–1.6) | <0.001 * |
| LDL cholesterol, mmol/L | 3.2 (2.9–3.7) | 3.1 (2.8–3.4) | 0.13 |
| Triglycerides, mmol/L | 1.8 (1.4–2.1) | 1.7 (0.9–1.9) | <0.001 * |
| Glucose, mmol/L | 5.7 (4.9–6.1) | 5.4 (4.9–5.8) | 0.10 |
| Creatinine, μmol/L | 88.3 (78.0–98.0) | 79.2 (69.3–92.1) | <0.001 * |
| C-reactive protein, mg/L | 4.8 (3.6–6.5) | 2.8 (1.8–3.9) | <0.001 * |
| Homocysteine, μmol/L | 13.1 (10.2–15.2) | 10.6 (9.4–13.5) | <0.001 * |
| Parameter | Patients n = 126 | Controls n = 107 | p-Value |
|---|---|---|---|
| Ultrasound parameters of endothelial injury and atherosclerosis | |||
| Relative increase in flow-mediated dilatation of a brachial artery, % | 5.88 (4.40–7.69) | 9.52 (7.50–11.36) | <0.001 * |
| Mean value of intima-media thickness of a common carotid artery, mm | 0.80 (0.69–0.98) | 0.65 (0.58–0.73) | <0.001 * |
| β (95% CI) | R2 | Adjustment Statistics | |
|---|---|---|---|
| Relative increase in flow-mediated dilatation of the brachial artery, % | |||
| Age, years | −0.269 (−0.36 to −0.18) | 0.33 | F = 6.68, p < 0.00001 |
| Body mass index, kg/m2 | −0.137 (−0.23 to −0.05) | ||
| C-reactive protein, mg/L | −0.155 (−0.25 to −0.06) | ||
| Tricuspid regurgitation velocity, m/s | −0.253 (−0.35 to −0.16) | ||
| Left ventricular ejection fraction, % | 0.124 (0.03 to 0.22) | ||
| Interventricular septum thickness, cm | −0.288 (−0.38 to −0.19) | ||
| Intima-media thickness of the common carotid artery, mm | |||
| Systolic blood pressure, mmHg | 0.120 (0.04 to 0.20) | 0.35 | F = 7.95, p < 0.00001 |
| White blood cells, 103/μL | −0.112 (−0.20 to −0.02) | ||
| Total cholesterol, mmol/L | 0.174 (0.07 to 0.28) | ||
| Glucose, mmol/L | 0.260 (0.16 to 0.36) | ||
| C-reactive protein, mg/L | −0.099 (−0.19 to −0.01) | ||
| Interventricular septum thickness, cm | 0.430 (0.34 to 0.52) | ||
| Parameter | Patients n = 126 | Controls n = 107 | p-Value |
|---|---|---|---|
| Left ventricular basic parameters | |||
| LV ejection fraction, % | 67 (65–69) | 68 (66–70) | 0.026 * |
| LV end-diastolic dimension, mm | 49.5 (48.7–50.2) | 47.8 (47.2–48.5) | 0.008 * |
| LV end-systolic dimension, mm | 31.0 (29.0–33.0) | 30.0 (29.0–32.0) | 0.011 * |
| LV posterior wall thickness, cm | 1.1 (0.9–1.2) | 1.0 (0.9–1.0) | <0.001 * |
| Interventricular septum thickness, cm | 1.1 (1.0–1.4) | 1.0 (0.9–1.1) | <0.001 * |
| Left ventricular diastolic function | |||
| MV E-wave, cm/s | 90 (80–100) | 90 (80–95) | 0.26 |
| MV A-wave, cm/s | 95 (70–110) | 70 (70–88) | <0.001 * |
| MV E/A ratio, n | 0.90 (0.82–1.22) | 1.10 (0.80–1.28) | 0.14 |
| MV TDI septal e’, cm/s | 9.0 (7.0–11.0) | 11.0 (9.0–12.0) | <0.001 * |
| MV TDI lateral e’, cm/s | 9.5 (7.5–12.0) | 12.0 (10.0–13.0) | <0.001 * |
| MV TDI E/septal e’ ratio, n | 10.0 (8.0–12.9) | 8.1 (6.9–10.0) | <0.001 * |
| MV TDI E/lateral e’ ratio, n | 9.3 (7.3–12.0) | 7.4 (6.4–9.1) | <0.001 * |
| MV TDI mean value of E/e’ ratio, n | 9.7 (7.6–12.4) | 7.9 (6.7–9.6) | <0.001 * |
| Right ventricular diameter | |||
| Right ventricular mid diameter, mm | 22 (20–23) | 21 (20–23) | 0.004 * |
| Left atrium parameters | |||
| LA diameter, cm | 3.9 (3.7–4.2) | 3.8 (3.6–4.0) | 0.14 |
| LA area, cm2 | 21.5 (19.5–23.5) | 19.0 (17.8–21.0) | <0.001 * |
| LA volume, mL | 34.2 (30.6–36.5) | 30.3 (28.4–33.5) | <0.001 * |
| Assessment of pulmonary hypertension | |||
| Pulmonary artery systolic pressure, mmHg | 33.1 (31.9–34.3) | 28.7 (27.7–29.6) | <0.001 * |
| Tricuspid regurgitation velocity, m/s | 2.6 (2.4–2.9) | 2.4 (2.2–2.7) | <0.001 * |
| Ultrasound Parameter | A Group with: | p-Value # | |||||
|---|---|---|---|---|---|---|---|
| No Changes (0) | Mild Changes (1) | Severe Changes (2) | All Groups | 0–1 | 0–2 | 1–2 | |
| Relative increase in flow-mediated dilatation of a brachial artery, % | 8.88 (8.33–9.43) | 6.64 (6.00–7.27) | 5.85 (3.65–8.05) | 0.009 * | 0.09 | <0.001 * | 0.018 * |
| Mean value of intima-media thickness of a carotid artery, mm | 0.68 (0.66–0.70) | 0.80 (0.76–0.85) | 0.93 (0.85–1.01) | <0.001 * | 0.028 * | <0.001 * | 0.014 * |
| Interventricular septum thickness, cm | 1.02 (1.00–1.05) | 1.13 (1.09–1.17) | 1.31 (1.23–1.38) | <0.001 * | 0.015 * | <0.001 * | <0.001 * |
| LV posterior wall thickness, cm | 0.98 (0.95–1.00) | 1.06 (1.03–1.10) | 1.18 (1.12–1.23) | <0.001 * | 0.007 * | <0.001 * | 0.006 * |
| LA diameter, cm | 3.79 (3.73–3.86) | 3.95 (3.87–4.03) | 4.15 (4.00–4.29) | 0.002 * | 0.06 | <0.001 * | 0.004 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dropiński, J.; Dziedzic, R.; Kubicka-Trząska, A.; Romanowska-Dixon, B.; Iwaniec, T.; Zaręba, L.; Bazan, J.G.; Padjas, A.; Bazan-Socha, S. Central Retinal Artery Occlusion Is Related to Vascular Endothelial Injury and Left Ventricular Diastolic Dysfunction. J. Clin. Med. 2022, 11, 2263. https://doi.org/10.3390/jcm11082263
Dropiński J, Dziedzic R, Kubicka-Trząska A, Romanowska-Dixon B, Iwaniec T, Zaręba L, Bazan JG, Padjas A, Bazan-Socha S. Central Retinal Artery Occlusion Is Related to Vascular Endothelial Injury and Left Ventricular Diastolic Dysfunction. Journal of Clinical Medicine. 2022; 11(8):2263. https://doi.org/10.3390/jcm11082263
Chicago/Turabian StyleDropiński, Jerzy, Radosław Dziedzic, Agnieszka Kubicka-Trząska, Bożena Romanowska-Dixon, Teresa Iwaniec, Lech Zaręba, Jan G. Bazan, Agnieszka Padjas, and Stanisława Bazan-Socha. 2022. "Central Retinal Artery Occlusion Is Related to Vascular Endothelial Injury and Left Ventricular Diastolic Dysfunction" Journal of Clinical Medicine 11, no. 8: 2263. https://doi.org/10.3390/jcm11082263
APA StyleDropiński, J., Dziedzic, R., Kubicka-Trząska, A., Romanowska-Dixon, B., Iwaniec, T., Zaręba, L., Bazan, J. G., Padjas, A., & Bazan-Socha, S. (2022). Central Retinal Artery Occlusion Is Related to Vascular Endothelial Injury and Left Ventricular Diastolic Dysfunction. Journal of Clinical Medicine, 11(8), 2263. https://doi.org/10.3390/jcm11082263