
Does the Foot and Ankle Alignment Impact the Patellofemoral Pain Syndrome? A Systematic Review and Meta-Analysis

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
2.2. Exclusion Criteria
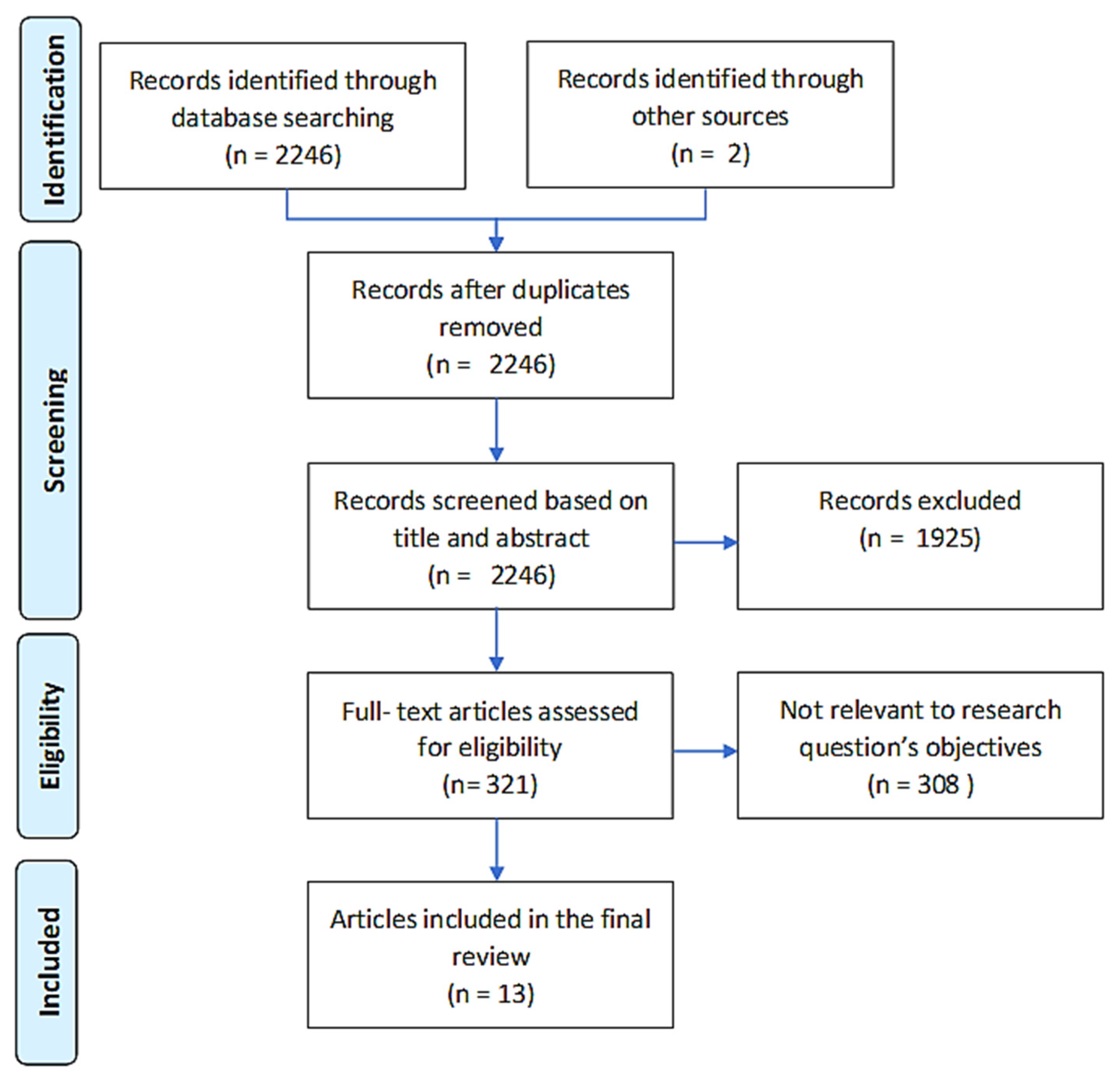
2.3. Search Strategy
2.4. Quality Assessment
2.5. Data Extraction
2.6. Statistical Analysis
3. Results
3.1. Static Alignment Measures
3.2. Dynamic Alignment Measures
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | Search Chain |
|---|---|
| Pubmed | (hindfoot*[tw] OR rearfoot*[tw] OR foot*[tw] OR ankle*[tw] OR forefoot*[tw]) AND (patellofemoral pain*[tw] OR patellofemoral syndrom*[tw] OR patello-femoral pain*[tw] OR patello-femoral syndrom*[tw] OR anterior knee pain*[tw] OR patellofemoral disorder*[tw] OR patello-femoral disorder*[tw]) OR ((arthralg*[tw] OR pain*[tw]) AND (knee joint[mesh] OR knee*[tw] OR patell*[tw] OR femoropatell*[tw] OR femoro-patell*[tw] OR retropatell*[tw] OR retro-patell*[tw] OR lateral facet*[tw] OR lateral compr*[tw] OR lateral press*[tw] OR odd facet*[tw] OR genu[tw]) AND (syndrom*[tw] OR dysfunct*[tw] OR disorder*[tw] OR chondromal*[tw] OR chondropath*[tw]))) AND (associat*[tw] OR risk*[tw] OR probabil*[tw] OR odds*[tw] OR relat*[tw] OR prevalen*[tw] OR predict*[tw] OR caus*[tw] OR etiol*[tw] OR interact*[tw] |
| Embase | ((‘rearfoot’/exp OR rearfoot OR ‘hindfoot’/exp OR hindfoot OR ‘foot’/exp OR foot OR ‘ankle’/exp OR ankle) AND (‘arthralgia’/exp OR arthralgia OR ‘knee joint’/exp OR ‘knee joint’ OR ((‘knee’/exp OR knee) AND (‘joint’/exp OR joint)) OR ‘anterior knee pain’/exp OR ‘anterior knee pain’ OR (anterior AND (‘knee’/exp OR knee) AND (‘pain’/exp OR pain))) OR patell* OR femoropatell* OR retropatell*) AND (‘pain’/exp OR pain OR ‘syndrome’/exp OR syndrome OR dysfunction) AND (‘risk factor’/exp OR ‘risk factor’ OR ((‘risk’/exp OR risk) AND factor) OR ‘association’/exp OR association OR ‘relative risk’/exp OR ‘relative risk’ OR ((‘relative’/exp OR relative) AND (‘risk’/exp OR risk)) OR ‘odds ratio’/exp OR ‘odds ratio’ OR (odds AND (‘ratio’/exp OR ratio))) |
| Web of Science | (((hindfoot* OR rearfoot* OR foot* OR ankle* OR forefoot*) AND (patellofemoral OR “patello-femoral” OR “anterior knee”) AND (pain* OR syndrom* OR disorder*)) OR ((arthralg* OR pain*) AND (knee* OR patell* OR femoropatell* OR retropatell* OR “retro-patellar” OR “lateral facet” OR “lateral compression” OR “lateral pressure” OR “odd facet” OR genu) AND (syndrom* OR dysfunct* OR disorder* OR chondromal* OR chondropath*))) AND (associat* OR risk* OR probabil* OR odds* OR relat* OR prevalen* OR predict* OR caus* OR etiol* OR interact*) |
| CINAHL | (rearfoot OR hindfoot OR foot OR ankle) AND (arthralgia OR knee joint OR anterior knee pain) OR (patell* OR femoropatell* OR femoropatell* OR retropatell*) AND (pain OR syndrome OR dysfunction) AND (risk factor OR association OR relative risk OR odds ratio). |
References
- Gaitonde, D.Y.; Ericksen, A.; Robbins, R.C. Patellofemoral Pain Syndrome. Am. Fam. Phys. 2019, 99, 88–94. [Google Scholar]
- de Oliveira Silva, D.; Magalhães, F.H.; Pazzinatto, M.F.; Briani, R.V.; Ferreira, A.S.; Aragão, F.A.; de Azevedo, F.M. Contribution of altered hip, knee and foot kinematics to dynamic postural impairments in females with patellofemoral pain during stair ascent. Knee 2016, 23, 376–381. [Google Scholar] [CrossRef]
- Novello, A.D.A.; Garbelotti, S.; Rabelo, N.D.D.A.; Ferraz, A.N.; Bley, A.S.; Correa, J.C.F.; Politti, F.; Lucareli, P.R.G. Descending stairs: Good or bad task to discriminate women with patellofemoral pain? Gait Posture 2018, 65, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Petersen, W.; Rembitzki, I.; Liebau, C. Patellofemoral pain in athletes. Open Access J. Sports Med. 2017, 8, 143–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devereaux, M.D.; Lachmann, S.M. Patello-femoral arthralgia in athletes attending a Sports Injury Clinic. Br. J. Sports Med. 1984, 18, 18–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schiavone Panni, A.; Braile, A.; De Cicco, A.; Lepore, F.; Vasso, M.; Toro, G. Reliability of the clinical examination in patello-femoral patology. G. Ital. Di Ortop. E Traumatol. 2018, 44, 30–37. [Google Scholar]
- Crossley, K.M.; van Middelkoop, M.; Barton, C.J.; Culvenor, A.G. Rethinking patellofemoral pain: Prevention, management and long-term consequences. Best Pract. Res. Clin. Rheumatol. 2019, 33, 48–65. [Google Scholar] [CrossRef]
- Lankhorst, N.; Bierma-Zeinstra, S.; Van Middelkoop, M. Factors associated with patellofemoral pain syndrome: A systematic review. Br. J. Sports Med. 2013, 47, 193–206. [Google Scholar] [CrossRef]
- Lack, S.; Barton, C.; Vicenzino, B.; Morrissey, D. Outcome Predictors for Conservative Patellofemoral Pain Management: A Systematic Review and Meta-Analysis. Sports Med. 2014, 44, 1703–1716. [Google Scholar] [CrossRef]
- Kannus, P.; Natri, A.; Paakkala, T.; Järvinen, M. An Outcome Study of Chronic Patellofemoral Pain Syndrome. Seven-Year Follow-up of Patients in a Randomized, Controlled Trial. J. Bone Jt. Surg. 1999, 81, 355–363. [Google Scholar] [CrossRef]
- Ferrari, D.; Kuriki, H.U.; Silva, C.; Alves, N.; de Azevedo, F.M. Diagnostic Accuracy of the Electromyography Parameters Associated With Anterior Knee Pain in the Diagnosis of Patellofemoral Pain Syndrome. Arch. Phys. Med. Rehabil. 2014, 95, 1521–1526. [Google Scholar] [CrossRef] [PubMed]
- Lankhorst, N.E.; Bierma-Zeinstra, S.M.; Van Middelkoop, M. Risk Factors for Patellofemoral Pain Syndrome: A Systematic Review. J. Orthop. Sports Phys. Ther. 2012, 42, 81–94. [Google Scholar] [CrossRef] [PubMed]
- Neal, B.S.; Griffiths, I.B.; Dowling, G.J.; Murley, G.S.; Munteanu, S.E.; Smith, M.M.F.; Collins, N.J.; Barton, C.J. Foot posture as a risk factor for lower limb overuse injury: A systematic review and meta-analysis. J. Foot Ankle Res. 2014, 7, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collins, N.J.; Barton, C.J.; Van Middelkoop, M.; Callaghan, M.; Rathleff, M.S.; Vicenzino, B.T.; Davis, I.S.; Powers, C.M.; Macri, E.; Hart, H.; et al. 2018 Consensus statement on exercise therapy and physical interventions (orthoses, taping and manual therapy) to treat patellofemoral pain: Recommendations from the 5th International Patellofemoral Pain Research Retreat, Gold Coast, Australia, 2017. Br. J. Sports Med. 2018, 52, 1170–1178. [Google Scholar] [CrossRef] [PubMed]
- Barton, C.J.; Levinger, P.; Webster, K.E.; Menz, H.B. Walking kinematics in individuals with patellofemoral pain syndrome: A case–control study. Gait Posture 2011, 33, 286–291. [Google Scholar] [CrossRef]
- Vicenzino, B.; Collins, N.; Cleland, J.; McPoil, T. A clinical prediction rule for identifying patients with patellofemoral pain who are likely to benefit from foot orthoses: A preliminary determination. Br. J. Sports Med. 2010, 44, 862–866. [Google Scholar] [CrossRef]
- Lee, J.; Yoon, J.; Cynn, H. Foot exercise and taping in patients with patellofemoral pain and pronated foot. J. Bodyw. Mov. Ther. 2017, 21, 216–222. [Google Scholar] [CrossRef]
- Luz, B.C.; dos Santos, A.F.; de Souza, M.C.; Sato, T.D.O.; Nawoczenski, D.A.; Serrão, F.V. Relationship between rearfoot, tibia and femur kinematics in runners with and without patellofemoral pain. Gait Posture 2018, 61, 416–422. [Google Scholar] [CrossRef]
- Thomeé, R.; Renström, P.; Karlsson, J.; Grimby, G. Patellofemoral pain syndrome in young women. I. A clinical analysis of alignment, pain parameters, common symptoms and functional activity level. Scand. J. Med. Sci. Sports 1995, 5, 237–244. [Google Scholar] [CrossRef]
- Aliberti, S.; Costa, M.D.S.; Passaro, A.D.C.; Arnone, A.C.; Hirata, R.; Sacco, I.C.N. Influence of patellofemoral pain syndrome on plantar pressure in the foot rollover process during gait. Clinics 2011, 66, 367–372. [Google Scholar] [CrossRef] [Green Version]
- Duffey, M.J.; Martin, D.F.; Cannon, D.W.; Craven, T.; Messier, S.P. Etiologic factors associated with anterior knee pain in distance runners. Med. Sci. Sports Exerc. 2000, 32, 1825–1832. [Google Scholar] [CrossRef] [PubMed]
- Livingston, L.A.; Mandigo, J.L. Bilateral Rearfoot Asymmetry and Anterior Knee Pain Syndrome. J. Orthop. Sports Phys. Ther. 2003, 33, 48–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haim, A.; Yaniv, M.; Dekel, S.; Amir, H. Patellofemoral pain syndrome: Validity of clinical and radiological features. Clin. Orthop. Relat. Res. 2006, 451, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Dierks, T.A.; Manal, K.T.; Hamill, J.; Davis, I.S. Proximal and Distal Influences on Hip and Knee Kinematics in Runners with Patellofemoral Pain During a Prolonged Run. J. Orthop. Sports Phys. Ther. 2008, 38, 448–456. [Google Scholar] [CrossRef]
- Barton, C.J.; Bonanno, D.; Levinger, P.; Menz, H. Foot and Ankle Characteristics in Patellofemoral Pain Syndrome: A Case Control and Reliability Study. J. Orthop. Sports Phys. Ther. 2010, 40, 286–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Oliveira Silva, D.; Briani, R.V.; Pazzinatto, M.F.; Ferrari, D.; Aragão, F.A.; Albuquerque, C.E.; Fábio, N.A.; Azevedoa, M. Reliability and differentiation capability of dynamic and static kinematic measurements of rearfoot eversion in patellofemoral pain. Clin. Biomech. 2015, 30, 144–148. [Google Scholar] [CrossRef]
- Aliberti, S.; Costa, M.S.; Passaro, A.C.; Arnone, A.C.; Sacco, I.C. Medial contact and smaller plantar loads characterize individuals with Patellofemoral Pain Syndrome during stair descent. Phys. Ther. Sport 2010, 11, 30–34. [Google Scholar] [CrossRef]
- Barton, C.J.; Levinger, P.; Crossley, K.M.; Webster, K.E.; Menz, H.B. The relationship between rearfoot, tibial and hip kinematics in individuals with patellofemoral pain syndrome. Clin. Biomech. 2012, 27, 702–705. [Google Scholar] [CrossRef]
- Steinberg, N.; Tenenbaum, S.; Hershkovitz, I.; Zeev, A.; Siev-Ner, I. Lower extremity and spine characteristics in young dancers with and without patellofemoral pain. Res. Sports Med. 2017, 25, 166–180. [Google Scholar] [CrossRef]
- Magee, D.J.; Manske, R.C. Orthopedic Physical Assessment, 2nd ed.; W.B. Saunders: Philadelphia, PA, USA, 1992. [Google Scholar]
- Cheung, R.T.H.; Ng, G.Y.F.; Chen, B.F.C. Association of Footwear with Patellofemoral Pain Syndrome in Runners. Sports Med. 2006, 36, 199–205. [Google Scholar] [CrossRef]
- Tiberio, D. The Effect of Excessive Subtalar Joint Pronation on Patellofemoral Mechanics: A Theoretical Model. J. Orthop. Sports Phys. Ther. 1987, 9, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Barg, A.; Bailey, T.; Richter, M.; Netto, C.D.C.; Lintz, F.; Burssens, A.; Phisitkul, P.; Hanrahan, C.J.; Saltzman, C.L. Weightbearing Computed Tomography of the Foot and Ankle: Emerging Technology Topical Review. Foot Ankle Int. 2018, 39, 376–386. [Google Scholar] [CrossRef] [PubMed]
- Bernasconi, A.; Cooper, L.; Lyle, S.; Patel, S.; Cullen, N.; Singh, D.; Welck, M. Intraobserver and interobserver reliability of cone beam weightbearing semi-automatic three-dimensional measurements in symptomatic pes cavovarus. Foot Ankle Surg. 2020, 26, 564–572. [Google Scholar] [CrossRef]
- Burssens, A.; Peeters, J.; Buedts, K.; Victor, J.; Vandeputte, G. Measuring hindfoot alignment in weight bearing CT: A novel clinical relevant measurement method. Foot Ankle Surg. 2016, 22, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Lintz, F.; Netto, C.D.C.; Barg, A.; Burssens, A.; Richter, M. Weight Bearing CT International Study Group Weight-bearing cone beam CT scans in the foot and ankle. EFORT Open Rev. 2018, 3, 278–286. [Google Scholar] [CrossRef] [PubMed]
- Richter, M.; Seidl, B.; Zech, S.; Hahn, S. PedCAT for 3D-imaging in standing position allows for more accurate bone position (angle) measurement than radiographs or CT. Foot Ankle Surg. 2014, 20, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Segal, N.A.; Frick, E.; Duryea, J.; Nevitt, M.C.; Niu, J.; Torner, J.C.; Felson, D.T.; Anderson, D.D. Comparison of tibiofemoral joint space width measurements from standing CT and fixed flexion radiography. J. Orthop. Res. 2017, 35, 1388–1395. [Google Scholar] [CrossRef] [Green Version]
- Roach, K.E.; Wang, B.; Kapron, A.L.; Fiorentino, N.M.; Saltzman, C.L.; Foreman, K.B.; Anderson, A.E. In Vivo Kinematics of the Tibiotalar and Subtalar Joints in Asymptomatic Subjects: A High-Speed Dual Fluoroscopy Study. J. Biomech. Eng. 2016, 138, 0910061–0910069. [Google Scholar] [CrossRef] [Green Version]
- Li, G.; De Frate, L.E.; Park, S.E.; Gill, T.J.; Rubash, H.E. In Vivo articular cartilage contact kinematics of the knee: An investigation using dual-orthogonal fluoroscopy and magnetic resonance image–based computer models. Am. J. Sports Med. 2005, 33, 102–107. [Google Scholar] [CrossRef]
- Gondim Teixeira, P.A.; Formery, A.S.; Jacquot, A.; Lux, G.; Loiret, I.; Perez, M.; Blum, A. Quantitative Analysis of Subtalar Joint Motion With 4D CT: Proof of Concept with Cadaveric and Healthy Subject Evaluation. Am. J. Roentgenol. 2017, 208, 150–158. [Google Scholar] [CrossRef]
- Forsberg, D.; Lindblom, M.; Quick, P.; Gauffin, H. Quantitative analysis of the patellofemoral motion pattern using semi-automatic processing of 4D CT data. Int. J. Comput. Assist. Radiol. Surg. 2016, 11, 1731–1741. [Google Scholar] [CrossRef] [PubMed]


| Author & Publication Year | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | Total Number |
|---|---|---|---|---|---|---|---|---|---|
| Thomee’ et al., 1995 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | ? | 6 |
| Duffey et al., 2000 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | ? | 6 |
| Livingston et al., 2003 | 1 | 0 | 0 | 1 | 1 | 1 | 0 | ? | 4 |
| Haim et al., 2006 | 0 | 1 | 0 | 1 | 1 | 1 | ? | 0 | 4 |
| Dierks et al., 2008 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | ? | 6 |
| Barton et al., 2010 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| Aliberti et al., 2010 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 6 |
| Aliberti et al., 2011 | 1 | 0 | 1 | 1 | 1 | 0 | ? | ? | 4 |
| Barton et al., 2012 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | ? | 6 |
| De Oliveira Silva et al., 2014 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 6 |
| Steinberg et al., 2017 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | ? | 6 |
| Novello et al., 2018 | 1 | 0 | 1 | 1 | 1 | 1 | ? | ? | 5 |
| Luz et al., 2018 | 1 | 0 | 1 | 1 | 1 | 1 | ? | ? | 5 |
| Author & Publication Year | Case Group | Control Group | ||||||
|---|---|---|---|---|---|---|---|---|
| N | Age | Height (cm) | Weight (Kg) | N | Age | Height (cm) | Weight (kg) | |
| Thomee’ et al., 1995 | 40 | 20 ± 3 | 169 ± 6 | 64 ± 9 | 20 | 22 ± 3 | 168 ± 6 | 61 ± 9 |
| Duffey et al., 2000 | 99 | 36 ± 9.9 & | 172.1 ± 10.9 & * | 69.5 ± 13.9 & * | 70 | 35 ± 8.4 & | 174.5 ± 9.2 & * | 70.2 ± 10.9 & * |
| Livingston et al., 2003 | 25 | 27.1 ± 7.9 $ | 174.3 ± 7.2 $ | 74.4 ± 10.3 $ | 50 | 26 ± 7 $ | 171.7 ± 5.5 $ | 74. 3 ± 11.5 $ |
| Haim et al., 2006 | 61 | 19.4 ± 1.2 | / | / | 25 | 24.1 ± 6.5 | / | / |
| Dierks et al., 2008 | 20 | 24.1 ± 7.4 | 171 ± 10 | 65.8 ± 12.6 | 20 | 22.7 ± 5.6 | 170 ± 8 | 63 ± 9.2 |
| Barton et al., 2010 | 20 | 22.8 ± 4.1 | 167.9 ± 6.8 | 66.8 ± 11.3 | 20 | 21.9 ± 3.5 | 169.9 ± 8.3 | 63.9 ± 14.0 |
| Aliberti et al., 2010 | 30 | 30 ± 7 | 165 ± 9 | 63 ± 11 | 44 | 30 ± 8 | 165 ± 8 | 60 ± 11 |
| Aliberti et al., 2011 | 22 | 30 ± 7 | 165 ± 9 | 63 ± 12 | 35 | 29 ± 7 | 164 ± 8 | 60 ± 11 |
| Barton et al., 2012 | 26 | 25 ± 5 | 169 ± 9 | 67 ± 14 | 20 | 23 ± 2 | 171 ± 8 | 66 ± 15 |
| De Oliveira Silva et al., 2014 | 29 | 21.9 ± 2.7 | 165 ± 5 | 65.7 ± 10.8 | 25 | 22.1 ± 3.7 | 165 ± 4 | 62.3 ± 7.3 |
| Steinberg et al., 2017 | 34 | 10–11 | 140.4 ± 8.4 | 31.1 ± 5.3 | 34 | 10–11 | 140.2 ± 8.2 | 31 ± 5.2 |
| 120 | 12–14 | 154.5 ± 8.1 | 43.1 ± 7.7 | 120 | 12–14 | 154.9 ± 8.3 | 43.5 ± 7.8 | |
| 117 | 15–16 | 160.6 ± 5.1 | 49.8 ± 5.6 | 117 | 15–16 | 161 ± 5.4 | 50.2 ± 5.5 | |
| Novello et al., 2018 | 34 | 23 (20–31) ^ | 1.61 (1.6–1.7) ^ * | 58 (52–62) ^ | 34 | 26 (23–28) ^ | 1.60 (1.55–1.65) ^ * | 55 (51–61) ^ |
| Luz et al., 2018 | 27 | 27 ± 4.2 | 172 ± 0.01 | 71.2 ± 12.8 | 27 | 26 ± 5.6 | 174 ± 0.1 | 72.5 ± 14.1 |
| (Part 1/3) | ||
| Author & Publication Year | Variables | Mean Difference (Patients–Controls) ± SD |
| Thomee’ et al., 1995 | -Angle between lower leg and horizontal | 0.1 ± 3.8 |
| -Angle between calcaneus and horizontal | 0.7 ± 3.5 | |
| -Angle between lower leg and calcaneus | 1.1 ± 4.5 | |
| -Arch index | 0.5 ± 10.2 | |
| Duffey et al., 2000 | -Dorsiflexion ankle ROM (°) | 0.4 ± 8.4 & |
| -Plantarflexion ankle ROM (°) | 1.1 ± 9.9 & | |
| -Arch index | 0.013 ± 0.762 & * | |
| -Calcaneus-tibia touchdown angle (°) | 2.8 ± 10.9 & | |
| -Pronation through first 10% of stance (°) | −1.3 ± 4.5 & * | |
| -Maximum pronation (°) | 0.5 ± 8.4 & | |
| -Total pronation (°) | −1.5 ± 8.4 & | |
| -Calcaneus-vertical tibial-distal angle (°) | 2 ± 10.3 & | |
| -Time to maximum pronation (%stance) | 1.4 ± 18.0 & | |
| -Time to maximum eversion (%stance) | 1.2 ± 14.5 & | |
| -Initial pronation velocity (° s−1) | −70 ± 231.0 & | |
| -Maximum pronation velocity (° s−1) | −79 ± 237.1 & | |
| -Time to maximum pronation velocity (%stance) | 1.5 ± 9.0 & | |
| Livingston et al., 2003 | -Right rearfoot angle (°) | −1.5 ± 6.9 |
| -Left rearfoot angle (°) | −0.5 ± 7.2 | |
| Haim et al., 2006 | -Pes cavus (patients vs. controls) | 16% vs. 16% |
| -Pes planus (patients vs. controls) | 31% vs. 15% | |
| Dierks et al., 2008 | -Arch height index | 0.011 ± 0.036 |
| -Rearfoot angle during cinematic study | Not disponible | |
| Barton et al., 2010 | Relax stance | |
| -Longitudinal arch angle (°) | −6.8 ± 10.5 * | |
| -Foot posture index (°) | 2.4 ± 4.9 * | |
| -Normalized vertical navicular height (%foot length) | −2 ± 4.3 | |
| -Calcaneal Angle (°) | 1.8 ± 5.5 | |
| -Normalized dorsal arch height (%foot length) | −1 ± 3.0 | |
| Foot posture relative, subtalar joint neutral | ||
| -Normalized navicular drop (%foot length) | 1.6 ± 2.3 * | |
| (part 2/3) | ||
| Author & Publication Year | Variables | Mean Difference (Patients–Controls) ± SD |
| Barton et al., 2010 (continue) | Foot posture relative, subtalar joint neutral | |
| -Normalized dorsal arch height difference (%foot length) | 0.7 ± 1.0 * | |
| -Normalized navicular drift (%foot length) | 1.6 ± 2.4 * | |
| -Longitudinal arch angle difference (°) | 3 ± 4.7 * | |
| -Calcaneal Angle difference | 2.6 ± 4.8 * | |
| Sagittal plane measures | ||
| -First metatarsophalangeal joint (°) | 3.1 ± 18.6 | |
| -Ankle dorsiflexion, knee flexed (°) | 3.8 ± 9.5 | |
| -Ankle dorsiflexion, knee extended (°) | 2.5 ± 10.4 | |
| Aliberti et al., 2010 | Contact area (cm2) | |
| -Medial Rearfoot | 1.8 ± 5.3 | |
| -Central Rearfoot | 0.1 ± 3.3 | |
| -Lateral Rearfoot | −0.4 ± 6.6 | |
| -Mid-foot | 3.6 ± 7.6 | |
| -Medial forefoot | 1.2 ± 4.0 | |
| -Lateral forefoot | 1.2 ± 3.8 | |
| Pressure-time integra (kPa·s) | ||
| -Medial Rearfoot | 3.5 ± 25.5 | |
| -Central Rearfoot | −0.6 ± 27.9 | |
| -Lateral Rearfoot | −0.7 ± 30.1 | |
| -Mid-foot | 0.7 ± 18.9 | |
| -Medial forefoot | −10.7 ± 46.3 | |
| -Lateral forefoot | −5.5 ± 47.2 | |
| Aliberti et al., 2011 | -Contact area medial rearfoot (kPa·s) -Contact area central rearfoot (kPa·s) -Contact area lateral rearfoot (kPa·s) -Contact area midfoot (kPa·s) -Contact area medial forefoot (kPa·s) -Contact area lateral forefoot (kPa·s) -Peak pressure medial rearfoot (kPa·s) -Peak pressure central rearfoot (kPa·s) -Peak pressure lateral rearfoot (kPa·s) -Peak pressure midfoot (kPa·s) -Peak pressure medial forefoot (kPa·s) -Peak pressure lateral forefoot (kPa·s) | Not disponible |
| (part 2/3) | ||
| Author & Publication Year | Variables | Mean Difference (Patients–Controls) ± SD |
| Barton et al., 2012 | -Gait velocity (m/s) | −0.1 ± 0.2 |
| Peak angles (°) | ||
| -Rearfoot eversion | 1.6 ± 5.4 | |
| Range of motion (°) | ||
| -Rearfoot eversion | 0.4 ± 2.9 | |
| De Oliveira Silva et al., 2014 | -Rearfoot eversion ROM (°) | 2.9 ± 5 * |
| -Rearfoot static angle (°) | 1.7 ± 5.2 | |
| Steinberg et al., 2017 | -Hind-foot varum (patients vs. controls) | 17.4% vs. 8.5% * |
| -Hind-foot valgus (patients vs. controls) | 17.5% vs. 13.7% | |
| -Ankle plantar-flexion (°) | −2.16 ± 10.54 * | |
| -Ankle dorsiflexion (°) | 1.37 ± 6.48 * | |
| Novello et al., 2018 | -Foot posture index | 5 (3–6) vs. 7.0 (5–8) ^ * |
| Hindfoot in relation to the horizontal plain (ROM) | ||
| -(+) Dorsiflexion (−) Plantar flexion | −1.0 ± 3.9 * | |
| -(+) Inversion (−) Eversion | −0.2 ± 1.8 | |
| -(+) Internal (−) External rotation | −0.3 ± 3.7 | |
| Hindfoot in relation to the tibia (ROM) | ||
| -(+) Dorsiflexion (−) Plantar flexion | −1.9 ± 7.2 * | |
| -(+) Inversion (−) Eversion | −1.4 ± 7.1 * | |
| -(+) Internal (−)External rotation | −1.7 ± 4.7 * | |
| Forefoot in relation to the hindfoot (ROM) | ||
| -(+) Dorsiflexion (−) Plantar flexion | 1.9 ± 5.6 * | |
| -(+) supination (−) Pronation | 1.3 ± 3.2 * | |
| -(+) Adduction (−) Abduction | −1 ± 2.6 * | |
| Luz et al., 2018 | Peak angles | |
| -Rearfoot eversion | 0.47 ± 5.7 | |
| Range of motion | ||
| -Rearfoot eversion | 0.89 ± 5.8 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martinelli, N.; Bergamini, A.N.; Burssens, A.; Toschi, F.; Kerkhoffs, G.M.M.J.; Victor, J.; Sansone, V. Does the Foot and Ankle Alignment Impact the Patellofemoral Pain Syndrome? A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 2245. https://doi.org/10.3390/jcm11082245
Martinelli N, Bergamini AN, Burssens A, Toschi F, Kerkhoffs GMMJ, Victor J, Sansone V. Does the Foot and Ankle Alignment Impact the Patellofemoral Pain Syndrome? A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2022; 11(8):2245. https://doi.org/10.3390/jcm11082245
Chicago/Turabian StyleMartinelli, Nicolò, Alberto Nicolò Bergamini, Arne Burssens, Filippo Toschi, Gino M. M. J. Kerkhoffs, Jan Victor, and Valerio Sansone. 2022. "Does the Foot and Ankle Alignment Impact the Patellofemoral Pain Syndrome? A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 11, no. 8: 2245. https://doi.org/10.3390/jcm11082245
APA StyleMartinelli, N., Bergamini, A. N., Burssens, A., Toschi, F., Kerkhoffs, G. M. M. J., Victor, J., & Sansone, V. (2022). Does the Foot and Ankle Alignment Impact the Patellofemoral Pain Syndrome? A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 11(8), 2245. https://doi.org/10.3390/jcm11082245