
Criteria for Return-to-Play (RTP) after Rotator Cuff Surgery: A Systematic Review of Literature

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
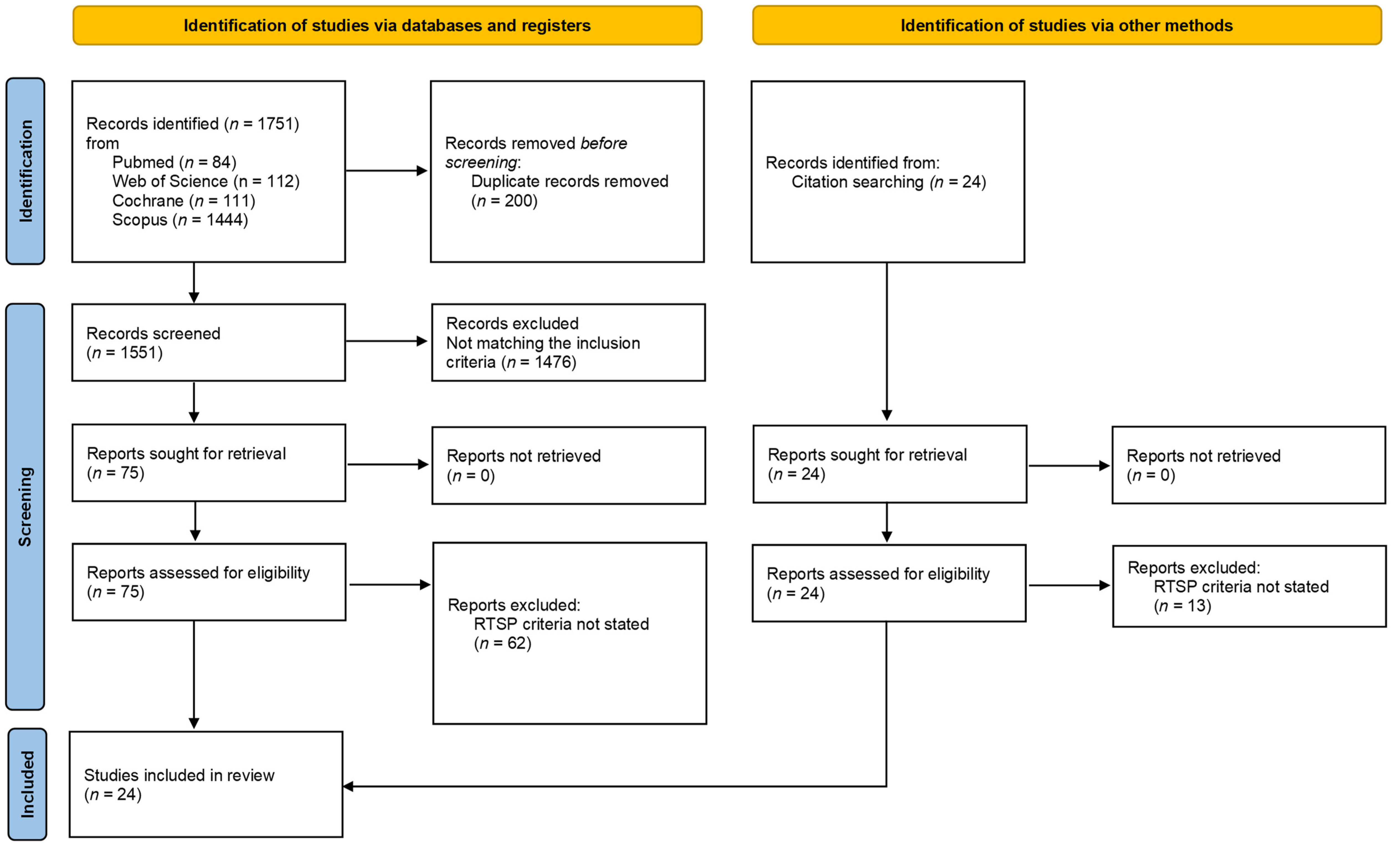
2.1. Systematic Literature Search
2.2. Eligibility Criteria and Data Extraction
2.3. Quality Assessment
3. Results
3.1. Patients’ Characteristics
3.2. Surgical Procedures
3.3. Return to Play Rates, Time and Criteria
3.3.1. Time
3.3.2. Strength
3.3.3. Pain
3.3.4. Range of Motion
3.3.5. Specific Training Programs
3.3.6. Other Criteria
3.3.7. Return to Preinjury Level and Retear
4. Discussion
5. Conclusions
- “Time from surgery” is the most used criterion to define readiness for RTP.
- Strength recovery is rarely used and poorly detailed.
- Preinjury performance levels and injury rates do not appear to be related to the use of specific RTP criteria
- Despite their importance, no clinical studies have used specific PROMS and psychological readiness assessment as RTP criteria.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Pulici, L.; Zanini, B.; Carrai, L.; Menon, A.; Compagnoni, R.; Randelli, P. Return to play after rotator cuff surgery. In Return to Play in Football; Springer: Berlin/Heidelberg, Germany, 2018; pp. 313–320. ISBN 9783662557136. [Google Scholar]
- Ji, X.; Bi, C.; Wang, F.; Wang, Q. Arthroscopic versus mini-open rotator cuff repair: An up-to-date meta-analysis of randomized controlled trials. Arthrosc. J. Arthrosc. Relat. Surg. 2015, 31, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Teunis, T.; Lubberts, B.; Reilly, B.T.; Ring, D. A systematic review and pooled analysis of the prevalence of rotator cuff disease with increasing age. J. Shoulder Elb. Surg. 2014, 23, 1913–1921. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, L.D.; Flanigan, D.C.; Norwig, J.; Jost, P.; Bradley, J. Prevalence and variance of shoulder injuries in elite collegiate football players. Am. J. Sports Med. 2005, 33, 1142–1146. [Google Scholar] [CrossRef] [PubMed]
- Mueller, M.; Hoy, G.; Branson, R. Management of in-season concurrent rotator cuff tear with shoulder instability in professional contact football athletes; respect the career goals! Asian J. Sports Med. 2016, 7, e28377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Headey, J.; Brooks, J.H.M.; Kemp, S.P.T. The epidemiology of shoulder injuries in English professional rugby union. Am. J. Sports Med. 2007, 35, 1537–1543. [Google Scholar] [CrossRef]
- Namdari, S.; Baldwin, K.; Ahn, A.; Huffman, G.R.; Sennett, B.J. Performance after rotator cuff tear and operative treatment: A case-control study of major league baseball pitchers. J. Athl. Train. 2011, 46, 296–302. [Google Scholar] [CrossRef] [Green Version]
- Cools, A.M.J.; Struyf, F.; De Mey, K.; Maenhout, A.; Castelein, B.; Cagnie, B. Rehabilitation of scapular dyskinesis: From the office worker to the elite overhead athlete. Br. J. Sports Med. 2014, 48, 692–697. [Google Scholar] [CrossRef] [Green Version]
- Creighton, D.W.; Shrier, I.; Shultz, R.; Meeuwisse, W.H.; Matheson, G.O. Return-to-play in sport: A decision-based model. Clin. J. Sport Med. 2010, 20, 379–385. [Google Scholar] [CrossRef]
- Ciccotti, M.C.; Syed, U.; Hoffman, R.; Abboud, J.A.; Ciccotti, M.G.; Freedman, K.B. Return to play criteria following surgical stabilization for traumatic anterior shoulder instability: A systematic review. Arthroscopy 2018, 34, 903–913. [Google Scholar] [CrossRef]
- Griffith, R.; Fretes, N.; Bolia, I.K.; Murray, I.R.; Meyer, J.; Weber, A.E.; Gamradt, S.C.; Petrigliano, F.A. Return-to-sport criteria after upper extremity surgery in athletes—A scoping review, part 1: Rotator cuff and shoulder stabilization procedures. Orthop. J. Sport. Med. 2021, 9, 23259671211021827. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef] [PubMed]
- Brown, D. A review of the pubmed PICO tool: Using evidence-based practice in health education. Health Promot. Pract. 2020, 21, 496–498. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, L.L.; Wang, Y.Y.; Yang, Z.H.; Huang, D.; Weng, H.; Zeng, X.T. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: What are they and which is better? Mil. Med. Res. 2020, 7, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (MINORS): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Andrews, J.R.; Broussard, T.S.; Carson, W.G. Arthroscopy of the shoulder in the management of partial tears of the rotator cuff: A preliminary report. Arthroscopy 1985, 1, 117–122. [Google Scholar] [CrossRef]
- Antoni, M.; Klouche, S.; Mas, V.; Ferrand, M.; Bauer, T.; Hardy, P. Return to recreational sport and clinical outcomes with at least 2 years follow-up after arthroscopic repair of rotator cuff tears. Orthop. Traumatol. Surg. Res. 2016, 102, 563–567. [Google Scholar] [CrossRef]
- Hawkins, R.J.; Morin, W.D.; Bonutti, P.M. Surgical treatment of full-thickness rotator cuff tears in patients 40 years of age or younger. J. Shoulder Elb. Surg. 1999, 8, 259–265. [Google Scholar] [CrossRef]
- Ide, J.; Maeda, S.; Takagi, K. Arthroscopic transtendon repair of partial-thickness articular-side tears of the rotator cuff: Anatomical clinical study. Am. J. Sports Med. 2005, 33, 1672–1679. [Google Scholar] [CrossRef]
- Kim, H.J.; Kim, J.Y.; Rhee, Y.G. When do patients return to previous daily activity after arthroscopic rotator cuff repair? Clin. Orthop. Relat. Res. 2019, 477, 403–413. [Google Scholar] [CrossRef]
- Krishnan, S.G.; Harkins, D.C.; Schiffern, S.C.; Pennington, S.D.; Burkhead, W.Z. Arthroscopic repair of full-thickness tears of the rotator cuff in patients younger than 40 years. Arthrosc. J. Arthrosc. Relat. Surg. 2008, 24, 324–328. [Google Scholar] [CrossRef] [PubMed]
- Liem, D.; Lichtenberg, S.; Magosch, P.; Habermeyer, P. Arthroscopic rotator cuff repair in overhead-throwing athletes. Am. J. Sports Med. 2008, 36, 1317–1322. [Google Scholar] [CrossRef] [PubMed]
- Mazoué, C.G.; Andrews, J.R. Repair of full-thickness rotator cuff tears in professional baseball players. Am. J. Sports Med. 2006, 34, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Ranalletta, M.; Rossi, L.A.; Sirio, A.; Bruchmann, G.; Maignon, G.D.; Bongiovanni, S.L. Return to sports after arthroscopic treatment of rotator cuff calcifications in athletes. Orthop. J. Sport. Med. 2016, 4, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Rossi, L.A.; Atala, N.A.; Bertona, A.; Bongiovanni, S.; Tanoira, I.; Maignon, G.; Ranalletta, M. Long-term outcomes after in situ arthroscopic repair of partial rotator cuff tears. Arthrosc. J. Arthrosc. Relat. Surg. 2019, 35, 698–702. [Google Scholar] [CrossRef]
- Rossi, L.A.; Atala, N.; Bertona, A.; Tanoira, I.; Bongiovanni, S.; Maignon, G.; Ranalletta, M. Return to sports after in situ arthroscopic repair of partial rotator cuff tears. Arthrosc. J. Arthrosc. Relat. Surg. 2019, 35, 32–37. [Google Scholar] [CrossRef]
- Shimada, Y.; Sugaya, H.; Takahashi, N.; Matsuki, K.; Tokai, M.; Morioka, T.; Ueda, Y.; Hoshika, S.; Hamada, H.; Inoue, S.; et al. Return to sport after arthroscopic rotator cuff repair in middle-aged and elderly swimmers. Orthop. J. Sport. Med. 2020, 8, 2325967120922203. [Google Scholar] [CrossRef]
- Azzam, M.G.; Dugas, J.R.; Andrews, J.R.; Goldstein, S.R.; Emblom, B.A.; Cain, E.L. Rotator cuff repair in adolescent athletes. Am. J. Sports Med. 2018, 46, 1084–1090. [Google Scholar] [CrossRef]
- Simon, M.; Popp, D.; Lutter, C.; Schöffl, V. Functional and sports-specific outcome after surgical repair of rotator cuff tears in rock climbers. Wilderness Environ. Med. 2017, 28, 342–347. [Google Scholar] [CrossRef] [Green Version]
- Spencer, E.E. Partial-thickness articular surface rotator cuff tears: An all-inside repair technique. Clin. Orthop. Relat. Res. 2010, 468, 1514–1520. [Google Scholar] [CrossRef] [Green Version]
- Tambe, A.; Badge, R.; Funk, L. Arthroscopic rotator cuff repair in elite rugby players. Int. J. Shoulder Surg. 2009, 3, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tibone, J.E.; Elrod, B.; Jobe, F.W.; Kerlan, R.K.; Carter, V.S.; Shields, C.L.; Lombardo, S.J.; Yocum, L. Surgical treatment of tears of the rotator cuff in athletes. J. Bone Jt. Surg. Am. 1986, 68, 887–891. [Google Scholar] [CrossRef]
- Bartl, C.; Scheibel, M.; Magosch, P.; Lichtenberg, S.; Habermeyer, P. Open repair of isolated traumatic subscapularis tendon tears. Am. J. Sports Med. 2011, 39, 490–496. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, S.; Greenspoon, J.A.; Horan, M.P.; Warth, R.J.; Millett, P.J. Two-year outcomes after arthroscopic rotator cuff repair in recreational athletes older than 70 years. Am. J. Sports Med. 2015, 43, 1737–1742. [Google Scholar] [CrossRef]
- Bigiliani, L.U.; Kimmel, J.; McCann, P.D.; Wolfe, I. Repair of rotator cuff tears in tennis players. Am. J. Sports Med. 1992, 20, 112–117. [Google Scholar] [CrossRef]
- Burns, J.P.; Snyder, S.J. Arthroscopic rotator cuff repair in patients younger than fifty years of age. J. Shoulder Elb. Surg. 2008, 17, 90–96. [Google Scholar] [CrossRef]
- Carbone, S.; Candela, V.; Gumina, S. High rate of return to crossfit training after arthroscopic management of rotator cuff tear. Orthop. J. Sport. Med. 2020, 8, 2325967120911039. [Google Scholar] [CrossRef]
- Carbone, S.; Castagna, V.; Passaretti, D.; Candela, V.; Cerciello, S.; Sante, E.D.; Gumina, S. Supraspinatus repair and biceps tenodesis in competitive CrossFit athletes allow for a 100% of return to sport. Knee Surg. Sport. Traumatol. Arthrosc. 2021, 29, 3929–3935. [Google Scholar] [CrossRef]
- Davey, M.S.; Hurley, E.T.; Scanlon, J.P.; Gaafar, M.; Pauzenberger, L.; Mullett, H. Excellent clinical outcomes and rates of return to play after arthroscopic rotator cuff repair for traumatic tears in athletes aged 30 years or less. Arthrosc. Sport. Med. Rehabil. 2021, 3, e667–e672. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372. [Google Scholar] [CrossRef]
- Sonnabend, D.H.; Howlett, C.R.; Young, A.A. Histological evaluation of repair of the rotator cuff in a primate model. J. Bone Joint Surg. Br. 2010, 92, 586–594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kibler, B.W.; Siascia, A. Rehabilitation following rotator cuff repair. In Shoulder Surgery Rehabilitation: A Teamwork Approach; Springer: Cham, Germany, 2016; pp. 1–202. ISBN 9783319248561. [Google Scholar]
- Schwank, A.; Blazey, P.; Asker, M.; Møller, M.; Hägglund, M.; Gard, S.; Skazalski, C.; Andersson, S.H.; Horsley, I.; Whiteley, R.; et al. 2022 bern consensus statement on shoulder injury prevention, rehabilitation, and return to sport for athletes at all participation levels. J. Orthop. Sports Phys. Ther. 2022, 52, 11–28. [Google Scholar] [CrossRef] [PubMed]
- Thigpen, C.A.; Shaffer, M.A.; Gaunt, B.W.; Leggin, B.G.; Williams, G.R.; Wilcox, R.B. The American Society of Shoulder and Elbow Therapists’ consensus statement on rehabilitation following arthroscopic rotator cuff repair. J. Shoulder Elb. Surg. 2016, 25, 521–535. [Google Scholar] [CrossRef] [PubMed]
- Sgroi, T.A.; Cilenti, M. Rotator cuff repair: Post-operative rehabilitation concepts. Curr. Rev. Musculoskelet. Med. 2018, 11, 86–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rokito, A.S.; Zuckerman, J.D.; Gallagher, M.A.; Cuomo, F. Strength after surgical repair of the rotator cuff. J. Shoulder Elb. Surg. 1996, 5, 12–17. [Google Scholar] [CrossRef]
- Pigozzi, F.; Giombini, A.; Macaluso, A. Do current methods of strength testing for the return to sport after injuries really address functional performance? Am. J. Phys. Med. Rehabil. 2012, 91, 458–460. [Google Scholar] [CrossRef] [Green Version]
- Lubiatowski, P.; Ogrodowicz, P.; Wojtaszek, M.; Kaniewski, R.; Stefaniak, J.; Dudziński, W.; Romanowski, L. Measurement of active shoulder proprioception: Dedicated system and device. Eur. J. Orthop. Surg. Traumatol. 2013, 23, 177–183. [Google Scholar] [CrossRef] [Green Version]
- Gumina, S.; Camerota, F.; Celletti, C.; Venditto, T.; Candela, V. The effects of rotator cuff tear on shoulder proprioception. Int. Orthop. 2019, 43, 229–235. [Google Scholar] [CrossRef] [Green Version]
- Myers, J.B.; Lephart, S.M. The Role of the Sensorimotor System in the Athletic Shoulder. J. Athl. Train. 2000, 35, 351. [Google Scholar]
- Cools, A.M.; Maenhout, A.G.; Vanderstukken, F.; Declève, P.; Johansson, F.R.; Borms, D. The challenge of the sporting shoulder: From injury prevention through sport-specific rehabilitation toward return to play. Ann. Phys. Rehabil. Med. 2021, 64, 101384. [Google Scholar] [CrossRef]
- Tkachuk, G.A.; Harris, C.A. Psychometric properties of the Tampa Scale for Kinesiophobia-11 (TSK-11). J. Pain 2012, 13, 970–977. [Google Scholar] [CrossRef] [PubMed]
- Glazer, D.D. Development and preliminary validation of the Injury-Psychological Readiness to Return to Sport (I-PRRS) scale. J. Athl. Train. 2009, 44, 185–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altintas, B.; Anderson, N.; Dornan, G.J.; Boykin, R.E.; Logan, C.; Millett, P.J. Return to sport after arthroscopic rotator cuff repair: Is there a difference between the recreational and the competitive athlete? Am. J. Sports Med. 2020, 48, 252–261. [Google Scholar] [CrossRef] [PubMed]
- Carnevale, A.; Longo, U.G.; Schena, E.; Massaroni, C.; Lo Presti, D.; Berton, A.; Candela, V.; Denaro, V. Wearable systems for shoulder kinematics assessment: A systematic review. BMC Musculoskelet. Disord. 2019, 20, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Thorpe, A.M.; O’Sullivan, P.B.; Mitchell, T.; Hurworth, M.; Spencer, J.; Booth, G.; Goebel, S.; Khoo, P.; Tay, A.; Smith, A. Are psychologic factors associated with shoulder scores after rotator cuff surgery? Clin. Orthop. Relat. Res. 2018, 476, 2062. [Google Scholar] [CrossRef]

{kind=link}
| Population | Intervention | Comparison | Outcome |
|---|---|---|---|
| Patients with rotator cuff tear | Rotator cuff repair Rotator cuff surgery | - | Return to play criteria, return to unrestricted activity criteria |
| Database | Search Terms |
|---|---|
| PubMed | (“rotator cuff repair” [All Fields] OR “rotator cuff surger *” [All Fields] OR “rotator cuff tear” [All Fields] OR “Rotator Cuff Injuries” [MeSH Terms] OR “Rotator Cuff” [MeSH Terms]) AND (“return to sport” [All Fields] OR “return to play” [All Fields] OR “unrestricted activity” [All Fields] OR “full activity” [All Fields]) |
| SCOPUS | ALL (“rotator cuff repair” OR “rotator cuff surger *” OR “rotator cuff tear” OR “Rotator Cuff”) AND (“return to sport” OR “return to play” OR “unrestricted activity” OR “full activity”) |
| Cochrane | (rotator cuff repair OR rotator cuff surger OR rotator cuff tear) AND (return to sport OR return to play OR unrestricted activity OR full activity) |
| WOS | (ALL = (“rotator cuff repair” OR “rotator cuff surger *” OR “rotator cuff tear” OR “Rotator Cuff”)) AND ALL = (“return to sport” OR “return to play” OR “unrestricted activity” OR “full activity”) |
| Combination of RTP Criteria | Number of Studies (%) |
|---|---|
| Time | 14 (58%) |
| Time, sport specific training program | 1 (4%) |
| Time, ROM | 1 (4%) |
| Time, strength | 1 (4%) |
| Time, functional recovery | 1 (4%) |
| Time, surgeon agreement, patients’ desire | 1 (4%) |
| ROM, strength, pain | 3 (13%) |
| ROM, strength, pain, sport specific training program | 1 (4%) |
| Time, ROM, strength, proprioception | 1 (4%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bravi, M.; Fossati, C.; Giombini, A.; Macaluso, A.; Lazzoli, J.K.; Santacaterina, F.; Bressi, F.; Vorini, F.; Campi, S.; Papalia, R.; et al. Criteria for Return-to-Play (RTP) after Rotator Cuff Surgery: A Systematic Review of Literature. J. Clin. Med. 2022, 11, 2244. https://doi.org/10.3390/jcm11082244
Bravi M, Fossati C, Giombini A, Macaluso A, Lazzoli JK, Santacaterina F, Bressi F, Vorini F, Campi S, Papalia R, et al. Criteria for Return-to-Play (RTP) after Rotator Cuff Surgery: A Systematic Review of Literature. Journal of Clinical Medicine. 2022; 11(8):2244. https://doi.org/10.3390/jcm11082244
Chicago/Turabian StyleBravi, Marco, Chiara Fossati, Arrigo Giombini, Andrea Macaluso, José Kawazoe Lazzoli, Fabio Santacaterina, Federica Bressi, Ferruccio Vorini, Stefano Campi, Rocco Papalia, and et al. 2022. "Criteria for Return-to-Play (RTP) after Rotator Cuff Surgery: A Systematic Review of Literature" Journal of Clinical Medicine 11, no. 8: 2244. https://doi.org/10.3390/jcm11082244
APA StyleBravi, M., Fossati, C., Giombini, A., Macaluso, A., Lazzoli, J. K., Santacaterina, F., Bressi, F., Vorini, F., Campi, S., Papalia, R., & Pigozzi, F. (2022). Criteria for Return-to-Play (RTP) after Rotator Cuff Surgery: A Systematic Review of Literature. Journal of Clinical Medicine, 11(8), 2244. https://doi.org/10.3390/jcm11082244