
Joint-Preserving Surgery in Varus Ankle Osteoarthritis

 , , , , , ,
, , , , , , 
Abstract
1. Introduction
2. Etiology and Biomechanics of the Varus Ankle and Hindfoot
2.1. Etiology
2.2. Biomechanics
3. Clinical Assessment
3.1. Imaging Modalities
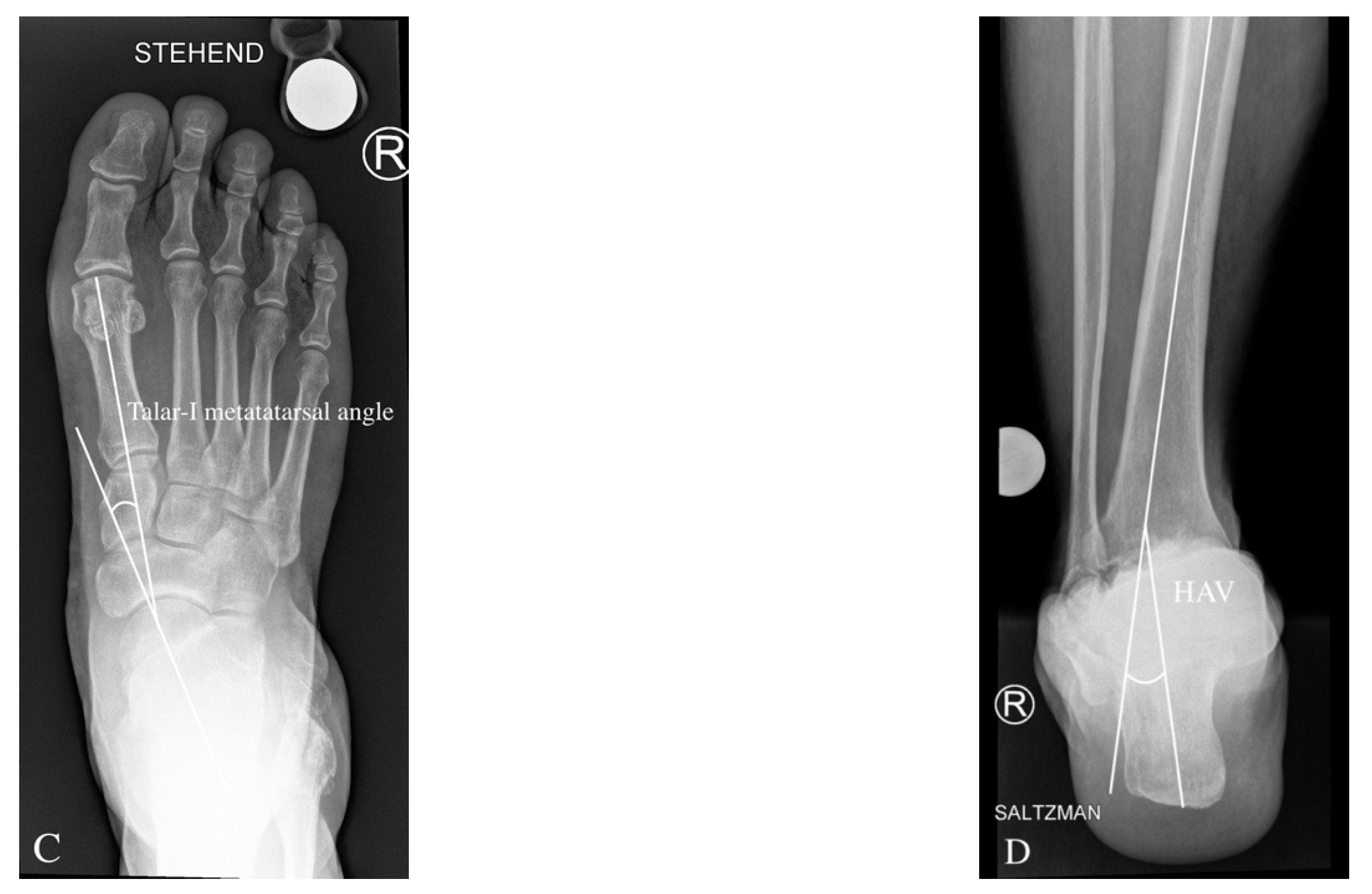
3.2. Preoperative Radiological Angle Measurements
3.3. Conservative Treatment of Varus Ankle Osteoarthritis
3.4. Surgical Treatment of the Varus Ankle Osteoarthritis
3.5. Joint-Preserving Surgery (JPS)
3.6. Supramalleolar Osteotomy
4. Surgical Technique
4.1. Medial Open Wedge Supramalleolar Tibia Osteotomy
4.2. Lateral Closing Wedge Supramalleolar Tibia and Fibula Osteotomy
5. Aftertreatment
6. Discussion
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lee, W.-C. Extraarticular Supramalleolar Osteotomy for Managing Varus Ankle Osteoarthritis, Alternatives for Osteotomy: How and Why? Foot Ankle Clin. 2016, 21, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Ahn, T.-K.; Yi, Y.; Cho, J.-H.; Lee, W.-C. A Cohort Study of Patients Undergoing Distal Tibial Osteotomy without Fibular Osteotomy for Medial Ankle Arthritis with Mortise Widening. J. Bone Jt. Surg. 2015, 97, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, N.A.; Herzenberg, J.E.; Lamm, B.M. Supramalleolar Osteotomy for Realignment of the Ankle Joint. Clin. Podiatr. Med. Surg. 2012, 29, 465–482. [Google Scholar] [CrossRef] [PubMed]
- Mulhern, J.L.; Protzman, N.M.; Brigido, S.A.; Deol, P.P.S. Supramalleolar Osteotomy: Indications and Surgical Techniques. Clin. Podiatr. Med. Surg. 2015, 32, 445–461. [Google Scholar] [CrossRef] [PubMed]
- Graehl, P.M.; Hersh, M.R.; Heckman, J.D. Supramalleolar osteotomy for the treatment of symptomatic tibial malunion. J. Orthop. Trauma 1987, 1, 281–292. [Google Scholar] [CrossRef]
- Takakura, Y.; Tanaka, Y.; Kumai, T.; Tamai, S. Low Tibial Osteotomy for Osteoarthritis of the Ankle. Results of a New Operation in 18 Patients. J. Bone Jt. Surgery. Br. 1995, 77, 50–54. [Google Scholar] [CrossRef]
- Hintermann, B.; Barg, A.; Knupp, M. Corrective supramalleolar osteotomy for malunited pronation-external rotation fractures of the ankle. Bone Jt. Surgery. Br. 2011, 93, 1367–1372. [Google Scholar] [CrossRef][Green Version]
- Tanaka, Y. The Concept of Ankle Joint Preserving Surgery: Why Does Supramalleolar Osteotomy Work and How to Decide When to Do an Osteotomy or Joint Replacement. Foot Ankle Clin. 2012, 17, 545–553. [Google Scholar] [CrossRef]
- Barg, A.; Saltzman, C.L. Joint-Preserving Procedures in Patients with Varus Deformity: Role of Supramalleolar Osteotomies. Foot Ankle Clin. 2019, 24, 239–264. [Google Scholar] [CrossRef]
- Kim, J.-B.; Yi, Y.; Kim, J.-Y.; Cho, J.-H.; Kwon, M.-S.; Choi, S.-H.; Lee, W.-C. Weight-Bearing Computed Tomography Findings in Varus Ankle Osteoarthritis: Abnormal Internal Rotation of the Talus in the Axial Plane. Skelet. Radiol. 2017, 46, 1071–1080. [Google Scholar] [CrossRef]
- Apostle, K.L.; Sangeorzan, B.J. Anatomy of the Varus Foot and Ankle. Foot Ankle Clin. 2012, 17, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Becker, A.S.; Myerson, M.S. The indications and technique of supramalleolar osteotomy. Foot Ankle Clin. 2009, 14, 549–561. [Google Scholar] [CrossRef] [PubMed]
- Rush, S.M. Supramalleolar osteotomy. Clin. Podiatr. Med. Surg. 2009, 26, 245–257. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, K.; Tanaka, Y.; Kumai, T.; Sugimoto, K.; Takakura, Y. Correlation of Compensatory Alignment of the Subtalar Joint to the Progression of Primary Osteoarthritis of the Ankle. Foot Ankle Int. 2008, 29, 400–406. [Google Scholar] [CrossRef]
- Tanaka, Y.; Takakura, Y.; Hayashi, K.; Taniguchi, A.; Kumai, T.; Sugimoto, K. Low tibial osteotomy for varus-type osteoarthritis of the ankle. J. Bone Jt. Surgery. Br. 2006, 88, 909–913. [Google Scholar] [CrossRef] [PubMed]
- Kellett, J.J.; Lovell, G.A.; Eriksen, D.A.; Sampson, M.J. Diagnostic Imaging of Ankle Syndesmosis Injuries: A General Review. J. Med. Imaging Radiat. Oncol. 2018, 62, 159–168. [Google Scholar] [CrossRef]
- van Wensen, R.J.A.; van den Bekerom, M.P.J.; Marti, R.K.; van Heerwaarden, R.J. Reconstructive Osteotomy of Fibular Malunion: Review of the Literature. Strateg. Trauma Limb Reconstr. 2011, 6, 51–57. [Google Scholar] [CrossRef][Green Version]
- Weber, B.G. Lengthening Osteotomy of the Fibula to Correct a Widened Mortice of the Ankle after Fracture. Int. Orthop. 1981, 4, 289–293. [Google Scholar] [CrossRef]
- Magerkurth, O.; Knupp, M.; Ledermann, H.; Hintermann, B. Evaluation of Hindfoot Dimensions: A Radiological Study. Foot Ankle Int. 2006, 27, 612–616. [Google Scholar] [CrossRef]
- Buck, F.M.; Hoffmann, A.; Mamisch-Saupe, N.; Espinosa, N.; Resnick, D.; Hodler, J. Hindfoot Alignment Measurements: Rotation-Stability of Measurement Techniques on Hindfoot Alignment View and Long Axial View Radiographs. AJR Am. J. Roentgenol. 2011, 197, 578–582. [Google Scholar] [CrossRef]
- Krähenbühl, N.; Lenz, A.L.; Lisonbee, R.; Deforth, M.; Zwicky, L.; Hintermann, B.; Saltzman, C.L.; Anderson, A.E.; Barg, A. Imaging of the subtalar joint: A novel approach to an old problem. J. Orthop. Res. 2019, 37, 921–926. [Google Scholar] [CrossRef] [PubMed]
- Barg, A.; Pagenstert, G.I.; Horisberger, M.; Paul, J.; Gloyer, M.; Henninger, H.B.; Valderrabano, V. Supramalleolar Osteotomies for Degenerative Joint Disease of the Ankle Joint: Indication, Technique and Results. Int. Orthop. 2013, 37, 1683–1695. [Google Scholar] [CrossRef] [PubMed]
- Schmid, T.; Krause, F.G. Conservative Treatment of Asymmetric Ankle Osteoarthritis. Foot Ankle Clin. 2013, 18, 437–448. [Google Scholar] [CrossRef] [PubMed]
- Simental-Mendía, M.; Sánchez-García, A.; Vilchez-Cavazos, F.; Acosta-Olivo, C.A.; Peña-Martínez, V.M.; Simental-Mendía, L.E. Effect of glucosamine and chondroitin sulfate in symptomatic knee osteoarthritis: A systematic review and meta-analysis of randomized placebo-controlled trials. Rheumatol Int. 2018, 38, 1413–1428. [Google Scholar] [CrossRef]
- Khosla, S.K.; Baumhauer, J.F. Dietary and viscosupplementation in ankle arthritis. Foot Ankle Clin. 2008, 13, 353–361. [Google Scholar] [CrossRef]
- Salk, R.S.; Chang, T.J.; D’Costa, W.F.; Soomekh, D.J.; Grogan, K.A. Sodium hyaluronate in the treatment of osteoarthritis of the ankle: A controlled, randomized, double-blind pilot study. J. Bone Jt. Surg. Am. 2006, 88, 295–302. [Google Scholar] [CrossRef]
- Sun, S.-F.; Hsu, C.-W.; Sun, H.-P.; Chou, Y.-J.; Li, H.-J.; Wang, J.-L. The effect of three weekly intra-articular injections of hyaluronate on pain, function, and balance in patients with unilateral ankle arthritis. J. Bone Jt. Surg. Am. 2011, 93, 1720–1726. [Google Scholar] [CrossRef]
- Henning, P.R.; Grear, B.J. Platelet-rich plasma in the foot and ankle. Curr. Rev. Musculoskelet. Med. 2018, 11, 616–623. [Google Scholar] [CrossRef]
- Kitaoka, H.B. Arthrodesis of the ankle: Technique, complications, and salvage treatment. Instr. Course Lect. 1999, 48, 255–261. [Google Scholar]
- Shih, L.-Y.; Wu, J.-J.; Lo, W.-H. Changes in gait and maximum ankle torque in patients with ankle arthritis. Foot Ankle 1993, 14, 97–103. [Google Scholar] [CrossRef]
- Hintermann, B.; Ruiz, R.; Barg, A. Novel Double Osteotomy Technique of Distal Tibia for Correction of Asymmetric Varus Osteoarthritic Ankle. Foot Ankle Int. 2017, 38, 970–981. [Google Scholar] [CrossRef] [PubMed]
- Myerson, M.S.; Zide, J.R. Management of Varus Ankle Osteoarthritis with Joint-Preserving Osteotomy. Foot Ankle Clin. 2013, 18, 471–480. [Google Scholar] [CrossRef] [PubMed]
- Stamatis, E.D.; Cooper, P.S.; Myerson, M.S. Supramalleolar Osteotomy for the Treatment of Distal Tibial Angular Deformities and Arthritis of the Ankle Joint. Foot Ankle Int. 2003, 24, 754–764. [Google Scholar] [CrossRef] [PubMed]
- Hintermann, B.; Knupp, M.; Barg, A. Joint-Preserving Surgery of Asymmetric Ankle Osteoarthritis with Peritalar Instability. Foot Ankle Clin. 2013, 18, 503–516. [Google Scholar] [CrossRef]
- LaCorda, J.B.; Jung, H.-G.; Im, J.-M. Supramalleolar Distal Tibiofibular Osteotomy for Medial Ankle Osteoarthritis: Current Concepts. Clin. Orthop. Surg. 2020, 12, 271–278. [Google Scholar] [CrossRef]
- Pagenstert, G.I.; Hintermann, B.; Barg, A.; Leumann, A.; Valderrabano, V. Realignment Surgery as Alternative Treatment of Varus and Valgus Ankle Osteoarthritis. Clin. Orthop. Relat. Res. 2007, 462, 156–468. [Google Scholar] [CrossRef]
- Krähenbühl, N.; Akkaya, M.; Deforth, M.; Zwicky, L.; Barg, A.; Hintermann, B. Extraarticular Supramalleolar Osteotomy in Asymmetric Varus Ankle Osteoarthritis. Foot Ankle Int. 2019, 40, 936–947. [Google Scholar] [CrossRef]
- Haraguchi, N.; Ota, K.; Tsunoda, N.; Seike, K.; Kanetake, Y.; Tsutaya, A. Weight-bearing-line analysis in supramalleolar osteotomy for varus-type osteoarthritis of the ankle. J. Bone Jt. Surg. Am. 2015, 97, 333–339. [Google Scholar] [CrossRef]
- Gross, C.E.; Barfield, W.; Schweizer, C.; Rasch, H.; Hirschmann, M.T.; Hintermann, B.; Knupp, M. The Utility of the Ankle SPECT/CT Scan to Predict Functional and Clinical Outcomes in Supramalleolar Osteotomy Patients. J. Orthop. Res. 2018, 36, 2015–2021. [Google Scholar] [CrossRef]
- Chopra, V.; Stone, P.; Ng, A. Supramalleolar Osteotomies. Clin. Podiatr. Med. Surg. 2017, 34, 445–460. [Google Scholar] [CrossRef]
- Cheng, Y.-M.; Huang, P.-J.; Hong, S.-H.; Lin, S.-Y.; Liao, C.-C.; Chiang, H.-C.; Chen, L.-C. Low tibial osteotomy for moderate ankle arthritis. Arch. Orthop. Trauma. Surg. 2001, 121, 355–358. [Google Scholar] [CrossRef] [PubMed]
- Ayyaswamy, B.; Jain, N.; Limaye, R. Functional and radiological medium term outcome following supramalleolar osteotomy for asymmetric ankle arthritis- A case series of 33 patients. J Orthop. 2020, 21, 500–506. [Google Scholar] [CrossRef] [PubMed]
- Hintermann, B.; Knupp, M.; Barg, A. Korrekturosteotomien am distalen Unterschenkel und Rückfuss [Osteotomies of the distal tibia and hindfoot for ankle realignment]. Orthopade 2008, 37, 212–223. [Google Scholar] [CrossRef] [PubMed]
- Knupp, M.; Stufkens, S.A.S.; Bolliger, L.; Barg, A.; Hintermann, B. Classification and treatment of supramalleolar deformities. Foot Ankle Int. 2011, 32, 1023–1031. [Google Scholar] [CrossRef]
- Pagenstert, G.; Leumann, A.; Hintermann, B.; Valderrabano, V. Sports and recreation activity of varus and valgus ankle osteoarthritis before and after realignment surgery. Foot Ankle Int. 2008, 29, 985–993. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Post-Traumatic | Varus malunion of tibial shaft fractures |
| Varus malunion of tibial plafond fractures or malleolar fractures | |
| Varus malunion of talus and calcaneus fractures | |
| Avascular necrosis of talus | |
| Chronic lateral ankle ligament instability | |
| Postcompartment syndrome | |
| Degenerative | Rheumatoid osteoarthritis |
| Varus knee osteoarthritis | |
| Charcot osteoarthropathy | |
| Neuromuscular | Stroke |
| Central and peripheral nerve disorders | |
| Hereditary motor sensory neuropathy/Charcot–Marie–Tooth disease | |
| Polio | |
| Cerebral palsy | |
| Peroneal brevis muscle insufficiency | |
| Peroneal tendon ruptures | |
| Congenital | Residual clubfoot (Talipes equinovarus) |
| Tarsal coalition | |
| Excessive tibial external rotation |
| Indications | Asymmetric medial ankle OA with associated varus deformity and a lateral partially preserved tibiotalar joint |
| Osteochondral lesions on the medial talar side of the tibiotalar joint | |
| Post-traumatic varus deformities after lower leg fractures | |
| Ankle–hindfoot realignment before or together with total ankle arthroplasty | |
| Contraindications | End-stage OA of the ankle with more than half of the tibiotalar joint surface involved |
| Unmanageable ankle–hindfoot instability/neuromuscular imbalance | |
| Osteomyelitis or infection | |
| Severe vascular and/or neurologic deficiency | |
| Relative Contraindications | Tobacco use (because of most likely expected high rate of nonunion or delayed union) |
| Advanced age (>70 years) | |
| Patients in poor general health who are unable to accomplish nonweight-bearing rehabilitation after surgery | |
| Untreated diabetes mellitus (with or without diabetic polyneuropathy) | |
| Altered bone quality due to medication (e.g., long-term medication with steroids) | |
| Large cysts | |
| Osteopenia or osteoporosis | |
| Untreated rheumatoid osteoarthritis | |
| Special Risks and Pitfalls | Intraoperative injury of neurovascular structures and/or tendons |
| Wound healing problems/infections | |
| Under correction/overcorrection | |
| Loss of correction due to OA progression | |
| Delayed union/nonunion | |
| Hardware removal because of pain/discomfort |
| Associated Deformities | Further Procedure Required in Addition to Smot |
|---|---|
| Osteochondral Lesion of the Medial Ankle (Talus, Tibia, and Plafond) | Autologous Matrix-Induced Chondrogenesis (AMIC) |
| Ventromedial Bony Ankle Impingement (Osteophytes) | Ventromedial Cheilectomy |
| Ankle Ligaments: Lateral Chronic Ankle Instability Deltoid Contracture | Anatomical Lateral Ankle Ligament Reconstruction Deltoid Release (at medial malleolus) |
| Varus Hindfoot with No Subtalar OA | Lateral Sliding Calcaneal Osteotomy/Dwyer Calcaneal Osteotomy |
| Varus Hindfoot with Subtalar Osteoarthritis | Valgisating Subtalar Arthrodesis |
| Varus Hindfoot with Hindfoot Osteoarthritis (Subtalar and Talonavicular/Calcaneocuboidal) | Valgisating Triple Arthrodesis |
| Medial Malleolus Deformity (Erosion, Malposition…) | Medial Malleolus Osteotomy |
| Tight Gastrocnemius–Soleus Complex | Strayer or Proximal Gastrocnemius Recession |
| Peroneal Tendon Pathologies Posterior Tibial Tendon Tightness | Primary Repair or PL-to-PB-tendon transfer Posterior Tibial Tendon Elongation |
| Pes Cavus | Reversed Cotton Osteotomy ± Plantar Fascia Release |
| Plantar Flexed First Metatarsal | Dorsal Closing Wedge First Metatarsal Osteotomy |
| Plantar Flexed First Metatarsal with Overdrive of Peroneal Longus Tendon | Dorsal Closing Wedge First Metatarsal Osteotomy and PL-to-PB Tendon Transfer |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alajlan, A.; Santini, S.; Alsayel, F.; Teoh, K.H.; Alharbi, W.; Puls, L.; Camathias, C.; Herrera-Pérez, M.; Tejero, S.; Barg, A.; et al. Joint-Preserving Surgery in Varus Ankle Osteoarthritis. J. Clin. Med. 2022, 11, 2194. https://doi.org/10.3390/jcm11082194
Alajlan A, Santini S, Alsayel F, Teoh KH, Alharbi W, Puls L, Camathias C, Herrera-Pérez M, Tejero S, Barg A, et al. Joint-Preserving Surgery in Varus Ankle Osteoarthritis. Journal of Clinical Medicine. 2022; 11(8):2194. https://doi.org/10.3390/jcm11082194
Chicago/Turabian StyleAlajlan, Ahmad, Simone Santini, Faisal Alsayel, Kar H. Teoh, Waheeb Alharbi, Luise Puls, Carlo Camathias, Mario Herrera-Pérez, Sergio Tejero, Alexej Barg, and et al. 2022. "Joint-Preserving Surgery in Varus Ankle Osteoarthritis" Journal of Clinical Medicine 11, no. 8: 2194. https://doi.org/10.3390/jcm11082194
APA StyleAlajlan, A., Santini, S., Alsayel, F., Teoh, K. H., Alharbi, W., Puls, L., Camathias, C., Herrera-Pérez, M., Tejero, S., Barg, A., Wiewiorski, M., & Valderrabano, V. (2022). Joint-Preserving Surgery in Varus Ankle Osteoarthritis. Journal of Clinical Medicine, 11(8), 2194. https://doi.org/10.3390/jcm11082194