

Evaluation of Drug Interactions in Patients Treated with DAAs for Hepatitis C Therapy with Comorbidities and Cardiovascular Issues—A Delphi Consensus Project

 , , , and
, , , and
Abstract
1. Introduction
2. Subjects and Methods
3. Results
Study Population
4. Discussion
- Treating HCV patients with comorbidities and comedications requires a particular multidisciplinary approach.
- Treating HCV patients taking medications for cardiovascular problems requires particular attention to the presence and management of drug–drug interactions.
- In HCV patients taking antihypertensive, antithrombotic or lipid-lowering agents for the prevention or treatment of cardiovascular diseases, the relevant drugs should not be withdrawn, changed or reduced in dosage—even for a short period—when treating hepatitis C.
- Oral DAAs have different profiles in terms of drug–drug interactions.
- The potential for DDIs with HCV DAAs is more frequent with GLE-PIB than SOF-VEL, and DDIs represent a significant reason one regimen may be selected in favor of another.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centre for Disease Analysis. Web Annex, B. WHO estimates of the prevalence and incidence of hepatitis C virus infection by WHO region, 2015. In Global Hepatitis Report 2017; World Health Organization: Geneve, Switzerland, 2018. [Google Scholar]
- Pawlotsky, J.M.; Negro, F.; Aghemo, A.; Berenguer, M.; Dalgard, O.; Dusheiko, G.; Marra, F.; Puoti, M.; Wedemeyer, H.; European Association for the Study of the Liver. EASL recommendations on treatment of hepatitis C: Final update of the series. J. Hepatol. 2020, 73, 1170–1218. [Google Scholar] [CrossRef] [PubMed]
- Garrison, K.L.; German, P.; Mogalian, E.; Mathias, A. The Drug-Drug Interaction Potential of Antiviral Agents for the Treatment of Chronic Hepatitis C Infection. Drug Metab. Dispos. 2018, 46, 1212–1225. [Google Scholar] [CrossRef] [PubMed]
- Mangia, A.; Scaglione, F.; Toniutto, P.; Pirisi, M.; Coppola, N.; Di Perri, G.; Nieto, G.A.; Calabrese, S.; Hernandez, C.; Perrone, V.; et al. Drug–Drug Interactions in Italian Patients with Chronic Hepatitis C Treated with Pangenotypic Direct Acting Agents: Insights from a Real-World Study. Int. J. Environ. Res. Public Health 2021, 18, 7144. [Google Scholar] [CrossRef] [PubMed]
- Curry, M.P.; Flamm, S.L.; Milligan, S.; Tsai, N.; Wick, N.; Younossi, Z.; Afdhal, N.H. Prevalence of drug-drug interactions with pangenotypic direct-acting antivirals for hepatitis C and real-world care management in the United States: A retrospective observational study. J. Manag. Care Spéc. Pharm. 2021, 27, 1239–1248. [Google Scholar] [CrossRef] [PubMed]
- Mangia, A.; Piazzolla, V.; Giannelli, A.; Visaggi, E.; Minerva, N.; Palmieri, V.; Carraturo, I.; Potenza, D.; Napoli, N.; Lauletta, G.; et al. SVR12 rates higher than 99% after sofosbuvir/velpatasvir combination in HCV infected patients with F0-F1 fibrosis stage: A real world experience. PLoS ONE 2019, 14, e0215783. [Google Scholar] [CrossRef]
- Fitch, K.; Bernstein, S.J.; Aguilar, M.D.; Burnand, B.; LaCalle, J.R. The RAND/UCLA Appropriateness Method User’s Manual; RAND Corporation: Santa Monica, CA, USA, 2001; Available online: https://www.rand.org/pubs/monograph_reports/MR1269.html (accessed on 6 August 2022).
- Diamond, I.R.; Grant, R.C.; Feldman, B.M.; Pencharz, P.B.; Ling, S.C.; Moore, A.M.; Wales, P.W. Defining consensus: A systematic review recommends methodologic criteria for reporting of Delphi studies. J. Clin. Epidemiol. 2014, 67, 401–409. [Google Scholar] [CrossRef] [PubMed]
- Linstone, H.; Turoff, M. (Eds.) The Delphi Method. Techniques and Applications; Addison-Wesley Publishing Company: Reading, MA, USA, 1995; pp. 1–616. [Google Scholar]
- Jones, J.; Hunter, D. Qualitative Research: Consensus methods for medical and health services research. BMJ 1995, 311, 376–380. [Google Scholar] [CrossRef] [PubMed]
- Rowe, G.; Wright, G. The Delphi technique as a forecasting tool: Issues and analysis. Int. J. Forecast. 1999, 15, 353–375. [Google Scholar] [CrossRef]
- Graham, B.; Regehr, G.; Wright, J.G. Delphi as a method to establish consensus for diagnostic criteria. J. Clin. Epidemiol. 2003, 56, 1150–1156. [Google Scholar] [CrossRef] [PubMed]
- Vermehren, J.; Park, J.S.; Jacobson, I.M.; Zeuzem, S. Challenges and perspectives of direct antivirals for the treatment of hepatitis C virus infection. J. Hepatol. 2018, 69, 1178–1187. [Google Scholar] [CrossRef] [PubMed]
- Weng, T.-C.; Yang, Y.-H.K.; Lin, S.-J.; Tai, S.-H. A systematic review and meta-analysis on the therapeutic equivalence of statins. J. Clin. Pharm. Ther. 2010, 35, 139–151. [Google Scholar] [CrossRef] [PubMed]
- Tavazzi, L. Observational research as a platform for evidence-based public health policies and learning health systems. Eur. Heart J. 2017, 38, 1891–1894. [Google Scholar] [CrossRef] [PubMed]
- Daskalopoulou, S.S.; Delaney, J.A.; Filion, K.B.; Brophy, J.M.; Mayo, N.E.; Suissa, S. Discontinuation of statin therapy following an acute myocardial infarction: A population-based study. Eur. Heart J. 2008, 29, 2083–2091. [Google Scholar] [CrossRef] [PubMed]
- Colivicchi, F.; Bassi, A.; Santini, M.; Caltagirone, C. Discontinuation of statin therapy and clinical outcome after ischemic stroke. Stroke 2007, 38, 2652–2657. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.-H.; Nie, Q.-H.; Zhao, X.-T. Drug–drug interactions of newly approved direct-acting antiviral agents in patients with hepatitis c. Int. J. Gen. Med. 2021, 14, 289–301. [Google Scholar] [CrossRef] [PubMed]
- Di Perri, G.; Cariti, G. Drug-drug interactions in anti-hcv therapy: A comparison among options available in Italy. Infez. Med. 2019, 27, 239–250. [Google Scholar] [PubMed]
- Ahmed, A.; Schriever, C.; Britt, N.; Yager, J.; Amin, R.; Mcguey, L.; Patel, N. Comparing drug interaction frequencies of various hepatitis C treatment regimens among monoinfected patients. Ann. Hepatol. 2019, 18, 601–606. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| n = 14 | |
|---|---|
| Age, years (median, min–max) | 61, 41–71 |
| Overall working experience, years (median, min–max) | 35, 17–46 |
| Field of prevalent activity | |
| Cardiology (n) | 3 |
| Hepatology (n) | 8 |
| Other (n) | 3 |
| Experience in the Field of prevalent activity, years (median, min–max) | 28.5, 7–35 |
| Geographical area | |
| North (n) | 4 |
| Center (n) | 6 |
| South Islands (n) | 4 |
| Questionnaire | Item | Median | IQR | IPRAS | Evaluation |
|---|---|---|---|---|---|
| Q1 | 7. In cases of concomitant HCV infection and CVD, discontinuation of antihypertensives, even if for 8–12 weeks, may result in increased pressor variability and thus increased risk of developing cardiovascular complications. | 9 | 1.8 | 7.5 | Appropriate |
| Q1 | 8. In cases of concomitant HCV infection and CVD, replacing antihypertensives, even if for 8–12 weeks, with a drug that is not equally potent may result in increased pressor variability and thus increased risk of developing cardiovascular complications. | 7 | 2.0 | 5.4 | Appropriate |
| Q1 | 9. In the case of concomitant HCV infection and CVD, changing the dosage of current antihypertensive medication may result in increased pressor variability and thus increased risk of developing cardiovascular complications. | 7 | 2.0 | 5.4 | Appropriate |
| Q1 | 10. In the case of concurrent HCV infection and CVD, discontinuation of statins, even if for 8–12 weeks, may result in an increased risk of developing cardiovascular complications. | 8 | 2.8 | 5.4 | Appropriate |
| Q1 | 11. In the case of concomitant HCV infection and CVD, replacing statins, even if for 8–12 weeks, with a drug that is not equally potent may result in an increased risk of developing cardiovascular complications. | 8 | 2.0 | 5.4 | Appropriate |
| Q1 | 12. In the case of concurrent HCV infection and CVD, changing the dosage of ongoing statins may result in an increased risk of developing cardiovascular complications. | 7 | 2.0 | 5.4 | Appropriate |
| Q1 | 13. In case of concomitant HCV infection and CVD, discontinuation of DOACs, even for 8–12 weeks, may result in an increased risk of developing cardiovascular complications. | 9 | 0.8 | 8.3 | Appropriate |
| Q1 | 14. In the case of concomitant HCV infection and CVD, replacing DOACs, even if for 8–12 weeks, with a drug that is not equally potent may result in an increased risk of developing cardiovascular complications. | 8 | 1.0 | 6.1 | Appropriate |
| Q1 | 15. In the case of concurrent HCV infection and CVD, changing the dosage of ongoing DOACs may result in an increased risk of developing cardiovascular complications. | 8 | 1.8 | 6.2 | Appropriate |
| Q1 | 16. For the management of hypertension in the HCV patient, ACE inhibitors should be given only as needed and preferably in combination with sofosbuvir/velpatasvir (SOF/VEL) and not in combination with glecaprevir/pibrentasvir (GLE/PIB). | 6 | 2.8 | 5.4 | Uncertain |
| Q1 | 17. In the case of combination therapy with antihypertensives, the choice of SOF/VEL appears to be the most effective and safe choice. | 8 | 1.0 | 6.1 | Appropriate |
| Q1 | 19. In case of polypharmacotherapy, it is important not to change the full doses of the current drug by favoring the choice of the antiviral with less interference. | 9 | 0.0 | 8.4 | Appropriate |
| Q1 | 20. Cardiovascular risk assessment through risk maps should take into account the latest evidence, considering additional elements such as modifiers and comorbidities. | 9 | 1.0 | 7.6 | Appropriate |
| Q1 | 21. The profile of drug interactions between HCV antiviral drugs and the main statins used is similar. | 2 | 4.3 | 6.6 | Inappropriate |
| Q1 | 22. Discontinuation of statin use for 8–12 weeks does not result in a significant increase in CVD risk in primary prevention. | 6 | 5.5 | 2.4 | Uncertain |
| Q1 | 23. Discontinuation of statin use for 8–12 weeks can also be tolerated in secondary prevention | 2 | 4.3 | 6.6 | Inappropriate |
| Q1 | 24. Management of drug interactions with HCV antiviral drugs is simple and does not require special multidisciplinary approaches. | 2 | 2.8 | 6.8 | Inappropriate |
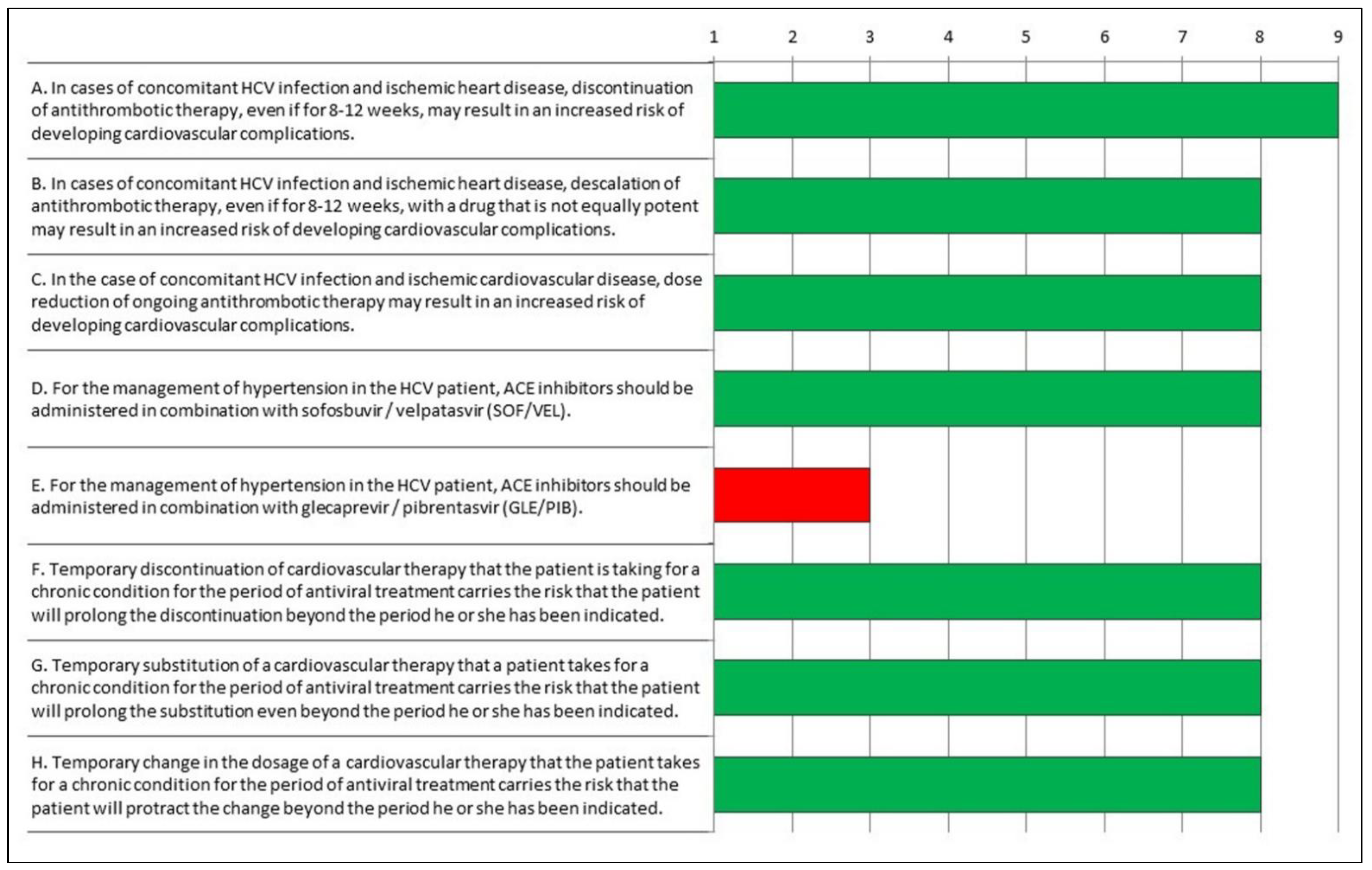
| Q2 | A. In cases of concomitant HCV infection and ischemic heart disease, discontinuation of antithrombotic therapy, even if for 8–12 weeks, may result in an increased risk of developing cardiovascular complications. | 9 | 1.0 | 7.6 | Appropriate |
| Q2 | B. In cases of concomitant HCV infection and ischemic heart disease, descalation of antithrombotic therapy, even if for 8–12 weeks, with a drug that is not equally potent may result in an increased risk of developing cardiovascular complications. | 8 | 1.0 | 6.1 | Appropriate |
| Q2 | C. In the case of concomitant HCV infection and ischemic cardiovascular disease, dose reduction of ongoing antithrombotic therapy may result in an increased risk of developing cardiovascular complications. | 8 | 1.8 | 6.0 | Appropriate |
| Q2 | D. For the management of hypertension in the HCV patient, ACE inhibitors should be administered in combination with sofosbuvir/velpatasvir (SOF/VEL). | 8 | 3.0 | 6.1 | Appropriate |
| Q2 | E. For the management of hypertension in the HCV patient, ACE inhibitors should be administered in combination with glecaprevir/pibrentasvir (GLE/PIB). | 3 | 3.8 | 4.5 | Inappropriate |
| Q2 | F. Temporary discontinuation of cardiovascular therapy that the patient is taking for a chronic condition for the period of antiviral treatment carries the risk that the patient will prolong the discontinuation beyond the period he or she has been indicated. | 8 | 1.8 | 6.2 | Appropriate |
| Q2 | G. Temporary substitution of a cardiovascular therapy that a patient takes for a chronic condition for the period of antiviral treatment carries the risk that the patient will prolong the substitution even beyond the period he or she has been indicated. | 8 | 2.5 | 6.0 | Appropriate |
| Q2 | H. Temporary change in the dosage of a cardiovascular therapy that the patient takes for a chronic condition for the period of antiviral treatment carries the risk that the patient will protract the change beyond the period he or she has been indicated. | 8 | 2.5 | 6.0 | Appropriate |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borghi, C.; Ciancio, A.; Gentile, I.; Perrone Filardi, P.; Pasqualetti, P.; Brillanti, S. Evaluation of Drug Interactions in Patients Treated with DAAs for Hepatitis C Therapy with Comorbidities and Cardiovascular Issues—A Delphi Consensus Project. J. Clin. Med. 2022, 11, 6946. https://doi.org/10.3390/jcm11236946
Borghi C, Ciancio A, Gentile I, Perrone Filardi P, Pasqualetti P, Brillanti S. Evaluation of Drug Interactions in Patients Treated with DAAs for Hepatitis C Therapy with Comorbidities and Cardiovascular Issues—A Delphi Consensus Project. Journal of Clinical Medicine. 2022; 11(23):6946. https://doi.org/10.3390/jcm11236946
Chicago/Turabian StyleBorghi, Claudio, Alessia Ciancio, Ivan Gentile, Pasquale Perrone Filardi, Patrizio Pasqualetti, and Stefano Brillanti. 2022. "Evaluation of Drug Interactions in Patients Treated with DAAs for Hepatitis C Therapy with Comorbidities and Cardiovascular Issues—A Delphi Consensus Project" Journal of Clinical Medicine 11, no. 23: 6946. https://doi.org/10.3390/jcm11236946
APA StyleBorghi, C., Ciancio, A., Gentile, I., Perrone Filardi, P., Pasqualetti, P., & Brillanti, S. (2022). Evaluation of Drug Interactions in Patients Treated with DAAs for Hepatitis C Therapy with Comorbidities and Cardiovascular Issues—A Delphi Consensus Project. Journal of Clinical Medicine, 11(23), 6946. https://doi.org/10.3390/jcm11236946