
The Role of Predictive Models in the Assessment of the Poor Outcomes in Pediatric Acute Liver Failure

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
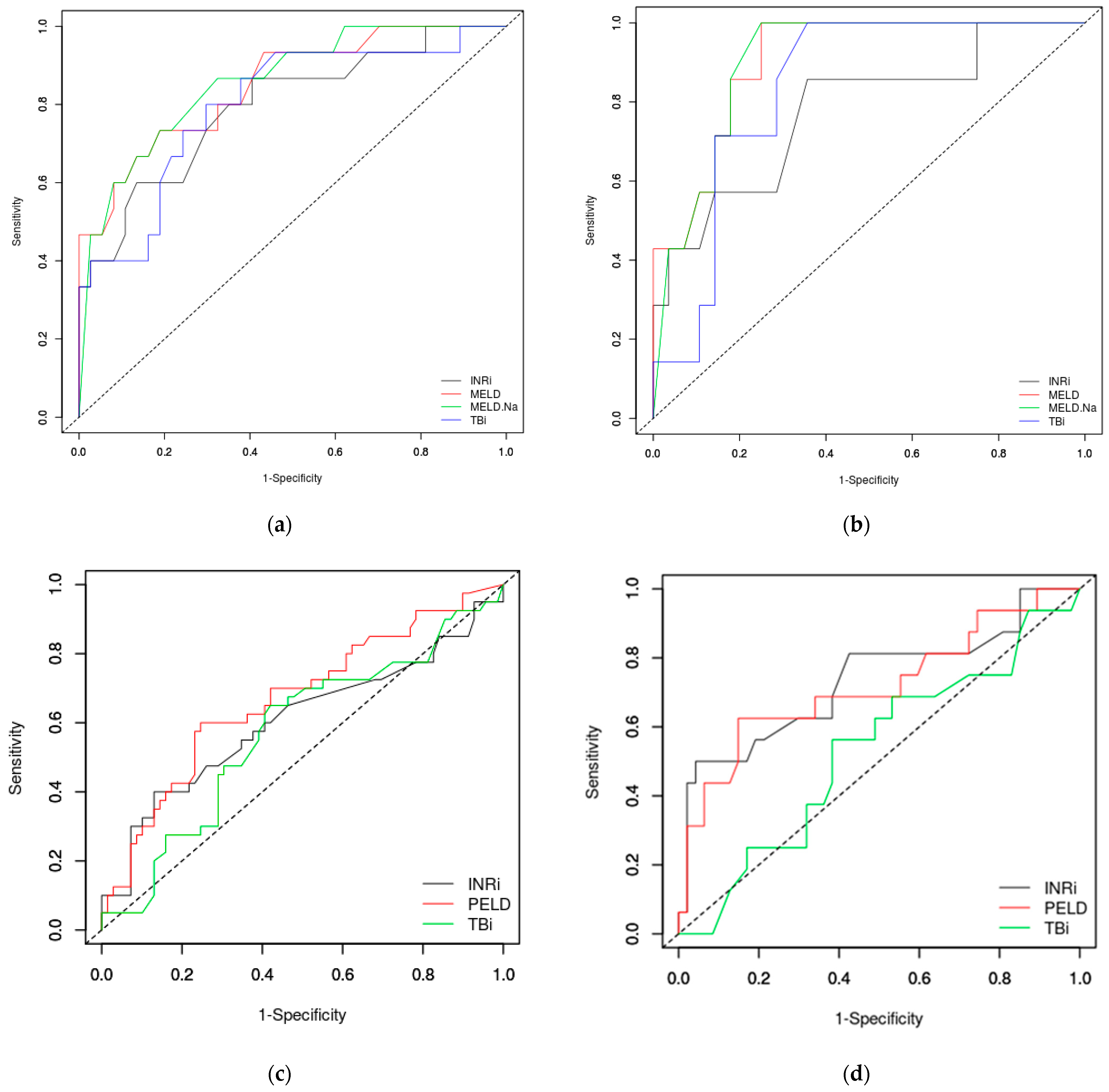
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jain, V.; Dhawan, A. Prognostic modeling in pediatric acute liver failure. Liver Transpl. 2016, 22, 1418–1430. [Google Scholar] [CrossRef]
- Sokol, J.R.; Narkewicz, R.M. Liver and pancreas. In Current Diagnosis & Treatment Paediatrics, 20th ed.; Hay, W.W., Levin, J.M., Sondheimer, M.J., Deterding, R.R., Eds.; Mc Graw Hill Education: New York, NY, USA, 2011; pp. 631–651. [Google Scholar]
- Gilbert Pérez, J.J.; Jordano Moreno, B.; Rodríguez Salas, M. Aetiology, outcomes and prognostic indicators of paediatric acute liver failure. An. Pediatr. (Engl. Ed.) 2018, 88, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Devictor, D.; Tissieres, P.; Durand, P.; Chevret, L.; Debray, D. Acute liver failure in neonates, infants and children. Expert Rev. Gastroenterol. Hepatol. 2011, 5, 717–729. [Google Scholar] [CrossRef] [PubMed]
- Devictor, D.; Tissieres, P.; Afanetti, M.; Debray, D. Acute liver failure in children. Clin. Res. Hepatol. Gastroenterol. 2011, 35, 430–437. [Google Scholar] [CrossRef] [PubMed]
- Grama, A.; Aldea, C.O.; Burac, L.; Delean, D.; Bulata, B.; Sirbe, C.; Duca, E.; Boghitoiu, D.; Coroleuca, A.; Pop, T.L. Etiology and outcome of acute liver failure in children—The experience of a single tertiary care hospital from Romania. Children 2020, 7, 282. [Google Scholar] [CrossRef] [PubMed]
- Squires, J.E.; McKiernan, P.; Squires, R.H. Acute liver failure: An update. Clin. Liver Dis. 2018, 22, 773–805. [Google Scholar] [CrossRef]
- Kathemann, S.; Bechmann, L.P.; Sowa, J.P.; Manka, P.; Dechêne, A.; Gerner, P.; Lainka, E.; Hoyer, P.F.; Feldstein, A.E.; Canbay, A. Etiology, outcome and prognostic factors of childhood acute liver failure in a German single center. Ann. Hepatol. 2015, 14, 722–728. [Google Scholar] [CrossRef]
- Lee, W.S.; McKiernan, P.; Kelly, D.A. Etiology, outcome and prognostic indicators of childhood fulminant hepatic failure in the United Kingdom. J. Pediatr. Gastroenterol. Nutr. 2005, 40, 575–581. [Google Scholar] [CrossRef]
- Squires, R.H. Acute liver failure in children. Semin. Liver Dis. 2008, 28, 153–166. [Google Scholar] [CrossRef]
- Saluja, V.; Sharma, A.; Pasupuleti, S.S.; Mitra, L.G.; Kumar, G.; Agarwal, P.M. Comparison of prognostic models in acute liver failure: Decision is to be dynamic. Indian J. Crit. Care Med. 2019, 23, 574–581. [Google Scholar] [CrossRef]
- Sanchez, M.C.; D’Agostino, D.E. Pediatric end-stage liver disease score in acute liver failure to assess poor prognosis. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 193–196. [Google Scholar] [CrossRef]
- Batra, Y.; Acharya, S.K. Acute liver failure: Prognostic markers. Indian J. Gastroenterol. 2003, 22, 66–86. [Google Scholar]
- Bhatia, V.; Bavdekar, A. Management of acute liver failure in infants and children: Consensus statement of the pediatric gastroenterology chapter, Indian academy of pediatrics. Indian Pediatr. 2013, 50, 477–482. [Google Scholar] [CrossRef]
- Whitington, P.F.; Alonso, E.M. Fulminant hepatitis and acute liver failure. In Diseases of the Liver and Biliary System in Children, 2nd ed.; Deirdre, K., Ed.; Wiley-Blackwell: Oxford, UK, 2003; pp. 107–126. [Google Scholar] [CrossRef]
- Shneider, B.L. To transplant or not to transplant: Certainly one of the questions. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 164. [Google Scholar] [CrossRef] [PubMed]
- Wlodzimirow, K.A.; Eslami, S.; Chamuleau, R.A.F.M.; Nieuwoudt, M.; Abu-Hanna, A. Prediction of poor outcome in patients with acute liver failure-systematic review of prediction models. PLoS ONE 2012, 7, 50952. [Google Scholar] [CrossRef] [PubMed]
- Samuel, D.; Ichai, P. Prognosis indicator in acute liver failure: Is there a place for cell death markers? J. Hepatol. 2010, 53, 593–595. [Google Scholar] [CrossRef] [PubMed][Green Version]
- D’Agostino, D.; Diaz, S.; Sanchez, M.C.; Boldrini, G. Management and prognosis of acute liver failure in children. Curr. Gastroenterol. Rep. 2012, 14, 262–269. [Google Scholar] [CrossRef]
- Lu, B.R.; Zhang, S.; Narkewicz, M.R.; Belle, S.H.; Squires, R.H.; Sokol, R.J. Evaluation of the liver injury unit scoring system to predict survival in a multinational study of pediatric acute liver failure. J. Pediatr. 2013, 162, 1010–1016.e4. [Google Scholar] [CrossRef]
- Mishra, A.; Rustgi, V. Prognostic models in acute liver failure. Clin. Liver Dis. 2018, 22, 375–388. [Google Scholar] [CrossRef]
- Bansai, S.; Dhawan, A. Acute liver failure. Curr. Pediatr. 2006, 16, 36–42. [Google Scholar] [CrossRef]
- Bernal, W.; Auzinger, G.; Dhawan, A.; Wendon, J. Acute liver failure. Lancet 2010, 376, 190–201. [Google Scholar] [CrossRef]
- Bernuau, J.; Rueff, B.; Benhamou, J.P. Fulminant and subfulminant liver failure: Definitions and causes. Semin. Liver Dis. 1986, 6, 97–106. [Google Scholar] [CrossRef] [PubMed]
- Grama, A.; Burac, L.; Aldea, C.O.; Bulata, B.; Delean, D.; Samasca, G.; Abrudan, C.; Sirbe, C.; Pop, T.L. Vitamin D-binding protein (Gc-Globulin) in acute liver failure in children. Diagnostics 2020, 10, 278. [Google Scholar] [CrossRef] [PubMed]
- Du, W.B.; Pan, X.P.; Li, L.J. Prognostic models for acute liver failure. Hepatobiliary Pancreat. Dis. Int. 2010, 9, 122–128. [Google Scholar] [PubMed]
- Bhatia, V.; Singh, R.; Acharya, S.K. Predictive value of arterial ammonia for complications and outcome in acute liver failure. Gut 2006, 55, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Bernal, W.; Wendon, J. Acute liver failure. N. Engl. J. Med. 2013, 369, 2525–2534. [Google Scholar] [CrossRef] [PubMed]
- Ayoub, B.A.H.; Ali, M.A.H.; Salem, T.A.H.; Rizk, M.S.; Nagi, S.A.M.; Adawy, N.M. Pediatric chronic liver failure-sequential organ failure assessment score and outcome of acute liver failure in children. Clin. Exp. Hepatol. 2020, 6, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Tissières, P.; Prontera, W.; Chevret, L.; Devictor, D. The pediatric risk of mortality score in infants and children with fulminant liver failure. Pediatr. Transplant. 2003, 7, 64–68. [Google Scholar] [CrossRef]
- O’Grady, J.G. Prognostication in acute liver failure: A tool or an anchor? Liver Transpl. 2007, 13, 786–787. [Google Scholar] [CrossRef]
- Vulturar, R.; Nicolescu, A.; Pop, T.; Deleanu, C. NMR Spectroscopy as a tool in differential diagnosis, our experience in a patient suspected for tyrosinemia type I. J. Inherit. Metab. Dis. 2015, 38, S144. [Google Scholar]
- Vulturar, R.; Nicolescu, A.; Pop, T.L.; Tatar, S.; Deleanu, C. Biochemical and clinical aspects in several patients with galactose-1-phosphate uridyl transferase deficiency. J. Inherit. Metab. Dis. 2016, 39, 148. [Google Scholar]
- McDiarmid, S.V.; Anand, R.; Lindblad, A.S.; Principal investigators and institutions of the studies of pediatric liver transplantation (SPLIT) research group. Development of a pediatric end-stage liver disease score to predict poor outcome in children awaiting liver transplantation. Transplantation 2002, 74, 173–181. [Google Scholar] [CrossRef]
- Kamath, P.S.; Wiesner, R.H.; Malinchoc, M.; Kremers, W.; Therneau, T.M.; Kosberg, C.L.; D’Amico, G.; Dickson, E.R.; Kim, W.R. A model to predict survival in patients with end-stage liver disease. Hepatology 2001, 33, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Ruf, A.E.; Kremers, W.K.; Chavez, L.L.; Descalzi, V.I.; Podesta, L.G.; Villamil, F.G. Addition of serum sodium into the MELD score predicts waiting list mortality better than MELD alone. Liver Transpl. 2005, 11, 336–343. [Google Scholar] [CrossRef] [PubMed]
- Sundaram, V.; Shneider, B.L.; Dhawan, A.; Ng, V.L.; Im, K.; Belle, S.; Squires, R.H. King’s college hospital criteria for non-acetaminophen induced acute liver failure in an international cohort of children. J. Pediatr. 2013, 162, 319–323.e1. [Google Scholar] [CrossRef] [PubMed]
- Nazer, H.; Ede, R.J.; Mowat, A.P.; Williams, R. Wilson’s disease: Clinical presentation and use of prognostic index. Gut 1986, 27, 1377–1381. [Google Scholar] [CrossRef]
- Dhawan, A.; Taylor, R.M.; Cheeseman, P.; de Silva, P.; Katsiyiannakis, L.; Mieli-Vergani, G. Wilson’s disease in children: 37-year experience and revised King’s for liver transplantation. Liver Transpl. 2005, 11, 441–448. [Google Scholar] [CrossRef]
- Goksuluk, D.; Korkmaz, S.; Zararsiz, G.; Karaagaoglu, A.E. EasyROC: An interactive web-tool for roc curve analysis using r language environment. R J. 2016, 8, 213–230. [Google Scholar] [CrossRef]
- Cholongitas, E.; Theocharidou, E.; Vasianopoulou, P.; Betrosian, A.; Shaw, S.; Patch, D.; O’Beirne, J.; Agarwal, B.; Burroughs, A.K. Comparison of the sequential organ failure assessment score with the King’s college hospital criteria and the model for end-stage liver disease score for the prognosis of acetaminophen-induced acute liver failure. Liver Transpl. 2012, 18, 405–412. [Google Scholar] [CrossRef]
- Rivera-Penera, T.; Moreno, J.; Skaff, C.; McDiarmid, S.; Vargas, J.; Ament, M.E. Delayed encephalopathy in fulminant hepatic failure in the pediatric population and the role of liver transplantation. J. Pediatr. Gastroenterol. Nutr. 1997, 24, 128–134. [Google Scholar] [CrossRef]
- Mochida, S.; Nakayama, N.; Matsui, A.; Nagoshi, S.; Fujiwara, K. Re-evaluation of the guideline published by the acute liver failure study group of Japan in 1996 to determine the indications of liver transplantation in patients with fulminant hepatitis. Hepatol. Res. 2008, 38, 970–979. [Google Scholar] [CrossRef]
- Ciocca, M.; Ramonet, M.; Cuarterolo, M.; López, S.; Cernadas, C.; Álvarez, F. Prognostic factors in paediatric acute liver failure. Arch. Dis. Child 2008, 93, 48–51. [Google Scholar] [CrossRef]
- Dhiman, R.K.; Jain, S.; Maheshwari, U.; Bhalla, A.; Sharma, N.; Ahluwalia, J.; Duseja, A.; Chawla, Y. Early indicators of prognosis in fulminant hepatic failure: An assessment of the model for end-stage liver disease (MELD) and King’s college hospital criteria. Liver Transpl. 2007, 13, 814–821. [Google Scholar] [CrossRef] [PubMed]
- Stravitz, R.T.; Ellerbe, C.; Durkalski, V.; Reuben, A.; Lisman, T.; Lee, W.M. Thrombocytopenia is associated with multi-organ system failure in patients with acute liver failure. Clin. Gastroenterol. Hepatol. 2016, 14, 613–620.e4. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Dong, R.; Chen, G.; Dong, K.; Zheng, S. Risk factors and prognostic effects of cholangitis after Kasai procedure in biliary atresia patients: A retrospective clinical study. J. Pediatr. Surg. 2019, 54, 2559–2564. [Google Scholar] [CrossRef] [PubMed]
- Schiødt, F.V. Gc-globulin in liver disease. Dan. Med. Bull. 2008, 55, 131–146. [Google Scholar] [PubMed]
- Schiodt, F.V.; Bondesen, S.; Tygstrup, N. Serial measurements of serum Gc-globilin in acetaminophen intoxication. Eur. J. Gastroenterol. Hepatol. 1995, 7, 635–640. [Google Scholar] [PubMed]
- Schiødt, F.V.; Ott, P.; Tygstrup, N.; Dahl, B.; Bondesen, S. Temporal profile of total, bound, and free Gc-globulin after acetaminophen overdose. Liver Transpl. 2001, 7, 732–738. [Google Scholar] [CrossRef] [PubMed]
- Schiødt, F.V.; Bondesen, S.; Petersen, I.; Dalhoff, K.; Ott, P.; Tygstrup, N. Admission levels of serum Gc-globulin: Redictive value in fulminant hepatic failure. Hepatology 1996, 23, 713–718. [Google Scholar] [CrossRef] [PubMed]
- Schiødt, F.V.; Rossaro, L.; Stravitz, R.T.; Shakil, A.O.; Chung, R.T.; Lee, W.M. Gc-globulin and prognosis in acute liver failure. Liver Transpl. 2005, 11, 1223–1227. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, L.E.; Dalhoff, K. Serum phosphate is an early predictor of outcome in severe acetaminophen-induced hepatotoxicity. Hepatology 2002, 36, 659–665. [Google Scholar] [CrossRef]
- Craig, D.G.N.; Ford, A.C.; Hayes, P.C.; Simpson, K.J. Systematic review: Prognostic tests of paracetamol-induced acute liver failure. Aliment. Pharmacol. Ther. 2010, 31, 1064–1076. [Google Scholar] [CrossRef]
- Rosen, H.R.; Biggins, S.W.; Niki, T.; Gralla, J.; Hillman, H.; Hirashima, M.; Schilsky, M.; Lee, W.M.; Acute liver failure study group. Association between plasma level of galectin-9 and survival of patients with drug-induced acute liver failure. Clin. Gastroenterol. Hepatol. 2016, 14, 606–612.e3. [Google Scholar] [CrossRef] [PubMed]
- Craig, D.G.; Simpson, K.J. Accuracy of the ALFSG index as a triage marker in acute liver failure. Gastroenterology 2013, 144, e25. [Google Scholar] [CrossRef] [PubMed]
- Dhawan, A.; Cheeseman, P.; Mieli-Vergani, G. Approaches to acute liver failure in children. Pediatr. Transplant. 2004, 8, 584–588. [Google Scholar] [CrossRef] [PubMed]
- Rajanayagam, J.; Coman, D.; Cartwright, D.; Lewindon, P.J. Pediatric acute liver failure: Etiology, outcomes, and the role of serial pediatric end-stage liver disease scores. Pediatr. Transplant. 2013, 17, 362–368. [Google Scholar] [CrossRef] [PubMed]
- Durand, P.; Debray, D.; Mandel, R.; Baujard, C.; Branchereau, S.; Gauthier, F.; Jacquemin, E.; Devictor, D. Acute liver failure in infancy: A 14-year experience of a pediatric liver transplantation center. J. Pediatr. 2001, 139, 871–876. [Google Scholar] [CrossRef]
- Rajanayagam, J.; Frank, E.; Shepherd, R.W.; Lewindon, P.J. Artificial neural network is highly predictive of outcome in paediatric acute liver failure. Pediatr. Transplant. 2013, 17, 535–542. [Google Scholar] [CrossRef]
- McPhail, M.J.W.; Wendon, J.A.; Bernal, W. Meta-analysis of performance of King’s college hospital criteria in prediction of outcome in non-paracetamol-induced acute liver failure. J. Hepatol. 2010, 53, 492–499. [Google Scholar] [CrossRef]
- Bernal, W.; Williams, R. Beyond KCH selection and options in acute liver failure. Hepatol. Int. 2018, 12, 204–213. [Google Scholar] [CrossRef]
- Panchal, H.J.; Durinka, J.B.; Patterson, J.; Karipineni, F.; Ashburn, S.; Siskind, E.; Ortiz, J. Survival outcomes in liver transplant recipients with model for end-stage liver disease scores of 40 or higher: A decade-long experience. HPB (Oxford) 2015, 17, 1074–1084. [Google Scholar] [CrossRef]
- Figorilli, F.; Putignano, A.; Roux, O.; Houssel-Debry, P.; Francoz, C.; Paugam-Burtz, C.; Soubrane, O.; Agarwal, B.; Durand, F.; Jalan, R. Development of an organ failure score in acute liver failure for transplant selection and identification of patients at high risk of futility. PLoS ONE 2017, 12, 188151. [Google Scholar] [CrossRef]
- Levesque, E.; Hoti, E.; Azoulay, D.; Ichaï, P.; Habouchi, H.; Castaing, D.; Samuel, D.; Saliba, F. Prospective evaluation of the prognostic scores for cirrhotic patients admitted to an Intensive Care Unit. J. Hepatol. 2012, 56, 95–102. [Google Scholar] [CrossRef]
- Barshes, N.R.; Lee, T.C.; Udell, I.W.; O’Mahoney, C.A.; Karpen, S.J.; Carter, B.A.; Goss, J.A. The pediatric end-stage liver disease (PELD) model as a predictor of survival benefit and posttransplant survival in pediatric liver transplant recipients. Liver Transpl. 2006, 12, 475–480. [Google Scholar] [CrossRef]
- Núñez-Ramos, R.; Montoro, S.; Bellusci, M.; Del Fresno-Valencia, M.R.; Germán-Díaz, M.; Urruzuno, P.; Medina, E.; Manzanares, J. Acute liver failure: Outcome and value of pediatric end-stage liver disease score in pediatric cases. Pediatr. Emerg. Care 2018, 34, 409–412. [Google Scholar] [CrossRef]
- Yantorno, S.E.; Kremers, W.K.; Ruf, A.E.; Trentadue, J.J.; Podestá, L.G.; Villamil, F.G. MELD is superior to King’s college and Clichy’s criteria to assess prognosis in fulminant hepatic failure. Liver Transpl. 2007, 13, 822–828. [Google Scholar] [CrossRef]
- McPhail, M.J.W.; Farne, H.; Senvar, N.; Wendon, J.A.; Bernal, W. Ability of King’s college criteria and model for end-stage liver disease scores to predict mortality of patients with acute liver failure: A meta-analysis. Clin. Gastroenterol. Hepatol. 2016, 14, 516–525.e5. [Google Scholar] [CrossRef] [PubMed]
- Ng, V.L.; Li, R.; Loomes, K.M.; Leonis, M.A.; Rudnick, D.A.; Belle, S.H.; Squires, R.H. Pediatric acute liver failure study group (PALFSG). Outcomes of children with and without hepatic encephalopathy from the pediatric acute liver failure study group. J. Pediatr. Gastroenterol. Nutr. 2016, 63, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, L.E.; Larsen, F.S. Prognostic implications of hyperlactatemia, multiple organ failure, and systemic inflammatory response syndrome in patients with acetaminophen-induced acute liver failure. Crit. Care Med. 2006, 34, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Lee, H.J.; Ryoo, S.M.; Ahn, S.; Sohn, C.H.; Seo, D.W.; Lim, K.S.; Kim, W.Y. Prognostic value of decision criteria for emergency liver transplantation in patients with wild mushroom induced acute liver injury. Hepatobiliary Pancreat. Dis. Int. 2018, 17, 210–213. [Google Scholar] [CrossRef] [PubMed]
- Ganzert, M.; Felgenhauer, N.; Zilker, T. Indication of liver transplantation following amatoxin intoxication. J. Hepatol. 2005, 42, 202–209. [Google Scholar] [CrossRef]
- Escudié, L.; Francoz, C.; Vinel, J.P.; Moucari, R.; Cournot, M.; Paradis, V.; Sauvanet, A.; Belghiti, J.; Valla, D.; Bernuau, J.; et al. Amanita phalloides poisoning: Reassessment of prognostic factors and indications for emergency liver transplantation. J. Hepatol. 2007, 46, 466–473. [Google Scholar] [CrossRef] [PubMed]
- Stefanescu, A.; Pop, T.; Stefanescu, H.; Feier, D.; Bizo, A.; Miu, N. 1012 serum creatinine and the presence of encephalopathy at presentation may predict mortality in children with acute liver failure. J. Hepatol. 2013, 58, S417. [Google Scholar] [CrossRef]
- Pop, T.L.; Grama, A.; Stefanescu, A.; Delean, D.; Aldea, C.; Bizo, A. PELD score as a prognostic factor in fulminant liver failure caused by mushroom poisoning in children. J. Hepatol. 2016, 64, S304–S305. [Google Scholar] [CrossRef]
- Grama, A.; Aldea, C.; Burac, L.; Delean, D.; Boghitoiu, D.; Bulata, B.; Nitescu, V.; Ulmeanu, C.; Pop, T.L. Acute liver failure secondary to toxic exposure in children. Arch. Med. Sci. 2022, 18. [Google Scholar] [CrossRef]
- Kamath, P.S.; Heimbach, J.; Wiesner, R.H. Acute liver failure prognostic scores: Is good enough good enough? Clin. Gastroenterol. Hepatol. 2016, 14, 621–623. [Google Scholar] [CrossRef][Green Version]
- Sankar, J. Acute physiology and chronic health evaluation II for critically ill children? Indian J. Crit. Care Med. 2015, 19, 446–448. [Google Scholar] [CrossRef]
- Cholongitas, E.B.; Betrossian, A.; Leandro, G.; Shaw, S.; Patch, D.; Burroughs, A.K. King’s criteria, APACHE II, and SOFA scores in acute liver failure. Hepatology 2006, 43, 881. [Google Scholar] [CrossRef]
- Rutherford, A.; King, L.Y.; Hynan, L.S.; Vedvyas, C.; Lin, W.; Lee, W.M.; Chung, R.T.; ALF study group. Development of an accurate index for predicting outcomes of patients with acute liver failure. Gastroenterology 2012, 143, 1237–1243. [Google Scholar] [CrossRef]
- Kumar, R.; Sharma, H.; Goyal, R.; Kumar, A.; Khanal, S.; Prakash, S.; Gupta, S.D.; Panda, S.K.; Acharya, S.K. Prospective derivation and validation of early dynamic model for predicting outcome in patients with acute liver failure. Gut 2012, 61, 1068–1075. [Google Scholar] [CrossRef]
- Oliveira, V.M.; Brauner, J.S.; Rodrigues Filho, E.; Susin, R.G.; Draghetti, V.; Bolzan, S.T.; Vieira, S.R. Is SAPS 3 better than APACHE II at predicting mortality in critically ill transplant patients? Clinics (Sao Paulo Braz.) 2013, 68, 153–158. [Google Scholar] [CrossRef]
- Matthews, C.E.; Goonasekera, C.; Dhawan, A.; Deep, A. Validity of pediatric index of mortality 2 (PIM2) score in pediatric acute liver failure. Crit. Care 2014, 18, 665. [Google Scholar] [CrossRef] [PubMed]
- Lu, B.R.; Gralla, J.; Liu, E.; Dobyns, E.L.; Narkewicz, M.R.; Sokol, R.J. Evaluation of a scoring system for assessing prognosis in pediatric acute liver failure. Clin. Gastroenterol. Hepatol. 2008, 6, 1140–1145. [Google Scholar] [CrossRef]
- Socha, P.; Janczyk, W.; Dhawan, A.; Baumann, U.; D’Antiga, L.; Tanner, S.; Iorio, R.; Vajro, P.; Houwen, R.; Fischler, B.; et al. Wilson’s disease in children: A position paper by the hepatology committee of the European Society for paediatric gastroenterology, hepatology and nutrition. J. Pediatr. Gastroenterol. Nutr. 2018, 66, 334–344. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Survivors with Native Liver under Medical Treatment (n = 106) | Poor Outcome (LT or Deceased) (n = 55) | p-Value |
|---|---|---|---|
| Age (years) | 8.53 ± 5.91 | 5.51 ± 6.43 | 0.003304 |
| Males (n, %) | 45 (42.45%) | 28 (50.91%) | 0.30670 |
| AST (UI/L) | 1 332.02 ± 2 057.03 | 1 028.38 ± 1 779.19 | 0.354363 |
| ALT (UI/L) | 1 051.47 ± 1 305.89 | 699.35 ± 1 229.77 | 0.099954 |
| TB (mg/dL) | 4.40 ± 5.45 | 9.27 ± 12.30 | 0.000663 |
| DB (mg/dL) | 3.26 ± 4.41 | 7.04 ± 10.05 | 0.001158 |
| INR | 2.44 ± 1.21 | 3.76 ± 2.78 | 0.000046 |
| Albumin (mg/dL) | 3.29 ± 0.48 | 2.97 ± 0.71 | 0.000732 |
| Hemoglobin (g/dL) | 10.79 ± 2.26 | 9.36 ± 2.34 | 0.000341 |
| White blood cells (/mm3) | 14 422 ± 21 178 | 14 126 ± 8 990 | 0.921381 |
| Platelets (/mm3) | 198 490 ± 106 904 | 207 418 ± 166 127 | 0.680128 |
| Ceruloplasmin (mg/dL) * | 10.175 ± 5.863 | 7.75 ± 4.179 | 0.52570 |
| Encephalopathy (n, %) | 17 (16.04%) | 28 (50.91%) | <0.00001 |
| Metabolic acidosis (n, %) | 58 (54.72%) | 40 (72.73%) | 0.02637 |
| Acute kidney injury (n, %) | 13 (12.26%) | 27 (49.09%) | <0.00001 |
| Renal replacement (n, %) | 11 (10.38%) | 10 (18.18%) | 0.16317 |
| PELD (n = 109) | 13.99 ± 10.07 | 21.04 ± 13.28 | 0.002282 |
| MELD (n = 52) | 19.51 ± 8.57 | 36.20 ± 13.44 | 0.000002 |
| MELD-Na (n = 52) | 20.08 ± 8.47 | 33.07 ± 8.29 | 0.000006 |
| KCC (n, %) | 6 (5.66%) | 16 (29.09%) | 0.0004 |
| Survivors with Native Liver under Medical Treatment | Poor Outcome (LT or Deceased) | p-Value | |
|---|---|---|---|
| Toxic causes | |||
| PELD | 9.90 ± 7.16 | 25.32 ± 17.16 | 0.003192 |
| MELD | 18.36 ± 9.09 | 37.28 ± 10.73 | 0.000037 |
| MELD-Na | 18.82 ± 8.96 | 34.28 ± 6.02 | 0.000142 |
| Infectious causes | |||
| PELD | 13.63 ± 7.80 | 15.52 ± 9.61 | 0.546069 |
| MELD | 17 ± 4.24 | 26 ± 0 | 0.333333 |
| MELD-Na | 21 ± 7.07 | 26 ± 0 | 0.666667 |
| Autoimmune causes | |||
| PELD | 15.06 ± 6.12 | 14.50 ± 0 | 0.9333 |
| MELD | 23.50 ± 6.89 | ||
| MELD-Na | 24.17 ± 6.55 | ||
| Metabolic causes | |||
| IEM—PELD | 31.92 ± 14.06 | 25.90 ± 16.92 | 0.491631 |
| WD—MELD | 20 ± 0 | 45.80 ± 8.93 | 0.057692 |
| WD—MELD-Na | 21 ± 0 | 39 ± 2.24 | 0.001826 |
| Unknown etiology | |||
| PELD | 5.467 ± 1.955 | 23.544 ± 8.898 | 0.006922 |
| MELD | 21 ± 0 | 19 ± 0 | |
| MELD-Na | 24 ± 0 | 19 ± 0 | |
| Parameter | Cut-Off | Sensitivity | Specificity | PPV | NPV | AUROC |
|---|---|---|---|---|---|---|
| Teenagers (n = 52) | ||||||
| INR | 3 | 60% | 86.5% | 64.3% | 84.2% | 0.7946 |
| TB | 2.3 mg/dL | 80% | 70.3% | 52.2% | 89.7% | 0.7991 |
| MELD | 28 | 73.3% | 81.1% | 61.1% | 88.2% | 0.8495 |
| MELD-Na | 28 | 73.3% | 81.1% | 61.1% | 88.2% | 0.8576 |
| Teenagers with ALF of toxic causes (n = 35) | ||||||
| INR | 2.5 | 85.7% | 64.3% | 37.5% | 94.7% | 0.7781 |
| TB | 1.3 mg/dL | 100% | 64.3% | 41.2% | 100% | 0.8367 |
| MELD | 24 | 100% | 75% | 50% | 100% | 0.9056 |
| MELD-Na | 26 | 100% | 75% | 50% | 100% | 0.9031 |
| Children under 12 years old (n = 109) | ||||||
| INR | 3 | 40% | 87% | 64% | 71.4% | 0.6045 |
| TB | 3.4 mg/dL | 65% | 58% | 47.3% | 74.1% | 0.5725 |
| PELD | 18.9 | 60% | 75.4% | 58.5% | 76.5% | 0.6686 |
| Children under 12 years old—excluding neonates and infants (n = 63) | ||||||
| INR | 3 | 50% | 95.7% | 80% | 84.9% | 0.7334 |
| TB | 4 mg/dL | 56.2% | 61.7% | 33.3% | 80.6% | 0.5286 |
| PELD | 19.5 | 62.5% | 85.1% | 58.8% | 87% | 0.7181 |
| Neonates and infants (n = 46) | ||||||
| INR | 10 | 12.5% | 100% | 100% | 51.2% | 0.4896 |
| TB | 6.6 mg/dL | 54.2% | 77.3% | 72.2% | 60.7% | 0.6146 |
| PELD | 12.9 | 75% | 40.9% | 58.1% | 60% | 0.5511 |
| Accuracy | ||||||
| KCC based on age | ||||||
| Neonates and infants (n = 46) | 25.00% | 77.27% | 54.55% | 48.57% | 50% | |
| Children (n = 63) | 18.75% | 97.87% | 75% | 77.97% | 77.78% | |
| Teenagers (n = 52) | 46.67% | 100% | 100% | 82.22% | 84.61% | |
| KCC based on ALF etiology | ||||||
| Toxic causes (n = 64) | 36.36% | 100% | 100% | 88.33% | 89.06% | |
| Metabolic (n = 27) | 44.44% | 66.67% | 72.73% | 37.50% | 51.85% | |
| Infectious (n = 41) | 0% | 88.46% | 0% | 60.53% | 56.10% | |
| Autoimmune (n = 15) | 0% | 100% | 0% | 93.33% | 93.33% | |
| Unknown (n = 14) | 40% | 100% | 100% | 40% | 57.14% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pop, T.L.; Aldea, C.O.; Delean, D.; Bulata, B.; Boghiţoiu, D.; Păcurar, D.; Ulmeanu, C.E.; Grama, A. The Role of Predictive Models in the Assessment of the Poor Outcomes in Pediatric Acute Liver Failure. J. Clin. Med. 2022, 11, 432. https://doi.org/10.3390/jcm11020432
Pop TL, Aldea CO, Delean D, Bulata B, Boghiţoiu D, Păcurar D, Ulmeanu CE, Grama A. The Role of Predictive Models in the Assessment of the Poor Outcomes in Pediatric Acute Liver Failure. Journal of Clinical Medicine. 2022; 11(2):432. https://doi.org/10.3390/jcm11020432
Chicago/Turabian StylePop, Tudor Lucian, Cornel Olimpiu Aldea, Dan Delean, Bogdan Bulata, Dora Boghiţoiu, Daniela Păcurar, Coriolan Emil Ulmeanu, and Alina Grama. 2022. "The Role of Predictive Models in the Assessment of the Poor Outcomes in Pediatric Acute Liver Failure" Journal of Clinical Medicine 11, no. 2: 432. https://doi.org/10.3390/jcm11020432
APA StylePop, T. L., Aldea, C. O., Delean, D., Bulata, B., Boghiţoiu, D., Păcurar, D., Ulmeanu, C. E., & Grama, A. (2022). The Role of Predictive Models in the Assessment of the Poor Outcomes in Pediatric Acute Liver Failure. Journal of Clinical Medicine, 11(2), 432. https://doi.org/10.3390/jcm11020432