
Therapeutic Anticoagulation Impacts MR Morphologic Recurrence Patterns in Glioblastoma—A Matched-Pair Analysis

 , , , ,
, , , ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Data Collection
2.2. Image Analysis
2.3. Patient Follow-Up
2.4. Statistics
3. Results
4. Discussion
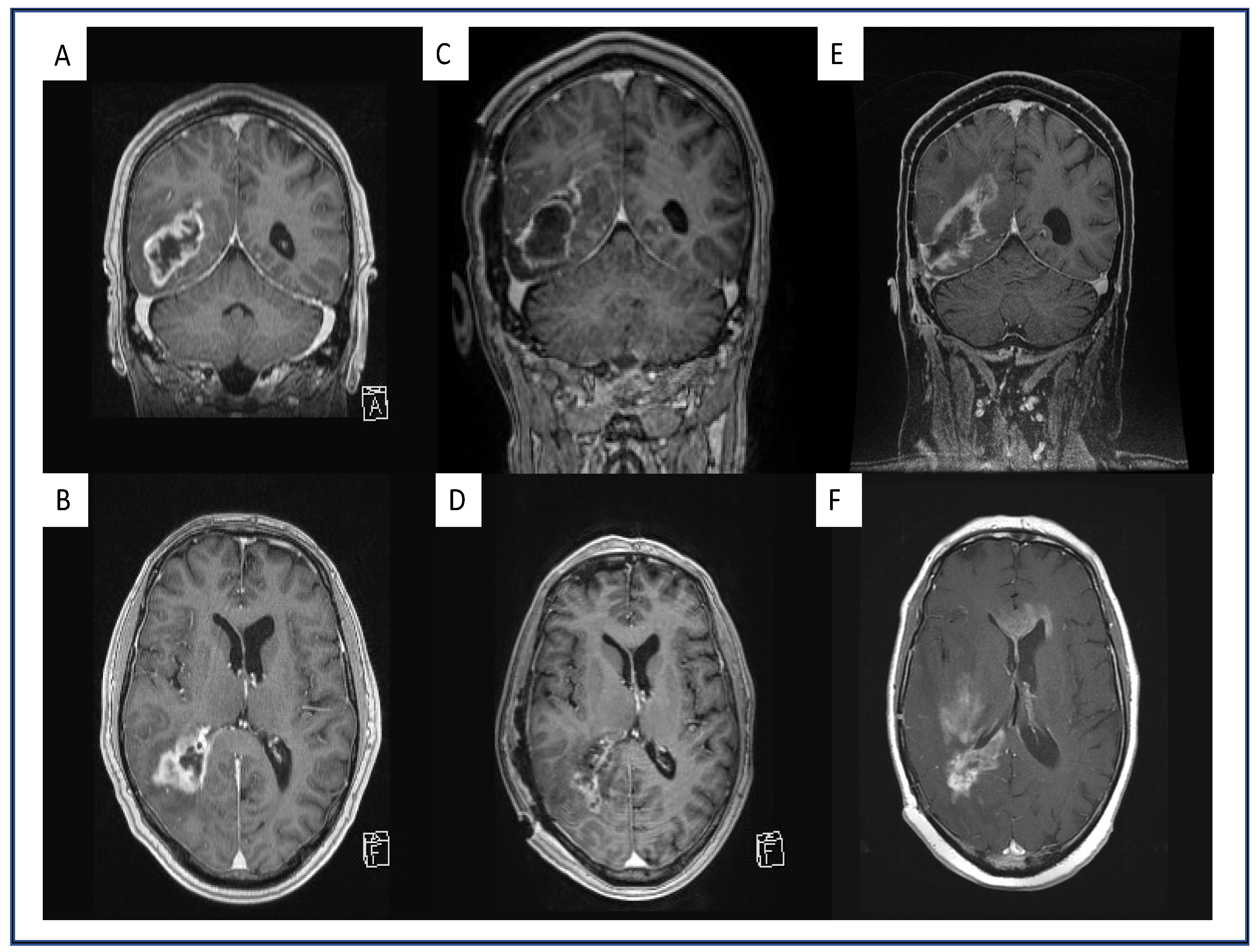
4.1. Multifocal and Midline-Crossing Relapse
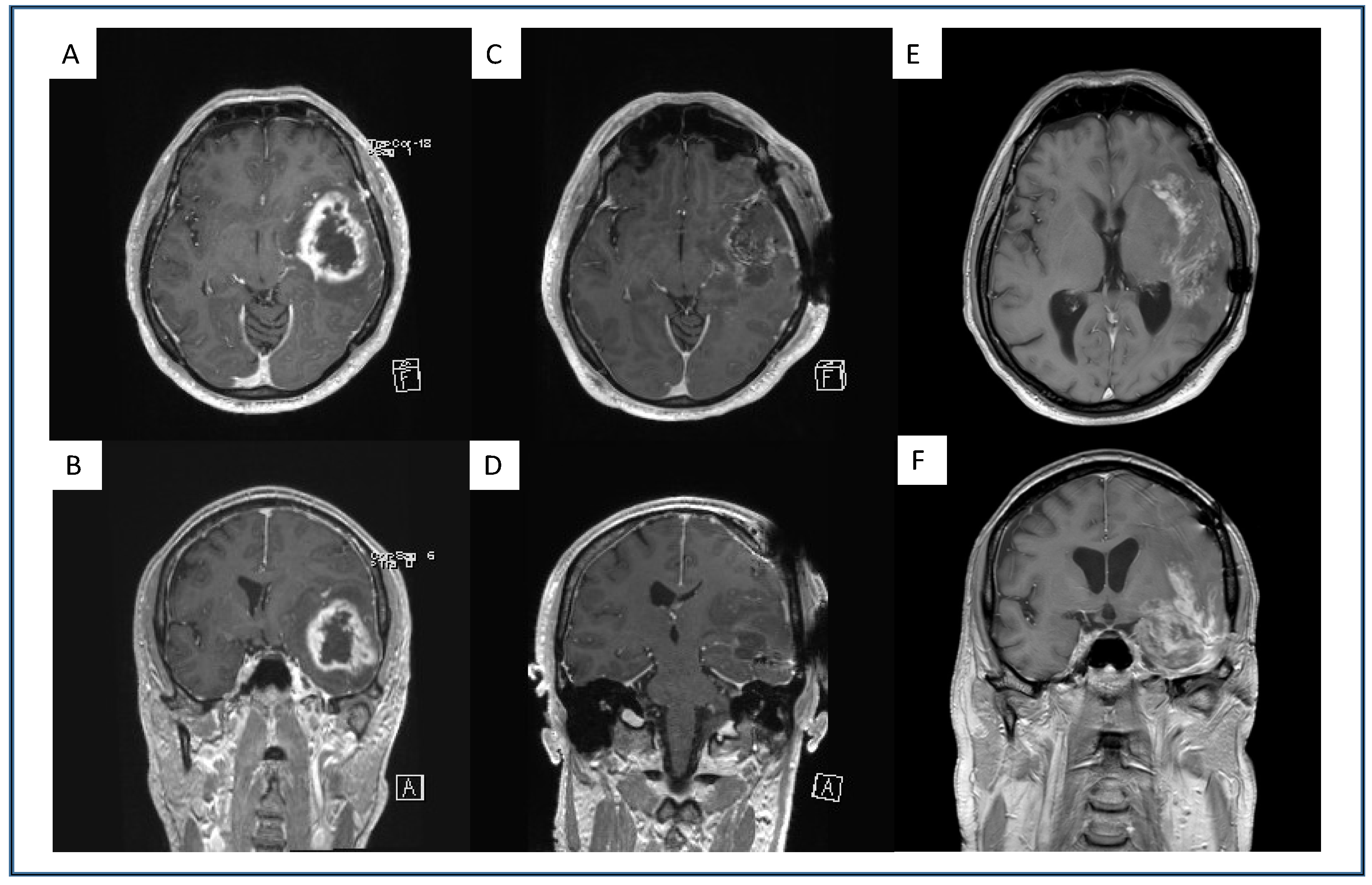
4.2. Sharp Demarcated Lesions
4.3. Analysis of Intratumoral Hemorrhage
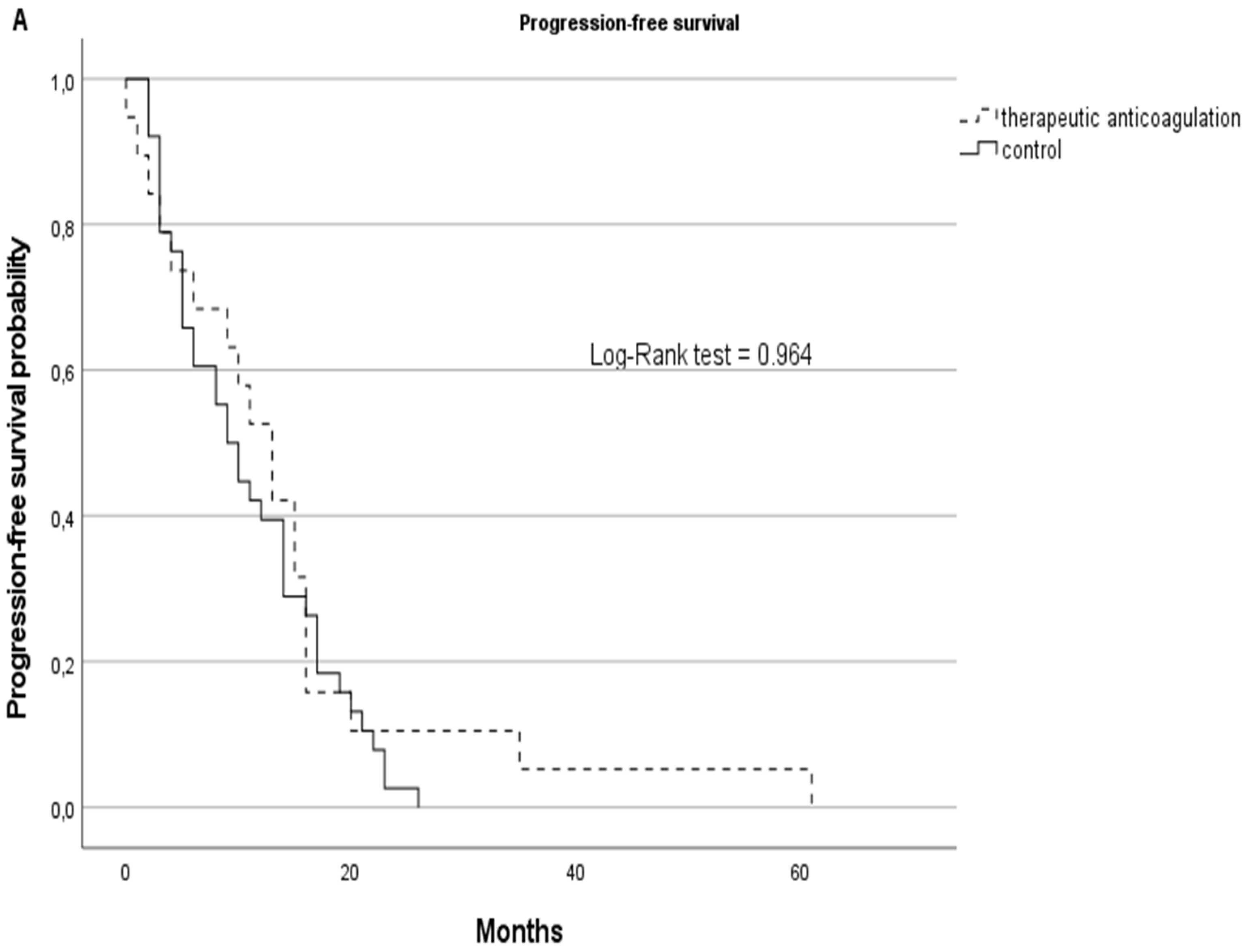
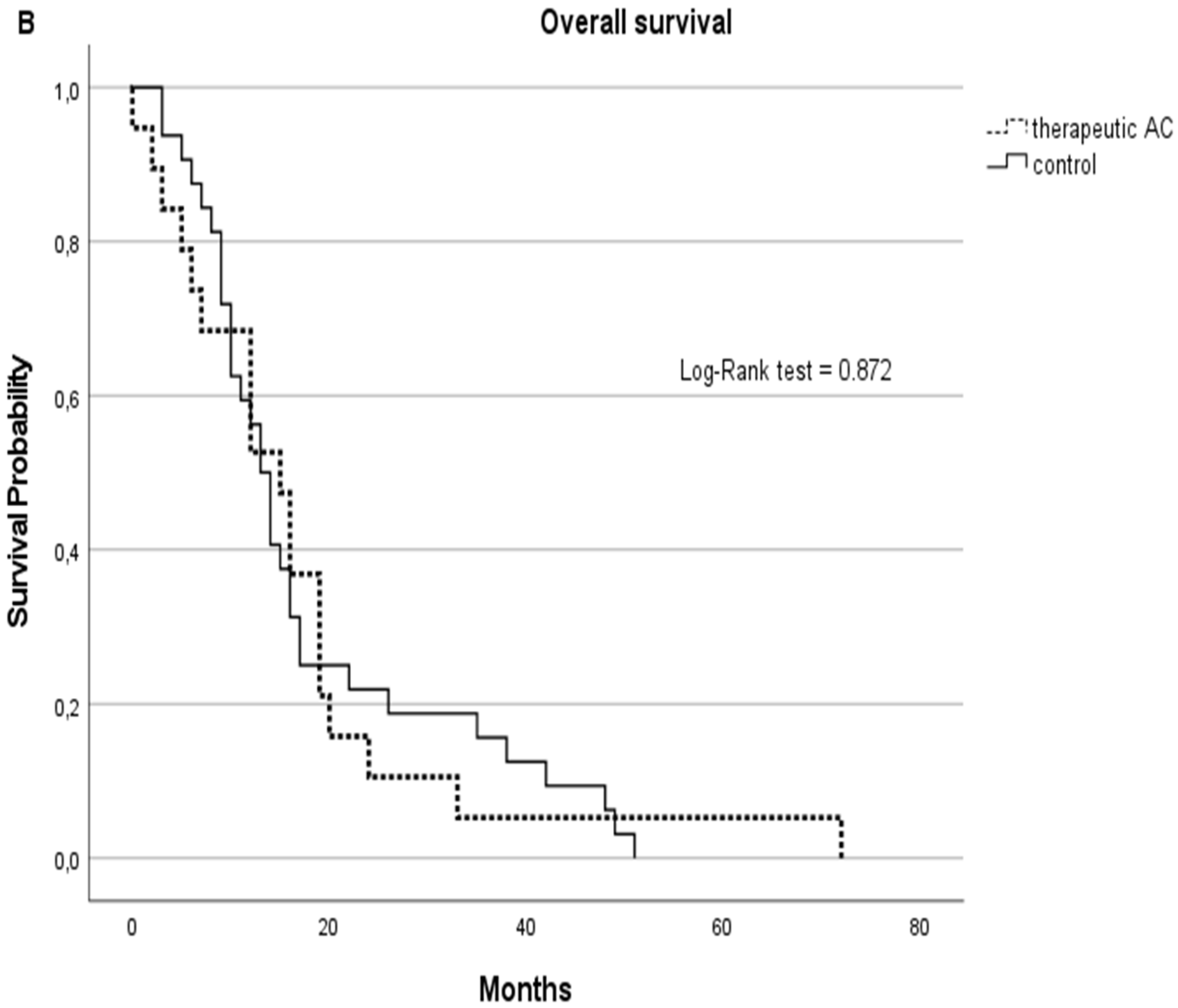
4.4. Progression-Free and Overall Survival
4.5. Limitations
4.6. Summary
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mandoj, C.; Tomao, L.; Conti, L. Coagulation in Brain Tumors: Biological Basis and Clinical Implications. Front. Neurol. 2019, 10, 181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puthucheary, Z.A.; Rawal, J.; McPhail, M.; Connolly, B.; Ratnayake, G.; Chan, P.; Hopkinson, N.S.; Phadke, R.; Padhke, R.; Dew, T.; et al. Acute skeletal muscle wasting in critical illness. JAMA 2013, 310, 1591–1600. [Google Scholar] [CrossRef] [Green Version]
- Falanga, A.; Marchetti, M.; Russo, L. The mechanisms of cancer-associated thrombosis. Thromb. Res. 2015, 135, S8–S11. [Google Scholar] [CrossRef]
- Rickles, F.R.; Falanga, A. Molecular basis for the relationship between thrombosis and cancer. Thromb. Res. 2001, 102. [Google Scholar] [CrossRef]
- Lima, L.G.; Monteiro, R.Q. Activation of blood coagulation in cancer: Implications for tumour progression. Biosci. Rep. 2013, 33, 701–710. [Google Scholar] [CrossRef] [PubMed]
- Chanakira, A.; Westmark, P.R.; Ong, I.M.; Sheehan, J.P. Tissue factor-factor VIIa complex triggers protease activated receptor 2-dependent growth factor release and migration in ovarian cancer. Gynecol. Oncol. 2017, 145, 167–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thaler, J.; Ay, C.; Mackman, N.; Bertina, R.M.; Kaider, A.; Marosi, C.; Key, N.S.; Barcel, D.A.; Scheithauer, W.; Kornek, G.; et al. Microparticle-associated tissue factor activity, venous thromboembolism and mortality in pancreatic, gastric, colorectal and brain cancer patients. J. Thromb. Haemost. 2012, 10, 1363–1370. [Google Scholar] [CrossRef]
- Wong, P.C.; Seiffert, D.; Bird, J.E.; Watson, C.A.; Bostwick, J.S.; Giancarli, M.; Allegretto, N.; Hua, J.; Harden, D.; Guay, J.; et al. Blockade of protease-activated receptor-4 (PAR4) provides robust antithrombotic activity with low bleeding. Sci. Transl. Med. 2017, 9. [Google Scholar] [CrossRef]
- Rong, Y.; Post, D.E.; Pieper, R.O.; Durden, D.L.; Van Meir, E.G.; Brat, D.J. PTEN and hypoxia regulate tissue factor expression and plasma coagulation by glioblastoma. Cancer Res. 2005, 65, 1406–1413. [Google Scholar] [CrossRef] [Green Version]
- Yust-Katz, S.; Mandel, J.J.; Wu, J.; Yuan, Y.; Webre, C.; Pawar, T.A.; Lhadha, H.S.; Gilbert, M.R.; Armstrong, T.S. Venous thromboembolism (VTE) and glioblastoma. J. Neurooncol. 2015, 124, 87–94. [Google Scholar] [CrossRef]
- Dubinski, D.; Won, S.Y.; Voss, M.; Keil, F.; Miesbach, W.; Behmanesh, B.; Dosch, M.; Baumgarten, P.; Bernstock, J.D.; Seifert, V.; et al. Direct oral anticoagulants vs. low-molecular-weight heparin for pulmonary embolism in patients with glioblastoma. Neurosurg. Rev. 2021. [Google Scholar] [CrossRef]
- Pope, W.B.; Xia, Q.; Paton, V.E.; Das, A.; Hambleton, J.; Kim, H.J.; Huo, J.; Brown, M.S.; Goldin, J.; Cloughesy, T. Patterns of progression in patients with recurrent glioblastoma treated with bevacizumab. Neurology 2011, 76, 432–437. [Google Scholar] [CrossRef] [PubMed]
- Adeberg, S.; König, L.; Bostel, T.; Harrabi, S.; Welzel, T.; Debus, J.; Combs, S.E. Glioblastoma recurrence patterns after radiation therapy with regard to the subventricular zone. Int. J. Radiat. Oncol. Biol. Phys. 2014, 90, 886–893. [Google Scholar] [CrossRef] [PubMed]
- Wick, W.; Stupp, R.; Beule, A.C.; Bromberg, J.; Wick, A.; Ernemann, U.; Platten, M.; Marosi, C.; Mason, W.P.; Van Den Bent, M.; et al. A novel tool to analyze MRI recurrence patterns in glioblastoma. Neuro. Oncol. 2008, 10, 1019–1024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chamberlain, M.C. Radiographic patterns of relapse in glioblastoma. J. Neuro-Oncol. 2011, 101, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Sherriff, J.; Tamangani, J.; Senthil, L.; Cruickshank, G.; Spooner, D.; Jones, B.; Brookes, C.; Sanghera, P. Patterns of relapse in glioblastoma multiforme following concomitant chemoradiotherapy with temozolomide. Br. J. Radiol. 2013, 86. [Google Scholar] [CrossRef] [Green Version]
- Niers, T.M.H.; Brüggemann, L.W.; van Sluis, G.L.; Liu, R.D.; Versteeg, H.H.; Büller, H.R.; van Noorden, C.J.F.; Reitsma, P.H.; Spek, C.A.; Richel, D.J. Long-term thrombin inhibition promotes cancer cell extravasation in a mouse model of experimental metastasis. J. Thromb. Haemost. 2009, 7, 1595–1597. [Google Scholar] [CrossRef] [PubMed]
- Stong, D.B.; Carlsson, S.C.; Bjurström, S.; Fransson-Steen, R.; Healing, G.; Skånberg, I. Two-year carcinogenicity studies with the oral direct thrombin inhibitor ximelagatran in the rat and the mouse. Int. J. Toxicol. 2012, 31, 348–357. [Google Scholar] [CrossRef]
- Najidh, S.; Versteeg, H.H.; Buijs, J.T. A systematic review on the effects of direct oral anticoagulants on cancer growth and metastasis in animal models. Thromb. Res. 2020, 187. Available online: https://reader.elsevier.com/reader/sd/pii/S0049384819305559?token=50D93BC4863E563FE44AC7421D2761921B95ACDEB0118F7E027122C703A7675220295A6DD7A27996F4991C0A54193EFD&originRegion=eu-west-1&originCreation=20210828092045 (accessed on 28 August 2021). [CrossRef] [Green Version]
- Monteiro, A.; Hill, R.; Pilkington, G.; Madureira, P. The Role of Hypoxia in Glioblastoma Invasion. Cells 2017, 6, 45. [Google Scholar] [CrossRef] [Green Version]
- Reardon, D.A.; Turner, S.; Peters, K.B.; Desjardins, A.; Gururangan, S.; Sampson, J.H.; McLendon, R.E.; Herndon, J.E.; Jones, L.W.; Kirkpatrick, J.P.; et al. A review of VEGF/VEGFR-targeted therapeutics for recurrent glioblastoma. J. Natl. Compr. Cancer Netw. 2011, 9, 414–427. [Google Scholar] [CrossRef] [Green Version]
- Featherby, S.; Xiao, Y.P.; Ettelaie, C.; Nikitenko, L.L.; Greenman, J.; Maraveyas, A. Low molecular weight heparin and direct oral anticoagulants influence tumour formation, growth, invasion and vascularisation by separate mechanisms. Sci. Rep. 2019, 9, 1–13. [Google Scholar] [CrossRef]
- Ma, S.-N.; Mao, Z.-X.; Wu, Y.; Liang, M.-X.; Wang, D.-D.; Chen, X.; Chang, P.-A.; Zhang, W.; Tang, J.-H. The anti-cancer properties of heparin and its derivatives: A review and prospect. Cell Adh. Migr. 2020, 14. [Google Scholar] [CrossRef] [PubMed]
- Carney, B.J.; Uhlmann, E.J.; Puligandla, M.; Mantia, C.; Weber, G.M.; Neuberg, D.S.; Zwicker, J.I. Intracranial hemorrhage with direct oral anticoagulants in patients with brain tumors. J. Thromb. Haemost. 2019, 17, 72–76. [Google Scholar] [CrossRef] [Green Version]
- Key, N.S.; Khorana, A.A.; Kuderer, N.M.; Bohlke, K.; Lee, A.Y.Y.; Arcelus, J.I.; Wong, S.L.; Balaban, E.P.; Flowers, C.R.; Francis, C.W.; et al. Venous thromboembolism prophylaxis and treatment in patients with cancer: ASCO clinical practice guideline update. J. Clin. Oncol. 2020, 38, 496–520. [Google Scholar] [CrossRef] [PubMed]
- Wojtukiewicz, M.Z.; Skalij, P.; Tokajuk, P.; Politynska, B.; Wojtukiewicz, A.M.; Tucker, S.C.; Honn, K.V. Direct Oral Anticoagulants in Cancer Patients. Time for a Change in Paradigm. Cancers 2020, 12, 1144. [Google Scholar] [CrossRef] [PubMed]
- Anticoagulant Treatment and Survival in Cancer Patients. The Evidence from CLINICAL studies|Haematologica. Available online: https://www.haematologica.org/article/view/3657 (accessed on 3 January 2022).
- Le Rhun, E.; Genbrugge, E.; Stupp, R.; Chinot, O.L.; Nabors, L.B.; Cloughesy, T.; Reardon, D.A.; Wick, W.; Gorlia, T.; Weller, M. Associations of anticoagulant use with outcome in newly diagnosed glioblastoma. Eur. J. Cancer 2018, 101, 95–104. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Therapeutic Anticoagulation | Univariate | Multivariate | |
|---|---|---|---|---|
| Yes (n = 19) | No (n = 38) | p-Value | ||
| Characteristics | ||||
| Male, n (%) | 9 (47%) | 26 (68) | n.s. | n.s. |
| Age, n (SD) | 62 (6) | 64 (8) | n.s. | n.s. |
| Clinical course | ||||
| Gross total resection, n (%) | 14 (73) | 25 (72) | n.s. | n.s. |
| Subtotal resection, n (%) | 5 (27) | 13 (28) | n.s. | n.s. |
| Progression-free survival, months (SD) | 13 (14) | 9.5 (7) | n.s. | n.s. |
| Overall survival, months (SD) | 15 (15) | 12.5 (13) | n.s. | n.s. |
| Histopathology | ||||
| MGMT methylated | 10 (53) | 15 (40) | n.s. | n.s. |
| MRI charateristics of reccurent tumor | ||||
| Local | 10 (53) | 32 (84) | 0.02 | n.s. |
| Multifocal | 9 (47) | 6 (16) | 0.02 | n.s. |
| Midline crossing | 9 (47) | 4 (11) | 0.004 | 0.006 |
| No midline crossing | 10 (53) | 34 (89) | 0.004 | 0.006 |
| Hemorrhage | 0 (0) | 1 (3) | n.s. | n.s. |
| No hemorrhage | 19 (100) | 37 (97) | n.s. | n.s. |
| Sharp demarcation | 7 (37) | 4 (11) | 0.03 | 0.008 |
| Without sharp demarcation | 12 (63) | 34 (89) | 0.03 | 0.008 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dubinski, D.; Won, S.-Y.; Behmanesh, B.; Dosch, M.; Puchinin, V.; Baumgarten, P.; Bernstock, J.D.; Voss, M.; Schuss, P.; Konczalla, J.; et al. Therapeutic Anticoagulation Impacts MR Morphologic Recurrence Patterns in Glioblastoma—A Matched-Pair Analysis. J. Clin. Med. 2022, 11, 422. https://doi.org/10.3390/jcm11020422
Dubinski D, Won S-Y, Behmanesh B, Dosch M, Puchinin V, Baumgarten P, Bernstock JD, Voss M, Schuss P, Konczalla J, et al. Therapeutic Anticoagulation Impacts MR Morphologic Recurrence Patterns in Glioblastoma—A Matched-Pair Analysis. Journal of Clinical Medicine. 2022; 11(2):422. https://doi.org/10.3390/jcm11020422
Chicago/Turabian StyleDubinski, Daniel, Sae-Yeon Won, Bedjan Behmanesh, Max Dosch, Viktoria Puchinin, Peter Baumgarten, Joshua D. Bernstock, Martin Voss, Patrick Schuss, Jürgen Konczalla, and et al. 2022. "Therapeutic Anticoagulation Impacts MR Morphologic Recurrence Patterns in Glioblastoma—A Matched-Pair Analysis" Journal of Clinical Medicine 11, no. 2: 422. https://doi.org/10.3390/jcm11020422
APA StyleDubinski, D., Won, S.-Y., Behmanesh, B., Dosch, M., Puchinin, V., Baumgarten, P., Bernstock, J. D., Voss, M., Schuss, P., Konczalla, J., Czabanka, M., Freiman, T. M., & Gessler, F. (2022). Therapeutic Anticoagulation Impacts MR Morphologic Recurrence Patterns in Glioblastoma—A Matched-Pair Analysis. Journal of Clinical Medicine, 11(2), 422. https://doi.org/10.3390/jcm11020422