
Use of a Deep Learning Approach for the Sensitive Prediction of Hepatitis B Surface Antigen Levels in Inactive Carrier Patients

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
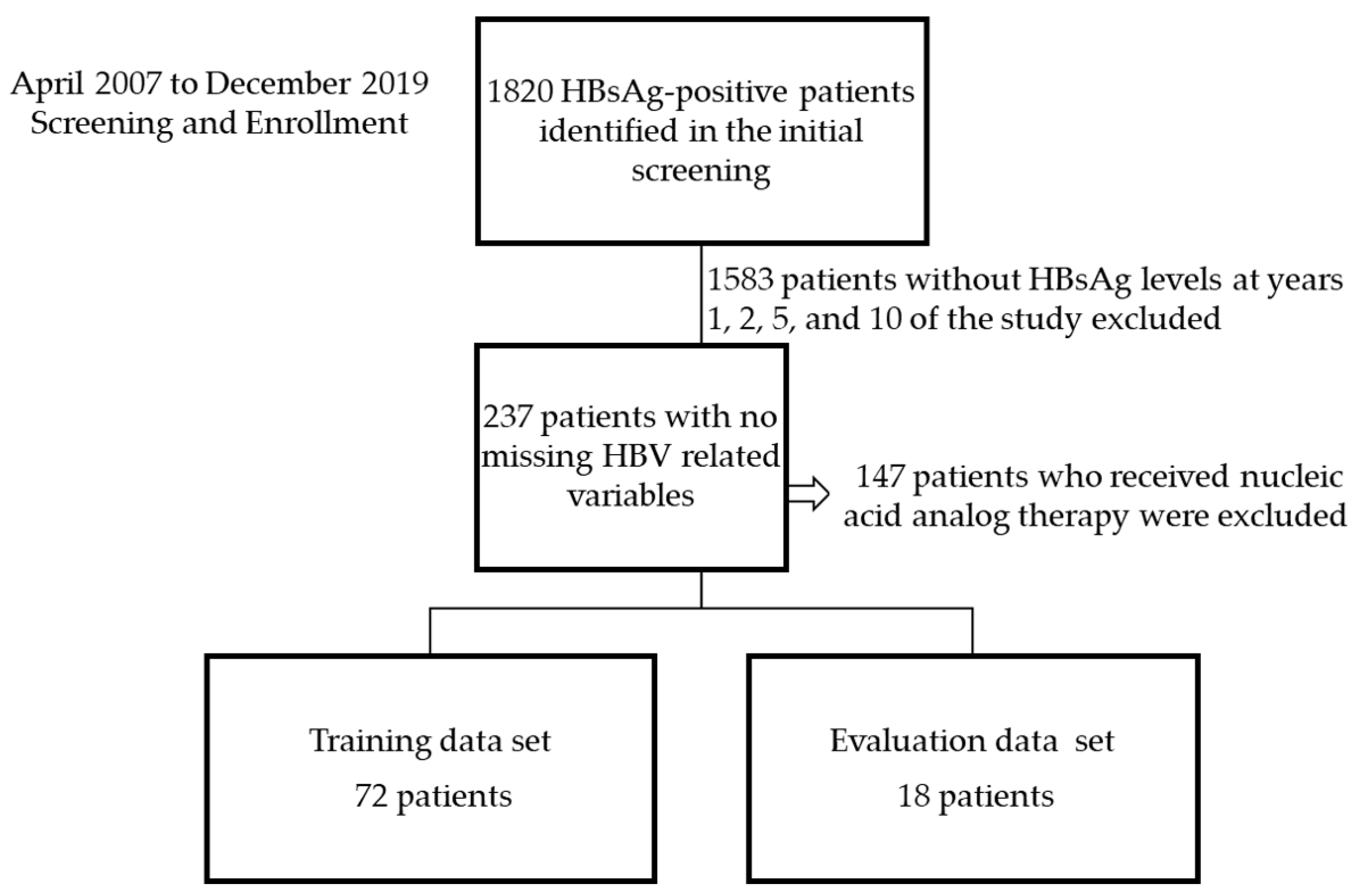
2.2. Study Design, Participants, and Settings
2.3. Sample Analysis
2.4. Statistical Analysis
2.5. Deep Neural Network (DNN)
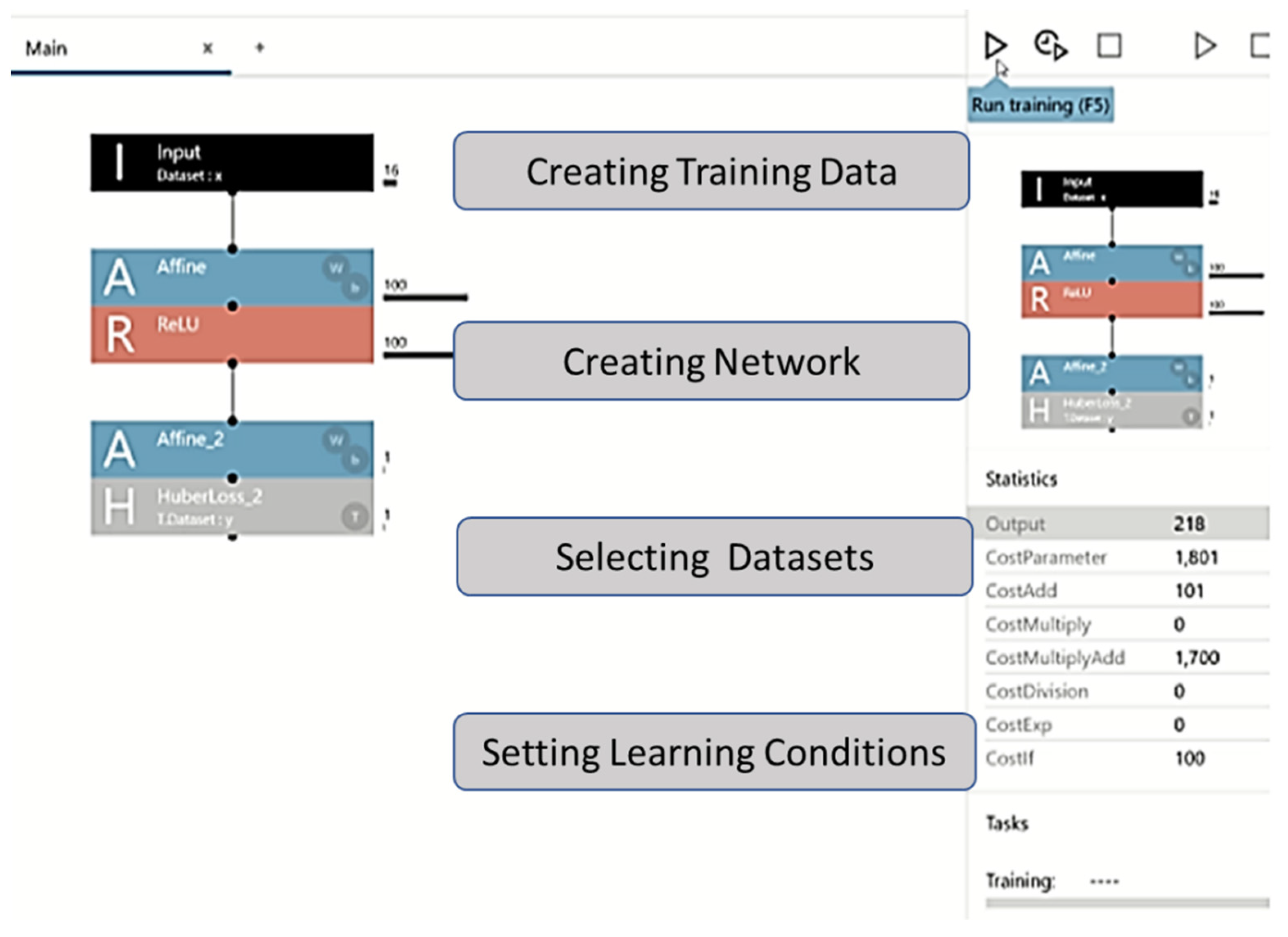
2.6. Dataset Creation
2.7. Network Configuration
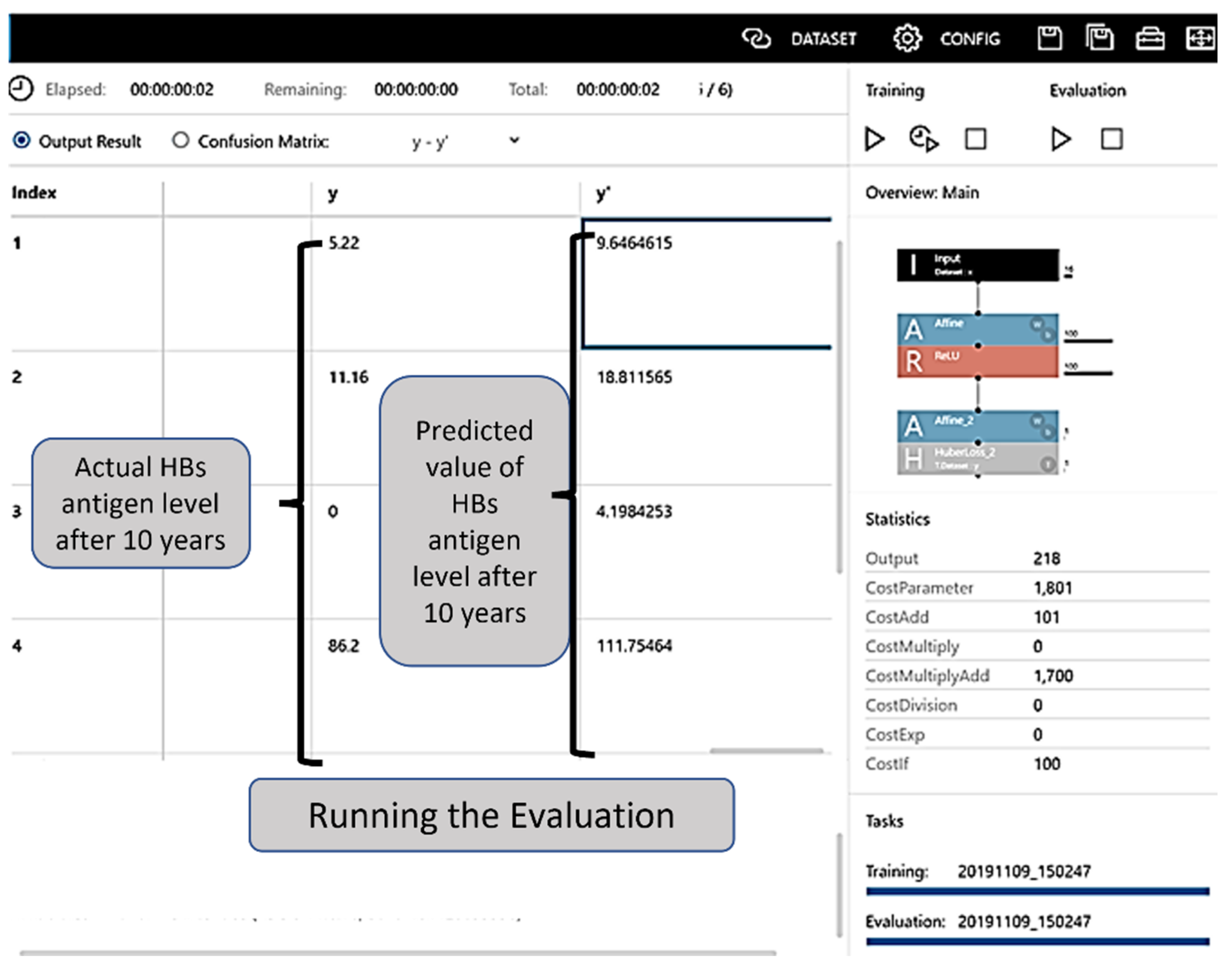
2.8. Evaluation
3. Results
3.1. Patient Characteristics
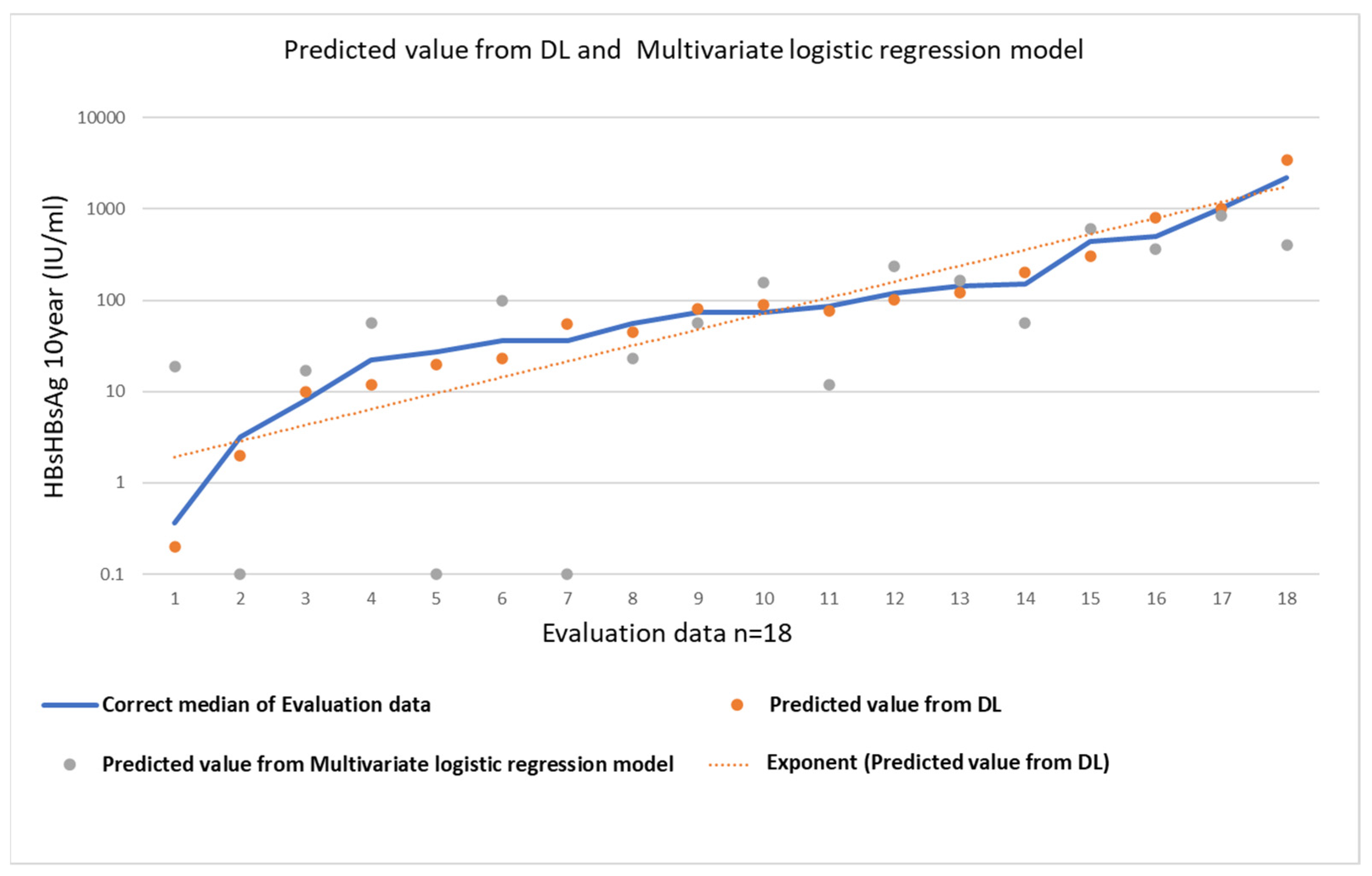
3.2. Evaluation of Statistical Analysis
Multivariate Logistic Regression Model
3.3. Evaluation of DL
Implementation and Evaluation of Learning
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Caviglia, G.P.; Troshina, Y.; Garro, E.; Gesualdo, M.; Aneli, S.; Birolo, G.; Pittaluga, F.; Cavallo, R.; Saracco, G.M.; Ciancio, A. Usefulness of a hepatitis B surface antigen-based model for the prediction of functional cure in patients with chronic hepatitis B virus infection treated with nucleos(t)ide analogues: A real-world study. J. Clin. Med. 2021, 10, 3308. [Google Scholar] [CrossRef]
- Xue, Y.; Zhang, M.; Li, T.; Liu, F.; Zhang, L.X.; Fan, X.P.; Yang, B.H.; Wang, L. Exploration of nu-cleos(t)ide analogs cessation in chronic hepatitis B patients with hepatitis B e antigen loss. World J. Gastroenterol. 2021, 27, 1497–1506. [Google Scholar] [CrossRef] [PubMed]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Shamshirband, S.; Fathi, M.; Dehzangi, A.; Chronopoulos, A.T.; Alinejad-Rokny, H. A review on deep learning approaches in healthcare systems: Taxonomies, challenges, and open issues. J. Biomed. Inform. 2021, 113, 103627. [Google Scholar] [CrossRef] [PubMed]
- WHO Fact Sheet. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-b (accessed on 26 November 2021).
- Chen, C.J.; Yang, H.I.; Su, J.; Jen, C.L.; You, S.L.; Lu, S.N.; Huang, G.T.; Iloeje, U.H.; REVEAL-HBV Study Group. Risk of hepatocellular carcinoma across a biological gradient of serum hepatitis B virus DNA level. JAMA 2006, 295, 65–73. [Google Scholar] [CrossRef] [Green Version]
- Tseng, T.C.; Liu, C.J.; Yang, H.C.; Su, T.H.; Wang, C.C.; Chen, C.L.; Kuo, S.F.; Liu, C.H.; Chen, P.J.; Chen, D.S.; et al. High levels of hepatitis B surface antigen increase risk of hepatocellular carcinoma in patients with low HBV load. Gastroenterology 2012, 142, 1140–1149. [Google Scholar] [CrossRef] [Green Version]
- Kapoor, R.; Kottilil, S. Strategies to eliminate HBV infection. Future Virol. 2014, 9, 565–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piratvisuth, T.; Marcellin, P.; Popescu, M.; Kapprell, H.P.; Rothe, V.; Lu, Z.M. Hepatitis B surface antigen: Association with sustained response to peginterferon alfa-2a in hepatitis B e antigen-positive patients. Hepatol. Int. 2013, 7, 429–436. [Google Scholar] [CrossRef]
- Takkenberg, B.; Zaaijer, H.; De Niet, A.; Weegink, C.J.; Terpstra, V.; Kool, M.; Dijkgraaf, M.; Jansen, P.L.; Janssen, H.L.; Beld, M.; et al. Baseline HBsAg level and on-treatment HBsAg and HBV DNA decline predict sustained virological response in HBeAg negative chronic hepatitis B patients treated with peginterferon alfa-2a (Pegasys) and Adefovir (Hepsera); an interim analysis. Hepatology 2009, 50, 538A–539A. [Google Scholar]
- Drafting Committee for Hepatitis Management Guidelines, the Japan Society of Hepatology. Japan Society of Hepatology Guidelines for the Management of Hepatitis B Virus Infection: 2019 update. Hepatol. Res. 2020, 50, 892–923. [Google Scholar] [CrossRef]
- Seto, W.K.; Wong, D.K.; Fung, J.; Ip, P.P.; Yuen, J.C.; Hung, I.F.; Lai, C.L.; Yuen, M.F. High hepatitis B surface antigen levels predict insignificant fibrosis in hepatitis B e antigen positive chronic hepatitis B. PLoS ONE 2012, 7, e43087. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tseng, T.C.; Liu, C.J.; Yang, H.C.; Su, T.H.; Wang, C.C.; Chen, C.L.; Hsu, C.A.; Kuo, S.F.; Liu, C.H.; Chen, P.J.; et al. Serum hepatitis B surface antigen levels help predict disease progression in patients with low hepatitis B virus loads. Hepatology 2013, 57, 441–450. [Google Scholar] [CrossRef]
- Liu, J.; Tseng, T.C.; Yang, H.I.; Lee, M.H.; Batrla-Utermann, R.; Jen, C.L.; Lu, S.N.; Wang, L.Y.; You, S.L.; Chen, P.J.; et al. Predicting hepatitis B virus (HBV) surface antigen seroclearance in HBV e antigen-negative patients with chronic hepatitis B: External validation of a scoring system. J. Infect. Dis. 2015, 211, 1566–1573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murayama, A.; Momose, H.; Yamada, N.; Hoshi, Y.; Muramatsu, M.; Wakita, T.; Ishimaru, K.; Hamaguchi, I.; Kato, T. Evaluation of in vitro screening and diagnostic kits for hepatitis B virus infection. J. Clin. Virol. 2019, 117, 37–42. [Google Scholar] [CrossRef]
- Boglione, L.; D’Avolio, A.; Cariti, G.; Gregori, G.; Burdino, E.; Baietto, L.; Cusato, J.; Ghisetti, V.; De Rosa, F.G.; Di Perri, G. Kinetics and prediction of HBsAg loss during therapy with analogues in patients affected by chronic hepatitis B HBeAg negative and genotype D. Liver Int. 2013, 33, 580–585. [Google Scholar] [CrossRef]
- Sejnowski, T.J. The unreasonable effectiveness of deep learning in artificial intelligence. Proc. Natl. Acad. Sci. USA 2020, 117, 30033–30038. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Velichko, A. A method for medical data analysis using the LogNNet for clinical decision support systems and edge computing in healthcare. Sensors 2021, 21, 6209. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. EASL 2017 Clinical practice guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, G.A.; Lim, Y.S.; An, J.; Lee, D.; Shim, J.H.; Kim, K.M.; Lee, H.C.; Chung, Y.H.; Lee, Y.S.; Suh, D.J. HBsAg seroclearance after nucleoside analogue therapy in patients with chronic hepatitis B: Clinical outcomes and durability. Gut 2014, 63, 1325–1332. [Google Scholar] [CrossRef]
- Liu, J.; Yang, H.I.; Lee, M.H.; Lu, S.N.; Jen, C.L.; Batrla-Utermann, R.; Wang, L.Y.; You, S.L.; Hsiao, C.K.; Chen, P.J.; et al. Spontaneous seroclearance of hepatitis B seromarkers and subsequent risk of hepatocellular carcinoma. Gut 2014, 63, 1648–1657. [Google Scholar] [CrossRef]
- Thi Vo, T.; Poovorawan, K.; Charoen, P.; Soonthornworasiri, N.; Nontprasert, A.; Kittitrakul, C.; Phumratanaprapin, W.; Tangkijvanich, P. Association between Hepatitis B surface antigen levels and the risk of hepatocellular carcinoma in patients with chronic hepatitis B infection: Systematic review and meta-analysis. Asian Pac. J. Cancer Prev. 2019, 20, 2239–2246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, T.; Thompson, A.J.; Bowden, S.; Croagh, C.; Bell, S.; Desmond, P.V.; Levy, M.; Locarnini, S.A. Hepatitis B surface antigen levels during the natural history of chronic hepatitis B: A perspective on Asia. J. Hepatol. 2010, 52, 508–513. [Google Scholar] [CrossRef]
- Alghamdi, A.; Aref, N.; El-Hazmi, M.; Al-Hamoudi, W.; Alswat, K.; Helmy, A.; Sanai, F.M.; Abdo, A.A. Correlation between hepatitis B surface antigen titers and HBV DNA levels. Saudi J. Gastroenterol. 2013, 19, 252–257. [Google Scholar] [CrossRef]
- Nowak, M.A.; Bonhoeffer, S.; Hill, A.M.; Boehme, R.; Thomas, H.C.; McDade, H. Viral dynamics in hepatitis B virus infection. Proc. Natl. Acad. Sci. USA 1996, 93, 4398–4402. [Google Scholar] [CrossRef] [Green Version]
- Liaw, Y.F. HBeAg seroconversion as an important end point in the treatment of chronic hepatitis B. Hepatol. Int. 2009, 3, 425–433. [Google Scholar] [CrossRef] [Green Version]
- Thompson, A.J.; Nguyen, T.; Iser, D.; Ayres, A.; Jackson, K.; Littlejohn, M.; Slavin, J.; Bowden, S.; Gane, E.J.; Abbott, W.; et al. Serum hepatitis B surface antigen and hepatitis B e antigen titers: Disease phase influences correlation with viral load and intrahepatic hepatitis B virus markers. Hepatology 2010, 51, 1933–1944. [Google Scholar] [CrossRef] [PubMed]
- Nagaoka, S.; Abiru, S.; Komori, A.; Sasaki, R.; Bekki, S.; Hashimoto, S.; Saeki, A.; Yamasaki, K.; Migita, K.; Nakamura, M.; et al. Hepatic flares promote rapid decline of serum hepatitis B surface antigen (HBsAg) in patients with HBsAg seroclearance: A long-term follow-up study. Hepatol. Res. 2016, 46, E89–E99. [Google Scholar] [CrossRef]
- Mak, L.Y.; Seto, W.K.; Fung, J.; Yuen, M.F. Use of HBsAg quantification in the natural history and treatment of chronic hepatitis B. Hepatol. Int. 2020, 14, 35–46. [Google Scholar] [CrossRef] [PubMed]
- Aishwarya, T.; Ravi Kumar, V. Machine learning and deep learning approaches to analyze and detect COVID-19: A review. SN Comput. Sci. 2021, 2, 226. [Google Scholar] [CrossRef] [PubMed]
- Un, K.C.; Wong, C.K.; Lau, Y.M.; Lee, J.C.; Tam, F.C.; Lai, W.H.; Lau, Y.M.; Chen, H.; Wibowo, S.; Zhang, X.; et al. Observational study on wearable biosensors and machine learning-based remote monitoring of COVID-19 patients. Sci. Rep. 2021, 11, 4388. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Liu, P.; Huang, X.; Cao, Y. Teacher online informal learning as a means to innovative teaching during home quarantine in the COVID-19 pandemic. Front. Psychol. 2021, 12, 596582. [Google Scholar] [CrossRef] [PubMed]
- Hassan, M.R.; Hassan, M.M.; Altaf, M.; Yeasar, M.S.; Hossain, M.I.; Fatema, K.; Shaharin, R.; Ahmed, A.F. B5G-enabled distributed artificial intelligence on edges for COVID-19 pandemic outbreak prediction. IEEE Netw. 2021, 35, 48–55. [Google Scholar] [CrossRef]
- Valtchev, S.Z.; Asgary, A.; Chen, M.; Cronemberger, F.A.; Najafabadi, M.M.; Cojocaru, M.G.; Wu, J. Managing SARS-CoV-2 Testing in schools with an artificial intelligence model and application developed by simulation data. Electronics 2021, 10, 1626. [Google Scholar] [CrossRef]
- Tsai, E. Review of current and potential treatments for chronic hepatitis b virus infection. Gastroenterol. Hepatol. 2021, 17, 367–376. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Continuous Survey over 10 Years (n = 90); Median (Range or %) | |||
|---|---|---|---|
| Variable | Training Data (n = 72) | Evaluation Data (n = 18) | p-Value |
| Sex, male (%) | 69 (63) | 13 (65) | n.s. |
| Age (y) | 69 (14–78) | 67 (20–81) | n.s. |
| HT (cm) | 162 (123–189) | 165 (144–177) | n.s. |
| Body weight (kg) | 59 (33–98) | 61 (39–88) | n.s. |
| HBeAg negative rate (%) * | 67/72 (92) | 16/18 (93) | n.s. |
| HBV DNA first year (Log(IU/mL)) | 3.2 (1.9–5.2) | 3.1 (2.2–5.4) | n.s. |
| HBsAg first year (IU/mL) | 455 (45–7202) | 421 (42–5915) | n.s. |
| ALT first year (IU/L) | 33 (15–42) | 31 (21–49) | n.s. |
| AST first year (IU/L) | 28 (7–51) | 22 (9–45) | n.s. |
| HBV DNA second year (Log(IU/mL)) | 2.7 (1.5–5.0) | 2.9 (1.9–5.1) | n.s. |
| HBsAg second year (IU/mL) | 233 (7.2–4949) | 201 (9.3–4233) | n.s. |
| ALT second year (IU/L) | 29 (11–39) | 31 (13–45) | n.s. |
| AST second year (IU/L) | 26 (19–48) | 23 (11–45) | n.s. |
| HBV DNA fifth year (Log(IU/mL)) | 2.5 (1.4–4.3) | 2.8 (2.1–4.9) | n.s. |
| HBsAg fifth year (IU/mL) | 112 (0.7–4025) | 101 (0.9–3336) | n.s. |
| ALT fifth year (IU/L) | 21 (9–46) | 26 (9–44) | n.s. |
| AST fifth year (IU/L) | 26 (19–45) | 26 (11–49) | n.s. |
| HBV DNA tenth year (Log(IU/mL)) | 2.5 (N.D–4.3) | 2.8 (N.D–4.9) | n.s. |
| HBsAg tenth year (IU/mL) | 98 (0.1–4551) | 78 (0.4–2221) | n.s. |
| ALT tenth year (IU/L) | 19 (7–39) | 21 (8–56) | n.s. |
| AST tenth year (IU/L) | 22 (12–35) | 21 (11–46) | n.s. |
| Factors for Predicting Serum HBsAg 10 Years after HBs Titer According to Univariable and Multivariable Analyses | ||||||||
|---|---|---|---|---|---|---|---|---|
| Variable | Univariable Analysis | Multivariable Analysis | ||||||
| OR | 95% CI | p | OR | 95% CI | p | |||
| Constant | −1167 | |||||||
| Sex | 28.378 | −58.158 | 114.914 | 0.514 | ||||
| HT, cm | 5.809 | 0.963 | 10.655 | 0.020 | 6.942 | 4.068 | 9.816 | 0.068 |
| Body weight, kg | 1.183 | −1.659 | 4.024 | 0.408 | ||||
| Age, y | −1.214 | −4.302 | 1.873 | 0.434 | ||||
| HBeAg negative rate, % * | −142.964 | −244.111 | −41.816 | 0.006 | −154.811 | −255.179 | −54.442 | 0.003 |
| HBV DNA first year, Log (IU/mL) | −40.079 | −70.535 | −9.623 | 0.011 | −35.566 | −64.631 | −6.502 | 0.017 |
| HBsAg first year, IU/mL | 0.278 | 0.209 | 0.347 | 0.000 | 0.117 | 0.060 | 0.175 | 0.000 |
| ALT first year, IU/L | 12.037 | 6.186 | 17.889 | 0.000 | 12.273 | 7.286 | 17.261 | 0.000 |
| AST first year, IU/L | −5.747 | −24.151 | 12.657 | 0.536 | ||||
| HBV DNA second year, Log (IU/mL) | −20.074 | −51.535 | −7.623 | 0.068 | ||||
| HBsAg second year, IU/mL | −0.756 | −0.880 | −0.632 | 0.000 | −0.736 | −0.843 | −0.628 | 0.000 |
| ALT second year, IU/L | 7.512 | −18.602 | 33.627 | 0.568 | ||||
| AST second year, IU/L | 22.523 | −1.205 | 46.250 | 0.062 | 0.675 | −1.788 | 3.139 | 0.586 |
| HBV DNA fifth year, Log (IU/mL) | −18.156 | −50.424 | −8.362 | 0.075 | ||||
| HBsAg fifth year, IU/mL | 1.218 | 1.126 | 1.310 | 0.000 | 1.215 | 1.135 | 1.295 | 0.000 |
| ALT fifth year, IU/L | −12.791 | −19.521 | −6.060 | 0.000 | −9.955 | −15.016 | −4.894 | 0.000 |
| AST fifth year, IU/L | −1.363 | −7.135 | 4.409 | 0.638 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kamimura, H.; Nonaka, H.; Mori, M.; Kobayashi, T.; Setsu, T.; Kamimura, K.; Tsuchiya, A.; Terai, S. Use of a Deep Learning Approach for the Sensitive Prediction of Hepatitis B Surface Antigen Levels in Inactive Carrier Patients. J. Clin. Med. 2022, 11, 387. https://doi.org/10.3390/jcm11020387
Kamimura H, Nonaka H, Mori M, Kobayashi T, Setsu T, Kamimura K, Tsuchiya A, Terai S. Use of a Deep Learning Approach for the Sensitive Prediction of Hepatitis B Surface Antigen Levels in Inactive Carrier Patients. Journal of Clinical Medicine. 2022; 11(2):387. https://doi.org/10.3390/jcm11020387
Chicago/Turabian StyleKamimura, Hiroteru, Hirofumi Nonaka, Masaya Mori, Taichi Kobayashi, Toru Setsu, Kenya Kamimura, Atsunori Tsuchiya, and Shuji Terai. 2022. "Use of a Deep Learning Approach for the Sensitive Prediction of Hepatitis B Surface Antigen Levels in Inactive Carrier Patients" Journal of Clinical Medicine 11, no. 2: 387. https://doi.org/10.3390/jcm11020387
APA StyleKamimura, H., Nonaka, H., Mori, M., Kobayashi, T., Setsu, T., Kamimura, K., Tsuchiya, A., & Terai, S. (2022). Use of a Deep Learning Approach for the Sensitive Prediction of Hepatitis B Surface Antigen Levels in Inactive Carrier Patients. Journal of Clinical Medicine, 11(2), 387. https://doi.org/10.3390/jcm11020387