
Impact of the COVID-19 Pandemic on Healthcare Activity in the Regional Hospitals of Andalusia (Spain)

 , ,
, ,  and
and
Abstract
:1. Introduction
Impact of the COVID-19 Pandemic in Spain through 2020
2. Materials and Methods
2.1. Design
2.2. Data Collection
2.3. Ethical Considerations
2.4. Statistical Analysis
3. Results
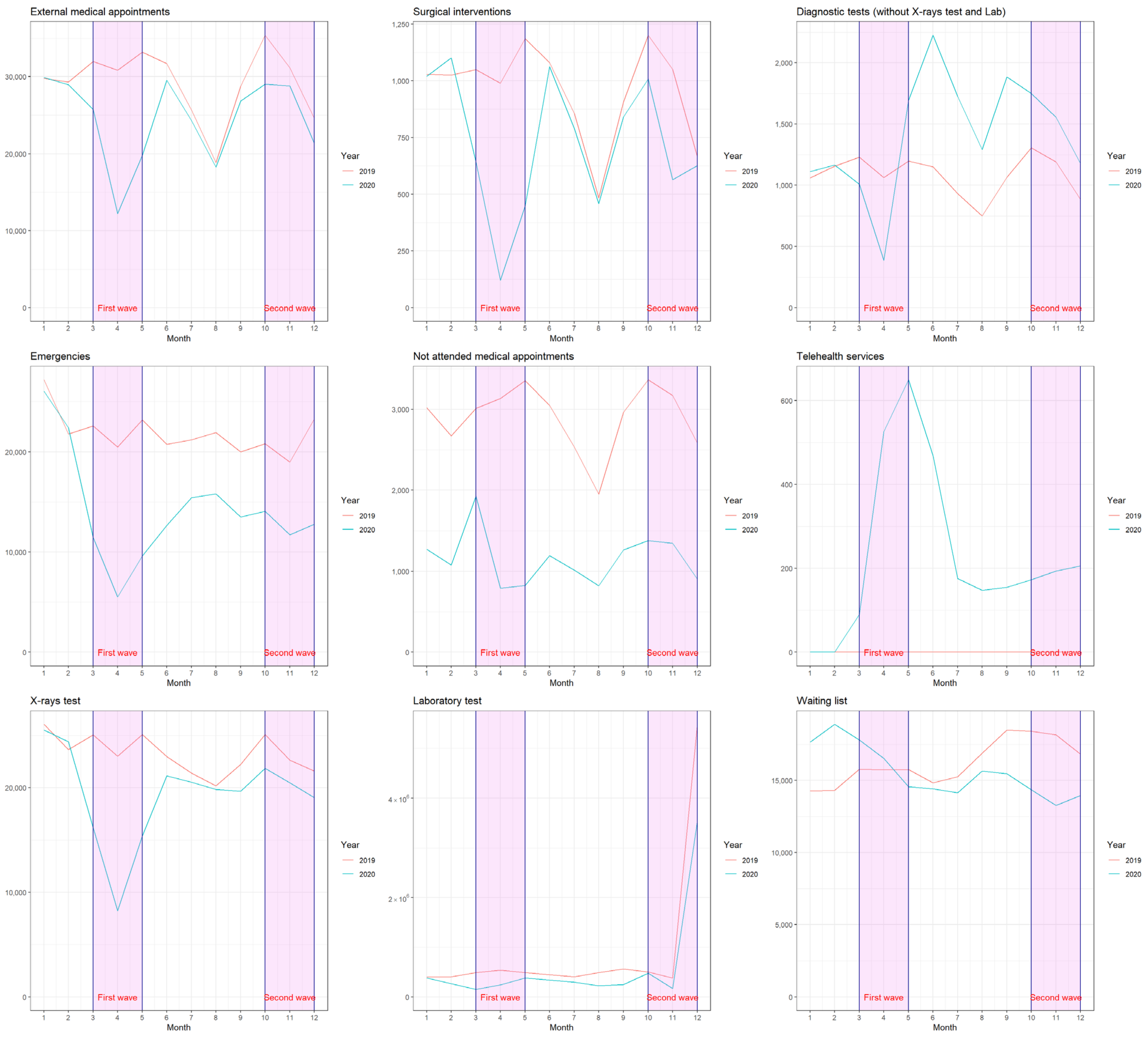
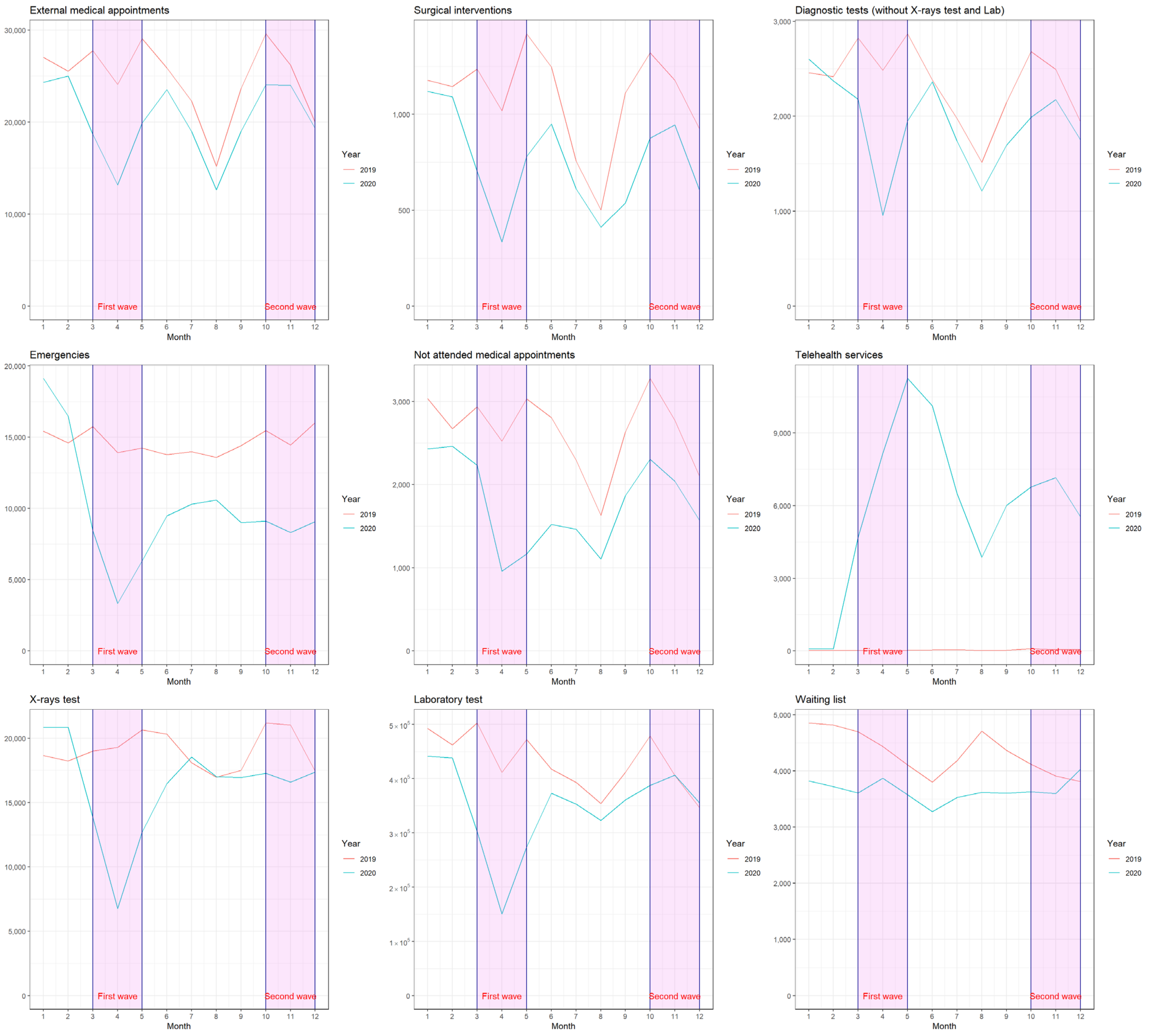
3.1. Healthcare Activity Carried out in Both Healthcare Institutions Pre- and during the First Year of the Pandemic
3.2. Comparison of Healthcare Activity between PH and AGHA
4. Discussion
4.1. Main Findings
4.2. Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Organización Mundial de la Salud (OMS). Nuevo Coronavirus. Available online: https://www.who.int/es/emergencies/diseases/novel-coronavirus-2019 (accessed on 17 October 2021).
- Giwa, A.L.; Desai, A.; Duca, A. Novel 2019 coronavirus SARS-CoV-2 (COVID-19): An updated overview for emergency clinicians. Emerg Med. Pract. 2020, 22, 1–28. [Google Scholar] [PubMed]
- Lopez-Villegas, A.; Maroto-Martin, S.; Baena-Lopez, M.A.; Garzon-Miralles, A.; Bautista-Mesa, R.J.; Peiro, S.; Leal-Costa, C. Telemedicine in times of the pandemic produced by COVID-19: Implementation of a teleconsultation protocol in a hospital emergency department. Healthcare 2020, 8, 357. [Google Scholar] [CrossRef] [PubMed]
- Rothan, H.A.; Byrareddy, S.N. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J. Autoimmun. 2020, 109, 102433. [Google Scholar] [CrossRef] [PubMed]
- Sohrabi, C.; Alsafi, Z.; O’Neill, N.; Khan, M.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, R. World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). Int. J. Surg. 2020, 76, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Fernández Landa, M.J.; Sánchez, P. Impacto en la actividad asistencial y la salud de los profesionales de Atención Primaria durante el confinamiento. Metas De Enfermería 2021, 24, 17. [Google Scholar] [CrossRef]
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 11 November 2021).
- Características de Los Casos Investigados Por COVID-2019 en España CNE. CNM.ISCIII. 11 Febrero. Available online: https://www.isciii.es (accessed on 11 November 2021).
- Centro Nacional de Epidemiología. Informe n Situación COVID-19 en España a 29 de Diciembre de 2021. Available online: https://www.isciii.es/QueHacemos/Servicios/VigilanciaSaludPublicaRENAVE/EnfermedadesTransmisibles/Paginas/InformesCOVID-19.aspx (accessed on 11 November 2021).
- Ministerio de Sanidad, Consumo y Bienestar Social. Situación Actual Coronavirus. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov-China/situacionActual.htm (accessed on 11 November 2021).
- Centro de Coordinación de Alertas y Emergencias Sanitarias. Actualización n 534: Enfermedad por SARS-CoV-2 (COVID-19) 03.01.2022. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/documentos/Actualizacion_534_COVID-19.pdf (accessed on 11 November 2021).
- RTVE.es «La Pandemia Deja un Exceso de Muertes de más de 80.000 Personas en 2020». RTVE.es. Available online: https://www.rtve.es/noticias/20210113/80000-exceso-muertes-pandemia-espana-2020/2065963.shtml (accessed on 11 November 2021).
- Arroyo, J.; «Uno de Cada 10 Españoles se ha Contagiado de Covid, la Mitad en Segunda Ola». Redacción Médica. Available online: https://www.redaccionmedica.com/secciones/sanidad-hoy/uno-cada-10-espanoles-contagiado-covid-mitad-segunda-ola-5591 (accessed on 11 November 2021).
- Rosenbaum, L. The untold toll—The pandemic’s efects on patients without COVID-19. N. Engl. J. Med. 2020, 382, 2368–2371. [Google Scholar] [CrossRef] [PubMed]
- Sociedad Española de Oncología Médica. Impacto Sanitaria Del Coronavirus en La Atención Hospitalaria a Pacientes Oncohematológicos Conclusiones. Available online: https://seom.org/images/Resumen_COVID_pacientes.pdf (accessed on 17 October 2021).
- Centro de Coordinación de Alertas y Emergencias Sanitarias. Enfermedad por Nuevo Coronavirus, COVID-Madrid: Ministerio de Sanidad de España. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/home.htm (accessed on 17 October 2021).
- Rodríguez-Leor, O.; Cid-Álvarez, B.; Ojeda, S.; Martín-Moreiras, J.; Ramón Rumoroso, J.; López-Palop, R.; Serrador, A.; Cequier, Á.; Romaguera, R.; Cruz, I.; et al. Impact of the COVID-19 pandemic on interventional cardiology activity in Spain. REC Interv. Cardiol. 2020, 2, 82–89. [Google Scholar] [CrossRef]
- Wilder-Smith, A.; Freedman, D.O. Isolation, quarantine, social distancing and community containment: Pivotal role for old-style public health measures in the novel coronavirus (2019-nCoV) outbreak. J. Travel. Med. 2020, 27, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Real Decreto 463/2020, de 14 de Marzo, Por el Que se Declara el Estado de Alarma Para la Gestión de la Situación de Crisis Sanitaria Ocasionada Por el COVID-Boletín Oficial del Estado (BOE), núm 67, de 14 de Marzo de 2020. p. 25390. Available online: https://www.boe.es/boe/dias/2020/03/14/pdfs/BOE-A-2020-3692.pdf (accessed on 11 November 2021).
- Lamoncloa.Gob.es. Plan de Desescalada. Available online: https://www.lamoncloa.gob.es/consejodeministros/resumenes/Paginas/2020/280420-consejo_ministros.aspx (accessed on 11 November 2021).
- Negreira Caamaño, M.; Piqueras Flores, J.; Mateo Gómez, C. Impact of COVID-19 pandemic in cardiology admissions. Med. Clin. 2020, 155, 179–180. [Google Scholar] [CrossRef] [PubMed]
- Boserup, B.; McKenney, M.; Elkbuli, A. The financial strain placed on America’s hospitals in the wake of the COVID-19 pandemic. Am. J. Emerg. Med. 2021, 45, 530–531. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Coronavirus Disease (COVID-19) Situation Report. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200615-covid-19-sitrep-147.pdf (accessed on 11 November 2021).
- Lapostolle, F.; Goix, L.; Vianu, I.; Chanzy, E.; De Stefano, C.; Gorlicki, J.; Petrovic, T.; Adnet, F. COVID-19 epidemic in the Seine-Saint-Denis Department of Greater Paris: One month and three waves for a tsunami. Eur. J. Emerg. Med. 2020, 27, 274–278. [Google Scholar] [CrossRef] [PubMed]
- Saberian, P.; Conovaloff, J.L.; Vahidi, E.; Hasani-Sharamin, P.; Kolivand, P.-H. How the COVID-19 Epidemic Affected Prehospital Emergency Medical Services in Tehran, Iran. West. J. Emerg. Med. 2020, 21, 110–116. [Google Scholar]
- Katayama, Y.; Tanaka, K.; Kitamura, T.; Takeuchi, T.; Nakao, S.; Nitta, M.; Iwami, T.; Fujimi, S.; Uejima, T.; Miyamoto, Y.; et al. Incidence and mortality of emergency patients transported by emergency medical service personnel during the novel corona virus pandemic in Osaka Prefecture, Japan: A population-based study. J. Clin. Med. 2021, 10, 5662. [Google Scholar] [CrossRef] [PubMed]
- Agencia Pública Sanitaria Poniente. Memoria. Available online: http://www.ephpo.es/memorias/Memoria%202017.pdf (accessed on 11 November 2021).
- Agencia Sanitaria Alto Guadalquivir. Memoria. Available online: http://www.ephag.es/Documents/ASAGmem2017_OK.pdf (accessed on 11 November 2021).
- WMA—The World Medical Association-Declaration of Helsinki—Ethical Principles for Medical Research Involving Human Subjects. Available online: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (accessed on 16 October 2021).
- Ley 41/2002, de 14 de Noviembre, Básica Reguladora de la Autonomía del Paciente y de Derechos y Obligaciones en Materia de Información y Documentación Clínica. Available online: https://www.boe.es/buscar/pdf/2002/BOE-A-2002–22188-consolidado.pdf (accessed on 16 October 2021).
- Ley Orgánica 3/2018, de 5 de Diciembre, de Protección de datos Personales y Garantía de los Derechos Digitales. Available online: https://www.boe.es/boe/dias/2018/12/06/pdfs/BOE-A-2018–16673.pdf (accessed on 16 October 2021).
- Valdés, I. La Crisis del Coronavirus: La Primera ola de Covid Provocó la Pérdida de 1.979.323 Consultas Entre Marzo y Agosto. Available online: https://elpais.com/espana/madrid/2020–12–14/la-primera-ola-de-covid-provoco-la-perdida-de-1979323-consultas-entre-marzo-y-agosto.html (accessed on 16 October 2021).
- Acadèmia de Ciències Mèdiques i de la Salut de Catalunya i Balears. Impacto de la Pandemia del Covid-19 en las Organizaciones Sanitarias: 25 Propuestas a Partir de lo que Hemos Aprendido Sociedad Catalana de Gestión Sanitaria. Available online: http://dabaitieslc.sg-host.com/wp-content/uploads/2020/06/Documento-25-propuestas-a-partir-del-COVID-CAST2.pdf (accessed on 20 October 2021).
- Martínez-Navarro, G.; Lozano-Zafra, C.; Caballero-Chabrera, F.; Modesto-Alapont, V.; Oltra-Benavent, M. COVID-19 impact on the emergency and hospitalization of a tertiary hospital. Management lessons learned. Enferm. Infecc. Microbiol. Clin. 2021, in press. [Google Scholar] [CrossRef]
- Ortega Benítez, A.; Rodríguez Gómez, J.; Novo Muñoz, M.; Rodríguez Novo, N.; Rodríguez Novo, Y.; Aguirre Jaime, A. Inadecuación de la urgencia pediátrica hospitalaria y sus factores asociados. Ene 2019, 13, 1324. [Google Scholar]
- Díaz Pérez, D.; Lorente Sorolla, M.; González Lago, S.; De Carlos Vicente, J.C.; Figueroa Mulet, J.; Osona Rodríguez, B. Impacto de la pandemia por SARS-CoV-2 en la asistencia a urgencias en ingresos de un hospital terciario. An. Pediatr. 2021, 94, 125–126. [Google Scholar] [CrossRef] [PubMed]
- Ramos Lacuey, B.; Herranz Aguirre, M.; Calderón Gallego, C.; Ilundain López, A.; Gembero Esarte, E.; Moreno Galarraga, L. Consecuencias de la pandemia COVID-19 en los ingresos por otras enfermedades Estudio ECIEN-2020. Poster communication. In Proceedings of the I Digital Congress of the Spanish Association of Pediatrics, Barcelona, Spain, 5–7 November 2020. 1191. [Google Scholar]
- Herrero Álvarez, M.; Bello Gutierrez, P.; Ares Mateos, G. Reorganización de Urgencias pediátricas en un hospital de 2º nivel. Poster communication. In Proceedings of the I Digital Congress of the Spanish Association of Pediatrics, Barcelona, Spain, 5–7 November 2020. 1214. [Google Scholar]
- Álvarez García, N.; Núñez García, B.; Pérez-Gaspar, M.; Jiménez Gómez, J.; Betancourth Alvarenga, J.E.; Santiago Martínez, S. Impacto inicial de la pandemia por COVID-19 en cirugía pediátrica: Análisis de un centro terciario. Poster communication. In Proceedings of the I Digital Congress of the Spanish Association of Pediatrics, Barcelona, Spain, 5–7 November 2020. 1209. [Google Scholar]
- Asociación Española Contra el Cáncer. Impacto del COVID-19 en la Atención Hospitalaria: El Número de Pacientes de Cáncer Nuevos Bajó un 21% Durante el Confinamiento. Available online: https://blogaecc.azurewebsites.net/diagnosticos-cancer-coronavirus/ (accessed on 11 November 2021).

{kind=link}
{kind=link}
| Poniente Hospital [27] | Alto Guadalquivir Health Agency [28] | |
|---|---|---|
| Reference population (inhabitants) | 264,386 | 264,733 |
| Municipalities covered | 15 | 47 |
| Total professionals working | 1419 | 1874 |
| Outpatient Consultations | 280,337 | 403,490 |
| Emergencies | 151,170 | 255,833 |
| Surgical activity | 12,516 | 11,613 |
| Admissions | 14,067 | 8874 |
| Deliveries | 2567 | 961 |
| Laboratory diagnostic tests | 3,966,819 | 4,638,51 |
| Diagnostic radiology tests | 165,680 | 281,883 |
| Healthcare centers included | (1) Adra: Adra health center and La Curva and Puente del Rio clinics. (2) Berja: Berja Health Center and the clinics of Alcolea, Balanegra, Dalías, Fondón, Láujar de Andarax, Paterna del Rio, Bayárcal and Fuente Victoria. (3) El Ejido: Health Centers of El Ejido, El Ejido Sur, Las Norias and Santa María del Águila and the clinics of Almerimar, Balerma, Matagorda-Guardias Viejas, Pampanico, San Agustín and Santo Domingo. (4) Roquetas de Mar: Aguadulce Sur, El Parador, Las Marinas, Roquetas and Roquetas Sur health centers and the clinics of Aguadulce, Cortijos Marín, Felix, El Solanillo and Enix auxiliary. (5) Vícar: La Gangosa, La Mojonera and Puebla de Vícar health centers and the clinics of Barrio Archilla-Cañada Sebastiana, Cabañuelas Bajas, Llanos de Vícar, Venta del Viso and La Envía. | 1. In the province of Jaén: the Alto Guadalquivir Hospital and the High Resolution Hospitals of Sierra de Segura, Alcaudete and Alcalá la Real. 2. In the province of Cordoba: the Montilla Hospital and the Puente Genil and Valle del Guadiato High Resolution Hospitals. |
| Poniente Hospital | Alto Guadalquivir Health Agency | |||||||
|---|---|---|---|---|---|---|---|---|
| 2019 | 2020 | Difference | p-Value | 2019 | 2020 | Difference | p-Value | |
| No. of external consultations cited * | 24,690.33 ± 4070.60 | 20,218.17 ± 4189.12 | −4472.17 ± 3498.28 | <0.001 | 29,270.42 ± 4433.65 | 24,560.33 ± 5576.88 | −4710.08 ± 5766.78 | <0.001 |
| No. of external consultations cited-not presented * | 2642.17 ± 456.87 | 1760.08 ± 535.28 | −882.08 ± 471.99 | <0.001 | 2899.67 ± 402.60 | 1150.17 ± 323.43 | −1749.50 ± 420.08 | <0.001 |
| No. Surgical Interventions * | 1085.75 ± 255.33 | 746.75 ± 256.05 | −339.00 ± 230.92 | <0.001 | 960.08 ± 208.16 | 723.25 ± 300.49 | −236.83 ± 313.50 | <0.01 |
| No. Diagnostic tests (not RX or Laboratory) * | 2349.92 ± 394.03 | 1915.25 ± 480.53 | −434.67 ± 459.88 | <0.01 | 1081.92 ± 159.64 | 1414.08 ± 489.00 | 332.17 ± 485.34 | <0.05 |
| No. Emergencies * | 14,637.42 ± 822.10 | 9964.67 ± 4179.52 | −4672.75 ± 4046.89 | <0.01 | 21,835.08 ± 2117.57 | 14,246.17 ± 5447.95 | −7588.92 ± 4548.63 | <0.001 |
| Number of external telephone inquiries * | 40.42 ± 22.26 | 5850.83 ± 3409.88 | 5810.42 ± 3404.99 | <0.001 | 0.000 ± 0.000 | 232.25 ± 206.02 | 232.25 ± 206.02 | <0.01 |
| No. Radiodiagnosis tests * | 19,032.33 ± 1467.06 | 16,261.33 ± 3806.65 | −2771.00 ± 4442.76 | 0.054 | 23,241.33 ± 1787.42 | 19,351.50 ± 4520.03 | −3889.83 ± 4692.48 | <0.05 |
| No. of laboratory tests * | 428,910.58 ± 52,088.19 | 347,075.00 ± 79,617.42 | −81,835.58 ± 88,169.37 | <0.01 | 882,306.67 ± 1,451,828.23 | 558,611.33 ± 943,747.59 | −323,695.33 ± 523,559.12 | <0.001 |
| No. patients on the waiting list * | 4315.42 ± 386.552 | 3656.33 ± 190.58 | −659.083 ± 391.70 | <0.001 | 16,224.58 ± 1522.70 | 15,557.25 ± 1784.66 | −667.33 ± 2921.43 | 0.446 |
| 2019 | 2020 | |||||||
|---|---|---|---|---|---|---|---|---|
| Alto Guadalquivir Health Agency | Poniente Hospital | Total | p-Value | Alto Guadalquivir Health Agency | Poniente Hospital | Total | p-Value | |
| No. of external consultations cited * | 29,270.41 ± 4433.65 | 24,690.33 ± 4070.60 | 26,980.38 ± 4774.75 | 0.015 | 24,560.33 ± 5576.88 | 20,218.17 ± 4189.12 | 22,389.25 ± 5309.06 | 0.042 |
| No. of external consultations cited-not presented * | 2899.67 ± 402.60 | 2642.17 ± 456.87 | 2770.92 ± 441.19 | 0.128 | 1150.17 ± 323.43 | 1760.08 ± 535.28 | 1455.13 ± 533.01 | <0.01 |
| No. Surgical Interventions * | 960.08 ± 208.16 | 1085.75 ± 255.33 | 1022.92 ± 236.69 | 0.200 | 723.25 ± 300.49 | 746.75 ± 256.05 | 735.00 ± 273.28 | 0.839 |
| No. Diagnostic tests (not RX or Laboratory) * | 1081.92 ± 159.638 | 2349.92 ± 394.03 | 1715.92 ± 711.25 | <0.001 | 1414.08 ± 489.00 | 1915.25 ± 480.53 | 1664.67 ± 538.81 | 0.019 |
| No. Emergencies * | 21,835.08 ± 2117.57 | 14,637.42 ± 822.10 | 18,236.25 ± 3997.81 | <0.001 | 14,246.17 ± 5447.95 | 9964.67 ± 4179.52 | 12,105.42 ± 5227.94 | 0.042 |
| Number of external telephone inquiries * | 0.000 ± 0.00 | 40.42 ± 22.26 | 20.21 ± 25.75 | <0.001 | 232.25 ± 206.02 | 5850.83 ± 3409.88 | 3041.54 ± 3717.05 | <0.01 |
| No. Radiodiagnosis tests * | 23,241.33 ± 1787.42 | 19,032.33 ± 1467.06 | 21,136.83 ± 2679.33 | <0.01 | 19,351.50 ± 4520.03 | 16,261.33 ± 3806.65 | 17,806.42 ± 4380.93 | 0.060 |
| No. of laboratory tests * | 882,306.67 ± 1,451,828.23 | 428,910.58 ± 52,088.19 | 655,608.63 ± 1,031,021.24 | 0.198 | 558,611.33 ± 943,747.59 | 347,075.00 ± 79,617.43 | 452,843.17 ± 663,831.72 | 0.242 |
| No. patients on the waiting list * | 16,224.58 ± 1522.70 | 4315.42 ± 386.55 | 10,270.00 ± 6178.92 | <0.001 | 15,557.25 ± 1784.66 | 3656.33 ± 190.58 | 9606.79 ± 6203.88 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lopez-Villegas, A.; Bautista-Mesa, R.J.; Baena-Lopez, M.A.; Garzon-Miralles, A.; Castellano-Ortega, M.A.; Leal-Costa, C.; Peiro, S. Impact of the COVID-19 Pandemic on Healthcare Activity in the Regional Hospitals of Andalusia (Spain). J. Clin. Med. 2022, 11, 363. https://doi.org/10.3390/jcm11020363
Lopez-Villegas A, Bautista-Mesa RJ, Baena-Lopez MA, Garzon-Miralles A, Castellano-Ortega MA, Leal-Costa C, Peiro S. Impact of the COVID-19 Pandemic on Healthcare Activity in the Regional Hospitals of Andalusia (Spain). Journal of Clinical Medicine. 2022; 11(2):363. https://doi.org/10.3390/jcm11020363
Chicago/Turabian StyleLopez-Villegas, Antonio, Rafael Jesus Bautista-Mesa, Miguel Angel Baena-Lopez, Antonio Garzon-Miralles, Miguel Angel Castellano-Ortega, Cesar Leal-Costa, and Salvador Peiro. 2022. "Impact of the COVID-19 Pandemic on Healthcare Activity in the Regional Hospitals of Andalusia (Spain)" Journal of Clinical Medicine 11, no. 2: 363. https://doi.org/10.3390/jcm11020363
APA StyleLopez-Villegas, A., Bautista-Mesa, R. J., Baena-Lopez, M. A., Garzon-Miralles, A., Castellano-Ortega, M. A., Leal-Costa, C., & Peiro, S. (2022). Impact of the COVID-19 Pandemic on Healthcare Activity in the Regional Hospitals of Andalusia (Spain). Journal of Clinical Medicine, 11(2), 363. https://doi.org/10.3390/jcm11020363