

Erector Spinae Plane Block Decreases Chronic Postoperative Pain Severity in Patients Undergoing Coronary Artery Bypass Grafting
 ,
,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
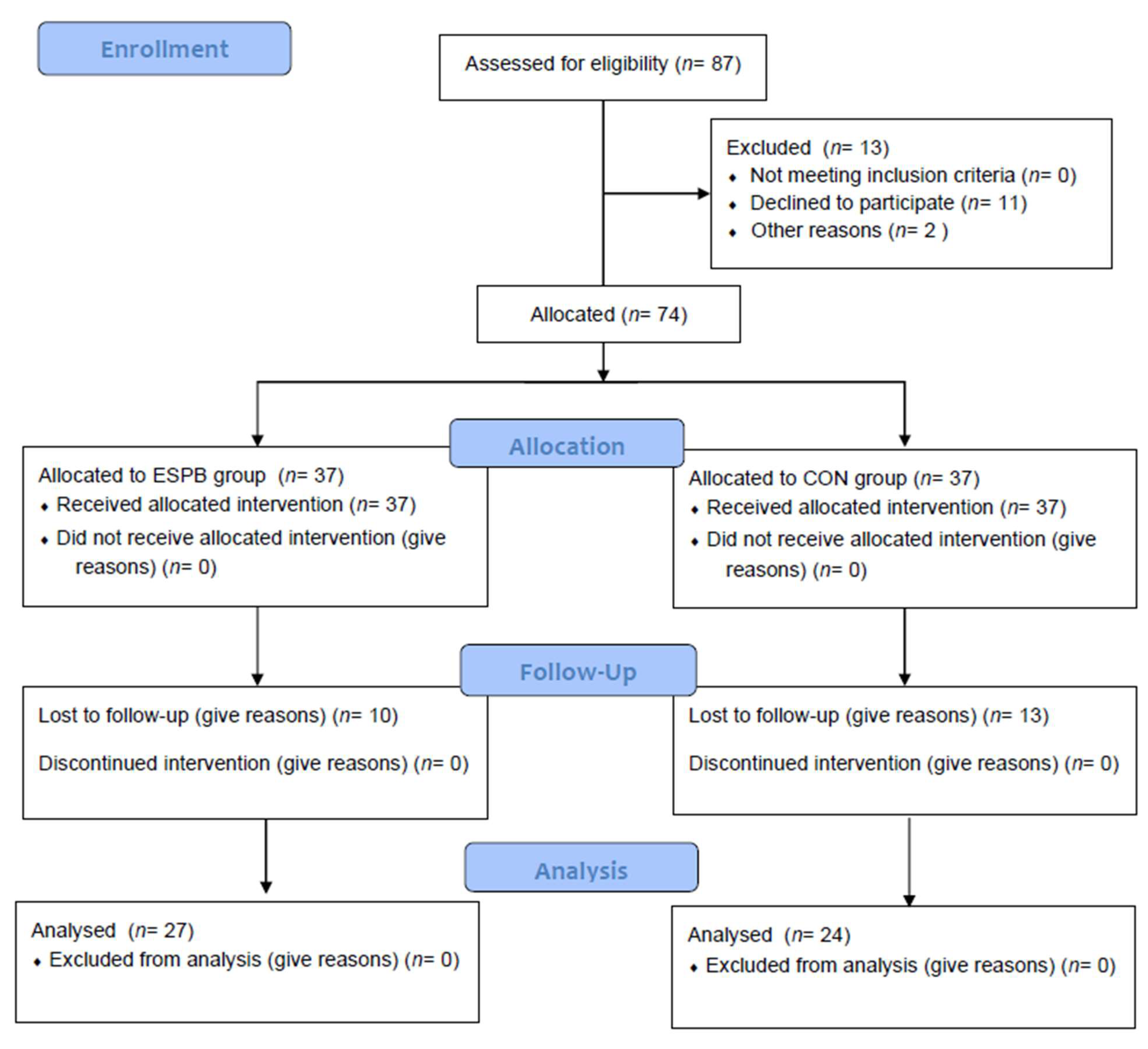
2.1. Participants
2.2. General Anesthesia
2.3. Regional Block and Postoperative Care
2.4. Persistent Postoperative Pain
2.5. Outcomes
2.6. Statistics
3. Results
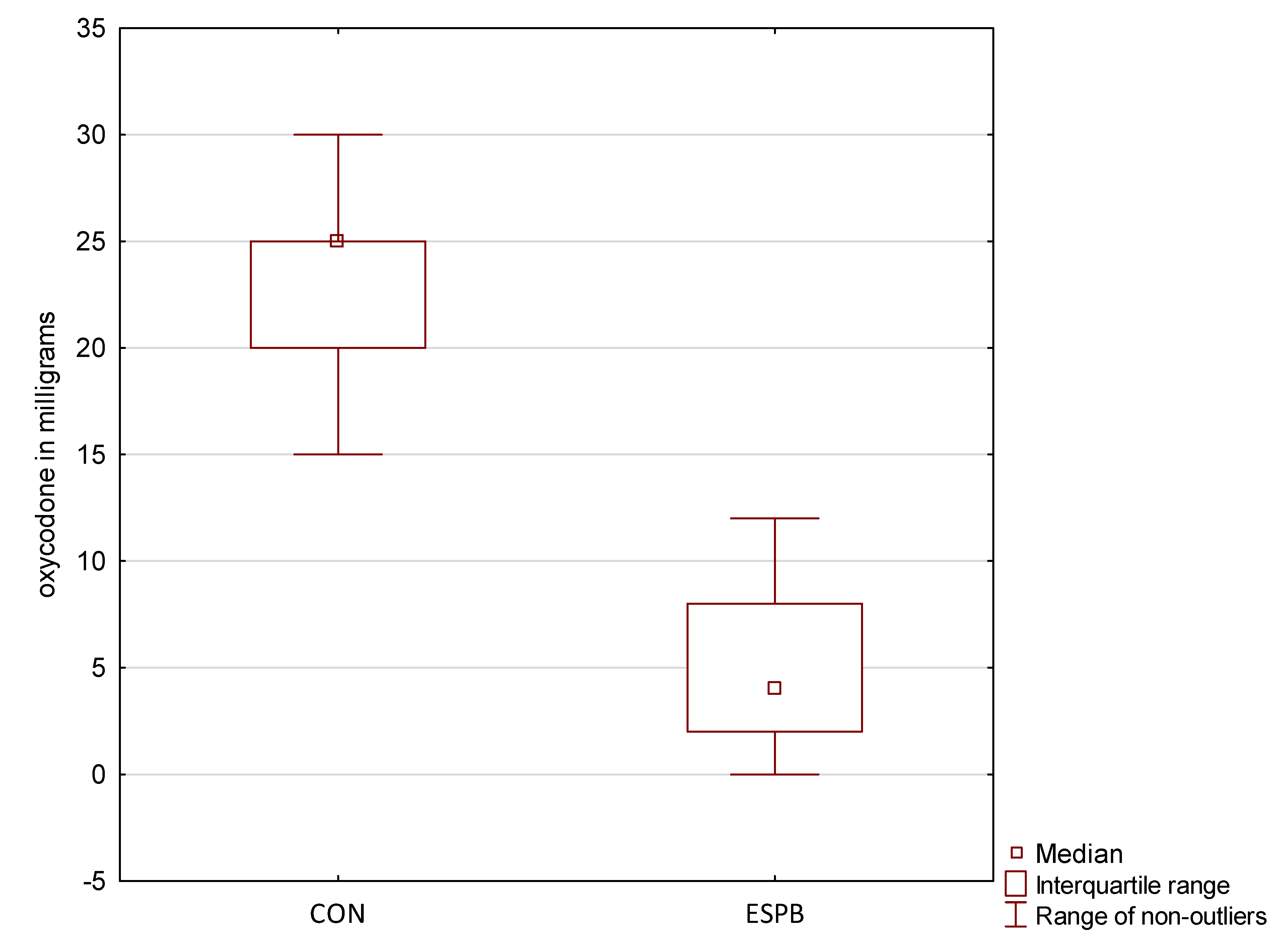
3.1. Primary Outcome
3.2. Secondary Outcomes
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Head, S.J.; Milojevic, M.; Taggart, D.P.; Puskas, J.D. Current practice of state-of-the-art surgical coronary revascularization. Circulation 2017, 136, 1331–1345. [Google Scholar] [CrossRef] [PubMed]
- Kalso, E.; Mennander, S.; Tasmuth, T. Chronic post-sternotomy pain. Acta Anaesthesiol. Scand. 2001, 45, 935–939. [Google Scholar] [CrossRef] [PubMed]
- Eisenberg, E.; Pultorak, Y.; Pud, D.; Bar-El, Y. Prevalence and characteristics of post coronary artery bypass graft surgery pain (PCP). Pain 2001, 92, 11–17. [Google Scholar] [CrossRef]
- Andreae, M.H.; Andreae, D.A. Regional anaesthesia to prevent chronic pain after surgery: A Cochrane systematic review and meta-analysis. Br. J. Anaesth. 2013, 111, 711–720. [Google Scholar] [CrossRef]
- Borys, M.; Hanych, A.; Czuczwar, M. Paravertebral block versus preemptive ketamine effect on pain intensity after posterolateral thoracotomies: A randomized controlled trial. J. Clin. Med. 2020, 9, 793. [Google Scholar] [CrossRef]
- Forero, M.; Rajarathinam, M.; Adhikary, S.; Chin, J.K. Continuous erector spinae plane block for rescue analgesia in thoracotomy after epidural failure: A case report. A A Case. Rep. 2017, 8, 254–256. [Google Scholar] [CrossRef]
- Nagaraja, P.S.; Ragavendran, S.; Singh, N.G.; Omshubham, A.; Bhavya, G.; Manjunath, N.; Rajesh, K. Comparison of continuous thoracic epidural analgesia with bilateral erector spinae plane block for perioperative pain management in cardiac surgery. Ann. Card. Anaesth. 2018, 21, 323–327. [Google Scholar]
- Krishna, S.N.; Chauhan, S.; Bhoi, D.; Kaushal, B.; Hasija, S.; Sangdup, T.; Bisoi, A.K. Bilateral erector spinae plane block for acute post-surgical pain in adult cardiac surgical patients: A randomized controlled trial. J. Cardiothorac. Vasc. Anesth. 2019, 33, 368–375. [Google Scholar] [CrossRef]
- Borys, M.; Gawęda, B.; Horeczy, B.; Kolowca, M.; Olszówka, P.; Czuczwar, M. Erector spinae-plane block as an analgesic alternative in patients undergoing mitral and/or tricuspid valve repair through a right mini-thoracotomy—An observational cohort study. Videosurg. Other Miniinvasive Tech. 2020, 15, 208–214. [Google Scholar] [CrossRef]
- Gawęda, B.; Borys, M.; Belina, B.; Bąk, J.; Czuczwar, M.; Wołoszczuk-Gębicka, B.; Kolowca, M.; Widenka, K. Postoperative pain treatment with erector spinae plane block and pectoralis nerve blocks in patients undergoing mitral/tricuspid valve repair—a randomized controlled trial. BMC Anesthesiol. 2020, 20, 51. [Google Scholar] [CrossRef]
- Borys, M.; Żurek, S.; Kurowicki, A.; Horeczy, B.; Bielina, B.; Sejboth, J.; Wołoszczuk-Gębicka, B.; Czuczwar, M.; Widenka, K. Implementation of enhanced recovery after surgery (ERAS) protocol in off-pump coronary artery bypass graft surgery.A prospective cohort feasibility study. Anaesthesiol. Intensive Ther. 2020, 52, 10–14. [Google Scholar] [CrossRef]
- Bouhassira, D.; Attal, N.; Fermanian, J.; Alchaar, H.; Gautron, M.; Masquelier, E.; Rostaing, S.; Lanteri-Minet, M.; Collin, E.; Grisart, J.; et al. Development and validation of the neuropathic pain symptom inventory. Pain 2004, 108, 248–257. [Google Scholar] [CrossRef]
- Borys, M.; Potręć-Studzińska, B.; Wiech, M.; Piwowarczyk, P.; Sysiak-Sławecka, J.; Rypulak, E.; Gęca, T.; Kwaśniewska, A.; Czuczwar, M. Transversus abdominis plane block and quadratus lumborum block did not reduce the incidence or severity of chronic postsurgical pain following cesarean section: A prospective, observational study. Anaesthesiol. Intensive Ther. 2019, 51, 257–261. [Google Scholar] [CrossRef]
- Borys, M.; Zamaro, A.; Horeczy, B.; Gęszka, E.; Janiak, M.; Węgrzyn, P.; Czuczwar, M.; Piwowarczyk, P. Quadratus lumborum and transversus abdominis plane blocks and their impact on acute and chronic pain in patients after cesarean section: A randomized controlled Study. Int. J. Environ. Res. Public Health 2021, 18, 3500. [Google Scholar] [CrossRef]
- Weinstein, E.; Levene, J.; Cohen, M.; Andreae, D.; Chao, J.; Johnson, M.; Hall, C.; Andreae, M. Local anaesthetics and regional anaesthesia versus conventional analgesia for preventing persistent postoperative pain in adults and children. Cochrane Database Syst. Rev. 2018. [Google Scholar] [CrossRef]
- Lu, Y.; Wang, X.; Lai, R.; Huang, W.; Xu, M. Correlation of acute pain treatment to occurrence of chronic pain in tumor patients after thoracotomy. Aizheng 2008, 27, 206–209. [Google Scholar]
- Kairaluoma, P.; Bachmann, M.; Rosenberg, P.; Pere, P. Preincisional paravertebral block reduces the prevalence of chronic pain after breast surgery. Anesth. Analg. 2006, 103, 703–708. [Google Scholar] [CrossRef]
- Borys, M.; Szajowska, P.; Jednakiewicz, M.; Wita, G.; Czarnik, T.; Mieszkowski, M.; Tuyakov, B.; Gałkin, P.; Rahnama-Hezavah, M.; Czuczwar, M.; et al. Quadratus Lumborum Block Reduces Postoperative Opioid Consumption and Decreases Persistent Postoperative Pain Severity in Patients Undergoing Both Open and Laparoscopic Nephrectomies-A Randomized Controlled Trial. J. Clin. Med. 2021, 10, 3590. [Google Scholar] [CrossRef]
- Kleiman, A.M.; Sanders, D.T.; Nemergut, E.C.; Huffmyer, J.L. Chronic Poststernotomy Pain: Incidence, Risk Factors, Treatment, Prevention, and the Anesthesiologist’s Role. Reg. Anesth. Pain Med. 2017, 42, 698–708. [Google Scholar] [CrossRef]
- Carley, M.E.; Chaparro, L.E.; Choinière, M.; Kehlet, H.; Moore, R.A.; Van Den Kerkhof, E.; Gilron, I. Pharmacotherapy for the Prevention of Chronic Pain after Surgery in Adults: An Updated Systematic Review and Meta-analysis. Anesthesiology 2021, 135, 304–325. [Google Scholar] [CrossRef]
- Leong, R.; Tan, E.; Wong, S.; Tan, K.; Liu, C. Efficacy of erector spinae plane block for analgesia in breast surgery: A systematic review and meta-analysis. Anaesthesia 2021, 76, 404–413. [Google Scholar] [CrossRef] [PubMed]
- Uppal, V.; Retter, S.; Kehoe, E.; McKeen, D.M. Quadratus lumborum block for postoperative analgesia: A systematic review and meta-analysis. Can. J. Anaesth. 2020, 67, 1557–1575. [Google Scholar] [CrossRef] [PubMed]
- Macaire, P.; Ho, N.; Nguyen, T.; Nguyen, B.; Vu, V.; Quach, C.; Roques, V.; Capdevila, X. Ultrasound-Guided Continuous Thoracic Erector Spinae Plane Block Within an Enhanced Recovery Program Is Associated with Decreased Opioid Consumption and Improved Patient Postoperative Rehabilitation After Open Cardiac Surgery-A Patient-Matched, Controlled Before-and-After Study. J. Cardiothorac. Vasc. Anesth. 2019, 33, 1659–1667. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Parameters | ESPB | CON | p Value |
|---|---|---|---|
| Number of patients | 27 | 24 | |
| Male (%) | 24 (88.9) | 22 (91.7) | 1.0 |
| Age (years) | 64.7 (62.0–67.4) | 67.1 (63.4–70.7) | 0.28 |
| Weight (kg) | 85.2 (80.4–90.0) | 83.7 (77.9–89.4) | 0.68 |
| Height (cm) | 171.1 (167.7–174.5) | 170.6 (167.1–174.1) | 0.85 |
| BMI | 29.1 (27.8–30.3) | 28.6 (27.1–30.1) | 0.65 |
| ASA | 3 (2–3) | 3 (3–3) | 0.45 |
| Anesthesia time (minutes) | 194 (174–215) | 201 (141–185) | 0.63 |
| Surgery time (minutes) | 159 (140–179) | 163 (177–225) | 0.79 |
| Intraoperative fentanyl (mcg) | 381 (359–404) | 499 (463–535) | <0.001 |
| After Discharge | ESPB | CON | p Value |
|---|---|---|---|
| 1 month | 1 (0–2) * | 4 (3–6) | <0.001 |
| 3 months | 0 (0–1) * | 4 (2–6) | <0.001 |
| 6 months | 0 (0–0) * | 2 (14) | <0.001 |
| After Discharge | Number of Patients (%) | p Value | |
|---|---|---|---|
| ESPB | CON | ||
| 1 month | 17 (63) * | 23 (96) | <0.01 |
| 3 months | 8 (30) * | 23 (96) | <0.001 |
| 6 months | 6 (22) * | 22 (92) | <0.001 |
| Hours after Extubation | ESPB | CON | p Value |
|---|---|---|---|
| 0 | 3.0 (2.0−4.5) * | 5.0 (4.0−5.8) | <0.001 |
| 6 | 2.5 (2.0−4.0) * | 4.5 (3.5–5.0) | <0.001 |
| 12 | 3.0 (2.0−3.5) * | 4.0 (3.0−4.0) | <0.01 |
| 18 | 2.0 (0.0−3.0) * | 3.0 (2.0−4.0) | <0.01 |
| 24 | 0.0 (0.0−1.5) * | 3.0 (1.0−3.5) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wiech, M.; Żurek, S.; Kurowicki, A.; Horeczy, B.; Czuczwar, M.; Piwowarczyk, P.; Widenka, K.; Borys, M. Erector Spinae Plane Block Decreases Chronic Postoperative Pain Severity in Patients Undergoing Coronary Artery Bypass Grafting. J. Clin. Med. 2022, 11, 5949. https://doi.org/10.3390/jcm11195949
Wiech M, Żurek S, Kurowicki A, Horeczy B, Czuczwar M, Piwowarczyk P, Widenka K, Borys M. Erector Spinae Plane Block Decreases Chronic Postoperative Pain Severity in Patients Undergoing Coronary Artery Bypass Grafting. Journal of Clinical Medicine. 2022; 11(19):5949. https://doi.org/10.3390/jcm11195949
Chicago/Turabian StyleWiech, Marcin, Sławomir Żurek, Arkadiusz Kurowicki, Beata Horeczy, Mirosław Czuczwar, Paweł Piwowarczyk, Kazimierz Widenka, and Michał Borys. 2022. "Erector Spinae Plane Block Decreases Chronic Postoperative Pain Severity in Patients Undergoing Coronary Artery Bypass Grafting" Journal of Clinical Medicine 11, no. 19: 5949. https://doi.org/10.3390/jcm11195949
APA StyleWiech, M., Żurek, S., Kurowicki, A., Horeczy, B., Czuczwar, M., Piwowarczyk, P., Widenka, K., & Borys, M. (2022). Erector Spinae Plane Block Decreases Chronic Postoperative Pain Severity in Patients Undergoing Coronary Artery Bypass Grafting. Journal of Clinical Medicine, 11(19), 5949. https://doi.org/10.3390/jcm11195949