

Features of Masticatory Behaviors in Older Adults with Oral Hypofunction: A Cross-Sectional Study

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Survey Items
2.2.1. Poor Oral Hygiene
2.2.2. Oral Dryness
2.2.3. Occlusal Force
2.2.4. Tongue–Lip Motor Function
2.2.5. Maximum Tongue Pressure
2.2.6. Masticatory Performance
2.2.7. Swallowing Function
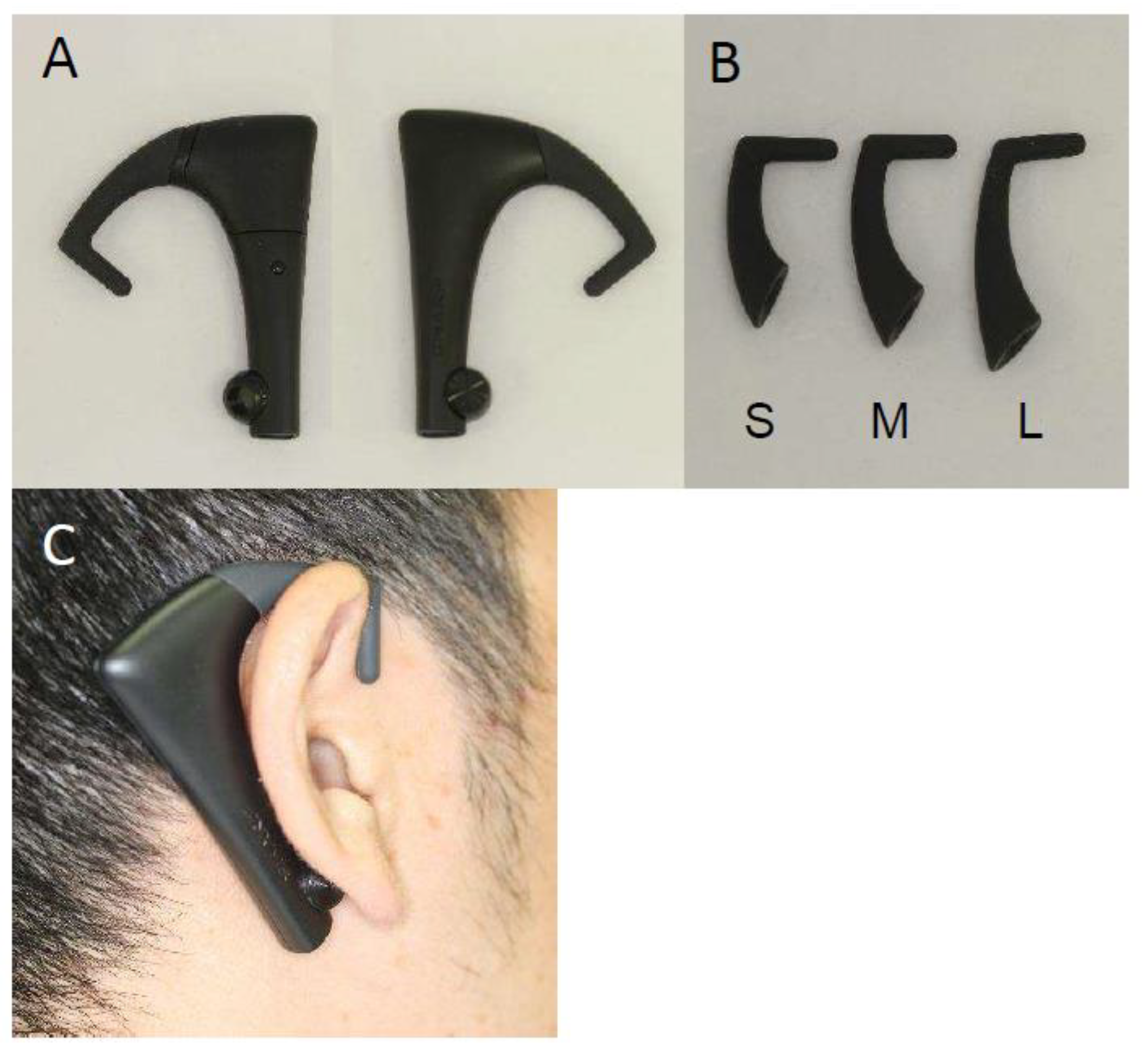
2.2.8. Masticatory Behaviors
- Number of chews (no.): The total number of chewing cycles during the time to eat 1 rice ball.
- Number of chews per bite (no.): Mean number of chews per bite which is an uptake action.
- Chewing rate (no./min): The number of chews per minutes calculated by dividing by total chewing time.
- Total chewing time (s): The time taken to eat 1 rice ball.
2.3. Analysis
3. Results
3.1. Participants’ Oral Condition and Oral Hypofunction
3.2. Comparison of Masticatory Behaviors in Participants with and without Oral Hypofunction
3.3. Comparison of Masticatory Behaviors by Oral Hypofunction Sub-Symptoms
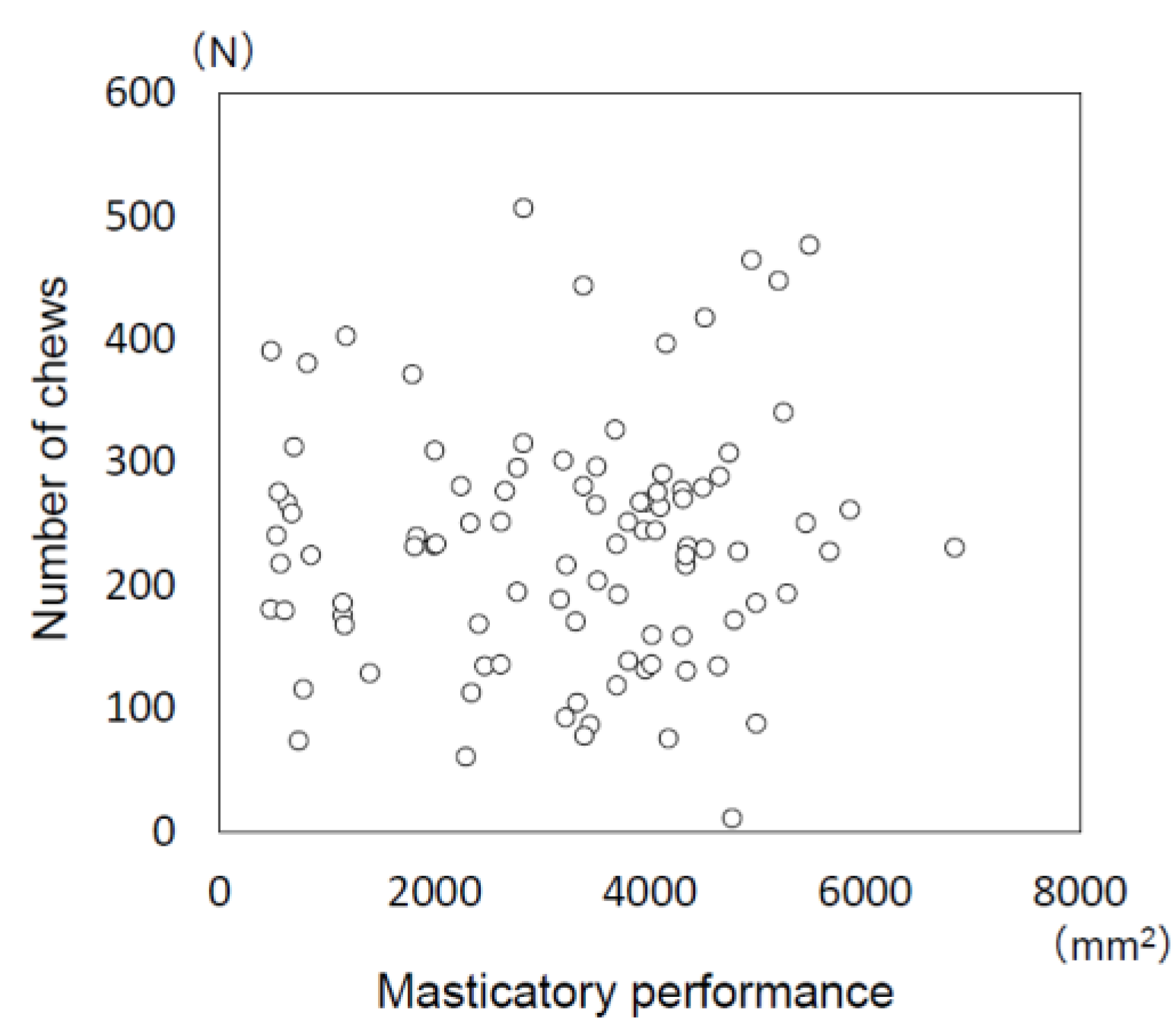
3.4. Relationship between Masticatory Performance and Number of Chews
4. Discussion
4.1. Measurement of Masticatory Behaviors
4.2. Oral Hypofunction
4.3. The Characteristics of Masticatory Behaviors in Older Adults with Oral Hypofunction (and Its Sub-Symptoms)
4.4. Relationship between Masticatory Behaviors and Masticatory Performance
4.5. Limitations and Future Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Matsuyama, Y.; Aida, J.; Watt, R.G.; Tsuboya, T.; Koyama, S.; Sato, Y.; Kondo, K.; Osaka, K. Dental Status and Compression of Life Expectancy with Disability. J. Dent. Res. 2017, 96, 1006–1013. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, Y.; Okada, K.; Kondo, M.; Matsushita, T.; Nakazawa, S.; Yamazaki, Y. Oral health for achieving longevity. Geriatr. Gerontol. Int. 2020, 20, 526–538. [Google Scholar] [CrossRef] [PubMed]
- Hatta, K.; Ikebe, K. Association between oral health and sarcopenia: A literature review. J. Prosthodont. Res. 2021, 65, 131–136. [Google Scholar] [CrossRef]
- Kugimiya, Y.; Iwasaki, M.; Ohara, Y.; Motokawa, K.; Edahiro, A.; Shirobe, M.; Watanabe, Y.; Obuchi, S.; Kawai, H.; Fujiwara, Y.; et al. Relationship between Oral Hypofunction and Sarcopenia in Community-Dwelling Older Adults: The Otassha Study. Int. J. Environ. Res. Public Health 2021, 18, 6666. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, M.; Hiraoka, A.; Takeda, C.; Mori, T.; Maruyama, M.; Yoshikawa, M.; Tsuga, K. Oral hypofunction and its relation to frailty and sarcopenia in community-dwelling older people. Gerodontology 2022, 39, 26–32. [Google Scholar] [CrossRef]
- Minakuchi, S.; Tsuga, K.; Ikebe, K.; Ueda, T.; Tamura, F.; Nagao, K.; Furuya, J.; Matsuo, K.; Yamamoto, K.; Kanazawa, M.; et al. Oral hypofunction in the older population: Position paper of the Japanese Society of Gerodontology in 2016. Gerodontology 2018, 35, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Palmer, J.B.; Rudin, N.J.; Lara, G.; Crompton, A.W. Coordination of mastication and swallowing. Dysphagia 1992, 7, 187–200. [Google Scholar] [CrossRef] [PubMed]
- Goncalves, T.; Schimmel, M.; van der Bilt, A.; Chen, J.; van der Glas, H.W.; Kohyama, K.; Hennequin, M.; Peyron, M.A.; Woda, A.; Leles, C.R.; et al. Consensus on the terminologies and methodologies for masticatory assessment. J. Oral Rehabil. 2021, 48, 745–761. [Google Scholar] [CrossRef]
- Otsuka, R.; Tamakoshi, K.; Yatsuya, H.; Murata, C.; Sekiya, A.; Wada, K.; Zhang, H.M.; Matsushita, K.; Sugiura, K.; Takefuji, S.; et al. Eating fast leads to obesity: Findings based on self-administered questionnaires among middle-aged Japanese men and women. J. Epidemiol. 2006, 16, 117–124. [Google Scholar] [CrossRef]
- Berzlanovich, A.M.; Fazeny-Dorner, B.; Waldhoer, T.; Fasching, P.; Keil, W. Foreign body asphyxia: A preventable cause of death in the elderly. Am. J. Prev. Med. 2005, 28, 65–69. [Google Scholar] [CrossRef]
- Kikutani, T.; Tamura, F.; Takahashi, Y.; Konishi, K.; Hamada, R. A novel rapid oral bacteria detection apparatus for effective oral care to prevent pneumonia. Gerodontology 2012, 29, e560–e565. [Google Scholar] [CrossRef] [PubMed]
- Yamada, H.; Nakagawa, Y.; Nomura, Y.; Yamamoto, K.; Suzuki, M.; Watanabe, N.Y.; Saito, I.; Seto, K. Preliminary results of moisture checker for Mucus in diagnosing dry mouth. Oral Dis. 2005, 11, 405–407. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Kumagai, H.; Watanabe, T.; Uchida, T.; Nagao, M. Evaluation of complete denture occlusal contacts using pressure-sensitive sheets. Int. J. Prosthodont. 1997, 10, 386–391. [Google Scholar]
- Yamada, A.; Kanazawa, M.; Komagamine, Y.; Minakuchi, S. Association between tongue and lip functions and masticatory performance in young dentate adults. J. Oral Rehabil. 2015, 42, 833–839. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, R.; Tsuga, K.; Hosokawa, R.; Yoshida, M.; Sato, Y.; Akagawa, Y. A novel handy probe for tongue pressure measurement. Int. J. Prosthodont. 2002, 15, 385–388. [Google Scholar]
- Nokubi, T.; Yoshimuta, Y.; Nokubi, F.; Yasui, S.; Kusunoki, C.; Ono, T.; Maeda, Y.; Yokota, K. Validity and reliability of a visual scoring method for masticatory ability using test gummy jelly. Gerodontology 2013, 30, 76–82. [Google Scholar] [CrossRef]
- Salazar, S.; Hori, K.; Uehara, F.; Okawa, J.; Shibata, A.; Higashimori, M.; Nokubi, T.; Ono, T. Masticatory performance analysis using photographic image of gummy jelly. J. Prosthodont. Res. 2020, 64, 48–54. [Google Scholar] [CrossRef]
- Belafsky, P.C.; Mouadeb, D.A.; Rees, C.J.; Pryor, J.C.; Postma, G.N.; Allen, J.; Leonard, R.J. Validity and reliability of the Eating Assessment Tool (EAT-10). Ann. Otol. Rhinol. Laryngol. 2008, 117, 919–924. [Google Scholar] [CrossRef]
- Hori, K.; Uehara, F.; Yamaga, Y.; Yoshimura, S.; Okawa, J.; Tanimura, M.; Ono, T. Reliability of a novel wearable device to measure chewing frequency. J. Prosthodont. Res. 2021, 65, 340–345. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Zhu, Y.; Hollis, J.H. Tooth loss and its association with dietary intake and diet quality in American adults. J. Dent. 2014, 42, 1428–1435. [Google Scholar] [CrossRef] [PubMed]
- Amagai, N.; Komagamine, Y.; Kanazawa, M.; Iwaki, M.; Jo, A.; Suzuki, H.; Minakuchi, S. The effect of prosthetic rehabilitation and simple dietary counseling on food intake and oral health related quality of life among the edentulous individuals: A randomized controlled trial. J. Dent. 2017, 65, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Doi, T.; Hinode, D.; Nakae, H.; Yoshioka, M.; Matsuyama, M.; Iga, H.; Fukushima, Y. Relationship between Chewing Behavior and Oral Conditions in Elementary School Children Based on the “Chewing 30” Program: An Intervention Study. J. Dent. Health 2016, 66, 438–444. [Google Scholar] [CrossRef]
- Le Reverend, B.; Saucy, F.; Moser, M.; Loret, C. Adaptation of mastication mechanics and eating behaviour to small differences in food texture. Physiol. Behav. 2016, 165, 136–145. [Google Scholar] [CrossRef]
- Mioche, L.; Bourdiol, P.; Martin, J.F.; Noel, Y. Variations in human masseter and temporalis muscle activity related to food texture during free and side-imposed mastication. Arch. Oral Biol. 1999, 44, 1005–1012. [Google Scholar] [CrossRef]
- van der Bilt, A.; Abbink, J.H. The influence of food consistency on chewing rate and muscular work. Arch. Oral Biol. 2017, 83, 105–110. [Google Scholar] [CrossRef]
- Goto, T.; Nakamich, A.; Watanabe, M.; Nagao, K.; Matsuyama, M.; Ichikawa, T. Influence of food volume per mouthful on chewing and bolus properties. Physiol. Behav. 2015, 141, 58–62. [Google Scholar] [CrossRef]
- Yoshimura, S.; Hori, K.; Uehara, F.; Hori, S.; Yamaga, Y.; Hasegawa, Y.; Akazawa, K.; Ono, T. Relationship between body mass index and masticatory factors evaluated with a wearable device. Sci. Rep. 2022, 12, 4117. [Google Scholar] [CrossRef]
- Uehara, F.; Hori, K.; Hasegawa, Y.; Yoshimura, S.; Hori, S.; Kitamura, M.; Akazawa, K.; Ono, T. Impact of masticatory behaviors measured with wearable device on metabolic syndrome: Cross-sectional study. JMIR Mhealth Uhealth 2022, 10, e30789. [Google Scholar] [CrossRef]
- Sun, L.; Ranawana, D.V.; Tan, W.J.; Quek, Y.C.; Henry, C.J. The impact of eating methods on eating rate and glycemic response in healthy adults. Physiol. Behav. 2015, 139, 505–510. [Google Scholar] [CrossRef]
- Iwasaki, M.; Motokawa, K.; Watanabe, Y.; Shirobe, M.; Ohara, Y.; Edahiro, A.; Kawai, H.; Fujiwara, Y.; Kim, H.; Ihara, K.; et al. Oral hypofunction and malnutrition among community-dwelling older adults: Evidence from the Otassha study. Gerodontology 2022, 39, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Hatanaka, Y.; Furuya, J.; Sato, Y.; Uchida, Y.; Shichita, T.; Kitagawa, N.; Osawa, T. Associations between Oral Hypofunction Tests, Age, and Sex. Int. J. Environ. Res. Public Health 2021, 18, 256. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Hamada, T.; Tanaka, A.; Nishi, K.; Kume, K.; Goto, Y.; Beppu, M.; Hijioka, H.; Higashi, Y.; Tabata, H.; et al. Association of Oral Hypofunction with Frailty, Sarcopenia, and Mild Cognitive Impairment: A Cross-Sectional Study of Community-Dwelling Japanese Older Adults. J. Clin. Med. 2021, 10, 1626. [Google Scholar] [CrossRef] [PubMed]
- Shimazaki, Y.; Nonoyama, T.; Tsushita, K.; Arai, H.; Matsushita, K.; Uchibori, N. Oral hypofunction and its association with frailty in community-dwelling older people. Geriatr. Gerontol. Int. 2020, 20, 917–926. [Google Scholar] [CrossRef]
- Yamaguchi, K.; Hara, K.; Nakagawa, K.; Yoshimi, K.; Ariya, C.; Nakane, A.; Furuya, J.; Tohara, H. Ultrasonography Shows Age-related Changes and Related Factors in the Tongue and Suprahyoid Muscles. J. Am. Med. Dir. Assoc. 2021, 22, 766–772. [Google Scholar] [CrossRef]
- Hiiemae, K.M.; Palmer, J.B. Food transport and bolus formation during complete feeding sequences on foods of different initial consistency. Dysphagia 1999, 14, 31–42. [Google Scholar] [CrossRef]
- Tsuga, K.; Yoshikawa, M.; Oue, H.; Okazaki, Y.; Tsuchioka, H.; Maruyama, M.; Yoshida, M.; Akagawa, Y. Maximal voluntary tongue pressure is decreased in Japanese frail elderly persons. Gerodontology 2012, 29, e1078–e1085. [Google Scholar] [CrossRef]
- Yoshida, M.; Kikutani, T.; Tsuga, K.; Utanohara, Y.; Hayashi, R.; Akagawa, Y. Decreased tongue pressure reflects symptom of dysphagia. Dysphagia 2006, 21, 61–65. [Google Scholar] [CrossRef]
- Namasivayam, A.M.; Steele, C.M.; Keller, H. The effect of tongue strength on meal consumption in long term care. Clin. Nutr. 2016, 35, 1078–1083. [Google Scholar] [CrossRef]
- Liu, H.Y.; Chen, J.H.; Hsu, K.J.; Yao, C.T.; Chen, P.H.; Hsiao, S.Y.; Lin, C.L. Decreased Tongue Pressure Associated with Aging, Chewing and Swallowing Difficulties of Community-Dwelling Older Adults in Taiwan. J. Pers. Med. 2021, 11, 653. [Google Scholar] [CrossRef]
- Murakami, K.; Hori, K.; Yoneda, H.; Sato, N.; Suwanarpa, K.; Sta Maria, M.T.; Marito, P.; Nokubi, T.; Ono, T. Compatibility of two types of gummy jelly tests for detecting decreased masticatory function. Gerodontology 2021, 39, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Yurkstas, A. Compensation for inadequate mastication. Br. Dent. J. 1951, 91, 261–262. [Google Scholar] [PubMed]
- Dahlberg, B. The masticatory habits; an analysis of the number of chews when consuming food. J. Dent. Res. 1946, 25, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Ohno, K.; Fujita, Y.; Ohno, Y.; Takeshima, T.; Maki, K. The factors related to decreases in masticatory performance and masticatory function until swallowing using gummy jelly in subjects aged 20–79 years. J. Oral Rehabil. 2020, 47, 851–861. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Hollis, J.H. Differences in chewing behaviors between healthy fully dentate young and older adults assessed by electromyographic recordings. Int. J. Food Sci. Nutr. 2015, 66, 452–457. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| All | Male | Female | ||||||
|---|---|---|---|---|---|---|---|---|
| n (%) | 98 | (100) | 33 | (33.7) | 65 | (66.3) | ||
| Age (y) | mean (SD) | 74.8 | (6.3) | 74.6 | (6.1) | 75.0 | (6.5) | |
| Oral hypofunction | n (%) | 71 | (72.4) | 23 | (69.7) | 48 | (73.8) | |
| Height (cm) | mean (SD) | 156.7 | (3.3) | 165.1 | (2.0) | 148.4 | (4.7) | |
| Body weight (kg) | mean (SD) | 59.4 | (1.5) | 63.8 | (3.3) | 55.0 | (1.8) | |
| Number of remain teeth | mean (SD) | 21.6 | (7.8) | 22.1 | (6.9) | 21.4 | (8.3) | |
| Occlusal status | Eichner A | n (%) | 53 | (54.2) | 15 | (45.5) | 38 | (58.5) |
| Eichner B | n (%) | 22 | (22.9) | 9 | (27.2) | 13 | (20.0) | |
| Eichner C | n (%) | 23 | (22.9) | 9 | (27.2) | 14 | (21.5) | |
| N of participants using removal denture | n (%) | 38 | (38.8) | 14 | (42.4) | 24 | (36.9) | |
| N of people living together | n (SD) | 2.2 | (1.2) | 2.3 | (1.3) | 2.1 | (1.1) | |
| n | Number of Chews (Cycles) | Number of Chews Per Bite (Cycles) | Chewing Rate (Cycles/min) | Total Chewing Time (s) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Median | IQR | P * | Median | IQR | P * | Median | IQR | P * | Median | IQR | P* | |||
| Oral hypofunction | Yes | 71 | 240 | (171–280) | 0.975 | 26.5 | (17.2–38.8) | 0.259 | 77.0 | (66.8–85.0) | 0.035 | 173 | (131–216) | 0.477 |
| No | 27 | 228 | (160–341) | 29.3 | (19.0–51.0) | 81.0 | (75.0–92.0) | 156 | (121–226) | |||||
| Poor oral hygiene | Yes | 91 | 232 | (168–280) | 0.327 | 27.0 | (18.0–44.0) | 0.644 | 78.7 | (70.7–88.0) | 0.200 | 165 | (127–207) | 0.161 |
| No | 7 | 262 | (169–313) | 24.0 | (22.0–28.2) | 72.1 | (66.0–81.0) | 210 | (156–258) | |||||
| Oral dryness | Yes | 56 | 230 | (161–274) | 0.208 | 27.2 | (18.7–38.5) | 0.892 | 79.5 | (73.3–87.8) | 0.277 | 163 | (128–195) | 0.088 |
| No | 42 | 251 | (171–308) | 26.2 | (18.8–45.5) | 75.9 | (65.0–84.5) | 186 | (125–252) | |||||
| Reduced occlusal force | Yes | 43 | 234 | (159–281) | 0.747 | 27.0 | (17.2–40.8) | 0.652 | 77.0 | (65.0–85.9) | 0.235 | 170 | (129–216) | 0.836 |
| No | 55 | 232 | (171–281) | 26.2 | (19.0–45.0) | 80.0 | (72.0–88.0) | 169 | (126–223) | |||||
| Decreased tongue pressure | Yes | 43 | 262 | (180–297) | 0.046 | 27.0 | (21.0–44.0) | 0.506 | 77.9 | (70.7–83.0) | 0.266 | 193 | (151–242) | 0.010 |
| No | 55 | 225 | (139–268) | 23.2 | (18.6–40.8) | 80.0 | (68.0–90.5) | 155 | (121–192) | |||||
| Decreased tongue-lip motor function | Yes | 55 | 230 | (139–277) | 0.229 | 17.1 | (16.8–43.6) | 0.594 | 75.0 | (66.0–83.0) | 0.003 | 169 | (127–210) | 0.783 |
| No | 43 | 234 | (180–316) | 19.0 | (18.7–40.8) | 82.5 | (75.0–90.7) | 164 | (129–223) | |||||
| Decreased masticatory function | Yes | 15 | 241 | (180–313) | 0.653 | 25.7 | (19.6–32.4) | 0.531 | 74.3 | (66.0–84.0) | 0.354 | 169 | (131–250) | 0.421 |
| No | 83 | 232 | (160–281) | 27.0 | (18.6–44.7) | 79.0 | (70.7–88.0) | 169 | (125–202) | |||||
| Deterioration of swallowing function | Yes | 10 | 251 | (218–267) | 0.651 | 29.7 | (22.3–47.4) | 0.439 | 80.5 | (63.7–91.8) | 0.972 | 186 | (154–212) | 0.372 |
| No | 88 | 232 | (162–287) | 26.4 | (18.2–39.4) | 78.0 | (71.0–86.2) | 164 | (126–221) | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hatayama, C.; Hori, K.; Izuno, H.; Fukuda, M.; Sawada, M.; Ujihashi, T.; Yoshimura, S.; Hori, S.; Togawa, H.; Uehara, F.; et al. Features of Masticatory Behaviors in Older Adults with Oral Hypofunction: A Cross-Sectional Study. J. Clin. Med. 2022, 11, 5902. https://doi.org/10.3390/jcm11195902
Hatayama C, Hori K, Izuno H, Fukuda M, Sawada M, Ujihashi T, Yoshimura S, Hori S, Togawa H, Uehara F, et al. Features of Masticatory Behaviors in Older Adults with Oral Hypofunction: A Cross-Sectional Study. Journal of Clinical Medicine. 2022; 11(19):5902. https://doi.org/10.3390/jcm11195902
Chicago/Turabian StyleHatayama, Chikako, Kazuhiro Hori, Hiromi Izuno, Masayo Fukuda, Misao Sawada, Takako Ujihashi, Shogo Yoshimura, Shoko Hori, Hitomi Togawa, Fumiko Uehara, and et al. 2022. "Features of Masticatory Behaviors in Older Adults with Oral Hypofunction: A Cross-Sectional Study" Journal of Clinical Medicine 11, no. 19: 5902. https://doi.org/10.3390/jcm11195902
APA StyleHatayama, C., Hori, K., Izuno, H., Fukuda, M., Sawada, M., Ujihashi, T., Yoshimura, S., Hori, S., Togawa, H., Uehara, F., & Ono, T. (2022). Features of Masticatory Behaviors in Older Adults with Oral Hypofunction: A Cross-Sectional Study. Journal of Clinical Medicine, 11(19), 5902. https://doi.org/10.3390/jcm11195902