
Impact of Using Population-Specific Cut-Points, Self-Reported Health, and Socio-Economic Parameters to Predict Sarcopenia: A Cross-Sectional Study in Community-Dwelling Kosovans Aged 60 Years and Older

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
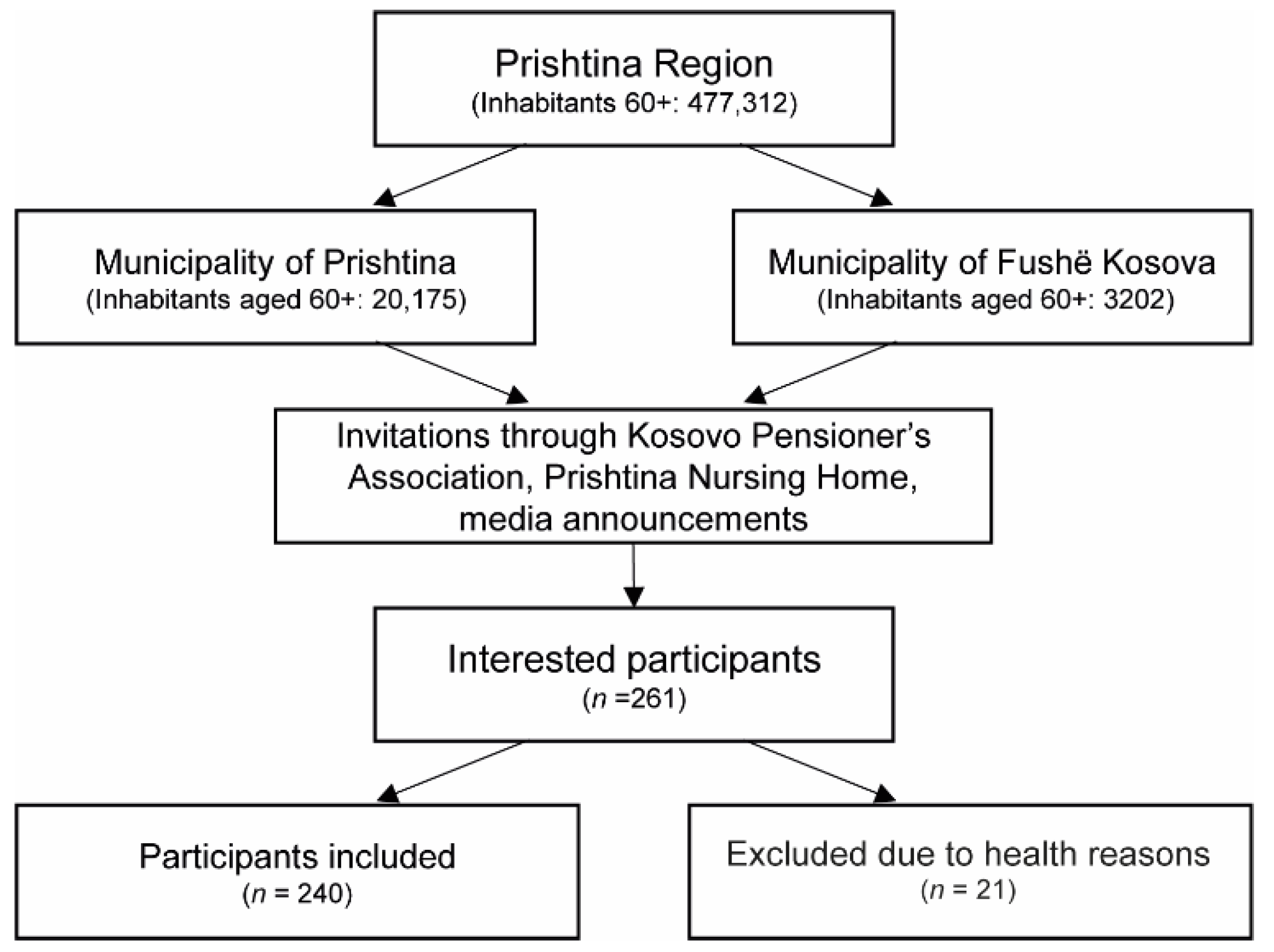
2.1. Study Design and Sample
2.2. Data Collection and Anthropometric Measurements
2.3. Physical Performance and Strength Measurements
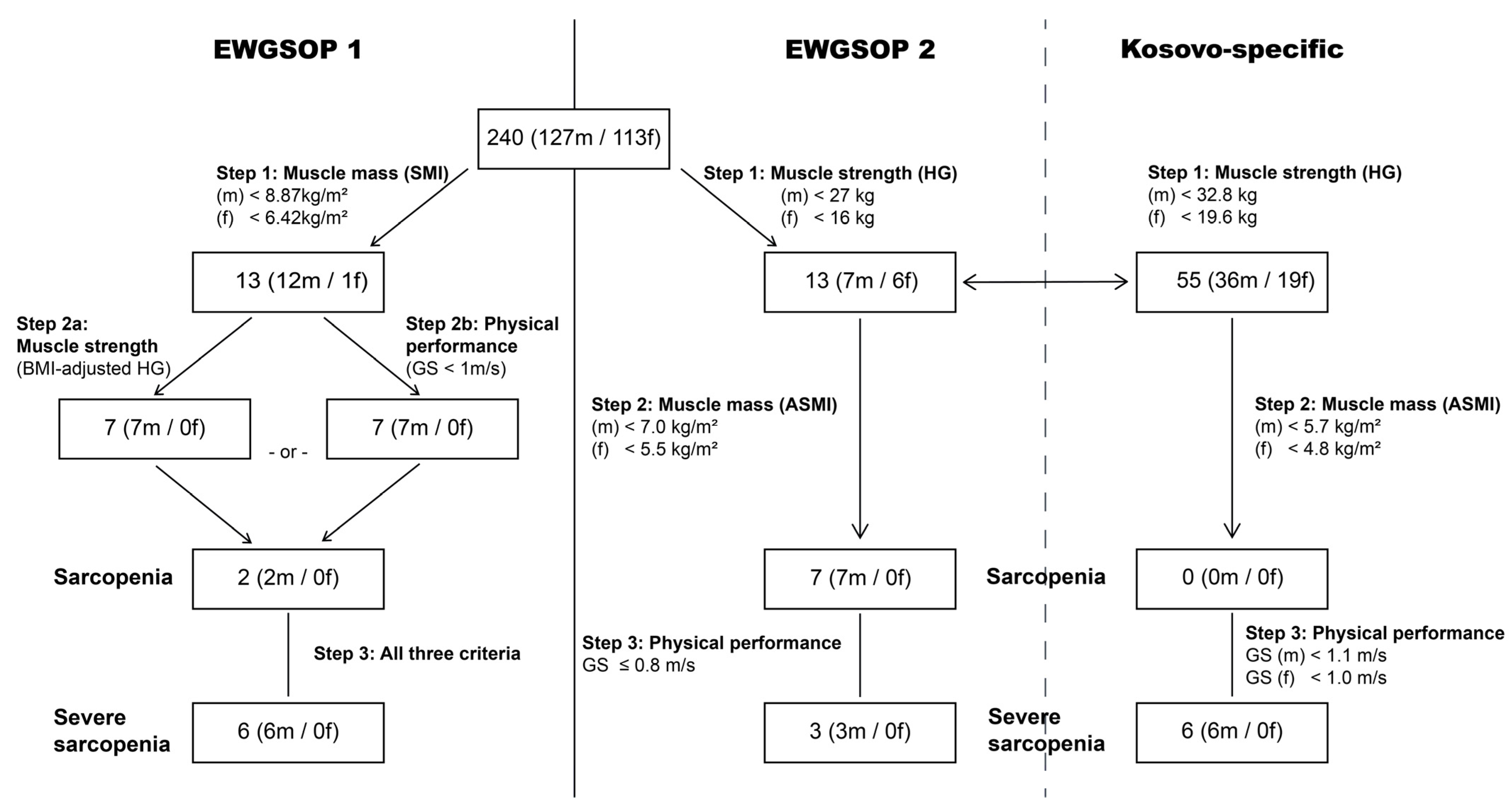
2.4. Assessment of Sarcopenia
2.5. Secondary Endpoints
2.6. Statistical Analysis
3. Results
3.1. Participants’ Characteristics
3.2. Sarcopenia and Conceptual Stages in the Study Population
3.3. Impact of EWGSOP2-Derived Sarcopenia States on Health-Related and Socio-Economic Factors
3.4. Impact of Kosovan-Specific Cut-Points on Health-Related and Socio-Economic Factors
3.5. Determinants of Sarcopenic States in Male Kosovan Older Adults (Kosovo-Derived Cut-Points)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Beaudart, C.; Gillain, S.; Petermans, J.; Reginster, J.Y.; Bruyere, O. Sarcopenia: What’s new in 2014. Rev. Med. Liege 2014, 69, 251–257. [Google Scholar]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyere, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Baumgartner, R.N.; Koehler, K.M.; Gallagher, D.; Romero, L.; Heymsfield, S.B.; Ross, R.R.; Garry, P.J.; Lindeman, R.D. Epidemiology of sarcopenia among the elderly in New Mexico. Am. J. Epidemiol. 1998, 147, 755–763. [Google Scholar] [CrossRef] [PubMed]
- Petermann-Rocha, F.; Balntzi, V.; Gray, S.R.; Lara, J.; Ho, F.K.; Pell, J.P.; Celis-Morales, C. Global prevalence of sarcopenia and severe sarcopenia: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2022, 13, 86–99. [Google Scholar] [CrossRef]
- Kenny, A.M.; Dawson, L.; Kleppinger, A.; Iannuzzi-Sucich, M.; Judge, J.O. Prevalence of sarcopenia and predictors of skeletal muscle mass in nonobese women who are long-term users of estrogen-replacement therapy. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2003, 58, M436–M440. [Google Scholar] [CrossRef]
- Geraci, A.; Calvani, R.; Ferri, E.; Marzetti, E.; Arosio, B.; Cesari, M. Sarcopenia and Menopause: The Role of Estradiol. Front. Endocrinol. 2021, 12, 682012. [Google Scholar] [CrossRef]
- Gregor, M.F.; Hotamisligil, G.S. Inflammatory mechanisms in obesity. Annu. Rev. Immunol. 2011, 29, 415–445. [Google Scholar] [CrossRef]
- Choi, K.M. Sarcopenia and sarcopenic obesity. Korean J. Intern. Med. 2016, 31, 1054–1060. [Google Scholar] [CrossRef]
- Dorosty, A.; Arero, G.; Chamar, M.; Tavakoli, S. Prevalence of Sarcopenia and Its Association with Socioeconomic Status among the Elderly in Tehran. Ethiop. J. Health Sci. 2016, 26, 389–396. [Google Scholar] [CrossRef]
- Jeng, C.; Zhao, L.J.; Wu, K.; Zhou, Y.; Chen, T.; Deng, H.W. Race and socioeconomic effect on sarcopenia and sarcopenic obesity in the Louisiana Osteoporosis Study (LOS). JCSM Clin. Rep. 2018, 3, 1–8. [Google Scholar] [CrossRef]
- Zengin, A.; Jarjou, L.M.; Prentice, A.; Cooper, C.; Ebeling, P.R.; Ward, K.A. The prevalence of sarcopenia and relationships between muscle and bone in ageing West-African Gambian men and women. J. Cachexia Sarcopenia Muscle 2018, 9, 920–928. [Google Scholar] [CrossRef] [PubMed]
- Dodds, R.M.; Granic, A.; Robinson, S.M.; Sayer, A.A. Sarcopenia, long-term conditions, and multimorbidity: Findings from UK Biobank participants. J. Cachexia Sarcopenia Muscle 2020, 11, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.; Jacob, L.; Barnett, Y.; Butler, L.T.; Shin, J.I.; Lopez-Sanchez, G.F.; Soysal, P.; Veronese, N.; Haro, J.M.; Koyanagi, A. Association between Food Insecurity and Sarcopenia among Adults Aged >/=65 Years in Low- and Middle-Income Countries. Nutrients 2021, 13, 1879. [Google Scholar] [CrossRef] [PubMed]
- Bank, G.W. World Bank in Kosovo. Available online: https://www.worldbank.org/en/country/kosovo/overview#3 (accessed on 5 July 2022).
- Brown, J.C.; Harhay, M.O.; Harhay, M.N. Sarcopenia and mortality among a population-based sample of community-dwelling older adults. J. Cachexia Sarcopenia Muscle 2016, 7, 290–298. [Google Scholar] [CrossRef]
- Statistics, K.A.O. Estimation of Kosovo Population in 2019. Available online: https://ask.rks-gov.net/en/kosovo-agency-of-statistics (accessed on 15 September 2022).
- Arya, R.; Antonisamy, B.; Kumar, S. Sample size estimation in prevalence studies. Indian J. Pediatr. 2012, 79, 1482–1488. [Google Scholar] [CrossRef]
- Eston, R.G.; Reilly, T. Kinanthropometry and Exercise Physiology Laboratory Manual: Tests, Procedures and Data, 3rd ed.; Routledge: London, UK, 2009; Volume 1, p. 352. [Google Scholar]
- Lee, S.Y.; Ahn, S.; Kim, Y.J.; Ji, M.J.; Kim, K.M.; Choi, S.H.; Jang, H.C.; Lim, S. Comparison between Dual-Energy X-ray Absorptiometry and Bioelectrical Impedance Analyses for Accuracy in Measuring Whole Body Muscle Mass and Appendicular Skeletal Muscle Mass. Nutrients 2018, 10, 738. [Google Scholar] [CrossRef]
- Chang, J.S.; Kim, T.H.; Kim, H.; Choi, E.H.; Kim, N.; Kong, I.D. Qualitative muscle mass index as a predictor of skeletal muscle function deficit in Asian older adults. Geriatr. Gerontol. Int. 2017, 17, 99–107. [Google Scholar] [CrossRef]
- Janssen, I.; Baumgartner, R.N.; Ross, R.; Rosenberg, I.H.; Roubenoff, R. Skeletal muscle cutpoints associated with elevated physical disability risk in older men and women. Am. J. Epidemiol. 2004, 159, 413–421. [Google Scholar] [CrossRef]
- Mijnarends, D.M.; Meijers, J.M.; Halfens, R.J.; ter Borg, S.; Luiking, Y.C.; Verlaan, S.; Schoberer, D.; Cruz Jentoft, A.J.; van Loon, L.J.; Schols, J.M. Validity and reliability of tools to measure muscle mass, strength, and physical performance in community-dwelling older people: A systematic review. J. Am. Med. Dir. Assoc. 2013, 14, 170–178. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.J.; Rikli, R.E. Measuring Functional Fitness in Older Adults. J. Act. Ageing 2002, 1, 25–30. [Google Scholar]
- Steffen, T.M.; Hacker, T.A.; Mollinger, L. Age- and gender-related test performance in community-dwelling elderly people: Six-Minute Walk Test, Berg Balance Scale, Timed Up & Go Test, and gait speeds. Phys. Ther. 2002, 82, 128–137. [Google Scholar] [CrossRef] [PubMed]
- Boshnjaku, A.; Bahtiri, A.; Feka, K.; Krasniqi, E.; Tschan, H.; Wessner, B. Test-retest reliability data of functional performance, strength, peak torque and body composition assessments in two different age groups of Kosovan adults. Data Brief. 2021, 36, 106988. [Google Scholar] [CrossRef] [PubMed]
- Vellas, B.; Guigoz, Y.; Garry, P.J.; Nourhashemi, F.; Bennahum, D.; Lauque, S.; Albarede, J.L. The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients. Nutrition 1999, 15, 116–122. [Google Scholar] [CrossRef]
- Svarstad, B.L.; Chewning, B.A.; Sleath, B.L.; Claesson, C. The Brief Medication Questionnaire: A tool for screening patient adherence and barriers to adherence. Patient Educ. Couns. 1999, 37, 113–124. [Google Scholar] [CrossRef]
- WHO-STEPS. STEPS Instrument (Core and Expanded). Available online: http://www.who.int/ncds/surveillance/steps/instrument/STEPS_Instrument_V3.2.pdf?ua=1 (accessed on 23 May 2022).
- Tessier, A.J.; Wing, S.S.; Rahme, E.; Morais, J.A.; Chevalier, S. Physical function-derived cut-points for the diagnosis of sarcopenia and dynapenia from the Canadian longitudinal study on aging. J. Cachexia Sarcopenia Muscle 2019, 10, 985–999. [Google Scholar] [CrossRef]
- Zhang, J.; Yu, K.F. What’s the relative risk? A method of correcting the odds ratio in cohort studies of common outcomes. JAMA 1998, 280, 1690–1691. [Google Scholar] [CrossRef]
- Sui, S.X.; Holloway-Kew, K.L.; Hyde, N.K.; Williams, L.J.; Tembo, M.C.; Leach, S.; Pasco, J.A. Prevalence of Sarcopenia Employing Population-Specific Cut-Points: Cross-Sectional Data from the Geelong Osteoporosis Study, Australia. J. Clin. Med. 2021, 10, 343. [Google Scholar] [CrossRef]
- Reiss, J.; Iglseder, B.; Alzner, R.; Mayr-Pirker, B.; Pirich, C.; Kassmann, H.; Kreutzer, M.; Dovjak, P.; Reiter, R. Consequences of applying the new EWGSOP2 guideline instead of the former EWGSOP guideline for sarcopenia case finding in older patients. Age Ageing 2019, 48, 719–724. [Google Scholar] [CrossRef]
- Shafiee, G.; Heshmat, R.; Ostovar, A.; Khatami, F.; Fahimfar, N.; Arzaghi, S.M.; Gharibzadeh, S.; Hanaei, S.; Nabipour, I.; Larijani, B. Comparison of EWGSOP-1and EWGSOP-2 diagnostic criteria on prevalence of and risk factors for sarcopenia among Iranian older people: The Bushehr Elderly Health (BEH) program. J. Diabetes Metab. Disord. 2020, 19, 727–734. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Yao, X.; Shen, J.; Sun, G.; Sun, Q.; Tian, X.; Li, X.; Li, X.; Ye, L.; Zhang, Z.; et al. Comparison of revised EWGSOP criteria and four other diagnostic criteria of sarcopenia in Chinese community-dwelling elderly residents. Exp. Gerontol. 2020, 130, 110798. [Google Scholar] [CrossRef] [PubMed]
- Van Ancum, J.M.; Alcazar, J.; Meskers, C.G.M.; Nielsen, B.R.; Suetta, C.; Maier, A.B. Impact of using the updated EWGSOP2 definition in diagnosing sarcopenia: A clinical perspective. Arch. Gerontol. Geriatr. 2020, 90, 104125. [Google Scholar] [CrossRef] [PubMed]
- Arnal-Gomez, A.; Cebria, I.I.M.A.; Tomas, J.M.; Tortosa-Chulia, M.A.; Balasch-Bernat, M.; Sentandreu-Mano, T.; Forcano, S.; Cezon-Serrano, N. Using the Updated EWGSOP2 Definition in Diagnosing Sarcopenia in Spanish Older Adults: Clinical Approach. J. Clin. Med. 2021, 10, 1018. [Google Scholar] [CrossRef] [PubMed]
- Stuck, A.K.; Mader, N.C.; Bertschi, D.; Limacher, A.; Kressig, R.W. Performance of the EWGSOP2 Cut-Points of Low Grip Strength for Identifying Sarcopenia and Frailty Phenotype: A Cross-Sectional Study in Older Inpatients. Int. J. Environ. Res. Public Health 2021, 18, 3498. [Google Scholar] [CrossRef]
- Fernandes, L.V.; Paiva, A.E.G.; Silva, A.C.B.; de Castro, I.C.; Santiago, A.F.; de Oliveira, E.P.; Porto, L.C.J. Prevalence of sarcopenia according to EWGSOP1 and EWGSOP2 in older adults and their associations with unfavorable health outcomes: A systematic review. Aging Clin. Exp. Res. 2022, 34, 505–514. [Google Scholar] [CrossRef]
- De Freitas, M.M.; de Oliveira, V.L.P.; Grassi, T.; Valduga, K.; Miller, M.E.P.; Schuchmann, R.A.; Souza, K.L.A.; de Azevedo, M.J.; Viana, L.V.; de Paula, T.P. Difference in sarcopenia prevalence and associated factors according to 2010 and 2018 European consensus (EWGSOP) in elderly patients with type 2 diabetes mellitus. Exp. Gerontol. 2020, 132, 110835. [Google Scholar] [CrossRef]
- Shafiee, G.; Keshtkar, A.; Soltani, A.; Ahadi, Z.; Larijani, B.; Heshmat, R. Prevalence of sarcopenia in the world: A systematic review and meta- analysis of general population studies. J. Diabetes Metab. Disord. 2017, 16, 21. [Google Scholar] [CrossRef]
- Sousa-Santos, A.R.; Afonso, C.; Borges, N.; Santos, A.; Padrao, P.; Moreira, P.; Amaral, T.F. Sarcopenia, physical frailty, undernutrition and obesity cooccurrence among Portuguese community-dwelling older adults: Results from Nutrition UP 65 cross-sectional study. BMJ Open 2020, 10, e033661. [Google Scholar] [CrossRef]
- Bosello, O.; Vanzo, A. Obesity paradox and aging. Eat. Weight Disord. 2021, 26, 27–35. [Google Scholar] [CrossRef]
- Peralta, M.; Ramos, M.; Lipert, A.; Martins, J.; Marques, A. Prevalence and trends of overweight and obesity in older adults from 10 European countries from 2005 to 2013. Scand J. Public Health 2018, 46, 522–529. [Google Scholar] [CrossRef] [PubMed]
- Doulougou, B.; Gomez, F.; Alvarado, B.; Guerra, R.O.; Ylli, A.; Guralnik, J.; Zunzunegui, M.V. Factors associated with hypertension prevalence, awareness, treatment and control among participants in the International Mobility in Aging Study (IMIAS). J. Hum. Hypertens. 2016, 30, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Cooper, R.; Hardy, R.; Aihie Sayer, A.; Ben-Shlomo, Y.; Birnie, K.; Cooper, C.; Craig, L.; Deary, I.J.; Demakakos, P.; Gallacher, J.; et al. Age and gender differences in physical capability levels from mid-life onwards: The harmonisation and meta-analysis of data from eight UK cohort studies. PLoS ONE 2011, 6, e27899. [Google Scholar] [CrossRef] [PubMed]
- Maffiuletti, N.A.; Jubeau, M.; Munzinger, U.; Bizzini, M.; Agosti, F.; De Col, A.; Lafortuna, C.L.; Sartorio, A. Differences in quadriceps muscle strength and fatigue between lean and obese subjects. Eur. J. Appl. Physiol. 2007, 101, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Krasniqi, E.; Boshnjaku, A.; Wagner, K.H.; Wessner, B. Association between Polymorphisms in Vitamin D Pathway-Related Genes, Vitamin D Status, Muscle Mass and Function: A Systematic Review. Nutrients 2021, 13, 3109. [Google Scholar] [CrossRef]
- Boshnjaku, A.; Krasniqi, E.; Tschan, H.; Wessner, B. ACTN3 Genotypes and Their Relationship with Muscle Mass and Function of Kosovan Adults. Int. J. Environ. Res. Public Health 2021, 18, 9135. [Google Scholar] [CrossRef]
- Masanes, F.; Rojano, I.L.X.; Salva, A.; Serra-Rexach, J.A.; Artaza, I.; Formiga, F.; Cuesta, F.; Lopez Soto, A.; Ruiz, D.; Cruz-Jentoft, A.J. Cut-off Points for Muscle Mass—Not Grip Strength or Gait Speed—Determine Variations in Sarcopenia Prevalence. J. Nutr. Health Aging 2017, 21, 825–829. [Google Scholar] [CrossRef]
- Kim, Y.H.; Kim, K.I.; Paik, N.J.; Kim, K.W.; Jang, H.C.; Lim, J.Y. Muscle strength: A better index of low physical performance than muscle mass in older adults. Geriatr. Gerontol. Int. 2016, 16, 577–585. [Google Scholar] [CrossRef]
- Leong, D.P.; Teo, K.K.; Rangarajan, S.; Lopez-Jaramillo, P.; Avezum, A., Jr.; Orlandini, A.; Seron, P.; Ahmed, S.H.; Rosengren, A.; Kelishadi, R.; et al. Prognostic value of grip strength: Findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet 2015, 386, 266–273. [Google Scholar] [CrossRef]
- Buckinx, F.; Landi, F.; Cesari, M.; Fielding, R.A.; Visser, M.; Engelke, K.; Maggi, S.; Dennison, E.; Al-Daghri, N.M.; Allepaerts, S.; et al. Pitfalls in the measurement of muscle mass: A need for a reference standard. J. Cachexia Sarcopenia Muscle 2018, 9, 269–278. [Google Scholar] [CrossRef]
- Kitamura, A.; Seino, S.; Abe, T.; Nofuji, Y.; Yokoyama, Y.; Amano, H.; Nishi, M.; Taniguchi, Y.; Narita, M.; Fujiwara, Y.; et al. Sarcopenia: Prevalence, associated factors, and the risk of mortality and disability in Japanese older adults. J. Cachexia Sarcopenia Muscle 2021, 12, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Hamilton-James, K.; Collet, T.H.; Pichard, C.; Genton, L.; Dupertuis, Y.M. Precision and accuracy of bioelectrical impedance analysis devices in supine versus standing position with or without retractable handle in Caucasian subjects. Clin. Nutr. ESPEN 2021, 45, 267–274. [Google Scholar] [CrossRef]
- Bosy-Westphal, A.; Jensen, B.; Braun, W.; Pourhassan, M.; Gallagher, D.; Muller, M.J. Quantification of whole-body and segmental skeletal muscle mass using phase-sensitive 8-electrode medical bioelectrical impedance devices. Eur. J. Clin. Nutr. 2017, 71, 1061–1067. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Shinkai, S.; Murayama, H.; Mori, S. Comparison of segmental multifrequency bioelectrical impedance analysis with dual-energy X-ray absorptiometry for the assessment of body composition in a community-dwelling older population. Geriatr. Gerontol. Int. 2015, 15, 1013–1022. [Google Scholar] [CrossRef]
- Kim, M.; Kim, H. Accuracy of segmental multi-frequency bioelectrical impedance analysis for assessing whole-body and appendicular fat mass and lean soft tissue mass in frail women aged 75 years and older. Eur. J. Clin. Nutr. 2013, 67, 395–400. [Google Scholar] [CrossRef]
- McLester, C.N.; Nickerson, B.S.; Kliszczewicz, B.M.; McLester, J.R. Reliability and Agreement of Various InBody Body Composition Analyzers as Compared to Dual-Energy X-Ray Absorptiometry in Healthy Men and Women. J. Clin. Densitom. 2020, 23, 443–450. [Google Scholar] [CrossRef]
- Janssen, I.; Heymsfield, S.B.; Baumgartner, R.N.; Ross, R. Estimation of skeletal muscle mass by bioelectrical impedance analysis. J. Appl. Physiol. (1985) 2000, 89, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Beaudart, C.; McCloskey, E.; Bruyere, O.; Cesari, M.; Rolland, Y.; Rizzoli, R.; Araujo de Carvalho, I.; Amuthavalli Thiyagarajan, J.; Bautmans, I.; Bertiere, M.C.; et al. Sarcopenia in daily practice: Assessment and management. BMC Geriatr. 2016, 16, 170. [Google Scholar] [CrossRef]
- Hajian-Tilaki, K. Sample size estimation in diagnostic test studies of biomedical informatics. J. Biomed. Inform. 2014, 48, 193–204. [Google Scholar] [CrossRef]
- Obesity: Preventing and Managing the Global Epidemic. Report of a WHO Consultation. Available online: https://apps.who.int/iris/handle/10665/42330 (accessed on 1 September 2022).
- Shkaqet e Vdekjeve në Kosovë. Available online: https://ask.rks-gov.net/media/5246/shkaqet-e-vdekjeve-n%C3%AB-kosov%C3%AB-2016-2017.pdf (accessed on 15 September 2022).



{kind=link}
{kind=link}
| Total (n = 240) | Female (n = 113) | Male (n = 127) | p Value | |
|---|---|---|---|---|
| Sex (%) | 100 | 47.1 | 52.9 | |
| Age (years) | 70.3 ± 5.8 | 68.4 ± 5.3 | 72.1 ± 5.7 | <0.001 |
| Height (m) | 1.64 ± 0.09 | 1.57 ± 0.06 | 1.70 ± 0.07 | <0.001 |
| Body mass (kg) | 79.9 ± 12.7 | 79.3 ± 11.7 | 80.4 ± 13.6 | 0.504 |
| BMI (kg/m2) | 29.7 ± 4.7 | 32.0 ± 4.3 | 27.7 ± 4.2 | <0.001 |
| Whole body fat mass (kg) | 29.6 ± 11.1 | 35.3 ± 8.9 | 24.4 ± 10.3 | <0.001 |
| Whole body fat percentage (%) | 36.4 ± 10.6 | 44.1 ± 6.5 | 29.6 ± 8.6 | <0.001 |
| Skeletal muscle mass (kg) | 26.9 ± 5.4 | 23.3 ± 3.2 | 30.2 ± 5.0 | <0.001 |
| SMI (kg/m2) | 9.9 ± 1.2 | 9.4 ± 0.9 | 10.3 ± 1.3 | <0.001 |
| Appendicular skeletal muscle mass (kg) | 19.4 ± 2.9 | 18.2 ± 2.2 | 20.5 ± 3.1 | <0.001 |
| ASMI (kg/m2) | 7.2 ± 0.8 | 7.3 ± 0.7 | 7.0 ± 0.8 | 0.003 |
| Hand grip strength (kg) | 30.1 ± 8.8 | 24.1 ± 5.1 | 35.4 ± 8.0 | <0.001 |
| Gait speed (m/s) | 1.08 ± 0.21 | 1.01 ± 0.19 | 1.14 ± 0.22 | <0.001 |
| Timed up and go test (s) | 7.12 ± 1.98 | 7.50 ± 2.20 | 6.78 ± 1.70 | 0.005 |
| 30-s arm curl test (repetitions) | 14 ± 3 | 14 ± 3 | 15 ± 3 | 0.100 |
| 30-s chair stand test (repetitions) | 11 ± 3 | 11 ± 3 | 12 ± 3 | 0.004 |
| 6-min walking test (m) | 420 ± 139 | 381 ± 127 | 455 ± 140 | <0.001 |
| Physical performance Score (-) | −1.26 ± 1.86 | −1.78 ± 1.81 | 0.8 ± 1.79 | <0.001 |
| Mini nutritional status (-) | 25 ± 3 | 24 ± 3 | 25 ± 2 | <0.001 |
| Malnourished (yes/risk/no, n (%)) | 4/64/172 (1.7/26.6/71.7) | 4/41/68 (3.5/36.3/60.2) | 0/23/104 (0.0/18.1/81.9) | <0.001 |
| BMI categories (underweight/normal weight/overweight/obese, n (%)) | 2/34/104/100 (0.8/14.2/43.3/41.7) | 0/7/35/71 (0.0/6.2/31.0/62.8) | 2/27/69/29 (1.6/21.3/54.3/22.8) | <0.001 |
| Smoking status (smoker/quit smoking/non-smoker, n (%)) | 53/24/163 (22.1/10/67.9) | 20/4/89 (17.7/3.5/78.8) | 33/20/74 (26/15.7/58.3) | 0.001 |
| Self-perceived health condition (good/not good, n (%)) | 103/137 (42.9/57.1) | 50/63 (44.2/55.8) | 53/74 (41.7/58.3) | 0.694 |
| Self-declared chronic disease (yes/no, n (%)) | 183/57 (76.2/23.8) | 90/23 (79.6/20.4) | 93/34 (73.2/26.8) | 0.244 |
| Intake of medication (yes/no, n (%)) | 186/54 (77.5/22.5) | 95/18 (84.1/15.9) | 91/36 (71.6/28.4) | 0.021 |
| Number of medications (n (%)) | 2.3 ± 1.9 | 2.8 ± 1.9 | 1.9 ± 1.7 | <0.001 |
| Education (no formal/1–8 years/>8 years, n (%)) | 10/95/135 (4.2/39.6/56.2) | 7/62/44 (6.2/54.9/38.9) | 3/33/91 (2.4/26/71.6) | <0.001 |
| Marital status (single/partnership or married/widowed, n (%)) | 7/166/67 (2.9/69.2/27.9) | 7/66/40 (6.2/58.4/35.4) | 0/100/27 (0/78.7/21.3) | 0.003 |
| Financial condition (enough to cover the month/not enough, n (%)) | 166/74 (69.2/30.8) | 70/43 (61.9/38.1) | 96/31 (75.6/24.4) | 0.022 |
| No Sarcopenia (n = 110) | Probable Sarcopenia (n = 7) | Sarcopenia (n = 7) | Severe Sarcopenia (n = 3) | p Value | |
|---|---|---|---|---|---|
| Age(years) | 71.4 ± 5.2 a | 74.5 ± 8.1 a,b | 79.2 ± 6.7 b | 73.9 ± 0.8 a,b | 0.002 |
| Height (m) | 1.71 ± 0.06 a | 1.65 ± 0.07 b | 1.61 ± 0.10 b | 1.66 ± 0.08 a,b | <0.001 |
| Body mass (kg) | 81.2 ± 14.2 | 78.3 ± 5.3 | 74.5 ± 7.6 | 69.5 ± 3.3 | 0.280 |
| BMI (kg/m2) | 27.6 ± 4.3 | 28.9 ± 1.7 | 28.8 ± 4.5 | 25.4 ± 2.7 | 0.579 |
| Whole body fat mass (kg) | 24.7 ± 10.7 | 22.5 ± 4.7 | 23.5 ± 11.2 | 22.7 ± 4.0 | 0.933 |
| Whole body fat percentage (%) | 29.4 ± 8.4 | 29.0 ± 6.7 | 31.7 ± 14.6 | 32.6 ± 4.1 | 0.830 |
| Skeletal muscle mass (kg) | 30.9 ± 4.5 a | 26.9 ± 6.0 a,b | 24.5 ± 7.0 b | 25.3 ± 0.7 a,b | <0.001 |
| SMI (kg/m2) | 10.5 ± 1.2 a | 9.9 ± 1.7 a | 9.3 ± 2.1 a | 9.2 ± 0.9 a | 0.037 |
| Appendicular skeletal muscle mass (kg) | 23.7 ± 3.5 a | 23.2 ± 3.1 a | 18.3 ± 3.4 b | 19.6 ± 0.7 a,b | <0.001 |
| ASMI (kg/m2) | 8.0 ± 0.9 a | 8.6 ± 0.9 a | 7.0 ± 0.6 b | 7.2 ± 0.5 a,b | 0.001 |
| PP score (-) | 1.06 ± 2.56 a | −0.31 ± 2.08 a | −0.86 ± 1.87 a | −5.65 ± 0.66 b | <0.001 |
| Handgrip strength (kg) | 37.7 ± 5.8 a | 22.6 ± 2.7 b | 19.8 ± 4.3 b | 19.8 ± 7.8 b | <0.001 |
| Relative handgrip strength (kg/kg) | 0.47 ± 0.08 a | 0.29 ± 0.03 b | 0.27 ± 0.06 b | 0.28 ± 0.10 b | <0.001 |
| Gait speed (m/s) | 1.16 ± 0.22 a | 1.08 ± 0.14 a | 1.04 ± 0.14 a,b | 0.68 ± 0.14 b | 0.001 |
| Timed up and go test (s) | 6.64 ± 1.52 a | 6.63 ± 0.91 a | 7.13 ± 2.37 a | 11.30 ± 2.01 b | <0.001 |
| 30-s arm curl test (repetitions) | 15 ± 3 a | 13 ± 3 a,b | 13 ± 3 a,b | 10 ± 2 b | 0.007 |
| 30-s chair stand test (repetitions) | 12 ± 3 a | 12 ± 3 a | 10 ± 2 a,b | 8 ± 2 b | 0.032 |
| 6-min walking test (m) | 470 ± 139 a | 369 ± 82 a,b | 384 ± 121 a,b | 261 ± 92 b | 0.008 |
| Mini nutritional status (-) | 25 ± 2 | 25 ± 3 | 26 ± 2 | 22 ± 3 | 0.059 |
| Malnourished (yes/risk/no, n (%)) | 19/91 (17.3/82.7) | 1/6 (14.3/85.7) | 0/1/6 (0/14.3/85.7) | 0/2/1 (0/66.7/33.3) | 0.175 |
| BMI categories (underweight/normal weight/overweight/obese, n (%)) | 2/24/60/24 (1.8/21.8/54.5/21.8) | 0/0/5/2 (0.0/0.0/71.4/28.6) | 0/2/2/3 (0/28.6/28.6/42.9) | 0/1/2/0 (0/33.3/66.7/0) | 0.781 |
| Smoking status (smoker/quit smoking/non-smoker, n (%)) | 31/19/60 (28.2/17.4/54.5) | 0/0/7 (0.0/0.0/100.0) | 2/0/5 (28.6/0/71.4) | 0/1/2 (0/33.3/66.7) | 0.212 |
| Self-perceived health condition (good/not good, n (%)) | 48/62 (43.6/56.4) | 3/4 (42.9/57.1) | 2/5 (28.6/71.4) | 0/3 (0/100) | 0.421 |
| Self-declared chronic disease (yes/no, n (%)) | 80/30 (72.7/27.3) | 4/3 (57.1/42.9) | 6/1 (85.7/14.3) | 3/0 (100/0) | 0.459 |
| Intake of medication (yes/no, n (%)) | 19/91 (17.3/82.7) | 3/4 (42.9/57.1) | 1/6 (14.3/85.7) | 2/1 (66.7/33.3) | 0.069 |
| Number of medications (-) | 1.9 ± 1.7 | 1.9 ± 1.8 | 1.9 ± 1.8 | 3.0 ± 1.7 | 0.741 |
| Education (no formal/1–8 years/>8 years, n (%)) | 2/25/83 (1.8/22.7/75.5) | 0/2/5 (0.0/28.6/71.4) | 1/4/2 (14.3/57.1/28.6) | 0/2/1 (0/66.7/33.3) | 0.057 |
| Marital status (single/partnership or married/widowed, n (%)) | 0/88/22 (0/80.0/20.0) | 0/6/1 (0/85.7/14.3) | 0/5/2 (0/71.4/28.6) | 0/1/2 (0/33.3/66.7) | 0.002 |
| Financial condition (enough to cover the month/not enough, n (%)) | 85/25 (77.3/22.7) | 4/3 (57.1/42.9) | 6/1 (85.7/14.3) | 1/2 (33.3/66.7) | 0.191 |
| No Sarcopenia (n = 85) | Probable Sarcopenia (n = 36) | Severe Sarcopenia (n = 6) | p Value | |
|---|---|---|---|---|
| Age (years) | 70.7 ± 4.5 a | 75.0 ± 6.4 a | 74.2 ± 10.0 a | <0.001 |
| Height (m) | 1.72 ± 5.51 a | 1.66 ± 7.51 a,b | 1.70 ± 4.15 b | <0.001 |
| Body mass (kg) | 83.0 ± 14.0 a | 78.0 ± 9.3 a | 58.7 ± 8.0 b | <0.001 |
| BMI (kg/m2) | 27.9 ± 4.1 a | 28.5 ± 3.6 a | 20.3 ± 2.1 b | <0.001 |
| Whole body fat mass (kg) | 25.2 ± 10.6 a | 24.5 ± 9.1 a | 13.2 ± 7.5 b | 0.022 |
| Whole body fat percentage (%) | 29.5 ± 7.8 a | 31.1 ± 9.6 a | 21.5 ± 10.7 b | 0.040 |
| Skeletal muscle mass (kg) | 31.7 ± 3.9 a | 27.7 ± 5.2 b | 22.3 ± 4.6 c | <0.001 |
| SMI (kg/m2) | 10.7 ± 1.0 a | 10.0 ± 1.4 a | 7.7 ± 1.4 b | <0.001 |
| Appendicular skeletal muscle mass (kg) | 21.2 ± 2.9 a | 19.5 ± 2.6 a | 15.6 ± 1.3 b | <0.001 |
| ASMI (kg/m2) | 8.2 ± 0.8 a | 7.9 ± 0.9 a | 6.3 ± 0.5 b | <0.001 |
| PP score (-) | 1.72 ± 2.29 a | −1.15 ± 2.27 b | −2.19 ± 2.78 b | <0.001 |
| Handgrip strength (kg) | 39.9 ± 4.5 a | 26.7 ± 4.7 b | 24.0 ± 8.7 b | <0.001 |
| Relative handgrip strength (kg/kg) | 0.49 ± 0.07 a | 0.35 ± 0.07 a | 0.43 ± 0.20 b | <0.001 |
| Gait speed(m/s) | 1.21 ± 0.20 a | 1.00 ± 0.19 b | 0.95 ± 0.13 b | <0.001 |
| Timed up and go test (s) | 6.37 ± 1.39 a | 7.40 ± 1.90 a,b | 8.77 ± 2.10 b | <0.001 |
| 30-s arm curl test (repetitions) | 16 ± 3 a | 12 ± 3 b | 12 ± 3 b | <0.001 |
| 30-s chair stand test (repetitions) | 12 ± 3 a | 10 ± 2 a,b | 10 ± 3 b | <0.001 |
| 6-min walking test (m) | 489 ± 138 a | 390 ± 113 a,b | 355 ± 149 b | <0.001 |
| Mini nutritional status (-) | 26 ± 2 a | 25 ± 2 a | 22 ± 3 b | <0.001 |
| Malnourished (yes/risk/no, n (%)) | 12/73 (14.1/85.9) | 7/29 (19.4/80.6) | 4/2 (66.7/33.3) | 0.005 |
| BMI categories (underweight/normal/overweight/obese, n (%)) | 0/17/50/18 (0.0/20.0/58.8/21.2) | 0/6/19/11 (0.0/16.7/52.8/30.6) | 2/4/0/0 (33.3/66.7/0.0/0.0) | <0.001 |
| Smoking status (smoker/quit smoking/non-smoker, n (%)) | 24/14/47 (28.2/16.5/55.3) | 5/5/26 (13.9/13.9/72.2) | 4/1/1 (66.7/16.7/16.7) | 0.055 |
| Self-perceived health condition [good/not good, n (%)] | 38/47 (44.7/55.3) | 11/25 (30.6/69.4) | 4/2 (66.7/33.3) | 0.158 |
| Self-declared chronic disease (yes/no, n (%)) | 62/23 (72.9/27.1) | 27/9 (75/25) | 4/2 (66.7/33.3) | 0.908 |
| Intake of medication (yes/no, n (%)) | 63/22 (74.1/25.9) | 24/12 (66.7/33.3) | 4/2 (66.7/33.3) | 0.681 |
| Number of medications (-) | 1.9 ± 1.7 | 2.0 ± 1.7 | 1.0 ± 1.7 | 0.406 |
| Education (no formal/1–8 years/>8 years, n (%)) | 0/20/65 (0.0/23.5/76.5) | 2/11/23 (5.6/30.6/63.9) | 1/2/3 (16.7/33.3/50.0) | 0.035 |
| Marital status (single/partnership or married/widowed, n (%)) | 0/70/15 (0/82.4/17.6) | 0/25/11 (0/69.4/30.6) | 0/5/1 (0/83.3/16.7) | 0.273 |
| Financial condition (enough to cover the month/not enough, n (%)) | 65/20 (76.5/23.5) | 28/8 (77.8/22.2) | 3/3 (50.0/50.0) | 0.323 |
| Unadjusted Model | Adjusted Model | |||||
|---|---|---|---|---|---|---|
| Probable Sarcopenia | Severe Sarcopenia | Probable Sarcopenia | Severe Sarcopenia | Probable Sarcopenia | Severe Sarcopenia | |
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | RR (95% CI) | RR (95% CI) | |
| Age (years) | 1.099 (0.971–1.244) | 1.172 (1.058–1.299) ** | 1.034 (0.890–1.200) | 1.227 (1.054–1.427) ** | 1.004 (0.984–1.023) | 1.025 (1.007–1.042) ** |
| BMI (kg/m2) | 1.067 (0.908–1.254) | 1.012 (0.868–1.179) | 1.928 (1.182–3.147) ** | 1.351 (0.896–2.039) | 1.069 (1.021–1.100) ** | 1.036 (0.985–1.073) |
| Body fat mass (kg) | 0.978 (0.900–1.062) | 0.986 (0.922–1.054) | 0.784 (0.658–0.935) ** | 0.864 (0.725–1.029) | 0.965 (0.935–0.991) ** | 0.979 (0.952–1.004) |
| SMM (kg) | 0.836 (0.711–0.984) * | 0.775 (0.667–0.900) *** | 0.770 (0.615–0.965) * | 0.693 (0.546–0.880) ** | 0.962 (0.923–0.995) * | 0.944 (0.900–0.982) ** |
| PP score (-) | 0.814 (0.606–1.094) | 0.611 (0.461–0.811) *** | 0.959 (0.621–1.481) | 0.659 (0.443–0.980) * | 0.994 (0.924–1.045) | 0.935 (0.856–0.997) * |
| MNA score (-) | 0.978 (0.716–1.336) | 0.893 (0.695–1.147) | 0.986 (0.613–1.586) | 1.210 (0.717–2.045) | 0.998 (0.922–1.052) | 1.024 (0.950–1.073) |
| Financial condition a | ||||||
| Not enough to cover the month | 0.392 (0.082–1.870) | 0.686 (0.165–2.851) | 0.106 (0.010–1.125) | 0.156 (0.012–1.949) | 0.469 (0.070–1.015) | 0.580 (0.086–1.070) |
| Health condition b | ||||||
| Not good | 0.969 (0.207–4.535) | 0.323 (0.066–1.591) | 0.692 (0.087–5.486) | 0.063 (0.004–0.941) * | 0.944 (0.417–1.123) | 0.335 (0.031–0.992) * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boshnjaku, A.; Bahtiri, A.; Feka, K.; Krasniqi, E.; Tschan, H.; Wessner, B. Impact of Using Population-Specific Cut-Points, Self-Reported Health, and Socio-Economic Parameters to Predict Sarcopenia: A Cross-Sectional Study in Community-Dwelling Kosovans Aged 60 Years and Older. J. Clin. Med. 2022, 11, 5579. https://doi.org/10.3390/jcm11195579
Boshnjaku A, Bahtiri A, Feka K, Krasniqi E, Tschan H, Wessner B. Impact of Using Population-Specific Cut-Points, Self-Reported Health, and Socio-Economic Parameters to Predict Sarcopenia: A Cross-Sectional Study in Community-Dwelling Kosovans Aged 60 Years and Older. Journal of Clinical Medicine. 2022; 11(19):5579. https://doi.org/10.3390/jcm11195579
Chicago/Turabian StyleBoshnjaku, Arben, Abedin Bahtiri, Kaltrina Feka, Ermira Krasniqi, Harald Tschan, and Barbara Wessner. 2022. "Impact of Using Population-Specific Cut-Points, Self-Reported Health, and Socio-Economic Parameters to Predict Sarcopenia: A Cross-Sectional Study in Community-Dwelling Kosovans Aged 60 Years and Older" Journal of Clinical Medicine 11, no. 19: 5579. https://doi.org/10.3390/jcm11195579
APA StyleBoshnjaku, A., Bahtiri, A., Feka, K., Krasniqi, E., Tschan, H., & Wessner, B. (2022). Impact of Using Population-Specific Cut-Points, Self-Reported Health, and Socio-Economic Parameters to Predict Sarcopenia: A Cross-Sectional Study in Community-Dwelling Kosovans Aged 60 Years and Older. Journal of Clinical Medicine, 11(19), 5579. https://doi.org/10.3390/jcm11195579