
A Paradigm Shift in the Diagnosis of Aspiration Pneumonia in Older Adults


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients
2.3. Definitions
2.4. Data Collection
2.5. Antimicrobial Treatment
- CAP: amoxicillin, or amoxicillin and clarithromycin, depending on CURB-65 score (if allergic to penicillin: vancomycin and clarithromycin).
- AP: amoxicillin, metronidazole, and gentamicin (if allergic to penicillin: teicoplanin, metronidazole, and gentamicin).
- HAP (including CAP presenting within 1 month of discharge from hospital): amoxicillin and gentamycin, or amoxicillin and clavulanic acid, or amoxicillin, clavulanic acid, and amikacin (if allergic to penicillin: teicoplanin and gentamicin).
- Infectious exacerbation of COPD: doxycycline.
2.6. Statistical Analyses
3. Results
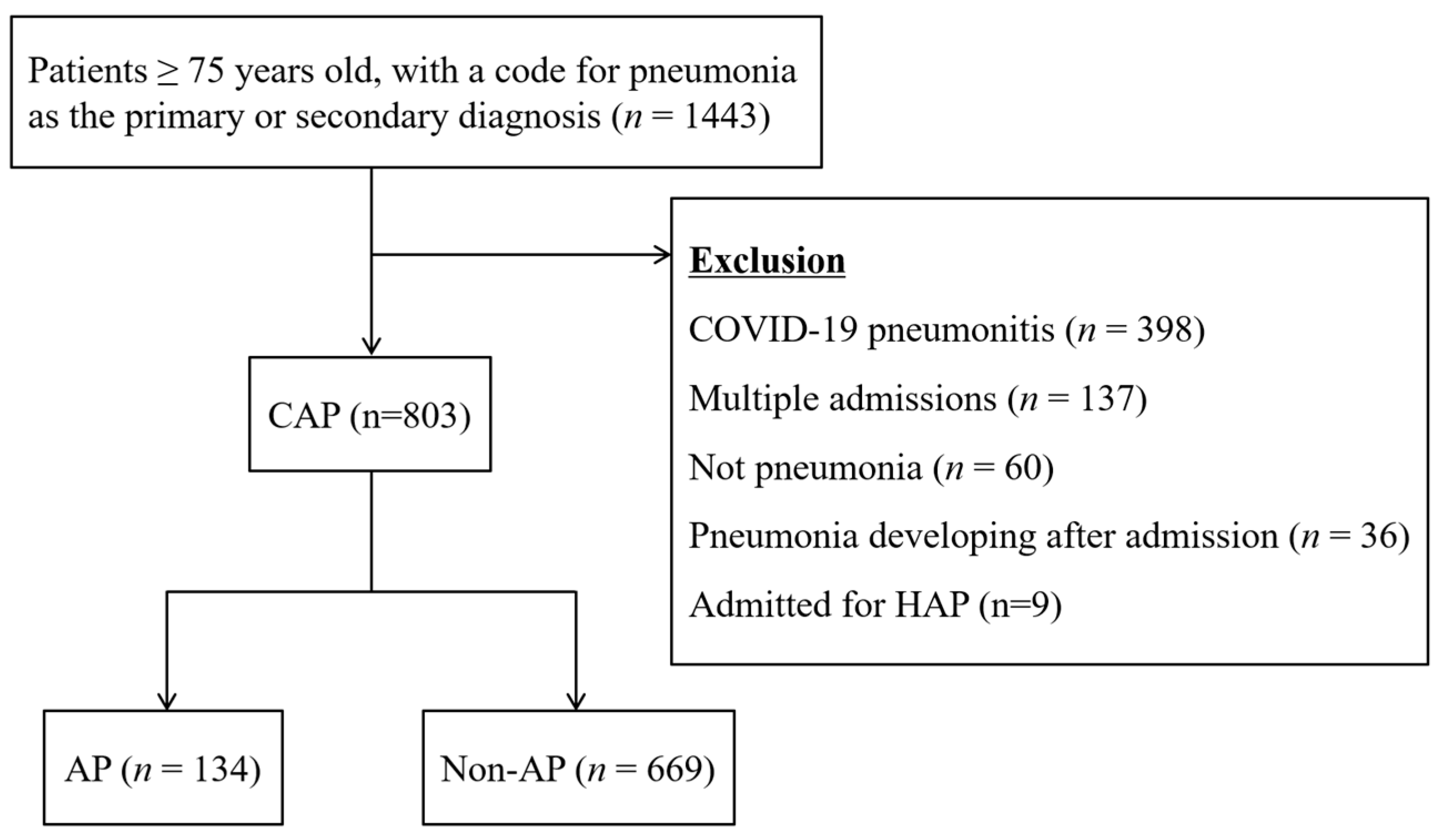
3.1. Patient Selection
3.2. Patient Background
3.3. Past Medical History
3.4. Symptoms and Signs
3.5. Diagnostic Investigations
3.6. Alternative Diagnoses of CT
3.7. Diagnosis of New Causative Conditions of Dysphagia and Aspiration
3.8. Management
4. Discussion
4.1. Diagnosis of Aspiration Pneumonia
4.2. Microbial Investigations
4.3. Further Investigations and Additional Diagnoses
4.4. Diagnosis of New Causes of Aspiration
4.5. Management of the Patient
4.6. Suggestions of a Paradigm Shift in the Diagnosis of Pneumonia
4.7. Strengths and Weaknesses of This Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Factor | AP (n = 130) | Non-AP (n = 622) | p-Value | ||
|---|---|---|---|---|---|
| Background | n | %, IQR | n | %, IQR | |
| Male (n, %) | 70 | (53.8) | 326 | (52.4) | 0.76 |
| Age (median, IQR) | 85 | (80–90) | 84 | (80–89) | 0.11 |
| Care home/nursing home (n, %) | 40 | (30.8) | 72 | (11.6) | <0.001 |
| Clinical frailty scale (median, IQR) | 6 | (5–7) | 5 | (4–6) | <0.001 |
| SARC-F score (median, IQR) | 7 | (4–10) | 4 | (2–7) | <0.001 |
| Past medical history, comorbidities | |||||
| Stroke (n, %) | 28 | (21.5) | 99 | (15.9) | 0.12 |
| Neurologic disorder (n, %) | 22 | (16.9) | 28 | (4.5) | <0.001 |
| Dementia (n, %) | 68 | (52.3) | 147 | (23.6) | <0.001 |
| Other mental disorder (n, %) | 15 | (11.5) | 63 | (10.1) | 0.63 |
| Gastroesophageal reflux disease (n, %) | 8 | (6.2) | 28 | (4.5) | 0.42 |
| Other gastroesophageal disorder (n, %) | 17 | (13.1) | 52 | (8.4) | 0.09 |
| Ischemic/congestive cardiac condition (n, %) | 29 | (22.3) | 198 | (31.8) | <0.05 |
| Type 2 diabetes mellitus (n, %) | 21 | (16.2) | 152 | (24.4) | <0.05 |
| Chronic respiratory disorder (n, %) | 21 | (16.2) | 184 | (29.6) | <0.05 |
| Active cancer (n, %) | 17 | (13.1) | 85 | (13.7) | 0.86 |
| Head and neck cancer (n, %) | 2 | (1.5) | 6 | (1.0) | 0.63 |
| Immunodeficiency (n, %) | 5 | (3.8) | 66 | (10.6) | <0.05 |
| Pneumonia within 1 year (n, %) | 36 | (27.7) | 126 | (20.3) | 0.06 |
| Number of daily drugs (median, IQR) | 6 | (5–9) | 7 | (4–9) | 0.07 |
| Known dysphagia (n, %) | 60 | (46.2) | 40 | (6.4) | <0.001 |
| Risk factors of multi-drug resistant pathogens | |||||
| Hospital admission ≥2 days in the past 90 days (n, %) | 33 | (25.4) | 173 | (27.8) | <0.001 |
| Haemodialysis (n, %) | 2 | (1.5) | 5 | (0.8) | 0.35 |
| Intravenous antibiotic therapy in the last 90 days (n, %) | 25 | (19.2) | 113 | (18.2) | 0.78 |
| Factor | AP (n = 130) | Non-AP (n = 622) | p-Value | ||
|---|---|---|---|---|---|
| Symptoms | n | %, IQR | n | %, IQR | |
| Cough (n, %) | 51 | (39.2) | 293 | (47.1) | 0.08 |
| Purulent sputum (n, %) | 30 | (23.1) | 151 | (24.3) | 0.55 |
| Pleuritic pain (n, %) | 1 | (0.8) | 28 | (4.5) | <0.05 |
| Dyspnoea (n, %) | 40 | (30.8) | 350 | (56.3) | <0.001 |
| Fever (n, %) | 26 | (20.0) | 181 | (29.1) | <0.05 |
| Coughing on oral intake (n, %) | 31 | (23.8) | 12 | (1.9) | <0.001 |
| Vomiting (n, %) | 57 | (43.8) | 42 | (6.8) | <0.001 |
| Altered mental status from baseline (n, %) | 43 | (33.1) | 144 | (23.2) | <0.05 |
| Severity of the pneumonia | |||||
| CURB-65, median (n, IQR) | 2 | (2–3) | 2 | (1–2) | <0.001 |
| Pneumonia severity index (median, IQR) | 107 | (95–128) | 103 | (85–119) | <0.05 |
References
- Marin, S.; Serra-Prat, M.; Ortega, O.; Clavé, P. Healthcare-related cost of oropharyngeal dysphagia and its complications pneumonia and malnutrition after stroke: A systematic review. BMJ Open 2020, 10, e031629. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Douiri, A.; Gulliford, M. Pneumonia incidence trends in UK primary care from 2002 to 2017: Population-based cohort study. Epidemiol. Infect. 2019, 147, e263. [Google Scholar] [CrossRef] [PubMed]
- Marik, P.E. Aspiration Pneumonitis and Aspiration Pneumonia. N. Engl. J. Med. 2001, 344, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Feldman, C.; Anderson, R. Epidemiology, virulence and management of pneumococcus. F1000Research 2016, 5, 2320. [Google Scholar] [CrossRef] [PubMed]
- Manabe, T.; Teramoto, S.; Tamiya, N.; Okochi, J.; Hizawa, N. Risk Factors for Aspiration Pneumonia in Older Adults. PLoS ONE 2015, 10, e0140060. [Google Scholar] [CrossRef]
- Pneumonia Statistics. Available online: https:statistics:blf.org.uk/pneumonia (accessed on 21 July 2022).
- Teramoto, S.; Fukuchi, Y.; Sasaki, H.; Sato, K.; Sekizawa, K.; Matsuse, T.; Japanese Study Group on Aspiration Pulmonary Disease. High incidence of aspiration pneumonia in community- and hospital-acquired pneumonia in hospitalized patients: A multicenter, prospective study in Japan. J. Am. Geriatr. Soc. 2008, 56, 577–579. [Google Scholar] [CrossRef]
- Ortega, O.; Martín, A.; Clavé, P. Diagnosis and Management of Oropharyngeal Dysphagia Among Older Persons, State of the Art. J. Am. Med. Dir. Assoc. 2017, 18, 576–582. [Google Scholar] [CrossRef]
- Langmore, S.; Terpenning, M.S.; Schork, A.; Chen, Y.; Murray, J.T.; Lopatin, D.E.; Loesche, W.J. Predictors of Aspiration Pneumonia: How Important Is Dysphagia? Dysphagia 1998, 13, 69–81. [Google Scholar] [CrossRef]
- Yamaya, M.; Yanai, M.; Ohrui, T.; Arai, H.; Sasaki, H. Interventions to Prevent Pneumonia Among Older Adults. J. Am. Geriatr. Soc. 2001, 49, 85–90. [Google Scholar] [CrossRef]
- Okazaki, T.; Suzukamo, Y.; Miyatake, M.; Komatsu, R.; Yaekashiwa, M.; Nihei, M.; Izumi, S.; Ebihara, T. Respiratory Muscle Weakness as a Risk Factor for Pneumonia in Older People. Gerontology 2021, 67, 581–590. [Google Scholar] [CrossRef]
- Okazaki, T.; Ebihara, S.; Mori, T.; Izumi, S.; Ebihara, T. Association between sarcopenia and pneumonia in older people. Geriatr. Gerontol. Int. 2019, 20, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, M.; Iwasaki, T.; Yamazaki, Y.; Takayasu, H.; Tateno, H.; Tazawa, S.; Kato, E.; Wakabayashi, A.; Yamaguchi, F.; Tsuchiya, Y.; et al. Clinical features and outcomes of aspiration pneumonia compared with non-aspiration pneumonia: A retrospective cohort study. J. Infect. Chemother. 2014, 20, 436–442. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.-Y.; Shim, S.S.; Kim, S.J.; Lee, J.H.; Chang, J.H.; Lee, S.H.; Ryu, Y.J. Long-Term Mortality and Prognostic Factors in Aspiration Pneumonia. J. Am. Med. Dir. Assoc. 2019, 20, 1098–1104.e4. [Google Scholar] [CrossRef] [PubMed]
- Metlay, J.P.; Waterer, G.W.; Long, A.C.; Anzueto, A.; Brozek, J.; Crothers, K.; Cooley, L.A.; Dean, N.C.; Fine, M.J.; Flanders, S.A.; et al. Diagnosis and treatment of adults with community-acquired pneumonia. An official clinical practice guideline of the american thoracic society and infectious diseases society of America. Am. J. Respir. Crit. Care Med. 2019, 200, e45–e67. [Google Scholar] [CrossRef]
- Lim, W.S.; Baudouin, S.V.; George, R.C.; Hill, A.T.; Jamieson, C.; Le Jeune, I.; Macfarlane, J.T.; Read, R.C.; Roberts, H.J.; Levy, M.L.; et al. BTS guidelines for the management of community acquired pneumonia in adults: Update 2009. Thorax 2009, 64, iii1–iii55. [Google Scholar] [CrossRef]
- The Japanese Respiratory Society. The JRS Guidelines for the Management of Pneumonia in Adults; Medical Review Co.: Tokyo, Japan, 2017. (In Japanese) [Google Scholar]
- Marrie, T.J.; Durant, H.; Yates, L. Community-Acquired Pneumonia Requiring Hospitalization: 5-Year Prospective Study. Clin. Infect. Dis. 1989, 11, 586–599. [Google Scholar] [CrossRef]
- Komiya, K.; Ishii, H.; Kadota, J.-I. Healthcare-associated Pneumonia and Aspiration Pneumonia. Aging Dis. 2015, 6, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Wei, C.; Cheng, Z.; Zhang, L.; Yang, J. Microbiology and prognostic factors of hospital- and community-acquired aspiration pneumonia in respiratory intensive care unit. Am. J. Infect. Control 2013, 41, 880–884. [Google Scholar] [CrossRef] [PubMed]
- Almirall, J.; Boixeda, R.; de la Torre, M.C.; Torres, A. Aspiration pneumonia: A renewed perspective and practical approach. Respir. Med. 2021, 185, 106485. [Google Scholar] [CrossRef]
- Komiya, K.; Rubin, B.K.; Kadota, J.-I.; Mukae, H.; Akaba, T.; Moro, H.; Aoki, N.; Tsukada, H.; Noguchi, S.; Shime, N.; et al. Prognostic implications of aspiration pneumonia in patients with community acquired pneumonia: A systematic review with meta-analysis. Sci. Rep. 2016, 6, 38097. [Google Scholar] [CrossRef]
- Yoshimatsu, Y.; Melgaard, D.; Westergren, A.; Skrubbeltrang, C.; Smithard, D.G. The Diagnosis of Aspiration Pneumonia: A Systematic Review. Eur. Geriatr. Med. 2022; in press. [Google Scholar]
- Kalil, A.C.; Metersky, M.L.; Klompas, M.; John Muscedere, J.; Sweeney, D.A.; Palmer, L.B.; Napolitano, L.M.; O’Grady, N.P.; Bartlett, J.G.; Carratalà, J.; et al. Management of Adults with Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin. Infect. Dis. 2016, 63, e61–e111. [Google Scholar] [CrossRef] [PubMed]
- Gidal, A.; Barnett, S. Risk Factors Associated with Multidrug-Resistant Pneumonia in Nonhospitalized Patients. Fed. Pr. Healthc. 2018, 35, 16–18. [Google Scholar]
- Shindo, Y.; Ito, R.; Kobayashi, D.; Ando, M.; Ichikawa, M.; Shiraki, A.; Goto, Y.; Fukui, Y.; Iwaki, M.; Okumura, J.; et al. Risk Factors for Drug-Resistant Pathogens in Community-acquired and Healthcare-associated Pneumonia. Am. J. Respir. Crit. Care Med. 2013, 188, 985–995. [Google Scholar] [CrossRef]
- Lim, W.S.; Van Der Eerden, M.M.; Laing, R.; Boersma, W.G.; Karalus, N.; I Town, G.; A Lewis, S.; Macfarlane, J.T. Defining community acquired pneumonia severity on presentation to hospital: An international derivation and validation study. Thorax 2003, 58, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Fine, M.J.; Auble, T.E.; Yealy, D.M.; Hanusa, B.H.; Weissfeld, L.A.; Singer, D.E.; Coley, C.M.; Marrie, T.J.; Kapoor, W.N. A Prediction Rule to Identify Low-Risk Patients with Community-Acquired Pneumonia. N. Engl. J. Med. 1997, 336, 243–250. [Google Scholar] [CrossRef]
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.B.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. CMAJ 2005, 173, 489–495. [Google Scholar] [CrossRef]
- Malmstrom, T.K.; Miller, D.K.; Simonsick, E.M.; Ferrucci, L.; Morley, J.E. SARC-F: A symptom score to predict persons with sarcopenia at risk for poor functional outcomes. J. Cachexia Sarcopenia Muscle 2016, 7, 28–36. [Google Scholar] [CrossRef]
- Chi-Square Test Calculator. Available online: https://www.socscistatistics.com/tests/chisquare/default2.aspx. (accessed on 1 July 2022).
- Fisher Exact Test Calculator. 2022. Available online: https://www.socscistatistics.com/tests/fisher/default2.aspx. (accessed on 1 July 2022).
- Hu, X.; Lee, J.S.; Pianosi, P.T.; Ryu, J.H. Aspiration-Related Pulmonary Syndromes. Chest 2015, 147, 815–823. [Google Scholar] [CrossRef]
- Yoshimatsu, Y.; Tobino, K.; Nagami, S.; Yagi, N.; Oku, Y. Breathing-Swallowing Discoordination and Inefficiency of an Airway Protective Mechanism Puts Patients at Risk of COPD Exacerbation. Int. J. Chron. Obstruct. Pulmon. Dis. 2020, 15, 1689–1696. [Google Scholar] [CrossRef]
- Yoshimatsu, Y.; Tobino, K.; Sueyasu, T.; Nishizawa, S.; Ko, Y.; Yasuda, M.; Ide, H.; Tsuruno, K.; Miyajima, H. Repetitive Saliva Swallowing Test Predicts COPD Exacerbation. Int. J. Chron. Obstruct. Pulmon. Dis. 2019, 14, 2777–2785. [Google Scholar] [CrossRef]
- Ribeiro, C.S.; Gonçalves, B.F.; Fernandes, N.; Antunes, V.; Mancopes, R.; Steidl, E. Relationship between Dysphagia and Exacerbations in Chronic Obstructive Pulmonary Disease: A Literature Review. Int. Arch. Otorhinolaryngol. 2015, 19, 074–079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raghu, G.; Collard, H.R.; Egan, J.J.; Martinez, F.J.; Behr, J.; Brown, K.K.; Colby, T.V.; Cordier, J.F.; Flaherty, K.R.; Lasky, J.A.; et al. An official ATS/ERS/JRS/ALAT statement: Idiopathic pulmonary fibrosis: Evidence-based guidelines for diagnosis and management. Am. J. Respir. Crit. Care Med. 2011, 183, 788–824. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Song, J.W.; Wolters, P.J.; Elicker, B.M.; King, T.E., Jr.; Kim, D.S.; Collard, H.R. Bronchoalveolar lavage pepsin in acute exacerbation of idiopathic pulmonary fibrosis. Eur. Respir. J. 2012, 39, 352–358. [Google Scholar] [CrossRef]
- Bush, A.; Floto, R.A. Pathophysiology, causes and genetics of paediatric and adult bronchiectasis. Respirology 2019, 24, 1053–1062. [Google Scholar] [CrossRef] [PubMed]
- Li, A.M. Non-CF bronchiectasis: Does knowing the aetiology lead to changes in management? Eur. Respir. J. 2005, 26, 8–14. [Google Scholar] [CrossRef] [PubMed]
- McShane, P.J.; Naureckas, E.T.; Strek, M.E. Bronchiectasis in a Diverse US Population. Chest 2012, 142, 159–167. [Google Scholar] [CrossRef]
- Komiya, K.; Ishii, H.; Umeki, K.; Mizunoe, S.; Okada, F.; Johkoh, T.; Kadota, J.-I. Impact of aspiration pneumonia in patients with community-acquired pneumonia and healthcare-associated pneumonia: A multicenter retrospective cohort study. Respirology 2013, 18, 514–521. [Google Scholar] [CrossRef]
- NICE. National Institute for Health and Care Excellence. Pneumonia (Including Community Acquired Pneumonia). 2014. Available online: http://www.nice.org.uk/guidance/cg191. (accessed on 22 August 2022).
- Bennett, J. Community-Acquired Pneumonia (Non COVID-19). BMJ Best Practice. July 2022. Available online: https://bestpractice.bmj.com/topics/en-gb/3000108. (accessed on 22 August 2022).
- Chandra, A.; Nicks, B.; Maniago, E.; Nouh, A.; Limkakeng, A. A multicenter analysis of the ED diagnosis of pneumonia. Am. J. Emerg. Med. 2010, 28, 862–865. [Google Scholar] [CrossRef]
- Yoshimatsu, Y.; Tobino, K.; Ko, Y.; Yasuda, M.; Ide, H.; Oku, Y. Careful history taking detects initially unknown underlying causes of aspiration pneumonia. Geriatr. Gerontol. Int. 2020, 20, 785–790. [Google Scholar] [CrossRef]
- Mandell, L.A.; Niederman, M.S. Aspiration Pneumonia. N. Engl. J. Med. 2019, 380, 651–663. [Google Scholar] [CrossRef]
- Maeda, K.; Koga, T.; Akagi, J. Tentative nil per os leads to poor outcomes in older adults with aspiration pneumonia. Clin. Nutr. 2016, 35, 1147–1152. [Google Scholar] [CrossRef] [PubMed]
- Shirado, K.; Wakabayashi, H.; Maeda, K.; Nishiyama, A.; Asada, M.; Isse, H.; Saito, S.; Kakitani, C.; Momosaki, R. Impact of Energy intake at One Week after Hospitalization on Prognosis for Older Adults with Pneumonia. J. Nutr. Heal. Aging 2019, 24, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Kenzaka, T.; Kumabe, A.; Kosami, K.; Ueda, Y.; Takahashi, T.; Yamamoto, Y.; Hayashi, Y.; Kitao, A.; Okayama, M. Effect of starting oral intake on weekends on the clinical course of patients with aspiration pneumonia. Clin. Interv. Aging 2018, 13, 895–901. [Google Scholar] [CrossRef] [PubMed]
- Momosaki, R. Rehabilitative management for aspiration pneumonia in elderly patients. J. Gen. Fam. Med. 2017, 18, 12–15. [Google Scholar] [CrossRef]
- Nakamura, T.; Kurosaki, S. Effects of Early Dysphagia Rehabilitation by Speech-language-hearing Therapists on Patients with Severe Aspiration Pneumonia. Prog. Rehabil. Med. 2020, 5, 20200020. [Google Scholar] [CrossRef]
- Serra-Prat, M.; Hinojosa, G.; López, D.; Juan, M.; Fabré, E.; Voss, D.S.; Calvo, M.; Marta, V.; Ribó, L.; Palomera, E.; et al. Prevalence of oropharyngeal dysphagia and impaired safety and efficacy of swallow in independently living older persons. J. Am. Geriatr. Soc. 2011, 59, 186–187. [Google Scholar] [CrossRef]
- Espinosa-Val, M.C.; Martín-Martínez, A.; Graupera, M.; Arias, O.; Elvira, A.; Cabré, M.; Palomera, E.; Bolívar-Prados, M.; Clavé, P.; Ortega, O. Prevalence, Risk Factors, and Complications of Oropharyngeal Dysphagia in Older Patients with Dementia. Nutrients 2020, 12, 863. [Google Scholar] [CrossRef]
- Almirall, J.; Rofes, L.; Serra-Prat, M.; Icart, R.; Palomera, E.; Arreola, V.; Clavé, P. Oropharyngeal dysphagia is a risk factor for community-acquired pneumonia in the elderly. Eur. Respir. J. 2013, 41, 923–926. [Google Scholar] [CrossRef]
- Pizzorni, N.; Valentini, D.; Gilardone, M.; Borghi, E.; Corbo, M.; Schindler, A. The Mealtime Assessment Scale (MAS): Part 1–Development of a Scale for Meal Assessment. Folia Phoniatr. Logop. 2019, 72, 169–181. [Google Scholar] [CrossRef]
- Chojin, Y.; Kato, T.; Noguchi, S.; Rikihisa, M.; Omori, M.; Mukae, H.; Yatera, K. Evaluating a novel swallowing assessment as a predictor of mortality and recurring pneumonia in elderly patients with pneumonia. Respir. Investig. 2021, 59, 783–791. [Google Scholar] [CrossRef]
- Yoshimatsu, Y.; Tobino, K.; Ortega, O.; Oda, H.; Ota, H.; Kawabata, T.; Hiramatsu, Y.; Murakami, Y.; Clavé, P. Development and Implementation of an Aspiration Pneumonia Cause Investigation Algorithm. Clin. Respir. J. 2022; Submitted. [Google Scholar]


| Factor | AP (n = 134) | Non-AP (n = 669) | p-Value | ||
|---|---|---|---|---|---|
| Background | n | %, IQR | n | %, IQR | |
| Male (n, %) | 72 | (53.7) | 351 | (52.5) | 0.79 |
| Age (median, IQR) | 85 | (80–90) | 84 | (80–89) | 0.11 |
| Care home/nursing home (n, %) | 40 | (29.9) | 76 | (11.4) | <0.001 |
| Clinical frailty scale (median, IQR) | 6 | (5–7) | 5 | (4–6) | <0.001 |
| SARC-F score (median, IQR) | 7 | (4–10) | 4 | (2–7) | <0.001 |
| Past medical history, comorbidities | |||||
| Stroke (n, %) | 28 | (20.9) | 102 | (15.2) | 0.11 |
| Neurologic disorder (n, %) | 23 | (17.2) | 28 | (4.2) | <0.001 |
| Dementia (n, %) | 69 | (51.5) | 154 | (23.0) | <0.001 |
| Other mental disorder (n, %) | 15 | (11.2) | 69 | (10.3) | 0.76 |
| Gastroesophageal reflux disease (n, %) | 8 | (6.0) | 28 | (4.2) | 0.36 |
| Other gastroesophageal disorder (n, %) | 17 | (12.7) | 53 | (7.9) | 0.07 |
| Ischemic/congestive cardiac condition (n, %) | 31 | (23.1) | 207 | (30.9) | 0.07 |
| Type 2 diabetes mellitus (n, %) | 22 | (16.4) | 161 | (24.1) | 0.05 |
| Chronic respiratory disorder (n, %) | 22 | (16.4) | 198 | (29.6) | <0.05 |
| Active cancer (n, %) | 18 | (13.4) | 93 | (13.9) | 0.89 |
| Head and neck cancer (n, %) | 2 | (1.5) | 7 | (1.0) | 0.65 |
| Immunodeficiency (n, %) | 5 | (3.7) | 72 | (10.8) | <0.05 |
| Pneumonia within 1 year (n, %) | 38 | (28.4) | 135 | (20.2) | <0.05 |
| Number of daily drugs (median, IQR) | 6 | (5–9) | 7 | (4–9) | 0.13 |
| Known dysphagia (n, %) | 60 | (44.8) | 40 | (6.0) | <0.001 |
| Risk factors of multi-drug resistant pathogens | |||||
| Hospital admission ≥2 days in the past 90 days (n, %) | 34 | (25.4) | 184 | (27.5) | <0.001 |
| Haemodialysis (n, %) | 2 | (1.5) | 5 | (0.7) | 0.33 |
| Intravenous antibiotic therapy in the last 90 days (n, %) | 26 | (19.4) | 122 | (18.2) | 0.75 |
| Factor | AP (n = 134) | Non-AP (n = 669) | p-Value | ||
|---|---|---|---|---|---|
| Symptoms | n | %, IQR | n | %, IQR | |
| Cough (n, %) | 52 | (38.8) | 314 | (46.9) | 0.08 |
| Purulent sputum (n, %) | 30 | (22.4) | 166 | (24.8) | 0.55 |
| Pleuritic pain (n, %) | 1 | (0.7) | 33 | (4.9) | <0.05 |
| Dyspnoea (n, %) | 40 | (29.9) | 380 | (56.8) | <0.001 |
| Fever (n, %) | 27 | (20.1) | 191 | (28.6) | <0.05 |
| Coughing on oral intake (n, %) | 32 | (23.9) | 12 | (1.8) | <0.001 |
| Vomiting (n, %) | 60 | (44.8) | 43 | (6.4) | <0.001 |
| Altered mental status from baseline (n, %) | 43 | (32.1) | 150 | (22.4) | <0.05 |
| Severity of the pneumonia | |||||
| CURB-65, median (n, IQR) | 2 | (2–3) | 2 | (1–2) | <0.001 |
| Pneumonia severity index (median, IQR) | 107 | (95–128) | 103 | (84–119) | <0.001 |
| Factor | AP (n = 134) | Non-AP (n = 669) | p-Value | ||
|---|---|---|---|---|---|
| Further Investigations Performed | n | % | n | % | |
| Blood culture (n, %) | 36 | (26.9) | 252 | (37.7) | <0.05 |
| Sputum culture (n, %) | 6 | (4.5) | 40 | (6.0) | 0.49 |
| Urine S. pneumoniae antigen (n, %) | 0 | (0) | 11 | (1.6) | 0.23 |
| Urine Legionella antigen (n, %) | 2 | (1.5) | 46 | (6.9) | <0.05 |
| Chest CT scan (n, %) | 12 | (9.9) | 118 | (17.6) | <0.05 |
| Antimicrobial treatment | |||||
| AP triple therapy (n, %) | 71 | (53.0) | 19 | (2.8) | <0.001 |
| Actions on admission | |||||
| SLT referral (n, %) | 94 | (70.1) | 119 | (17.8) | <0.001 |
| Nil by mouth orders (n, %) | 70 | (52.2) | 49 | (7.3) | <0.001 |
| VFSS/FEES (n, %) | 4 | (3.0) | 3 | (0.4) | <0.05 |
| Findings | AP (n = 12) | Non-AP (n = 118) | Total (n = 130) | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| No pneumonia | 4 | (33.3) | 47 | (39.8) | 51 | (39.2) |
| Only pneumonia | 6 | (50.0) | 56 | (47.5) | 62 | (47.7) |
| Other diagnosis (+/− pneumonia) | 5 | (41.7) | 51 | (43.2) | 56 | (43.1) |
| Pulmonary embolism | 0 | (0) | 14 | (11.9) | 14 | (10.8) |
| Cancer, previously unidentified | 1 | (8.3) | 16 | (13.6) | 17 | (13.1) |
| Lung | 1 | (8.3) | 12 | (10.2) | 13 | (10.0) |
| Other (mediastinal, breast, liver, adrenal) | 0 | (0) | 4 | (3.4) | 4 | (3.1) |
| New lung metastasis of known cancer | 2 | (16.7) | 6 | (5.1) | 8 | (6.2) |
| New lung nodules (no pathological diagnosis) | 0 | (0) | 3 | (2.5) | 3 | (2.3) |
| Pleural effusion | 0 | (0) | 6 | (5.1) | 6 | (4.6) |
| Pulmonary oedema | 0 | (0) | 3 | (2.5) | 3 | (2.3) |
| Other (ILD, pneumothorax, emphysema, hiatal hernia) | 2 | (16.7) | 3 | (2.5) | 5 | (3.8) |
| Causes | Total (n = 35) | |
|---|---|---|
| n | (%) | |
| Neurologic | 13 | (37.1) |
| Stroke | 7 | (20.0) |
| Dementia | 5 | (14.3) |
| Bell’s palsy | 1 | (2.9) |
| Head and neck | 3 | (8.6) |
| Oral thrush | 2 | (5.7) |
| Laryngocele | 1 | (2.9) |
| Cardiopulmonary | 3 | (8.6) |
| First-degree atrioventricular block, syncope | 1 | (2.9) |
| Chronic obstructive lung disease | 1 | (2.9) |
| Obstructive sleep apnoea | 1 | (2.9) |
| Gastrointestinal | 10 | (28.6) |
| Hiatal hernia | 4 | (11.4) |
| Cholecystitis | 1 | (2.9) |
| Metastatic oesophageal obstruction | 2 | (5.7) |
| Oesophageal stenosis | 1 | (2.9) |
| Candida esophagitis | 1 | (2.9) |
| Achalasia | 1 | (2.9) |
| Drug induced | 6 | (17.1) |
| Hypercalcemia (osteoporosis treatment) | 2 | (5.7) |
| Hypo-delirium (antipsychotic, antidepressant) | 2 | (5.7) |
| Opioid toxicity | 1 | (2.9) |
| Nausea (iron supplement) | 1 | (2.9) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoshimatsu, Y.; Smithard, D.G. A Paradigm Shift in the Diagnosis of Aspiration Pneumonia in Older Adults. J. Clin. Med. 2022, 11, 5214. https://doi.org/10.3390/jcm11175214
Yoshimatsu Y, Smithard DG. A Paradigm Shift in the Diagnosis of Aspiration Pneumonia in Older Adults. Journal of Clinical Medicine. 2022; 11(17):5214. https://doi.org/10.3390/jcm11175214
Chicago/Turabian StyleYoshimatsu, Yuki, and David G. Smithard. 2022. "A Paradigm Shift in the Diagnosis of Aspiration Pneumonia in Older Adults" Journal of Clinical Medicine 11, no. 17: 5214. https://doi.org/10.3390/jcm11175214
APA StyleYoshimatsu, Y., & Smithard, D. G. (2022). A Paradigm Shift in the Diagnosis of Aspiration Pneumonia in Older Adults. Journal of Clinical Medicine, 11(17), 5214. https://doi.org/10.3390/jcm11175214