
Long-Term Consequences of COVID-19 Lockdown in Neovascular AMD Patients in Spain: Structural and Functional Outcomes after 1 Year of Standard Follow-Up and Treatment

 , ,
, ,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. OCT Imaging
2.3. Statistical Analysis
3. Results
3.1. Characteristics of the Eyes Included in the Analysis
3.2. Functional and Anatomic Outcomes
3.2.1. Visual Acuity
3.2.2. Disease Activity Assessed by OCT
3.2.3. Intravitreal Anti-VEGF Treatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Xu, D.; Starr, M.R.; Boucher, N.; Chiang, A.; Yonekawa, Y.; Klufas, M.A.; Khan, M.A.; Cohen, M.N.; Mehta, S.; Kuriyan, A.E. Real-World Vitreoretinal Practice Patterns during the 2020 COVID-19 Pandemic: A Nationwide, Aggregated Health Record Analysis. Curr. Opin. Ophthalmol. 2020, 31, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical Course and Risk Factors for Mortality of Adult Inpatients with COVID-19 in Wuhan, China: A Retrospective Cohort Study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Shah, A.R.; Del Priore, L.V. Natural History of Predominantly Classic, Minimally Classic, and Occult Subgroups in Exudative Age-Related Macular Degeneration. Ophthalmology 2009, 116, 1901–1907. [Google Scholar] [CrossRef] [PubMed]
- Flores, R.; Carneiro, A.; Vieira, M.; Tenreiro, S.; Seabra, M.C. Age-Related Macular Degeneration: Pathophysiology, Management, and Future Perspectives. Ophthalmologica 2021, 244, 495–511. [Google Scholar] [CrossRef]
- Valverde-Megías, A.; Rego-Lorca, D.; Fernández-Vigo, J.I.; Murciano-Cespedosa, A.; Megías-Fresno, A.; García-Feijoo, J. Effect of COVID-19 Lockdown in Spain on Structural and Functional Outcomes of Neovascular AMD Patients. J. Clin. Med. 2021, 10, 3551. [Google Scholar] [CrossRef]
- Huang, Y.; Gangaputra, S.; Lee, K.E.; Narkar, A.R.; Klein, R.; Klein, B.E.K.; Meuer, S.M.; Danis, R.P. Signal Quality Assessment of Retinal Optical Coherence Tomography Images. Investig. Ophthalmol. Vis. Sci. 2012, 53, 2133–2141. [Google Scholar] [CrossRef]
- Borrelli, E.; Grosso, D.; Vella, G.; Sacconi, R.; Battista, M.; Querques, L.; Zucchiatti, I.; Prascina, F.; Bandello, F.; Querques, G. Short-Term Outcomes of Patients with Neovascular Exudative AMD: The Effect of COVID-19 Pandemic. Graefe’s Arch. Clin. Exp. Ophthalmol. 2020, 258, 2621–2628. [Google Scholar] [CrossRef]
- Stone, L.G.; Grinton, M.E.; Talks, J.S. Delayed Follow-up of Medical Retina Patients Due to COVID-19: Impact on Disease Activity and Visual Acuity. Graefe’s Arch. Clin. Exp. Ophthalmol. 2021, 259, 1773–1780. [Google Scholar] [CrossRef]
- Leng, T.; Gallivan, M.D.; Kras, A.; Lum, F.; Roe, M.T.; Li, C.; Parke, D.W.; Schwartz, S.D. Ophthalmology and COVID-19: The Impact of the Pandemic on Patient Care and Outcomes: An IRIS® Registry Study. Ophthalmology 2021, 128, 1782–1784. [Google Scholar] [CrossRef]
- Allegrini, D.; Raimondi, R.; Montesano, G.; Borgia, A.; Sorrentino, T.; Tsoutsanis, P.; Romano, M.R. Short-Term Outcomes after COVID-19-Related Treatment Interruption among Patients with Neovascular Age-Related Macular Degeneration Receiving Intravitreal Bevacizumab. Clin. Ophthalmol. 2021, 15, 4073–4079. [Google Scholar] [CrossRef]
- Sevik, M.O.; Aykut, A.; Özkan, G.; Dericioğlu, V.; Şahin, Ö. The Effect of COVID-19 Pandemic Restrictions on Neovascular AMD Patients Treated with Treat-and-Extend Protocol. Int. Ophthalmol. 2021, 41, 2951–2961. [Google Scholar] [CrossRef] [PubMed]
- Song, W.; Singh, R.P.; Rachitskaya, A.V. The Effect of Delay in Care among Patients Requiring Intravitreal Injections. Ophthalmol. Retin. 2021, 5, 975–980. [Google Scholar] [CrossRef] [PubMed]
- Jiang, B.; Gao, L.; Dong, S.; Hou, Q.; Sun, M.; Zhang, J.; Yu, H.; Zhang, Z.; Sun, D. The Influence of COVID-19 on the Stability of Patients with Neovascular Age-Related Macular Degeneration with Different Treatment Regimens. Adv. Ther. 2021, 39, 1568–1581. [Google Scholar] [CrossRef]
- Zhao, X.; Meng, L.; Luo, M.; Yu, W.; Min, H.; Dai, R.; Koh, A.; Chen, Y. The Influence of Delayed Treatment Due to COVID-19 on Patients with Neovascular Age-Related Macular Degeneration and Polypoidal Choroidal Vasculopathy. Ther. Adv. Vaccines 2018, 9, 259–261. [Google Scholar] [CrossRef] [PubMed]
- Montesel, A.; Gigon, A.; Giacuzzo, C.; Mantel, I.; Eandi, C.M. Treatment Deferral During COVID-19 Lockdown. Retina 2022, 42, 634–642. [Google Scholar] [CrossRef] [PubMed]
- Douglas, V.P.; Miller, J.B.; Douglas, K.A.A.; Vavvas, D.G.; Miller, J.W. Short-and Long-Term Visual Outcomes in Patients Receiving Intravitreal Injections: The Impact of the Coronavirus 2019 Disease (COVID-19)—Related Lockdown. J. Clin. Med. 2022, 11, 2097. [Google Scholar] [CrossRef] [PubMed]
- Stattin, M.; Ahmed, D.; Graf, A.; Haas, A.M.; Kickinger, S.; Jacob, M.; Krepler, K.; Ansari-Shahrezaei, S. The Effect of Treatment Discontinuation During the COVID-19 Pandemic on Visual Acuity in Exudative Neovascular Age-Related Macular Degeneration: 1-Year Results. Ophthalmol. Ther. 2021, 10, 935–945. [Google Scholar] [CrossRef]
- Rush, R.B.; Rush, S.W. Outcomes in Patients Resuming Intravitreal Anti-Vascular Endothelial Growth Factor Therapy Following Treatment Delay during the Coronavirus-19 Pandemic. Retina 2021, 41, 2456–2461. [Google Scholar] [CrossRef]
- Arruabarrena, C.; Toro, M.D.; Onen, M.; Malyugin, B.E.; Rejdak, R.; Tognetto, D.; Zweifel, S.; Giglio, R.; Teus, M.A. Impact on Visual Acuity in Neovascular Age Related Macular Degeneration (Namd) in Europe Due to COVID-19 Pandemic Lockdown. J. Clin. Med. 2021, 10, 3281. [Google Scholar] [CrossRef]
- Zarranz-Ventura, J.; Nguyen, V.; Creuzot-Garcher, C.; Verbraak, F.; O’Toole, L.; Invernizzi, A.; Viola, F.; Squirrel, D.; Barthelmes, D.; Gillies, M.C. International Impact of the COVID-19 Pandemic Lockdown on Intravitreal Therapy Outcomes. Retina 2022, 42, 616–627. [Google Scholar] [CrossRef]
- Arruabarrena, C.; Montejano-Milner, R.; de Aragón, F.; Allendes, G.; Teus, M.A. Resultados Del Tratamiento de Los Pacientes Con DMAE Exudativa Durante La Pandemia Por COVID-19. Arch. Soc. Esp. Oftalmol. 2021, 97, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Yeter, D.Y.; Dursun, D.; Bozali, E.; Ozec, A.V.; Erdogan, H. Effects of the COVID-19 Pandemic on Neovascular Age-Related Macular Degeneration and Response to Delayed Anti-VEGF Treatment. J. Fr. Ophtalmol. 2021, 44, 299–306. [Google Scholar] [CrossRef] [PubMed]
- Muether, P.S.; Hermann, M.M.; Koch, K.; Fauser, S. Delay between Medical Indication to Anti-VEGF Treatment in Age-Related Macular Degeneration Can Result in a Loss of Visual Acuity. Graefe’s Arch. Clin. Exp. Ophthalmol. 2011, 249, 633–637. [Google Scholar] [CrossRef] [PubMed]
- Muether, P.S.; Hoerster, R.; Hermann, M.M.; Kirchhof, B.; Fauser, S. Long-Term Effects of Ranibizumab Treatment Delay in Neovascular Age-Related Macular Degeneration. Graefe’s Arch. Clin. Exp. Ophthalmol. 2013, 251, 453–458. [Google Scholar] [CrossRef]
- Rosenfeld, P.J.; Brown, D.M.; Heier, J.S.; Boyer, D.S.; Kaiser, P.K.; Chung, C.Y.; Kim, R.Y. Ranibizumab for Neovascular Age-Related Macular Degeneration. N. Engl. J. Med. 2006, 355, 1419–1431. [Google Scholar] [CrossRef]
- Brown, D.M.; Michels, M.; Kaiser, P.K.; Heier, J.S.; Sy, J.P.; Ianchulev, T. Ranibizumab versus Verteporfin Photodynamic Therapy for Neovascular Age-Related Macular Degeneration: Two-Year Results of the ANCHOR Study. Ophthalmology 2006, 116, 57–65.e5. [Google Scholar] [CrossRef]
- Regillo, C.D.; Brown, D.M.; Abraham, P.; Yue, H.; Ianchulev, T.; Schneider, S.; Shams, N. Randomized, Double-Masked, Sham-Controlled Trial of Ranibizumab for Neovascular Age-Related Macular Degeneration: PIER Study Year 1. Am. J. Ophthalmol. 2008, 145, 239–248. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Age (years), mean (SD) | 82.5 (6.3) |
| Patients with both eyes eligible (%) | 26 (10.6%) |
| Years since MNV diagnosis, mean (SD; range) | 4.9 (3.2; 1–14.3) |
| MNV type, n (%) | |
| Type 1 | 161 (65.7%) |
| Type 2 | 50 (20.4%) |
| Type 3 | 29 (11.8%) |
| AT-1 | 5 (2%) |
| Anti-VEGF used, n (%) | |
| Ranibizumab | 95 (38.8%) |
| Aflibercept | 89 (36.3%) |
| Bevacizumab | 61 (24.9%) |
| Regimen | |
| Pro re nata | 102 (41.6%) |
| Treat-and-extend | 37 (15.1%) |
| Fixed | 106 (43.3%) |
| Anti-VEGF injections, mean (SD; range) | 5.4 (1.8; 1–11) |
| Delay in follow-up/treatment (days), mean (SD; range) | 101.4 (56.6; 28–298) |
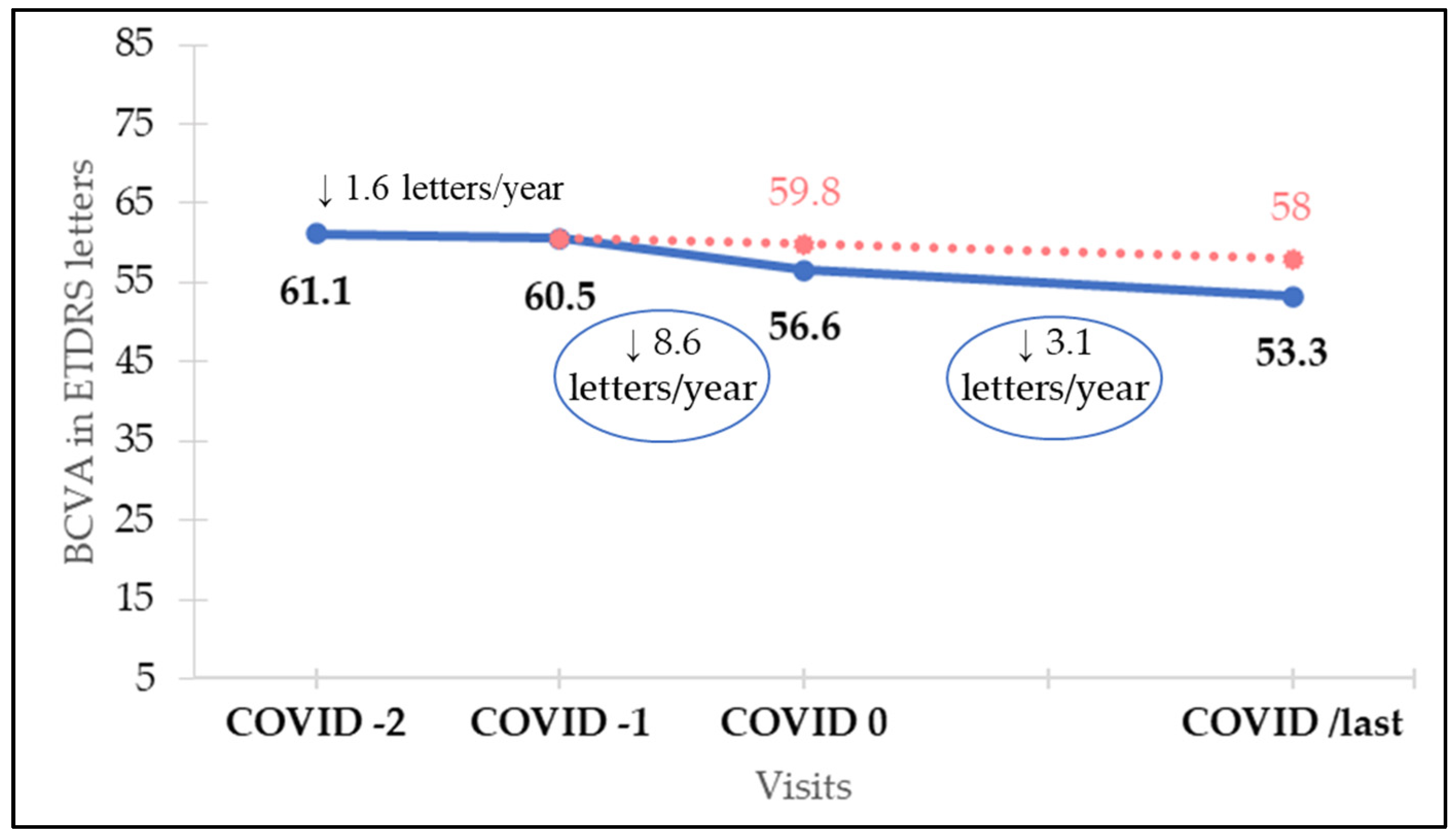
| ETDRS Letters, Mean (SD; Range) | vs. COVID 0 p Value | vs. COVID-1 p Value | |
|---|---|---|---|
| COVID-2 | 61.1 (18.7; 5–91) | 0.006 | 0.58 |
| COVID-1 | 60.5 (18.5; 5–85) | 0.028 | - |
| COVID 0 | 56.6 (20.4; 5–90) | - | 0.028 |
| COVID+1 | 55.8 (20.6; 5–90) | 0.57 | 0.0075 |
| COVID/last | 53.3 (22; 5–90) | 0.11 | <0.001 |
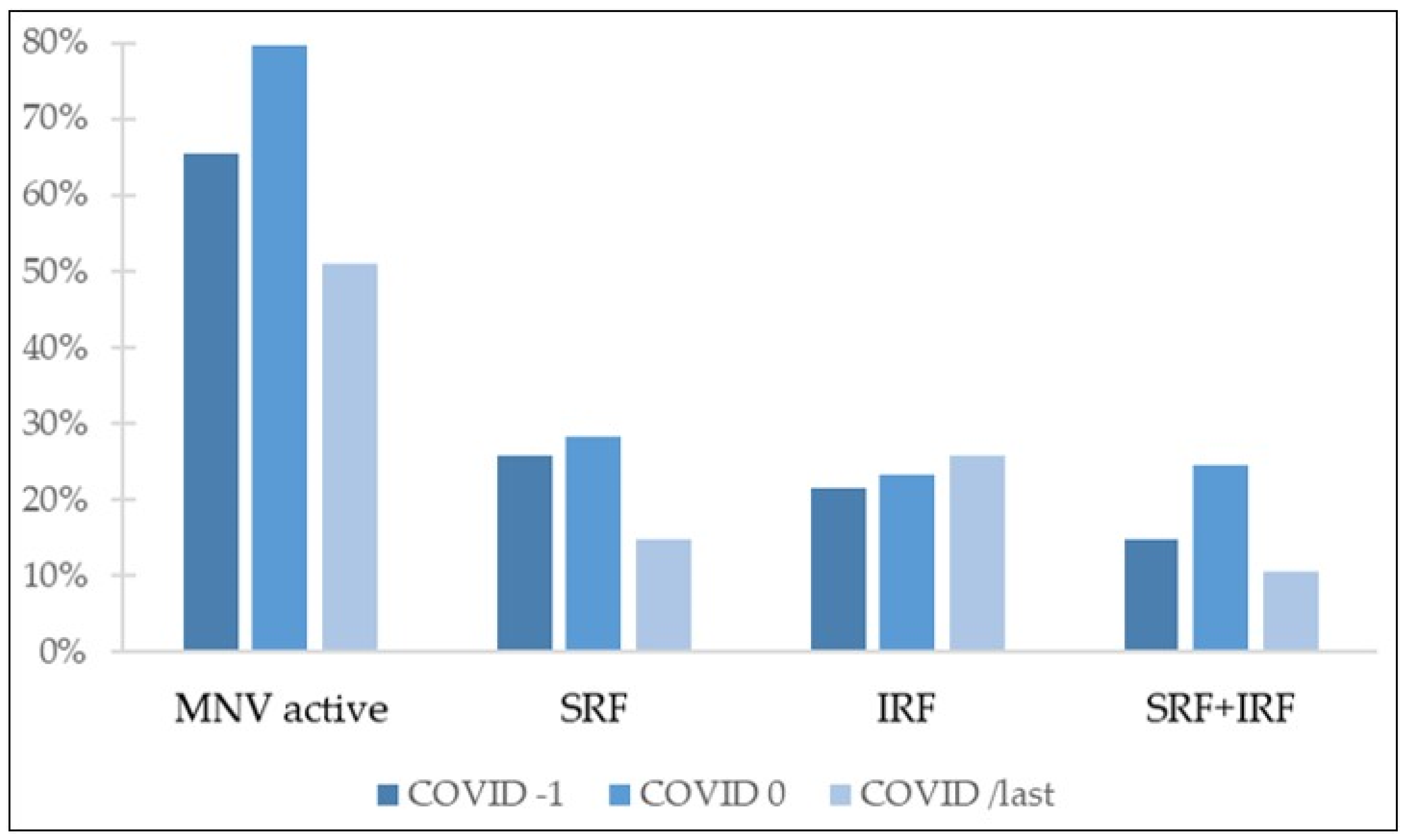
| Active MNV n (%) | SRF n (%) | IRF n (%) | SRF and IRF n (%) | CME n (%) | CRT Mean ± SD | |
|---|---|---|---|---|---|---|
| COVID-1 | 160 (65.3%) | 63 (25.7%) | 53 (21.6%) | 36 (14.7%) | 8 (3.3%) | 303.8 ± 162.2 |
| COVID 0 | 195 (79.6%) | 69 (28.2%) | 57 (23.3%) | 60 (24.5%) | 8 (3.3%) | 343.9 ± 186.6 |
| COVID/last | 125 (51%) | 36 (14.7%) | 63 (25.7%) | 26 (10.6%) | 0 (0%) | 293.4 ± 211.8 |
| COVID/last vs. COVID 0 p value | <0.001 | <0.001 | 0.532 | <0.001 | 0.0043 | <0.001 |
| COVID/last vs. COVID-1 p value | 0.0017 | <0.001 | 0.289 | 0.17 | 0.0043 | 0.117 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rego-Lorca, D.; Valverde-Megías, A.; Fernández-Vigo, J.I.; Oribio-Quinto, C.; Murciano-Cespedosa, A.; Sánchez-Quirós, J.; Donate-López, J.; García-Feijóo, J. Long-Term Consequences of COVID-19 Lockdown in Neovascular AMD Patients in Spain: Structural and Functional Outcomes after 1 Year of Standard Follow-Up and Treatment. J. Clin. Med. 2022, 11, 5063. https://doi.org/10.3390/jcm11175063
Rego-Lorca D, Valverde-Megías A, Fernández-Vigo JI, Oribio-Quinto C, Murciano-Cespedosa A, Sánchez-Quirós J, Donate-López J, García-Feijóo J. Long-Term Consequences of COVID-19 Lockdown in Neovascular AMD Patients in Spain: Structural and Functional Outcomes after 1 Year of Standard Follow-Up and Treatment. Journal of Clinical Medicine. 2022; 11(17):5063. https://doi.org/10.3390/jcm11175063
Chicago/Turabian StyleRego-Lorca, Daniela, Alicia Valverde-Megías, José Ignacio Fernández-Vigo, Carlos Oribio-Quinto, Antonio Murciano-Cespedosa, Julia Sánchez-Quirós, Juan Donate-López, and Julián García-Feijóo. 2022. "Long-Term Consequences of COVID-19 Lockdown in Neovascular AMD Patients in Spain: Structural and Functional Outcomes after 1 Year of Standard Follow-Up and Treatment" Journal of Clinical Medicine 11, no. 17: 5063. https://doi.org/10.3390/jcm11175063
APA StyleRego-Lorca, D., Valverde-Megías, A., Fernández-Vigo, J. I., Oribio-Quinto, C., Murciano-Cespedosa, A., Sánchez-Quirós, J., Donate-López, J., & García-Feijóo, J. (2022). Long-Term Consequences of COVID-19 Lockdown in Neovascular AMD Patients in Spain: Structural and Functional Outcomes after 1 Year of Standard Follow-Up and Treatment. Journal of Clinical Medicine, 11(17), 5063. https://doi.org/10.3390/jcm11175063