
The Value of Different Short-Term Risk Scoring Models in Predicting Long-Term Death of Acute Myocardial Infarction

Abstract
1. Introduction
2. Methods
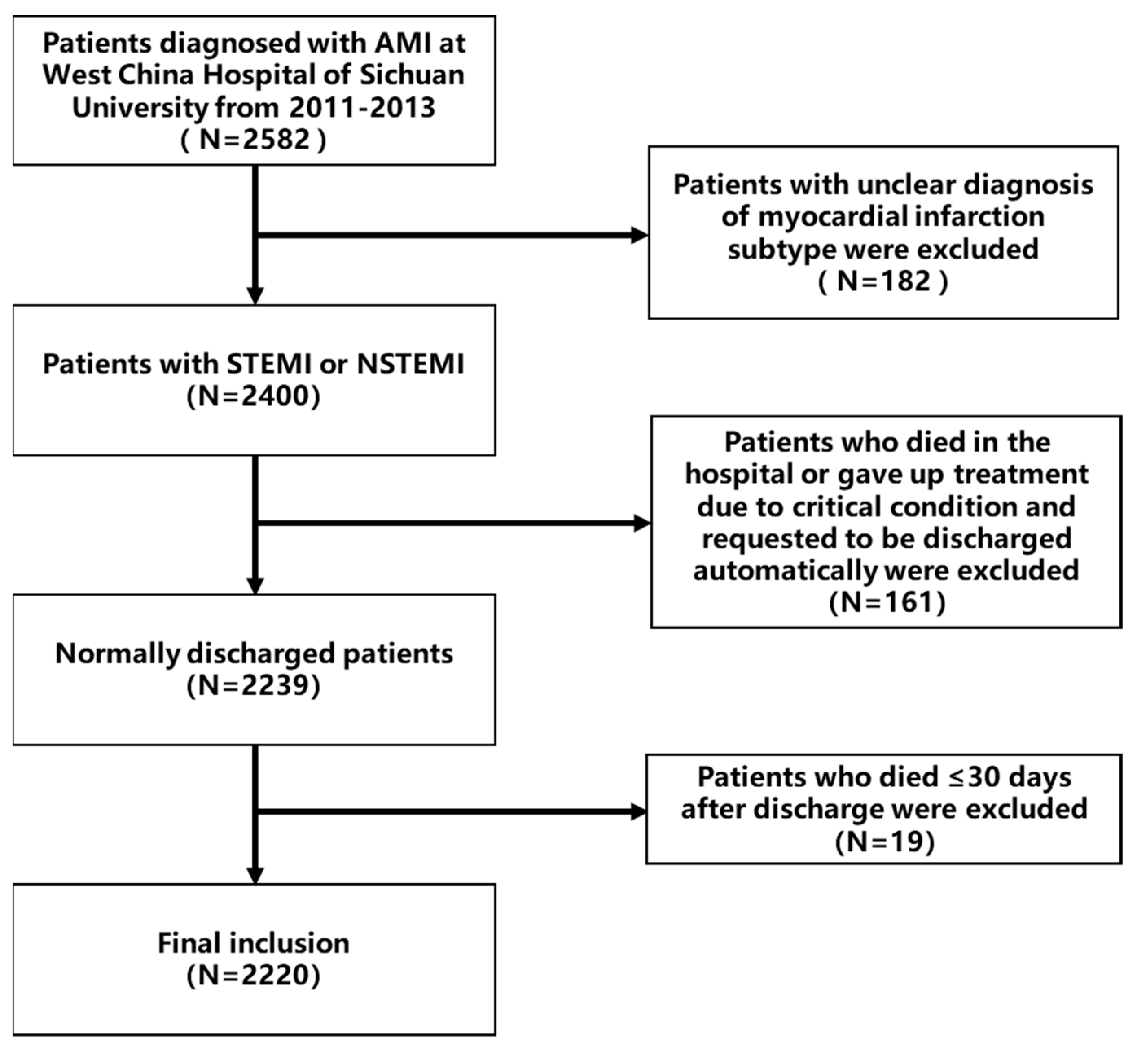
2.1. Study Population
2.2. Data Collection
2.3. Risk Scores
2.4. Follow-Up and Study Endpoint
2.5. Statistical Analysis
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Nichols, M.; Townsend, N.; Scarborough, P.; Rayner, M. Cardiovascular disease in Europe 2014: Epidemiological update. Eur. Heart J. 2014, 35, 2950–2959. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, E.J.; Blaha, M.J.; Chiuve, S.E.; Cushman, M.; Das, S.R.; Deo, R.; de Ferranti, S.D.; Floyd, J.; Fornage, M.; Gillespie, C.; et al. Heart Disease and Stroke Statistics-2017 Update: A Report From the American Heart Association. Circulation 2017, 135, e146–e603. [Google Scholar] [CrossRef] [PubMed]
- Rogers, W.J.; Frederick, P.D.; Stoehr, E.; Canto, J.G.; Ornato, J.P.; Gibson, C.M.; Pollack, C.V., Jr.; Gore, J.M.; Chandra-Strobos, N.; Peterson, E.D.; et al. Trends in presenting characteristics and hospital mortality among patients with ST elevation and non-ST elevation myocardial infarction in the National Registry of Myocardial Infarction from 1990 to 2006. Am. Heart J. 2008, 156, 1026–1034. [Google Scholar] [CrossRef]
- Krumholz, H.M.; Normand, S.L.; Wang, Y. Trends in hospitalizations and outcomes for acute cardiovascular disease and stroke, 1999–2011. Circulation 2014, 130, 966–975. [Google Scholar] [CrossRef]
- Roe, M.T.; Messenger, J.C.; Weintraub, W.S.; Cannon, C.P.; Fonarow, G.C.; Dai, D.; Chen, A.Y.; Klein, L.W.; Masoud, F.A.; McKay, C.; et al. Treatments, trends, and outcomes of acute myocardial infarction and percutaneous coronary intervention. J. Am. Coll. Cardiol. 2010, 56, 254–263. [Google Scholar] [CrossRef]
- China Cardiovascular Health and Disease Report Writing Group. China Cardiovascular Health and Disease Report 2020 Summary. Report on Cardiovascular Health and Diseases Burden in China: An Updated Summary of 2020. Chin. Circ. J. 2021, 36, 521–545. (In Chinese) [Google Scholar]
- Castro-Dominguez, Y.; Dharmarajan, K.; Mcnamara, R.L. Predicting death after acute myocardial infarction. Trends Cardiovasc. Med. 2018, 28, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar]
- Granger, C.B.; Goldberg, R.J.; Dabbous, O.; Pieper, K.S.; Eagle, K.A.; Cannon, C.P. Predictors of hospital mortality in the global registry of acute coronary events. Arch. Intern. Med. 2003, 163, 2345–2353. [Google Scholar] [CrossRef]
- Antman, E.M.; Cohen, M.; Bernink, P.J.; McCabe, C.H.; Horacek, T.; Papuchis, G.; Mautner, B.; Corbalan, R.; Radley, D.; Braunwald, E. The TIMI risk score for unstable angina/non-ST elevation MI: A method for prognostication and therapeutic decision making. JAMA 2000, 284, 835–842. [Google Scholar] [CrossRef]
- Morrow, D.A.; Antman, E.M.; Charlesworth, A.; Cairns, R.; Murphy, S.A.; de Lemos, J.A.; Giugliano, R.P.; McCabe, C.H.; Braunwald, E. TIMI risk score for ST-elevation myocardial infarction: A convenient, bedside, clinical score for risk assessment at presentation: An intravenous nPA for treatment of infarcting myocardium early II trial substudy. Circulation 2000, 102, 2031–2037. [Google Scholar] [CrossRef] [PubMed]
- Six, A.J.; Backus, B.E.; Kelder, J.C. Chest pain in the emergency room: Value of the HEART score. Neth. Heart J. 2008, 16, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Soiza, R.L.; Leslie, S.J.; Williamson, P.; Wai, S.; Harrild, K.; Peden, N.R.; Hargreaves, A.D. Risk stratification in acute coronary syndromes—does the TIMI risk score work in unselected cases? QJM 2006, 99, 81–87. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Morrow, D.A.; Antman, E.M.; Parsons, L.; de Lemos, J.A.; Cannon, C.P.; Giugliano, R.P.; McCabe, C.H.; Barron, H.V.; Braunwald, E. Application of the TIMI risk score for ST-elevation MI in the National Registry of Myocardial Infarction 3. JAMA 2001, 286, 1356–1359. [Google Scholar] [CrossRef]
- Jain, T.; Nowak, R.; Hudson, M.; Frisoli, T.; Jacobsen, G.; McCord, J. Short- and Long-Term Prognostic Utility of the HEART Score in Patients Evaluated in the Emergency Department for Possible Acute Coronary Syndrome. Crit. Pathw. Cardiol. 2016, 15, 40–45. [Google Scholar] [CrossRef]
- Poldervaart, J.M.; Langedijk, M.; Backus, B.E.; Dekker, I.M.C.; Six, A.J.; Doevendans, P.A.; Hoes, A.W.; Reitsma, J.B. Comparison of the GRACE, HEART and TIMI score to predict major adverse cardiac events in chest pain patients at the emergency department. Int. J. Cardiol. 2017, 227, 656–661. [Google Scholar] [CrossRef]
- Kristensen, S.D.; Laut, K.G.; Fajadet, J.; Kaifoszova, Z.; Kala, P.; Di Mario, C.; Wijns, W.; Clemmensen, P.; Agladze, V.; Antoniades, L.; et al. Reperfusion therapy for ST elevation acute myocardial infarction 2010/2011: Current status in 37 ESC countries. Eur. Heart J. 2014, 35, 1957–1970. [Google Scholar] [CrossRef]
- Pedersen, F.; Butrymovich, V.; Kelbæk, H.; Wachtell, K.; Helqvist, S.; Kastrup, J.; Holmvang, L.; Clemmensen, P.; Engstrøm, T.; Grande, P.; et al. Short- and long-term cause of death in patients treated with primary PCI for STEMI. J. Am. Coll. Cardiol. 2014, 64, 2101–2118. [Google Scholar] [CrossRef]
- Fokkema, M.L.; James, S.K.; Albertsson, P.; Akerblom, A.; Calais, F.; Eriksson, P.; Jensen, J.; Nilsson, T.; de Smet, B.J.; Sjögren, I.; et al. Population trends in percutaneous coronary intervention: 20-year results from the SCAAR (Swedish Coronary Angiography and Angioplasty Registry). J. Am. Coll. Cardiol. 2013, 61, 1222–1230. [Google Scholar] [CrossRef]
- Li, J.; Li, X.; Wang, Q.; Hu, S.; Wang, Y.; Masoudi, F.A.; Spertus, J.A.; Krumholz, H.M.; Jiang, L.; China PEACE Collaborative Group. ST-segment elevation myocardial infarction in China from 2001 to 2011 (the China PEACE-Retrospective Acute Myocardial Infarction Study): A retrospective analysis of hospital data. Lancet 2015, 385, 441–451. [Google Scholar] [CrossRef]
- Addala, S.; Grines, C.L.; Dixon, S.R.; Stone, G.W.; Boura, J.A.; Ochoa, A.B.; Pellizzon, G.; O’Neill, W.W.; Kahn, J.K. Predicting mortality in patients with ST-elevation myocardial infarction treated with primary percutaneous coronary intervention (PAMI risk score). Am. J. Cardiol. 2004, 93, 629–632. [Google Scholar] [CrossRef] [PubMed]
- Halkin, A.; Singh, M.; Nikolsky, E.; Grines, C.L.; Tcheng, J.E.; Garcia, E.; Cox, D.A.; Turco, M.; Stuckey, T.D.; Na, Y.; et al. Prediction of mortality after primary percutaneous coronary intervention for acute myocardial infarction: The CADILLAC risk score. J. Am. Coll. Cardiol. 2005, 45, 1397–1405. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.H.; Huang, S.S.; Lin, S.J. TIMI and GRACE Risk Scores Predict Both Short-Term and Long-Term Outcomes in Chinese Patients with Acute Myocardial Infarction. Acta Cardiol. Sin. 2018, 34, 4–12. [Google Scholar] [PubMed]
- Littnerova, S.; Kala, P.; Jarkovsky, J.; Kubkova, L.; Prymusova, K.; Kubena, P.; Tesak, M.; Toman, O.; Poloczek, M.; Spinar, J.; et al. GRACE Score among Six Risk Scoring Systems (CADILLAC, PAMI, TIMI, Dynamic TIMI, Zwolle) Demonstrated the Best Predictive Value for Prediction of Long-Term Mortality in Patients with ST-Elevation Myocardial Infarction. PLoS ONE 2015, 10, e0123215. [Google Scholar]
- Lev, E.I.; Kornowski, R.; Vaknin-Assa, H.; Porter, A.; Teplitsky, I.; Ben-Dor, I.; Brosh, D.; Fuchs, S.; Battler, A.; Assali, A. Comparison of the predictive value of four different risk scores for outcomes of patients with ST-elevation acute myocardial infarction undergoing primary percutaneous coronary intervention. Am. J. Cardiol. 2008, 102, 6–11. [Google Scholar] [CrossRef]
- Kozieradzka, A.; Kamiński, K.A.; Maciorkowska, D.; Olszewska, M.; Dobrzycki, S.; Nowak, K.; Kralisz, P.; Prokopczuk, P.; Musial, W.J. GRACE, TIMI, Zwolle and CADILLAC risk scores--do they predict 5-year outcomes after ST-elevation myocardial infarction treated invasively? Int. J. Cardiol. 2011, 148, 70–75. [Google Scholar] [CrossRef]
- Anavekar, N.S.; Mcmurray, J.J.; Velazquez, E.J.; Solomon, S.D.; Kober, L.; Rouleau, J.L.; White, H.D.; Nordlander, R.; Maggioni, A.; Dickstein, K.; et al. Relation between renal dysfunction and cardiovascular outcomes after myocardial infarction. N Engl. J. Med. 2004, 351, 1285–1295. [Google Scholar] [CrossRef]
- Nesković, A.N.; Otasević, P.; Bojić, M.; Popović, A.D. Association of Killip class on admission and left ventricular dilatation after myocardial infarction: A closer look into an old clinical classification. Am. Heart J. 1999, 137, 361–367. [Google Scholar] [CrossRef]
- Khot, U.N.; Jia, G.; Moliterno, D.J.; Lincoff, A.M.; Khot, M.B.; Harrington, R.A.; Topol, E.J. Prognostic importance of physical examination for heart failure in non-ST-elevation acute coronary syndromes: The enduring value of Killip classification. Jama 2003, 290, 2174–2181. [Google Scholar] [CrossRef]
- Sutton, M.G.; Sharpe, N. Left ventricular remodeling after myocardial infarction: Pathophysiology and therapy. Circulation 2000, 101, 2981–2988. [Google Scholar] [CrossRef]
- Francis Stuart, S.D.; De Jesus, N.M.; Lindsey, M.L.; Lindsey, M.L.; Ripplinger, C.M. The crossroads of inflammation, fibrosis, and arrhythmia following myocardial infarction. J. Mol. Cell Cardiol. 2016, 91, 114–122. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | GRACE | TIMI (STEMI) | TIMI (NSTEMI) | HEART | ||
|---|---|---|---|---|---|---|
| Age | X | X | X | X | ||
| Medical history | Time from onset to visit | X | ||||
| Suspicious degree | X | |||||
| Severe angina (≥2 events in last 24 h) | X | |||||
| Use of aspirin last 7 days | X | |||||
| Physical examination | Body weight | X | ||||
| Heart rate | X | X | ||||
| Systolic blood pressure | X | X | ||||
| Killip class | X | X | ||||
| ECG | ST deviation | X | X | X | X | |
| Repolarization disorder, BBB, or LVH | X | X | ||||
| Cardiac arrest at admission | X | |||||
| Laboratory results | Creatinine level | X | ||||
| Troponin T level | X | X | X | |||
| Risk factors | Cardiovascular risk factors * | X | X | X | ||
| Previous coronary artery disease (≥50%) | X | |||||
| Previous revascularization | X | |||||
| History of cerebrovascular vascular disease | X | |||||
| History of peripheral vascular disease | X | |||||
| Obesity | X | |||||
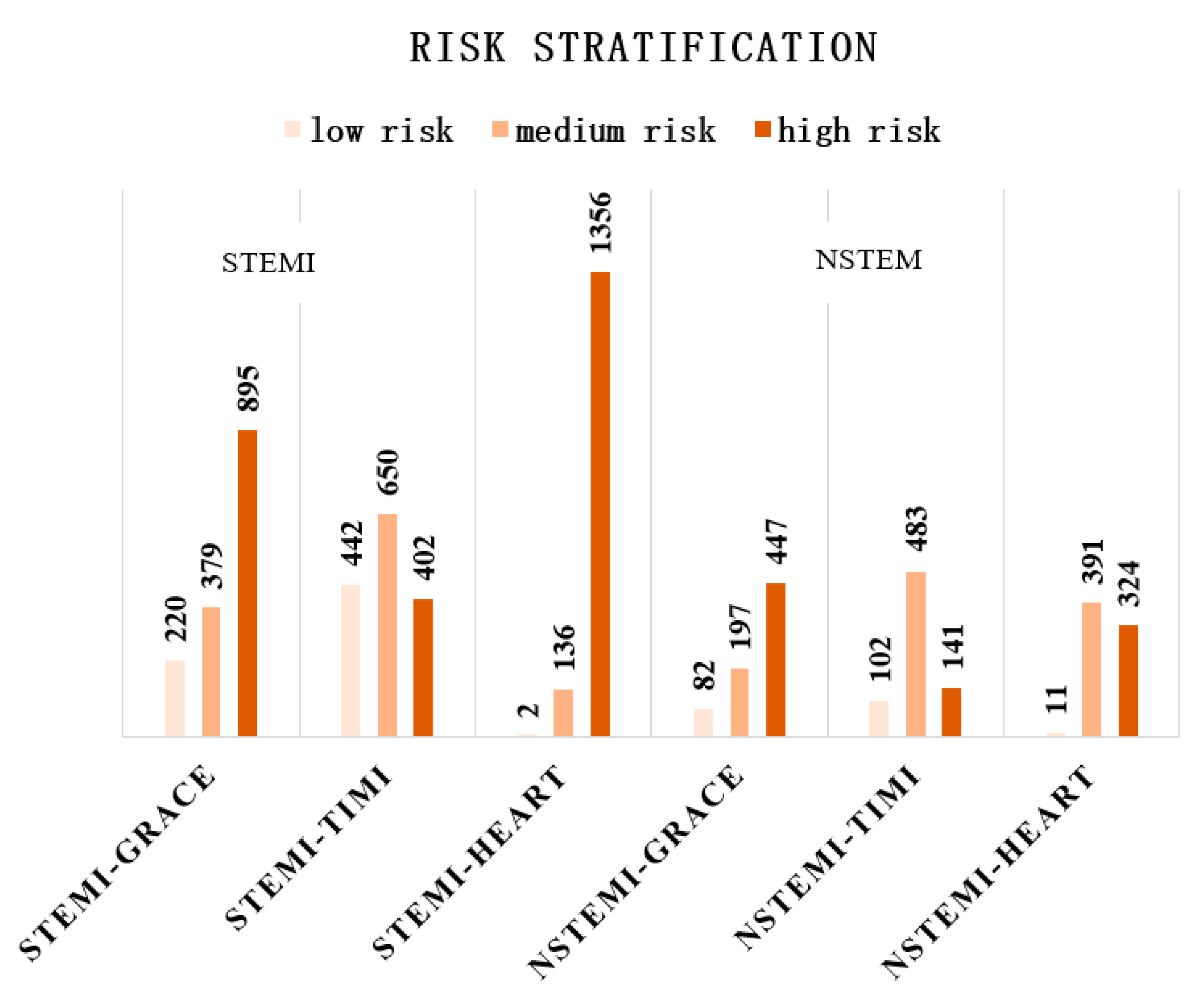
| Risk stratification | Low-risk | STEMI | <125 | 0–3 | 0–2 | 0–3 |
| NSTEMI | <108 | |||||
| Intermediate-risk | STEMI | 126–154 | 4–6 | 3–4 | 4–6 | |
| NSTEMI | 109–140 | |||||
| High-risk | STEMI | >154 | 7–14 | 5–7 | 7–10 | |
| NSTEMI | >140 | |||||
| CLINICAL CHARACTERISTICS | TOTAL (N = 2220) | STEMI (N = 1494) | NSTEMI (N = 726) |
|---|---|---|---|
| AGE, YRS | 66 (56, 74) | 63 (53, 72) | 70 (62, 75) |
| MALE, N (%) | 1752 (78.9) | 1220 (81.7) | 565 (73.3) |
| VITAL SIGNS AT PRESENTATION | |||
| SYSTOLIC BLOOD PRESSURE, MMHG | 125 (110, 140) | 122 (109, 138) | 130 (113, 146) |
| DIASTOLIC BLOOD PRESSURE, MMHG | 75 (66, 84) | 74 (66, 85) | 75 (66, 83) |
| HEART RATE, BEATS/MIN | 78 (67, 88) | 78 (68, 89) | 77 (66, 86) |
| KILLIP CLASS > II, N (%) | 1220 (55.0) | 793 (53.1) | 477 (58.8) |
| CARDIAC RISK FACTORS, N (%) | |||
| HYPERTENSION | 1099 (49.5) | 657 (44.0) | 468 (60.1) |
| DIABETES | 449 (20.2) | 261 (17.5) | 199 (25.9) |
| HYPERLIPIDEMIA | 69 (3.1) | 47 (3.1) | 22 (3.0) |
| CURRENT SMOKING | 1358 (61.2) | 1026 (65.0) | 388 (53.4) |
| OBESITY (BMI ≥ 28 KG/M2) | 307 (13.8) | 205 (13.7) | 102 (14.0) |
| POSITIVE FAMILY HISTORY | 103 (4.6) | 62 (4.1) | 41 (5.6) |
| HISTORY OF CARDIOVASCULAR DISEASE | 270 (12.2) | 119 (8.0) | 151 (20.8) |
| HISTORY OF AMI | 256 (11.5) | 173 (11.6) | 83 (11.4) |
| HISTORY OF PCI | 33 (1.5) | 13 (0.9) | 20 (2.8) |
| HISTORY OF CABG | 5 (0.2) | 1 (0.1) | 4 (0.6) |
| HISTORY OF CVA/TIA | 98 (4.4) | 63 (4.2) | 35 (4.8) |
| HISTORY OF PERIPHERAL ARTERIAL DISEASE | 11 (0.5) | 4 (0.3) | 7 (1.0) |
| LABORATORY RESULTS AT PRESENTATION | |||
| MEAN CREATININE IN μMOL/L (SD) | 97 (73,103) | 84 (72,100) | 90 (75, 111) |
| CTNT, NG/L | 1702 (343, 4025) | 2440 (593, 4801) | 743 (177, 2212) |
| NT-PROBNP, PG/ML | 1661 (646, 4222) | 1714 (671, 4142) | 1586 (566, 4466) |
| MEDICATION AT PRESENTATION, N (%) | |||
| ASPIRIN | 2046 (92.2) | 1390 (93.0) | 656 (90.3) |
| CLOPIDOGREL/TICLOPIDINE | 2099 (94.5) | 1411 (94.4) | 688 (94.8) |
| ACEI/ARB | 1183 (53.3) | 783 (52.4) | 398 (54.8) |
| BETA BLOCKERS | 1424 (64.1) | 963 (64.5) | 461 (63.5) |
| STATINS | 2033 (91.6) | 1360 (91.0) | 673 (92.7) |
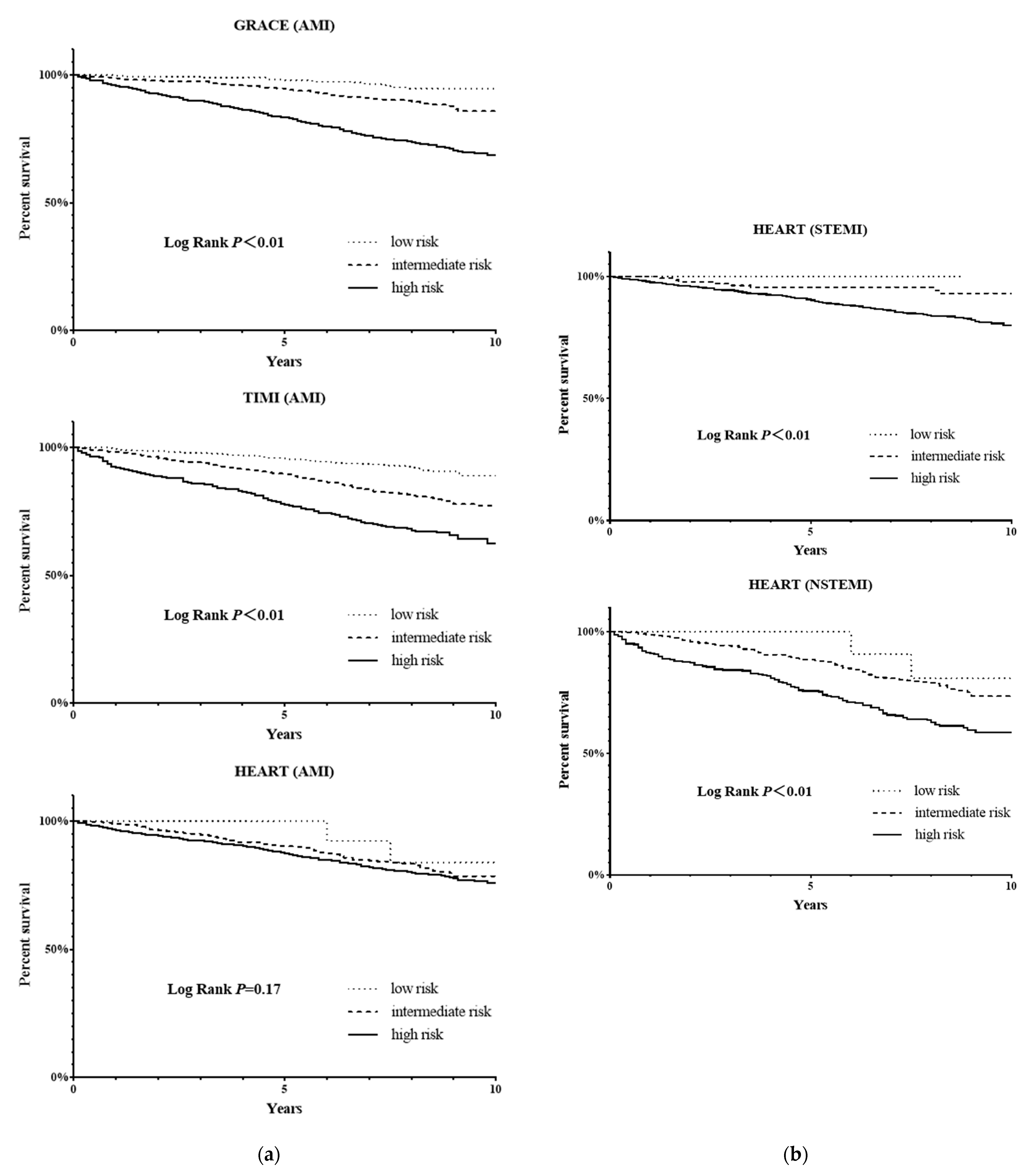
| FOLLOW-UP AND ENDPOINT EVENTS | |||
| FOLLOW-UP TIME, YEARS | 8 (7.3, 8.9) | 8.1 (7.4, 9) | 7.9 (6.8, 8.8) |
| 1-YEAR CUMULATIVE DEATH, N (%) | 64 (2.9) | 30 (2.0) | 34 (4.7) |
| 3-YEAR CUMULATIVE DEATH, N (%) | 152 (6.8) | 79 (5.3) | 73 (10.1) |
| 5-YEAR CUMULATIVE DEATH, N (%) | 259 (11.7) | 135 (9.0) | 124 (17.1) |
| CUMULATIVE DEATHS AT THE END OF FOLLOW-UP, N (%) | 454 (20.5) | 236 (15.8) | 218 (30.0) |
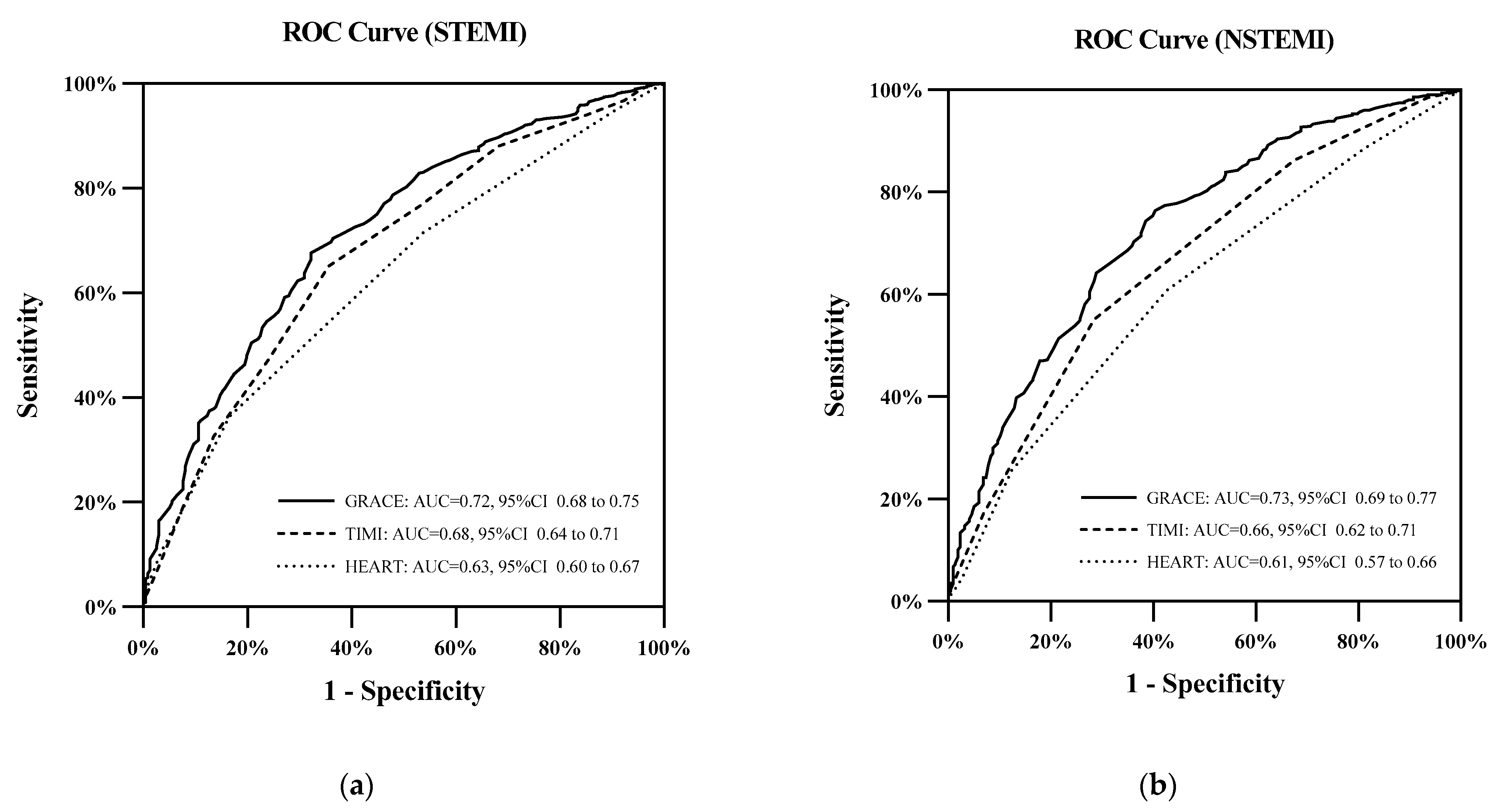
| Cumulative Deaths | GRACE | TIMI | HEART | p | ||
|---|---|---|---|---|---|---|
| G vs. T | G vs. H | T vs. H | ||||
| STEMI | ||||||
| 1-year | 0.775 | 0.770 | 0.719 | 0.87 | 0.25 | 0.29 |
| 3-year | 0.762 | 0.719 | 0.643 | <0.05 | <0.01 | <0.05 |
| 5-year | 0.740 | 0.702 | 0.617 | <0.05 | <0.01 | <0.01 |
| End of follow-up | 0.734 | 0.675 | 0.632 | <0.01 | <0.01 | <0.05 |
| NSTEMI | ||||||
| 1-year | 0.779 | 0.730 | 0.739 | 0.30 | 0.37 | 0.88 |
| 3-year | 0.762 | 0.678 | 0.658 | <0.05 | <0.01 | 0.58 |
| 5-year | 0.738 | 0.656 | 0.629 | <0.01 | <0.01 | 0.30 |
| End of follow-up | 0.730 | 0.665 | 0.611 | <0.01 | <0.01 | <0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, B.; Bai, L.; Zhang, Y.; Cheng, Y.; Zhao, C.; Huang, B.; Chen, M. The Value of Different Short-Term Risk Scoring Models in Predicting Long-Term Death of Acute Myocardial Infarction. J. Clin. Med. 2022, 11, 5054. https://doi.org/10.3390/jcm11175054
Yang B, Bai L, Zhang Y, Cheng Y, Zhao C, Huang B, Chen M. The Value of Different Short-Term Risk Scoring Models in Predicting Long-Term Death of Acute Myocardial Infarction. Journal of Clinical Medicine. 2022; 11(17):5054. https://doi.org/10.3390/jcm11175054
Chicago/Turabian StyleYang, Bosen, Lin Bai, Yike Zhang, Yiheng Cheng, Chunyan Zhao, Baotao Huang, and Mao Chen. 2022. "The Value of Different Short-Term Risk Scoring Models in Predicting Long-Term Death of Acute Myocardial Infarction" Journal of Clinical Medicine 11, no. 17: 5054. https://doi.org/10.3390/jcm11175054
APA StyleYang, B., Bai, L., Zhang, Y., Cheng, Y., Zhao, C., Huang, B., & Chen, M. (2022). The Value of Different Short-Term Risk Scoring Models in Predicting Long-Term Death of Acute Myocardial Infarction. Journal of Clinical Medicine, 11(17), 5054. https://doi.org/10.3390/jcm11175054