
Association between Outpatient Visits and Initiating Medication among Elderly Patients after an Osteoporotic Vertebral Fracture

 , and
, and
Abstract
1. Introduction
2. Methods
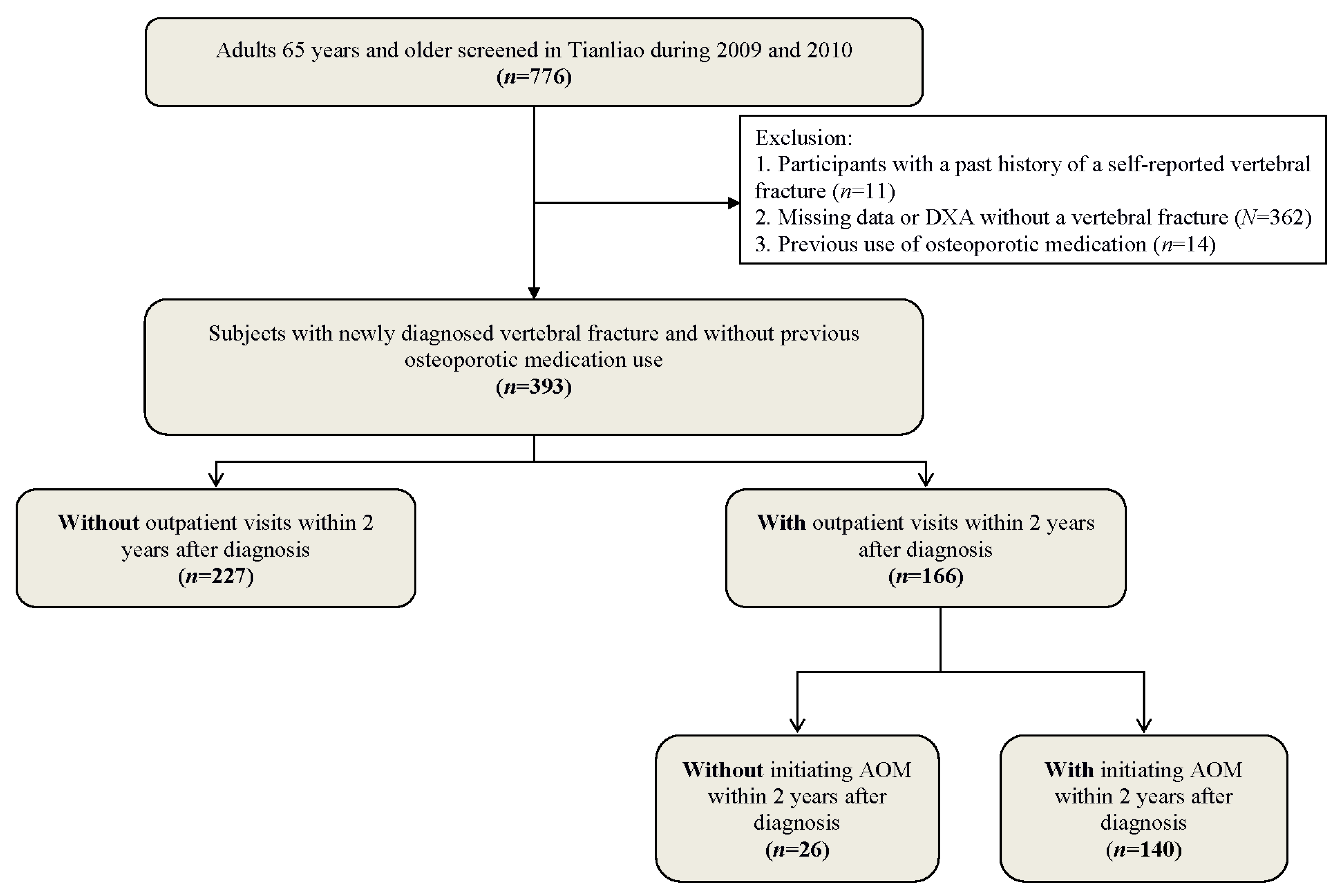
2.1. Participants
2.2. Data Collection
2.3. BMD Measurement
2.4. Vertebral Fracture Assessment
2.5. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Caires, E.L.P.; Bezerra, M.C.; Junqueira, A.; Fontenele, S.M.A.; Andrade, S.C.A.; d’Alva, C.B. Treatment of postmenopausal osteoporosis: A literature-based algorithm for use in the public health care system. Rev. Bras. Reumatol. Engl. Ed. 2017, 57, 254–263. [Google Scholar] [CrossRef]
- Stevenson, M.; Jones, M.L.; De Nigris, E.; Brewer, N.; Davis, S.; Oakley, J. A systematic review and economic evaluation of alendronate, etidronate, risedronate, raloxifene and teriparatide for the prevention and treatment of postmenopausal osteoporosis. Health Technol. Assess. 2005, 9, 1–160. [Google Scholar] [CrossRef]
- Fink, H.A.; Milavetz, D.L.; Palermo, L.; Nevitt, M.C.; Cauley, J.A.; Genant, H.K.; Black, D.M.; Ensrud, K.E. What proportion of incident radiographic vertebral deformities is clinically diagnosed and vice versa? J. Bone Miner. Res. 2005, 20, 1216–1222. [Google Scholar] [CrossRef] [PubMed]
- Delmas, P.D.; van de Langerijt, L.; Watts, N.B.; Eastell, R.; Genant, H.; Grauer, A.; Cahall, D.L. Underdiagnosis of vertebral fractures is a worldwide problem: The IMPACT study. J. Bone Miner. Res. 2005, 20, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Tsai, K.; Twu, S.; Chieng, P.; Yang, R.; Lee, T. Prevalence of vertebral fractures in chinese men and women in urban Taiwanese communities. Calcif. Tissue Int. 1996, 59, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.C.; McGirt, M.J. Vertebral compression fractures: A review of current management and multimodal therapy. J. Multidiscip. Healthc. 2013, 6, 205–214. [Google Scholar] [CrossRef]
- Saito, T.; Sterbenz, J.M.; Malay, S.; Zhong, L.; MacEachern, M.P.; Chung, K.C. Effectiveness of anti-osteoporotic drugs to prevent secondary fragility fractures: Systematic review and meta-analysis. Osteoporos. Int. 2017, 28, 3289–3300. [Google Scholar] [CrossRef]
- Giangregorio, L.; Papaioannou, A.; Cranney, A.; Zytaruk, N.; Adachi, J.D. Fragility fractures and the osteoporosis care gap: An international phenomenon. Semin. Arthritis Rheum. 2006, 35, 293–305. [Google Scholar] [CrossRef]
- Solomon, D.H.; Johnston, S.S.; Boytsov, N.N.; McMorrow, D.; Lane, J.M.; Krohn, K.D. Osteoporosis medication use after hip fracture in U.S. patients between 2002 and 2011. J. Bone Miner. Res. 2014, 29, 1929–1937. [Google Scholar] [CrossRef]
- Malle, O.; Borgstroem, F.; Fahrleitner-Pammer, A.; Svedbom, A.; Dimai, S.V.; Dimai, H.P. Mind the gap: Incidence of osteoporosis treatment after an osteoporotic fracture—results of the Austrian branch of the International Costs and Utilities Related to Osteoporotic Fractures Study (ICUROS). Bone 2021, 142, 115071. [Google Scholar] [CrossRef]
- Greenspan, S.L.; Wyman, A.; Hooven, F.H.; Adami, S.; Gehlbach, S.; Anderson, F.A., Jr.; Boone, S.; Lacroix, A.Z.; Lindsay, R.; Netelenbos, J.C.; et al. Predictors of treatment with osteoporosis medications after recent fragility fractures in a multinational cohort of postmenopausal women. J. Am. Geriatr. Soc. 2012, 60, 455–461. [Google Scholar] [CrossRef] [PubMed]
- Keshishian, A.; Boytsov, N.; Burge, R.; Krohn, K.; Lombard, L.; Zhang, X.; Xie, L.; Baser, O. Examining the treatment gap and risk of subsequent fractures among females with a fragility fracture in the US Medicare population. Osteoporos. Int. 2017, 28, 2485–2494. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Weaver, J.; de Papp, A.; Li, Z.; Martin, J.; Allen, K.; Hui, S.; Imel, E.A. Disparities in osteoporosis treatments. Osteoporos. Int. 2016, 27, 509–519. [Google Scholar] [CrossRef] [PubMed]
- Sattari, M.; Cauley, J.A.; Garvan, C.; Johnson, K.C.; LaMonte, M.J.; Li, W.; Limacher, M.; Manini, T.; Sarto, G.E.; Sullivan, S.D.; et al. Osteoporosis in the Women’s Health Initiative: Another Treatment Gap? Am. J. Med. 2017, 130, 937–948. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.Y.; Fu, S.H.; Huang, C.C.; Hung, C.C.; Yang, R.S.; Hsiao, F.Y. Visualisation of the unmet treatment need of osteoporotic fracture in Taiwan: A nationwide cohort study. Int. J. Clin. Pract. 2018, 72, e13246. [Google Scholar] [CrossRef]
- Yeam, C.T.; Chia, S.; Tan, H.C.C.; Kwan, Y.H.; Fong, W.; Seng, J.J.B. A systematic review of factors affecting medication adherence among patients with osteoporosis. Osteoporos. Int. 2018, 29, 2623–2637. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.S.; Chang, Y.F.; Wang, M.W.; Chen, C.Y.; Chao, Y.J.; Chang, H.J.; Kuo, P.H.; Yang, Y.C.; Wu, C.H. Inverse relationship between central obesity and osteoporosis in osteoporotic drug naive elderly females: The Tianliao Old People (TOP) Study. J. Clin. Densitom. 2013, 16, 204–211. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.F.; Chang, C.S.; Wang, M.W.; Wu, C.F.; Chen, C.Y.; Chang, H.J.; Kuo, P.H.; Wu, C.H. Effects of Age and Body Mass Index on Thoracolumbar Spine X-Ray for Diagnosing Osteoporosis in Elderly Women: Tianliao Old People (TOP) Study 07. PLoS ONE 2016, 11, e0161773. [Google Scholar] [CrossRef]
- Deyo, R.A.; Cherkin, D.C.; Ciol, M.A. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J. Clin. Epidemiol. 1992, 45, 613–619. [Google Scholar] [CrossRef]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef]
- Lu, F.H.; Tang, S.J.; Wu, J.S.; Yang, Y.C.; Chang, C.J. Hypertension in elderly persons: Its prevalence and associated cardiovascular risk factors in Tainan City, southern Taiwan. J. Gerontol. A Biol. Sci. Med. Sci. 2000, 55, M463–M468. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.C.; Lu, F.H.; Wu, J.S.; Wu, C.H.; Chang, C.J. The protective effect of habitual tea consumption on hypertension. Arch. Intern. Med. 2004, 164, 1534–1540. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.Y.; Majeed, A.; Kuo, K.N. An overview of the healthcare system in Taiwan. Lond. J. Prim. Care 2010, 3, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.; Juang, H.; Chang, C.J.; Tsai, H.C.; Chang, K.; Lin, K.K.; Zhao, Z. Persistence and Adherence With Osteoporosis Medication and Re-Fracture In Women With Postmenopausal Osteoporosis In Taiwan. Value Health 2018, 21, S82. [Google Scholar] [CrossRef]
- Position statement: Executive summary. The Writing Group for the International Society for Clinical Densitometry (ISCD) Position Development Conference. J. Clin. Densitom. 2004, 7, 7–12. [CrossRef]
- Genant, H.K.; Wu, C.Y.; van Kuijk, C.; Nevitt, M.C. Vertebral fracture assessment using a semiquantitative technique. J. Bone Miner. Res. 1993, 8, 1137–1148. [Google Scholar] [CrossRef]
- Iconaru, L.; Smeys, C.; Baleanu, F.; Kinnard, V.; Moreau, M.; Cappelle, S.; Surquin, M.; Rubinstein, M.; Rozenberg, S.; Paesmans, M.; et al. Osteoporosis treatment gap in a prospective cohort of volunteer women. Osteoporos. Int. 2020, 31, 1377–1382. [Google Scholar] [CrossRef]
- Lorentzon, M.; Johansson, H.; Harvey, N.C.; Odén, A.; Sanders, K.; Borgström, F.; Svedbom, A.; Mccloskey, E.; Kanis, J. Treatment gap following clinical vertebral fracture in the international cost and utility related to osteoporosis fractures study. J. Bone Miner. Res. 2018, 33, 115. [Google Scholar]
- Cuddihy, M.T.; Gabriel, S.E.; Crowson, C.S.; Atkinson, E.J.; Tabini, C.; O’Fallon, W.M.; Melton, L.J., 3rd. Osteoporosis intervention following distal forearm fractures: A missed opportunity? Arch. Intern. Med. 2002, 162, 421–426. [Google Scholar] [CrossRef]
- Brennan, R.M.; Wactawski-Wende, J.; Crespo, C.J.; Dmochowski, J. Factors associated with treatment initiation after osteoporosis screening. Am. J. Epidemiol. 2004, 160, 475–483. [Google Scholar] [CrossRef][Green Version]
- International Fracture Liaison Service Toolkit. Available online: https://www.osteoporosis.foundation/sites/iofbonehealth/files/2021-01/2014-IOF-CTF-FLS_toolkit_EN_WEB.pdf (accessed on 15 January 2022).
- Falkner, K.L.; Trevisan, M.; McCann, S.E. Reliability of recall of physical activity in the distant past. Am. J. Epidemiol. 1999, 150, 195–205. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Outpatient Visits within 2 Years after Diagnosis | ||
|---|---|---|
| without n = 227 | with n = 166 | |
| Gender, female *** | 49 (21.6) # | 126 (75.9) |
| Age, years * | 74.4 ± 6.3 | 76.0 ± 5.6 |
| Body mass index, kg/m2 | 24.7 ± 3.4 | 24.3 ± 3.4 |
| Previous fracture ** | 36 (16.0) | 45 (27.1) |
| Parent with fractured hip | 9 (4.0) | 9 (5.4) |
| Current smoking *** | 32 (14.1) | 6 (3.6) |
| Current alcohol consumption | 10 (4.4) | 6 (3.6) |
| Current steroid use | 14 (6.2) | 14 (8.4) |
| Current supplement use *** | 63 (27.8) | 76 (45.8) |
| Charlson comorbidity index score | 1.46 ± 1.85 | 1.39 ± 1.59 |
| T-score for bone mineral density *** | −1.46 ± 1.02 | −2.74 ± 1.01 |
| Interval between outpatient visits following diagnosis in months | - | 4.8 ± 4.8 |
| Outpatient Visits within 2 Years after Diagnosis | |
|---|---|
| OR (95% CI) | |
| Gender, female vs. male | 6.66 (3.52–12.60) *** |
| Age, years | 1.03 (0.99–1.08) |
| Body mass index, kg/m2 | 0.97 (0.89–1.05) |
| Previous fracture | 1.80 (0.93–3.46) |
| Parent with fractured hip | 0.99 (0.28–3.42) |
| Current smoking | 1.14 (0.40–3.25) |
| Current alcohol consumption | 2.45 (0.69–8.66) |
| Current steroid use | 0.87 (0.32–2.35) |
| Current supplement use | 2.14 (1.22–3.74) ** |
| Charlson comorbidity index score | 1.09 (0.93–1.27) |
| T-score for bone mineral density | 0.43 (0.31–0.59) *** |
| Initiating Anti-Osteoporotic Medication | ||
|---|---|---|
| without n = 253 | with n = 140 | |
| Gender, female *** | 62 (24.5) # | 113 (80.7) |
| Age, years * | 74.5 ± 6.1 | 76.2 ± 5.7 |
| Body mass index, kg/m2 | 24.7 ± 3.5 | 24.3 ± 3.3 |
| Previous fracture | 45 (17.9) | 36 (25.7) |
| Parent with fractured hip | 13 (5.2) | 5 (3.6) |
| Current smoking *** | 35 (13.8) | 3 (2.1) |
| Current alcohol consumption | 11 (4.4) | 5 (3.6) |
| Current steroid use | 15 (6.0) | 13 (9.3) |
| Current supplement use *** | 74 (29.0) | 65 (46.4) |
| Charlson comorbidity index score | 1.51 ± 1.85 | 1.29 ± 1.52 |
| T-score for bone mineral density *** | −1.49 ± 1.04 | −2.93 ± 0.85 |
| Interval between an outpatient visit following diagnosis, months ** | 9.5 ± 8.0 | 4.0 ± 3.4 |
| Initiating Anti-Osteoporotic Medication | |
|---|---|
| OR (95% CI) | |
| Gender, female vs. male | 0.67 (0.18–2.44) |
| Age, years | 1.08 (0.96–1.20) |
| Body mass index, kg/m2 | 1.03 (0.86–1.22) |
| Previous fracture | 0.65 (0.20–2.09) |
| Current smoking | 0.53 (0.06–4.37) |
| Current supplement use | 1.42 (0.47–4.30) |
| Charlson comorbidity index score | 0.79 (0.59–1.06) |
| T-score of bone mineral density | 0.33 (0.16–0.68) ** |
| Interval between an outpatient visit following diagnosis, months | 0.86 (0.78–0.96) * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, Y.-C.; Chen, C.-Y.; Chang, C.-S.; Li, C.-C.; Wang, R.-H.; Sun, Z.-J.; Wu, C.-H.; Chang, Y.-F. Association between Outpatient Visits and Initiating Medication among Elderly Patients after an Osteoporotic Vertebral Fracture. J. Clin. Med. 2022, 11, 5035. https://doi.org/10.3390/jcm11175035
Wu Y-C, Chen C-Y, Chang C-S, Li C-C, Wang R-H, Sun Z-J, Wu C-H, Chang Y-F. Association between Outpatient Visits and Initiating Medication among Elderly Patients after an Osteoporotic Vertebral Fracture. Journal of Clinical Medicine. 2022; 11(17):5035. https://doi.org/10.3390/jcm11175035
Chicago/Turabian StyleWu, Ya-Chi, Chuan-Yu Chen, Chin-Sung Chang, Chia-Chun Li, Ru-Hsueh Wang, Zih-Jie Sun, Chih-Hsing Wu, and Yin-Fan Chang. 2022. "Association between Outpatient Visits and Initiating Medication among Elderly Patients after an Osteoporotic Vertebral Fracture" Journal of Clinical Medicine 11, no. 17: 5035. https://doi.org/10.3390/jcm11175035
APA StyleWu, Y.-C., Chen, C.-Y., Chang, C.-S., Li, C.-C., Wang, R.-H., Sun, Z.-J., Wu, C.-H., & Chang, Y.-F. (2022). Association between Outpatient Visits and Initiating Medication among Elderly Patients after an Osteoporotic Vertebral Fracture. Journal of Clinical Medicine, 11(17), 5035. https://doi.org/10.3390/jcm11175035