
Correlation of Body Mass Index and Proinflammatory Cytokine Levels with Hematopoietic Stem Cell Mobilization


 , and
, and
Abstract
:1. Introduction
2. Results
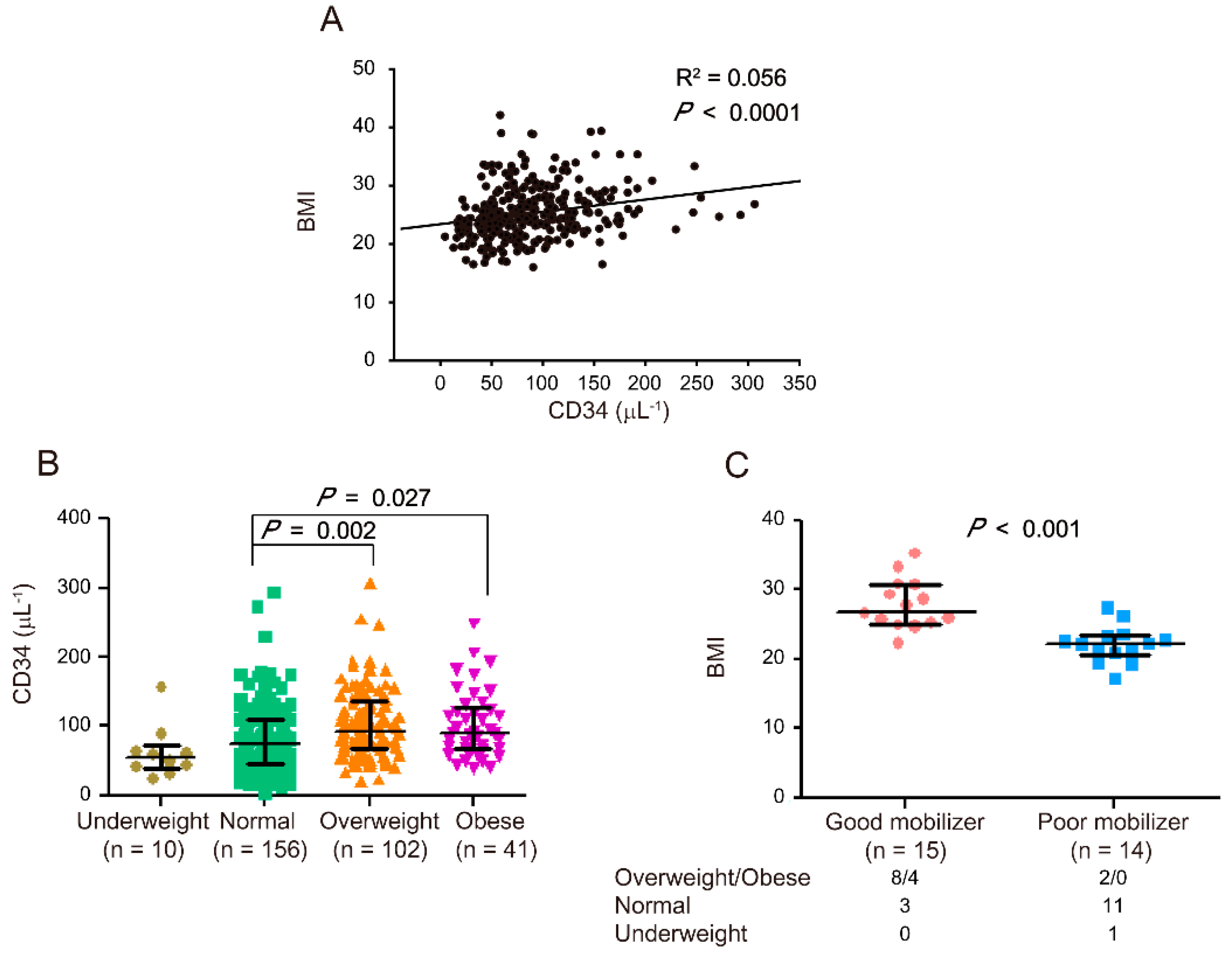
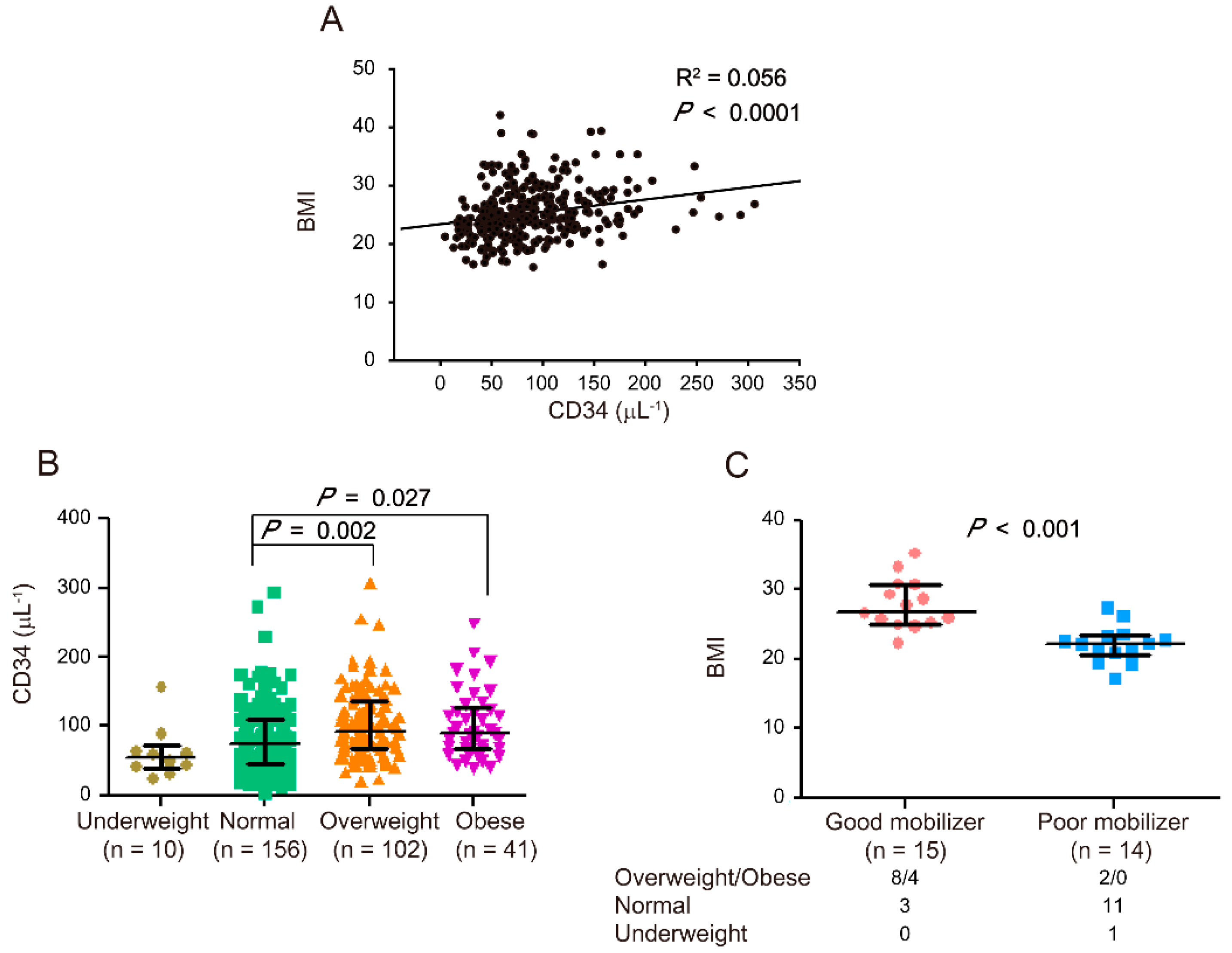
2.1. Correlation of BMI with HSC Mobilization
2.2. Correlation of Proinflammatory Cytokine Levels (IFN-γ, IL-22, and TNF-α) with HSC Mobilization
3. Discussion
4. Materials and Methods
4.1. Stem Cell Donors
4.2. Human Sample and Plasma Collection
4.3. Measurement of Cytokines
4.4. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| HSCT | hematopoietic stem cell transplantation |
| G-CSF | granulocyte colony-stimulating factor |
| HSCs | hematopoietic stem cells |
| BMI | body mass index |
| TNF-α | tumor necrosis factor alpha |
| IL | interleukin |
| IFN-γ | interferon gamma |
References
- Thomas, E.D.; Lochte, H.L., Jr.; Lu, W.C.; Ferrebee, J.W. Intravenous infusion of bone marrow in patients receiving radiation and chemotherapy. N. Engl. J. Med. 1957, 257, 491–496. [Google Scholar] [CrossRef] [PubMed]
- Copelan, E.A. Hematopoietic stem-cell transplantation. N. Engl. J. Med. 2006, 354, 1813–1826. [Google Scholar] [CrossRef]
- Chen, J.; Lazarus, H.M.; Dahi, P.B.; Avecilla, S.; Giralt, S.A. Getting blood out of a stone: Identification and management of patients with poor hematopoietic cell mobilization. Blood Rev. 2021, 47, 100771. [Google Scholar] [CrossRef] [PubMed]
- Gambell, P.; Herbert, K.; Dickinson, M.; Stokes, K.; Bressel, M.; Wall, D.; Harrison, S.; Prince, H.M. Peripheral blood CD34+ cell enumeration as a predictor of apheresis yield: An analysis of more than 1000 collections. Biol. Blood Marrow Transplant. 2012, 18, 763–772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moncada, V.; Bolan, C.; Yau, Y.Y.; Leitman, S.F. Analysis of PBPC cell yields during large-volume leukapheresis of subjects with a poor mobilization response to filgrastim. Transfusion 2003, 43, 495–501. [Google Scholar] [CrossRef]
- Pelus, L.M.; Broxmeyer, H.E. Peripheral blood stem cell mobilization; a look ahead. Curr. Stem Cell Rep. 2018, 4, 273–281. [Google Scholar] [CrossRef]
- Anasetti, C.; Logan, B.R.; Lee, S.J.; Waller, E.K.; Weisdorf, D.J.; Wingard, J.R.; Cutler, C.S.; Westervelt, P.; Woolfrey, A.; Couban, S.; et al. Peripheral-blood stem cells versus bone marrow from unrelated donors. N. Engl. J. Med. 2012, 367, 1487–1496. [Google Scholar] [CrossRef] [Green Version]
- Kollet, O.; Khatib-Massalha, E.; Lapidot, T. The doctor prescribed a fat-free diet for stem cell mobilization. Haematologica 2021, 106, 1512–1513. [Google Scholar] [CrossRef]
- Chang, H.H.; Liou, Y.S.; Sun, D.S. Hematopoietic stem cell mobilization. Tzu Chi Med. J. 2022, 34, 270–275. [Google Scholar]
- Gazitt, Y.; Liu, Q. High steady-state plasma levels of flt3-ligand in the peripheral blood is a good predictor for poor mobilization of CD34+ PBSC in patients undergoing high-dose chemotherapy and stem cell rescue. J. Hematother. Stem Cell Res. 2000, 9, 285–293. [Google Scholar] [CrossRef]
- Gomes, A.L.; Carvalho, T.; Serpa, J.; Torre, C.; Dias, S. Hypercholesterolemia promotes bone marrow cell mobilization by perturbing the SDF-1:CXCR4 axis. Blood 2010, 115, 3886–3894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishihara, T.; Mishima, S.; Kodama, R.; Yoshino, I.; Adachi, E.; Suyama, T.; Shibata, H.; Taketani, T.; Nagai, A. Low-density lipoprotein as a biomarker for the mobilization of hematopoietic stem cells in peripheral blood. Transfus. Apher. Sci. 2013, 49, 539–541. [Google Scholar] [CrossRef] [PubMed]
- Crysandt, M.; Hilgers, R.D.; von Hobe, S.; Eisert, A.; Jost, E.; Panse, J.; Brummendorf, T.H.; Wilop, S. Hypercholesterolemia and its association with enhanced stem cell mobilization and harvest after high-dose cyclophosphamide+G-CSF. Bone Marrow Transplant. 2011, 46, 1426–1429. [Google Scholar] [CrossRef]
- Donmez, A.; Kabaroglu, C.; Arik, B.; Tombuloglu, M. The effect of cholesterol levels on hematopoietic stem cell mobilization. Transfus. Apher. Sci. 2012, 47, 9–12. [Google Scholar] [CrossRef] [PubMed]
- Mishima, S.; Matsuda, C.; Ishihara, T.; Nagase, M.; Taketani, T.; Nagai, A. Single nucleotide polymorphisms of the DGKB and VCAM1 genes are associated with granulocyte colony stimulating factor-mediated peripheral blood stem cell mobilization. Transfus. Apher. Sci. 2017, 56, 154–159. [Google Scholar] [CrossRef]
- Martin-Antonio, B.; Carmona, M.; Falantes, J.; Gil, E.; Baez, A.; Suarez, M.; Marin, P.; Espigado, I.; Urbano-Ispizua, A. Impact of constitutional polymorphisms in VCAM1 and CD44 on CD34+ cell collection yield after administration of granulocyte colony-stimulating factor to healthy donors. Haematologica 2011, 96, 102–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, S.H.; Yang, S.H.; Chu, S.C.; Su, Y.C.; Chang, C.Y.; Chiu, Y.W.; Kao, R.H.; Li, D.K.; Yang, K.L.; Wang, T.F. The role of donor characteristics and post-granulocyte colony-stimulating factor white blood cell counts in predicting the adverse events and yields of stem cell mobilization. Int. J. Hematol. 2011, 93, 652–659. [Google Scholar] [CrossRef]
- Farhadfar, N.; Hsu, J.W.; Logan, B.R.; Sees, J.A.; Chitphakdithai, P.; Sugrue, M.W.; Abdel-Azim, H.; Anderlini, P.N.; Bredeson, C.; Chhabra, S.; et al. Weighty choices: Selecting optimal G-CSF doses for stem cell mobilization to optimize yield. Blood Adv. 2020, 4, 706–716. [Google Scholar] [CrossRef]
- Ings, S.J.; Balsa, C.; Leverett, D.; Mackinnon, S.; Linch, D.C.; Watts, M.J. Peripheral blood stem cell yield in 400 normal donors mobilised with granulocyte colony-stimulating factor (G-CSF): Impact of age, sex, donor weight and type of G-CSF used. Br. J. Haematol. 2006, 134, 517–525. [Google Scholar] [CrossRef]
- Lenk, J.; Bornhauser, M.; Kramer, M.; Holig, K.; Poppe-Thiede, K.; Schmidt, H.; Wiesneth, M.; Schaefer-Eckart, K.; Schlenke, P.; Punzel, M.; et al. Sex and body mass index but not CXCL12 801 G/A polymorphism determine the efficacy of hematopoietic cell mobilization: A study in healthy volunteer donors. Biol. Blood Marrow Transplant. 2013, 19, 1517–1521. [Google Scholar] [CrossRef] [Green Version]
- Ozkurt, Z.N.; Batmaz, L.; Yegin, Z.A.; Ilhan, C. Factors affecting hematopoietic stem cell mobilization and apheresis in allogeneic donors: The role of iron status. Transfus. Apher. Sci. 2017, 56, 470–473. [Google Scholar] [CrossRef] [PubMed]
- Pulsipher, M.A.; Chitphakdithai, P.; Miller, J.P.; Logan, B.R.; King, R.J.; Rizzo, J.D.; Leitman, S.F.; Anderlini, P.; Haagenson, M.D.; Kurian, S.; et al. Adverse events among 2408 unrelated donors of peripheral blood stem cells: Results of a prospective trial from the National Marrow Donor Program. Blood 2009, 113, 3604–3611. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.F.; Wen, S.H.; Chen, R.L.; Lu, C.J.; Zheng, Y.J.; Yang, S.H.; Chu, S.C.; Kao, R.H.; Chen, S.H. Factors associated with peripheral blood stem cell yield in volunteer donors mobilized with granulocyte colony-stimulating factors: The impact of donor characteristics and procedural settings. Biol. Blood Marrow Transplant. 2008, 14, 1305–1311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tam, C.S.; Clement, K.; Baur, L.A.; Tordjman, J. Obesity and low-grade inflammation: A paediatric perspective. Obes. Rev. 2010, 11, 118–126. [Google Scholar] [CrossRef]
- Mraz, M.; Haluzik, M. The role of adipose tissue immune cells in obesity and low-grade inflammation. J. Endocrinol. 2014, 222, R113–R127. [Google Scholar] [CrossRef] [Green Version]
- Catrysse, L.; van Loo, G. Inflammation and the Metabolic Syndrome: The Tissue-Specific Functions of NF-kappaB. Trends Cell Biol. 2017, 27, 417–429. [Google Scholar] [CrossRef]
- Shivappa, N.; Hebert, J.R.; Marcos, A.; Diaz, L.E.; Gomez, S.; Nova, E.; Michels, N.; Arouca, A.; Gonzalez-Gil, E.; Frederic, G.; et al. Association between dietary inflammatory index and inflammatory markers in the HELENA study. Mol. Nutr. Food Res. 2017, 61, 1600707. [Google Scholar] [CrossRef]
- Peters, U.; Suratt, B.T.; Bates, J.H.T.; Dixon, A.E. Beyond BMI: Obesity and Lung Disease. Chest 2018, 153, 702–709. [Google Scholar] [CrossRef]
- Azzouqa, A.M.; Jouni, K.; Roy, V.; Zubair, A.C. Impact of good and poor mobilizers on hematopoietic progenitor cell collection efficiency and product quality. J. Clin. Apher. 2019, 34, 39–43. [Google Scholar] [CrossRef] [Green Version]
- van Gorkom, G.; Finel, H.; Giebel, S.; Pohlreich, D.; Shimoni, A.; Ringhoffer, M.; Sucak, G.; Schaap, N.; Dreger, P.; Sureda, A.; et al. Prospective noninterventional study on peripheral blood stem cell mobilization in patients with relapsed lymphomas. J. Clin. Apher. 2017, 32, 295–301. [Google Scholar] [CrossRef]
- Spoerl, S.; Peter, R.; Wascher, D.; Gotze, K.; Verbeek, M.; Peschel, C.; Krackhardt, A.M. Patients’ outcome after rescue plerixafor administration for autologous stem cell mobilization: A single-center retrospective analysis. Transfusion 2017, 57, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Moretta, F.; Petronelli, F.; Lucarelli, B.; Pitisci, A.; Bertaina, A.; Locatelli, F.; Mingari, M.C.; Moretta, L.; Montaldo, E. The generation of human innate lymphoid cells is influenced by the source of hematopoietic stem cells and by the use of G-CSF. Eur. J. Immunol. 2016, 46, 1271–1278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gattillo, S.; Marktel, S.; Rizzo, L.; Malato, S.; Malabarba, L.; Coppola, M.; Assanelli, A.; Milani, R.; De Freitas, T.; Corti, C.; et al. Plerixafor on demand in ten healthy family donors as a rescue strategy to achieve an adequate graft for stem cell transplantation. Transfusion 2015, 55, 1993–2000. [Google Scholar] [CrossRef] [PubMed]
- Wood, W.A.; Whitley, J.; Goyal, R.; Brown, P.M.; Sharf, A.; Irons, R.; Rao, K.V.; Essenmacher, A.; Serody, J.S.; Coghill, J.M.; et al. Effectiveness of etoposide chemomobilization in lymphoma patients undergoing auto-SCT. Bone Marrow Transplant. 2013, 48, 771–776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andreola, G.; Vanazzi, A.; Radice, D.; Babic, A.; Rabascio, C.; Negri, M.; Martinelli, G.; Laszlo, D. Who should be really considered as a poor mobilizer in the plerixafor era? Transfus. Apher. Sci. 2012, 47, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Ivanovic, Z.; Kovacevic-Filipovic, M.; Jeanne, M.; Ardilouze, L.; Bertot, A.; Szyporta, M.; Hermitte, F.; Lafarge, X.; Duchez, P.; Vlaski, M.; et al. CD34+ cells obtained from “good mobilizers” are more activated and exhibit lower ex vivo expansion efficiency than their counterparts from “poor mobilizers”. Transfusion 2010, 50, 120–127. [Google Scholar] [CrossRef]
- Wang, T.F.; Chen, S.H.; Yang, S.H.; Su, Y.C.; Chu, S.C.; Li, D.K. Poor harvest of peripheral blood stem cell in donors with microcytic red blood cells. Transfusion 2013, 53, 91–95. [Google Scholar] [CrossRef]
- Furst, D.; Hauber, D.; Reinhardt, P.; Schauwecker, P.; Bunjes, D.; Schulz, A.; Mytilineos, J.; Wiesneth, M.; Schrezenmeier, H.; Korper, S. Gender, cholinesterase, platelet count and red cell count are main predictors of peripheral blood stem cell mobilization in healthy donors. Vox Sang. 2019, 114, 275–282. [Google Scholar] [CrossRef]
- Khouri, J.; Rybicki, L.; Majhail, N.S.; Kalaycio, M.; Pohlman, B.; Hill, B.; Jagadeesh, D.; Dean, R.; Hamilton, B.; Sobecks, R.; et al. Body mass index does not impact hematopoietic progenitor cell mobilization for autologous hematopoietic cell transplantation. J. Clin. Apher. 2019, 34, 638–645. [Google Scholar] [CrossRef]
- Suzuya, H.; Watanabe, T.; Nakagawa, R.; Watanabe, H.; Okamoto, Y.; Onishi, T.; Abe, T.; Kawano, Y.; Kagami, S.; Takaue, Y. Factors associated with granulocyte colony-stimulating factor-induced peripheral blood stem cell yield in healthy donors. Vox Sang. 2005, 89, 229–235. [Google Scholar] [CrossRef]
- Helfer, G.; Wu, Q.F. Chemerin: A multifaceted adipokine involved in metabolic disorders. J. Endocrinol. 2018, 238, R79–R94. [Google Scholar] [CrossRef] [PubMed]
- Ambrosio, G.; Kaufmann, F.N.; Manosso, L.; Platt, N.; Ghisleni, G.; Rodrigues, A.L.S.; Rieger, D.K.; Kaster, M.P. Depression and peripheral inflammatory profile of patients with obesity. Psychoneuroendocrinology 2018, 91, 132–141. [Google Scholar] [CrossRef] [PubMed]
- Weisberg, S.P.; McCann, D.; Desai, M.; Rosenbaum, M.; Leibel, R.L.; Ferrante, A.W., Jr. Obesity is associated with macrophage accumulation in adipose tissue. J. Clin. Investig. 2003, 112, 1796–1808. [Google Scholar] [CrossRef] [PubMed]
- Yudkin, J.S.; Stehouwer, C.D.; Emeis, J.J.; Coppack, S.W. C-reactive protein in healthy subjects: Associations with obesity, insulin resistance, and endothelial dysfunction: A potential role for cytokines originating from adipose tissue? Arterioscler. Thromb. Vasc. Biol. 1999, 19, 972–978. [Google Scholar] [CrossRef] [Green Version]
- Jahandideh, B.; Derakhshani, M.; Abbaszadeh, H.; Akbar Movassaghpour, A.; Mehdizadeh, A.; Talebi, M.; Yousefi, M. The pro-Inflammatory cytokines effects on mobilization, self-renewal and differentiation of hematopoietic stem cells. Hum. Immunol. 2020, 81, 206–217. [Google Scholar] [CrossRef]
- Samuel, C.E. Antiviral actions of interferons. Clin. Microbiol. Rev. 2001, 14, 778–809. [Google Scholar] [CrossRef] [Green Version]
- Zhao, X.; Ren, G.; Liang, L.; Ai, P.Z.; Zheng, B.; Tischfield, J.A.; Shi, Y.; Shao, C. Brief report: Interferon-gamma induces expansion of Lin(−)Sca-1(+)C-Kit(+) Cells. Stem Cells 2010, 28, 122–126. [Google Scholar] [CrossRef]
- Brugger, W.; Mocklin, W.; Heimfeld, S.; Berenson, R.J.; Mertelsmann, R.; Kanz, L. Ex vivo expansion of enriched peripheral blood CD34+ progenitor cells by stem cell factor, interleukin-1 beta (IL-1 beta), IL-6, IL-3, interferon-gamma, and erythropoietin. Blood 1993, 81, 2579–2584. [Google Scholar] [CrossRef] [Green Version]
- Baldridge, M.T.; King, K.Y.; Boles, N.C.; Weksberg, D.C.; Goodell, M.A. Quiescent haematopoietic stem cells are activated by IFN-gamma in response to chronic infection. Nature 2010, 465, 793–797. [Google Scholar] [CrossRef]
- Baldridge, M.T.; King, K.Y.; Goodell, M.A. Inflammatory signals regulate hematopoietic stem cells. Trends Immunol. 2011, 32, 57–65. [Google Scholar] [CrossRef] [Green Version]
- Rezzoug, F.; Huang, Y.; Tanner, M.K.; Wysoczynski, M.; Schanie, C.L.; Chilton, P.M.; Ratajczak, M.Z.; Fugier-Vivier, I.J.; Ildstad, S.T. TNF-alpha is critical to facilitate hemopoietic stem cell engraftment and function. J. Immunol. 2008, 180, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Sharma, B.; Altman, J.K.; Goussetis, D.J.; Verma, A.K.; Platanias, L.C. Protein kinase R as mediator of the effects of interferon (IFN) gamma and tumor necrosis factor (TNF) alpha on normal and dysplastic hematopoiesis. J. Biol. Chem. 2011, 286, 27506–27514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitagawa, M.; Saito, I.; Kuwata, T.; Yoshida, S.; Yamaguchi, S.; Takahashi, M.; Tanizawa, T.; Kamiyama, R.; Hirokawa, K. Overexpression of tumor necrosis factor (TNF)-alpha and interferon (IFN)-gamma by bone marrow cells from patients with myelodysplastic syndromes. Leukemia 1997, 11, 2049–2054. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopez-Garcia, L.; Castro-Manrreza, M.E. TNF-alpha and IFN-gamma Participate in Improving the Immunoregulatory Capacity of Mesenchymal Stem/Stromal Cells: Importance of Cell-Cell Contact and Extracellular Vesicles. Int. J. Mol. Sci. 2021, 22, 9531. [Google Scholar] [CrossRef]
- Hemeda, H.; Jakob, M.; Ludwig, A.K.; Giebel, B.; Lang, S.; Brandau, S. Interferon-gamma and tumor necrosis factor-alpha differentially affect cytokine expression and migration properties of mesenchymal stem cells. Stem Cells Dev. 2010, 19, 693–706. [Google Scholar] [CrossRef]
- Keir, M.; Yi, Y.; Lu, T.; Ghilardi, N. The role of IL-22 in intestinal health and disease. J. Exp. Med. 2020, 217, e20192195. [Google Scholar] [CrossRef]
- Dudakov, J.A.; Hanash, A.M.; van den Brink, M.R. Interleukin-22: Immunobiology and pathology. Annu. Rev. Immunol. 2015, 33, 747–785. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, T.; Ishii, S.; Shinohara, M.; Kawano, Y.; Wakahashi, K.; Kawano, H.; Sada, A.; Minagawa, K.; Hamada, M.; Takahashi, S.; et al. Mobilization efficiency is critically regulated by fat via marrow PPARdelta. Haematologica 2021, 106, 1671–1683. [Google Scholar] [CrossRef]
- D’Angelo, S.; Motti, M.L.; Meccariello, R. omega-3 and omega-6 Polyunsaturated Fatty Acids, Obesity and Cancer. Nutrients 2020, 12, 2751. [Google Scholar] [CrossRef]
- Cholewski, M.; Tomczykowa, M.; Tomczyk, M. A Comprehensive Review of Chemistry, Sources and Bioavailability of Omega-3 Fatty Acids. Nutrients 2018, 10, 1662. [Google Scholar] [CrossRef] [Green Version]
- Siriwardhana, N.; Kalupahana, N.S.; Cekanova, M.; LeMieux, M.; Greer, B.; Moustaid-Moussa, N. Modulation of adipose tissue inflammation by bioactive food compounds. J. Nutr. Biochem. 2013, 24, 613–623. [Google Scholar] [CrossRef]
- Kalupahana, N.S.; Claycombe, K.J.; Moustaid-Moussa, N. (n-3) Fatty acids alleviate adipose tissue inflammation and insulin resistance: Mechanistic insights. Adv. Nutr. 2011, 2, 304–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arimura, K.; Inoue, H.; Kukita, T.; Matsushita, K.; Akimot, M.; Kawamata, N.; Yamaguchi, A.; Kawada, H.; Ozak, A.; Arima, N.; et al. Acute lung Injury in a healthy donor during mobilization of peripheral blood stem cells using granulocyte-colony stimulating factor alone. Haematologica 2005, 90, ECR10. [Google Scholar] [PubMed]
- de Azevedo, A.M.; Goldberg Tabak, D. Life-threatening capillary leak syndrome after G-CSF mobilization and collection of peripheral blood progenitor cells for allogeneic transplantation. Bone Marrow Transplant. 2001, 28, 311–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
| Characteristic | Range | Number |
|---|---|---|
| * Age | 34.3 ± 7.7 | |
| Gender | ||
| Female | 106 | |
| Male | 203 | |
| * Body mass index (BMI) (kg/m2) | 24.7 (22.5, 27.8) | |
| BMI < 18.5 | 10 | |
| 18.5 ≤ BMI < 25 | 156 | |
| 25 ≤ BMI < 30 | 102 | |
| BMI ≥ 30 | 41 | |
| * CD34+ cell count (µL−1) | 80.4 (53.3, 120.3) | |
| CD34+ ≤ 25 | 14 | |
| 25 < CD34+ < 180 | 280 | |
| CD34+ ≥ 180 | 15 |
| Crude | Adjusted | |||
|---|---|---|---|---|
| β (95% CI) | p-Value | β (95% CI) | p-Value | |
| Age | 0.16 (−0.57, 0.89) | 0.670 | −0.10 (−0.80, 0.61) | 0.790 |
| Gender | 28.39 (17.00, 39.78) | <0.001 * | 26.25 (14.85, 37.65) | <0.001 * |
| (Male vs. Female) | ||||
| BMI group | - | - | - | - |
| Normal | Ref. | Ref. | Ref. | Ref. |
| Underweight | −17.94 (−49.32, 13.44) | 0.261 | −15.52 (−45.89, 14.85) | 0.315 |
| Overweight | 21.63 (9.38, 33.88) | 0.001 * | 16.99 (4.88, 29.11) | 0.006 * |
| Obese | 22.55 (5.67, 39.43) | 0.009 * | 18.13 (1.62, 34.65) | 0.032 * |
| BMI | IFN-γ | IL-22 | TNF-α | |||||
|---|---|---|---|---|---|---|---|---|
| β (95% CI) | p-Value | β (95% CI) | p-Value | β (95% CI) | p-Value | β (95% CI) | p-Value | |
| Age | 0.18 (0.02, 0.34) | 0.026 * | −0.20 (−0.96, 0.56) | 0.589 | −0.38 (−18.11, 17.36) | 0.965 | −0.24 (−1.11, 0.63) | 0.573 |
| Gender (Male vs. Female) | 0.15 (−2.62, 2.92) | 0.914 | −4.47 (−17.86, 8.92) | 0.497 | −252.47 (−564.45, 59.51) | 0.108 | −16.04 (−31.35, −0.74) | 0.041 * |
| Group (Good vs. Poor) | 5.42 (2.71, 8.14) | <0.001 * | 15.9 (2.76, 29.03) | 0.020 * | 462.07 (155.92, 768.22) | 0.005 * | 24.97 (9.95, 39.99) | 0.002 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, T.-F.; Liou, Y.-S.; Chang, H.-H.; Yang, S.-H.; Li, C.-C.; Wang, J.-H.; Sun, D.-S. Correlation of Body Mass Index and Proinflammatory Cytokine Levels with Hematopoietic Stem Cell Mobilization. J. Clin. Med. 2022, 11, 4169. https://doi.org/10.3390/jcm11144169
Wang T-F, Liou Y-S, Chang H-H, Yang S-H, Li C-C, Wang J-H, Sun D-S. Correlation of Body Mass Index and Proinflammatory Cytokine Levels with Hematopoietic Stem Cell Mobilization. Journal of Clinical Medicine. 2022; 11(14):4169. https://doi.org/10.3390/jcm11144169
Chicago/Turabian StyleWang, Tso-Fu, Yu-Shan Liou, Hsin-Hou Chang, Shang-Hsien Yang, Chi-Cheng Li, Jen-Hung Wang, and Der-Shan Sun. 2022. "Correlation of Body Mass Index and Proinflammatory Cytokine Levels with Hematopoietic Stem Cell Mobilization" Journal of Clinical Medicine 11, no. 14: 4169. https://doi.org/10.3390/jcm11144169
APA StyleWang, T.-F., Liou, Y.-S., Chang, H.-H., Yang, S.-H., Li, C.-C., Wang, J.-H., & Sun, D.-S. (2022). Correlation of Body Mass Index and Proinflammatory Cytokine Levels with Hematopoietic Stem Cell Mobilization. Journal of Clinical Medicine, 11(14), 4169. https://doi.org/10.3390/jcm11144169