
Greater Muscular Strength Is Associated with a Lower Risk of Pulmonary Dysfunction in Individuals with Non-Alcoholic Fatty Liver Disease


Abstract
:1. Introduction
2. Materials and Methods
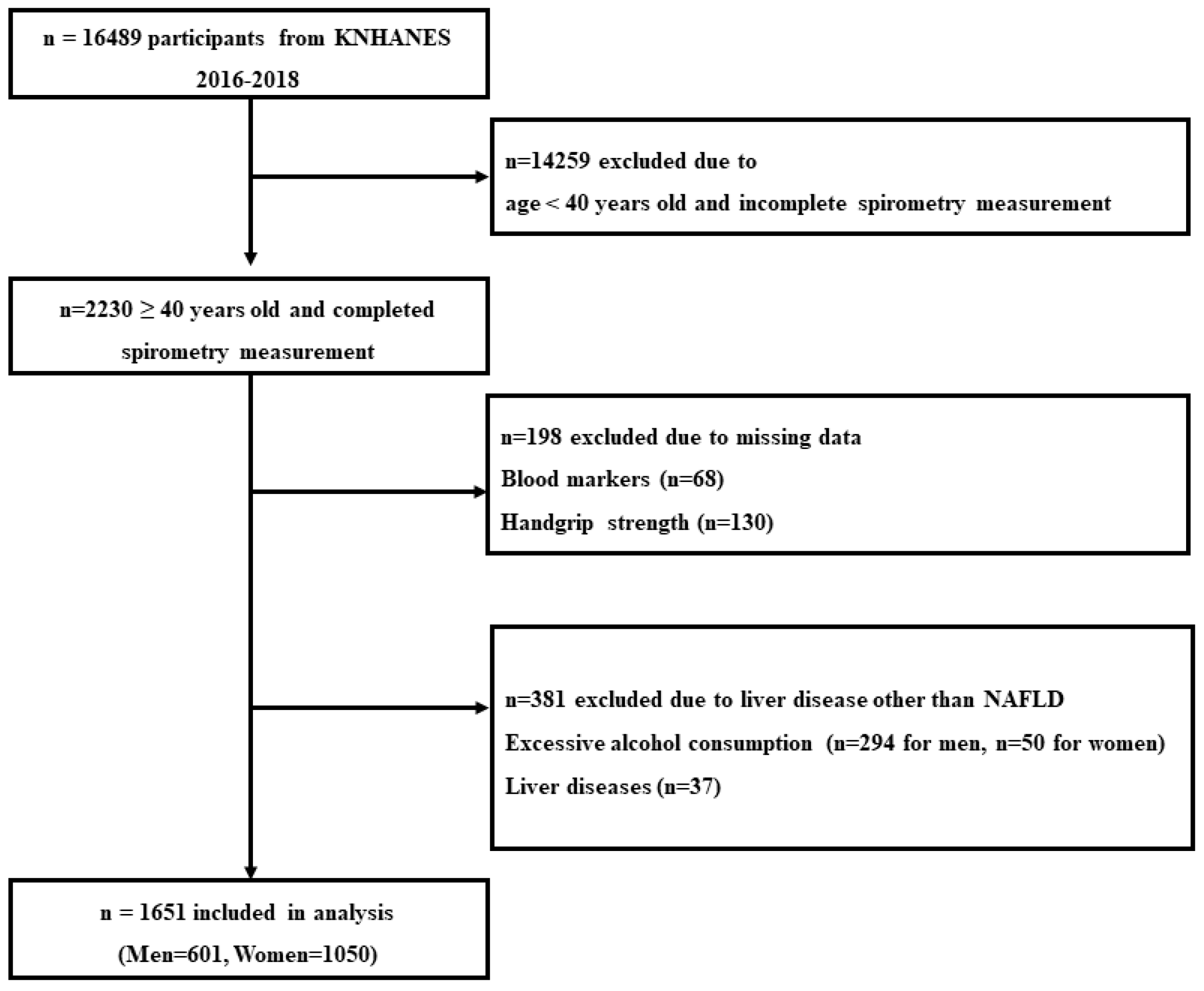
2.1. Study Participants
2.2. Covariates
2.3. Pulmonary Function Measurements
2.4. Definition of NAFLD
2.5. Relative Handgrip Strength
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Han, M.A.T.; Yu, Q.; Tafesh, Z.; Pyrsopoulos, N. Diversity in NAFLD: A Review of Manifestations of Nonalcoholic Fatty Liver Disease in Different Ethnicities Globally. J. Clin. Transl. Hepatol. 2021, 9, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease—Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitra, S.; De, A.; Chowdhury, A. Epidemiology of non-alcoholic and alcoholic fatty liver diseases. Transl. Gastroenterol. Hepatol. 2020, 5, 16. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zhong, G.-C.; Tan, H.-Y.; Hao, F.-B.; Hu, J.-J. Nonalcoholic fatty liver disease and mortality from all causes, cardiovascular disease, and cancer: A meta-analysis. Sci. Rep. 2019, 9, 11124. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.; Gong, X.; Li, X.; Shao, C.; Wu, T.; Li, M.; Li, F.; Ma, Q.; Ye, J.; Zhong, B. Distinct Cause of Death Profiles of Hospitalized Non-alcoholic Fatty Liver Disease: A 10 Years’ Cross-Sectional Multicenter Study in China. Front. Med. 2021, 7, 584396. [Google Scholar] [CrossRef]
- Botello-Manilla, A.E.; López-Sánchez, G.N.; Chávez-Tapia, N.C.; Uribe, M.; Nuño-Lámbarri, N. Hepatic steatosis and respiratory diseases: A new panorama. Ann. Hepatol. 2021, 24, 100320. [Google Scholar] [CrossRef]
- Paik, J.M.; Henry, L.; De Avila, L.; Younossi, E.; Racila, A.; Younossi, Z.M. Mortality Related to Nonalcoholic Fatty Liver Disease Is Increasing in the United States. Hepatol. Commun. 2019, 3, 1459–1471. [Google Scholar] [CrossRef] [Green Version]
- Jung, D.-H.; Shim, J.-Y.; Lee, H.-R.; Moon, B.-S.; Park, B.-J.; Lee, Y.-J. Relationship between non-alcoholic fatty liver disease and pulmonary function. Intern. Med. J. 2012, 42, 541–546. [Google Scholar] [CrossRef]
- Peng, T.-C.; Kao, T.-W.; Wu, L.-W.; Chen, Y.-J.; Chang, Y.-W.; Wang, C.-C.; Tsao, Y.-T.; Chen, W.-L. Association Between Pulmonary Function and Nonalcoholic Fatty Liver Disease in the NHANES III Study. Medicine 2015, 94, e907. [Google Scholar] [CrossRef]
- Ioachimescu, O.C.; Mehta, A.C.; Stoller, J.K. Hepatopulmonary syndrome following portopulmonary hypertension. Eur. Respir. J. 2007, 29, 1277–1280. [Google Scholar] [CrossRef]
- Fukumori, N.; Yamamoto, Y.; Takegami, M.; Yamazaki, S.; Onishi, Y.; Sekiguchi, M.; Otani, K.; Konno, S.-I.; Kikuchi, S.-I.; Fukuhara, S. Association between hand-grip strength and depressive symptoms: Locomotive Syndrome and Health Outcomes in Aizu Cohort Study (LOHAS). Age Ageing 2015, 44, 592–598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volaklis, K.; Mamadjanov, T.; Meisinger, C.; Linseisen, J. Association between muscular strength and depressive symptoms. Wien. Klin. Wochenschr. 2019, 131, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Cheung, C.-L.; Nguyen, U.-S.; Au, E.; Tan, K.C.B.; Kung, A.W.C. Association of handgrip strength with chronic diseases and multimorbidity. Age 2013, 35, 929–941. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trosclair, D.; Bellar, D.; Judge, L.W.; Smith, J.; Mazerat, N.; Brignac, A. Hand-Grip Strength as a Predictor of Muscular Strength and Endurance. J. Strength Cond. Res. 2011, 25, S99. [Google Scholar] [CrossRef]
- Akınoğlu, B.; Kocahan, T.; Özkan, T. The relationship between peripheral muscle strength and respiratory function and respiratory muscle strength in athletes. J. Exerc. Rehabil. 2019, 15, 44–49. [Google Scholar] [CrossRef] [Green Version]
- Bahat, G.; Tufan, A.; Ozkaya, H.; Tufan, F.; Akpinar, T.S.; Akin, S.; Bahat, Z.; Kaya, Z.; Kiyan, E.; Erten, N.; et al. Relation between hand grip strength, respiratory muscle strength and spirometric measures in male nursing home residents. Aging Male 2014, 17, 136–140. [Google Scholar] [CrossRef]
- Chen, L.; Liu, X.; Wang, Q.; Jia, L.; Song, K.; Nie, S.; Zhang, Y.; Cao, D.; Zhao, D.; Li, Z.; et al. Better pulmonary function is associated with greater handgrip strength in a healthy Chinese Han population. BMC Pulm. Med. 2020, 20, 114. [Google Scholar] [CrossRef]
- Kweon, S.; Kim, Y.; Jang, M.-J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.-H.; Oh, K. Data resource profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization Western Pacific Region. International Association for the Study of obesity and international obesity task force. In The Asia-Pacific Perspective: Redefining Obesity and Its Treatment; Health Communications Australia Pty Limited: Sydney, Australia, 2000. [Google Scholar]
- Jamal, A.; Phillips, E.; Gentzke, A.S.; Homa, D.M.; Babb, S.D.; King, B.A.; Neff, L.J. Current cigarette smoking among adults—United States, 2016. Morb. Mortal Wkly. Rep. 2018, 67, 53–59. [Google Scholar] [CrossRef] [Green Version]
- Rantakömi, S.H.; Kurl, S.; Sivenius, J.; Kauhanen, J.; Laukkanen, J.A. The frequency of alcohol consumption is associated with the stroke mortality. Acta Neurol. Scand. 2014, 130, 118–124. [Google Scholar] [CrossRef]
- Mancia, G.; Fagard, R.; Narkiewicz, K.; Redán, J.; Zanchetti, A.; Böhm, M.; Christiaens, T.; Cifkova, R.; De Backer, G.; Dominiczak, A. 2013 Practice guidelines for the management of arterial hypertension of the European Society of Hypertension (ESH) and the European Society of Cardiology (ESC): ESH/ESC Task Force for the Management of Arterial Hypertension. J. Hypertens. 2013, 31, 1925–1938. [Google Scholar] [CrossRef] [Green Version]
- International Diabetes Federation Guideline Development Group. Global guideline for type 2 diabetes. Diabetes Res. Clin. Pract. 2014, 104, 1–52. [Google Scholar] [CrossRef] [PubMed]
- American Thoracic Society. Standardization of spirometry. Am. J. Respir. Crit. Care Med. 1995, 152, 1107–1136. [Google Scholar]
- Choi, J.K.; Paek, D.; Lee, J.O. Normal Predictive Values of Spirometry in Korean Population. Tuberc. Respir. Dis. 2005, 58, 230–242. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.-H.; Jung, K.S.; Kim, S.U.; Yoon, H.-J.; Yun, Y.J.; Lee, B.-W.; Kang, E.S.; Han, K.-H.; Lee, H.C.; Cha, B.-S. Sarcopaenia is associated with NAFLD independently of obesity and insulin resistance: Nationwide surveys (KNHANES 2008–2011). J. Hepatol. 2015, 63, 486–493. [Google Scholar] [CrossRef] [PubMed]
- Fedchuk, L.; Nascimbeni, F.; Pais, R.; Charlotte, F.; Housset, C.; Ratziu, V.; The Lido Study Group. Performance and limitations of steatosis biomarkers in patients with nonalcoholic fatty liver disease. Aliment. Pharmacol. Ther. 2014, 40, 1209–1222. [Google Scholar] [CrossRef]
- Lischka, J.; Schanzer, A.; Hojreh, A.; Ba Ssalamah, A.; Item, C.B.; de Gier, C.; Walleczek, N.-K.; Metz, T.F.; Jakober, I.; Greber-Platzer, S.; et al. A branched-chain amino acid-based metabolic score can predict liver fat in children and adolescents with severe obesity. Pediatric Obes. 2021, 16, e12739. [Google Scholar] [CrossRef]
- Scicali, R.; Di Pino, A.; Urbano, F.; Ferrara, V.; Marchisello, S.; Di Mauro, S.; Scamporrino, A.; Filippello, A.; Rabuazzo, A.M.; Purrello, F.; et al. Analysis of steatosis biomarkers and inflammatory profile after adding on PCSK9 inhibitor treatment in familial hypercholesterolemia subjects with nonalcoholic fatty liver disease: A single lipid center real-world experience. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 869–879. [Google Scholar] [CrossRef]
- Mantovani, A.; Sani, E.; Fassio, A.; Colecchia, A.; Viapiana, O.; Gatti, D.; Idolazzi, L.; Rossini, M.; Salvagno, G.; Lippi, G.; et al. Association between non-alcoholic fatty liver disease and bone turnover biomarkers in post-menopausal women with type 2 diabetes. Diabetes Metab. 2019, 45, 347–355. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.W.; Lee, D.H.; Lee, J.-K.; Lee, S.; Koo, B.K.; Joo, S.K.; Heo, E.Y.; Jung, Y.J.; Kim, W.; Kim, D.K. Pulmonary function is associated with fibrosis severity in patients with biopsy-proven nonalcoholic fatty liver disease. Liver Int. 2020, 40, 3008–3017. [Google Scholar] [CrossRef]
- Song, J.-U.; Jang, Y.; Lim, S.-Y.; Ryu, S.; Song, W.J.; Byrne, C.D.; Sung, K.-C. Decreased lung function is associated with risk of developing non-alcoholic fatty liver disease: A longitudinal cohort study. PLoS ONE 2019, 14, e0208736. [Google Scholar] [CrossRef]
- El Amrousy, D.; El Ashry, H.; Maher, S.; Ganna, S.; Hasan, S. Pulmonary function test abnormalities in children and adolescents with non-alcoholic fatty liver disease. Eur. J. Pediatr. 2021, 180, 1693–1699. [Google Scholar] [CrossRef] [PubMed]
- Fallon, M.B.; Abrams, G.A.; Luo, B.; Hou, Z.; Dai, J.; Ku, D.D. The role of endothelial nitric oxide synthase in the pathogenesis of a rat model of hepatopulmonary syndrome. Gastroenterology 1997, 113, 606–614. [Google Scholar] [CrossRef]
- Maruyama, T.; Ohsaki, K.; Shimoda, S.; Kaji, Y.; Harada, M. Thromboxane-dependent portopulmonary hypertension. Am. J. Med. 2005, 118, 93–94. [Google Scholar] [CrossRef] [PubMed]
- Tsiakalos, A.; Hatzis, G.; Moyssakis, I.; Karatzaferis, A.; Ziakas, P.; Tzelepis, G.E. Portopulmonary hypertension and serum endothelin levels in hospitalized patients with cirrhosis. Hepatobiliary Pancreat. Dis. Int. 2011, 10, 393–398. [Google Scholar] [CrossRef]
- Rossi, A.; Fantin, F.; Di Francesco, V.; Guariento, S.; Giuliano, K.; Fontana, G.; Micciolo, R.; Solerte, S.B.; Bosello, O.; Zamboni, M. Body composition and pulmonary function in the elderly: A 7-year longitudinal study. Int. J. Obes. 2008, 32, 1423–1430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, C.-H.; Yi, Y.; Do, J.G.; Lee, Y.-T.; Yoon, K.J. Relationship between skeletal muscle mass and lung function in Korean adults without clinically apparent lung disease. Medicine 2018, 97, e12281. [Google Scholar] [CrossRef]
- Wright, P.; Heck, H.; Langenkamp, H. Effects of a resistance training on pulmonary function and performance measurements in patients with chronic obstructive pulmonary disease. Eur. J. Sport Sci. 2003, 3, 1–10. [Google Scholar] [CrossRef]
- Hoff, J.; Tjønna, A.E.; Steinshamn, S.; Høydal, M.; Richardson, R.S.; Helgerud, J. Maximal strength training of the legs in COPD: A therapy for mechanical inefficiency. Med. Sci. Sports Exerc. 2007, 39, 220–226. [Google Scholar] [CrossRef] [Green Version]
- Black, L.E.; Swan, P.D.; Alvar, B.A. Effects of Intensity and Volume on Insulin Sensitivity During Acute Bouts of Resistance Training. J. Strength Cond. Res. 2010, 24, 1109–1116. [Google Scholar] [CrossRef]
- Botezelli, J.D.; Coope, A.; Ghezzi, A.C.; Cambri, L.T.; Moura, L.P.; Scariot, P.P.; Gaspar, R.S.; Mekary, R.A.; Ropelle, E.R.; Pauli, J.R. Strength training prevents hyperinsulinemia, insulin resistance, and inflammation independent of weight loss in fructose-fed animals. Sci. Rep. 2016, 6, 31106. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.-H.; Choi, S.H.; Chung, G.E.; Park, B.; Kwak, M.-S. Nonalcoholic fatty liver disease is associated with decreased lung function. Liver Int. 2018, 38, 2091–2100. [Google Scholar] [CrossRef]
- Lee, J.-H.; Kim, D.; Kim, H.J.; Lee, C.-H.; Yang, J.I.; Kim, W.; Kim, Y.J.; Yoon, J.-H.; Cho, S.-H.; Sung, M.-W.; et al. Hepatic steatosis index: A simple screening tool reflecting nonalcoholic fatty liver disease. Dig. Liver Dis. 2010, 42, 503–508. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Total (n = 1651) | Normal (n = 1230) | NAFLD (n = 421) | p-Value |
|---|---|---|---|---|
| Anthropometrics | ||||
| Age (years) | 58.2 ± 11.4 | 58.0 ± 11.4 | 58.7 ± 11.5 | 0.244 |
| Male, n (%) | 601 (36.4) | 451 (36.7) | 150 (35.6) | 0.725 |
| BMI (kg/m2) | 24.2 ± 3.3 | 22.9 ± 2.3 | 28.0 ± 2.9 | <0.001 |
| Relative HGS (kg/BMI) | 1.25 ± 0.41 | 1.30 ± 0.40 | 1.10 ± 0.37 | <0.001 |
| Blood Markers | ||||
| AST (U/L) | 22.8 ± 10.2 | 21.5 ± 9.1 | 26.5 ± 12.3 | <0.001 |
| ALT (U/L) | 22.0 ± 15.3 | 18.2 ± 10.8 | 33.2 ± 20.3 | <0.001 |
| FBG (mg/dL) | 103.8 ± 26.1 | 99.0 ± 17.7 | 117.7 ± 38.8 | <0.001 |
| TC (mg/dL) | 195.6 ± 39.1 | 196.9 ± 37.3 | 191.6 ± 43.9 | 0.015 |
| HDL-C (mg/dL) | 50.3 ± 12.6 | 51.9 ± 12.8 | 45.7 ± 10.8 | <0.001 |
| TG (mg/dL) | 147.9 ± 120.1 | 127.0 ± 104.9 | 172.7 ± 101.6 | <0.001 |
| SBP (mmHg) | 121.6 ± 16.9 | 120.1 ± 16.8 | 126.0 ± 16.2 | <0.001 |
| DBP (mmHg) | 75.8 ± 9.6 | 75.1 ± 9.6 | 78.1 ± 9.6 | <0.001 |
| CRP (mg/L) | 1.27 ± 2.3 | 1.18 ± 2.36 | 1.52 ± 2.03 | 0.007 |
| Health-Related Factors | ||||
| Smoking, n (%) | 523 (32.1) | 385 (31.8) | 138 (32.9) | 0.671 |
| Alcohol consumption, n (%) | 1012 (61.3) | 783 (63.7) | 229 (54.4) | 0.001 |
| Hypertension, n (%) | 481 (29.1) | 290 (23.6) | 191 (45.4) | <0.001 |
| Diabetes, n (%) | 207 (12.5) | 97 (7.9) | 110 (26.1) | <0.001 |
| Pulmonary Function | ||||
| FEV1 (%pred.) | 90.7 ± 13.1 | 90.7 ± 13.3 | 90.7 ± 12.6 | 0.898 |
| FEV1 (L) | 2.5 ± 0.65 | 2.6 ± 0.65 | 2.5 ± 0.68 | 0.552 |
| FVC (%pred.) | 90.3 ± 12.6 | 91.5 ± 12.4 | 86.9 ± 12.3 | <0.001 |
| FVC (L) | 3.3 ± 0.82 | 3.31 ± 0.81 | 3.20 ± 0.85 | 0.014 |
| FEV1/FVC | 0.78 ± 0.07 | 0.77 ± 0.07 | 0.79 ± 0.06 | <0.001 |
| Steatosis Index | ||||
| HSI | 33.2 ± 4.8 | 31.0 ± 2.9 | 39.6 ± 3.2 | <0.001 |
| Variables | Total (n = 1651) | High HGS (n = 826) | Low HGS (n = 826) | p-Value |
|---|---|---|---|---|
| Anthropometrics | ||||
| Age (years) | 58.2 ± 11.4 | 53.7 ± 9.4 | 62.7 ± 11.5 | <0.001 |
| Male, n (%) | 601 (36.4) | 301 (36.4) | 300 (36.4) | 0.507 |
| BMI (kg/m2) | 24.2 ± 3.3 | 22.9 ± 2.7 | 25.5 ± 3.23 | <0.001 |
| Relative HGS (kg/BMI) | 1.25 ± 0.41 | 1.46 ± 0.37 | 1.03 ± 0.31 | <0.001 |
| Blood Markers | ||||
| AST (U/L) | 22.8 ± 10.2 | 21.8 ± 10.1 | 23.7 ± 10.2 | <0.001 |
| ALT (U/L) | 22.0 ± 15.3 | 20.6 ± 15.0 | 23.4 ± 15.5 | <0.001 |
| FBG (mg/dL) | 103.8 ± 26.1 | 99.3 ± 20.2 | 108.3 ± 30.3 | <0.001 |
| TC (mg/dL) | 195.6 ± 39.1 | 197.0 ± 38.0 | 194.1 ± 40.3 | 0.137 |
| HDL-C (mg/dL) | 50.3 ± 12.6 | 52.5 ± 12.6 | 48.1 ± 12.1 | <0.001 |
| TG (mg/dL) | 147.9 ± 120.1 | 127.4 ± 117.4 | 149.9 ± 91.6 | <0.001 |
| SBP (mmHg) | 121.6 ± 16.9 | 118.4 ± 15.8 | 124.8 ± 17.3 | <0.001 |
| DBP (mmHg) | 75.8 ± 9.6 | 76.2 ± 9.3 | 75.5 ± 10.0 | 0.160 |
| CRP (mg/L) | 1.27 ± 2.3 | 1.05 ± 2.0 | 1.48 ± 2.5 | <0.001 |
| Health-Related Factors | ||||
| Smoking, n (%) | 523 (32.1) | 259 (31.5) | 264 (32.7) | 0.314 |
| Alcohol consumption, n (%) | 1012 (61.3) | 583 (70.6) | 42.4 (52.0) | <0.001 |
| Hypertension, n (%) | 481 (29.1) | 138 (16.7) | 343 (41.6) | <0.001 |
| Diabetes, n (%) | 207 (12.5) | 63 (7.6) | 144 (17.5) | <0.001 |
| Pulmonary Function | ||||
| FEV1 (%pred.) | 90.7 ± 13.1 | 91.4 ± 11.9 | 90.0 ± 14.3 | 0.031 |
| FEV1 (L) | 2.5 ± 0.7 | 2.8 ± 0.6 | 2.3 ± 0.6 | <0.001 |
| FVC (%pred.) | 90.3 ± 12.6 | 93.3 ± 11.3 | 87.6 ± 13.1 | <0.001 |
| FVC (L) | 3.3 ± 0.8 | 3.5 ± 0.8 | 3.0 ± 0.8 | <0.001 |
| FEV1/FVC | 0.78 ± 0.07 | 0.78 ± 0.07 | 0.77 ± 0.08 | 0.001 |
| Steatosis Index | ||||
| HSI | 33.2 ± 4.8 | 31.6 ± 4.2 | 34.8 ± 4.8 | <0.001 |
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | ||
|---|---|---|---|---|---|
| FVC (%pred.) | FEV1 (%pred.) | ||||
| Normal | 1 | Normal | 1 | ||
| NAFLD | 1.938 (1.48–2.54) | <0.001 | NAFLD | 0.952 (0.71–1.28) | 0.747 |
| High HGS | 1 | High HGS | 1 | ||
| Low HGS | 1.951 (1.69–2.26) | <0.001 | Low HGS | 1.507 (1.16–1.96) | 0.002 |
| Crude Model | Model 1 | Model 2 | Model 3 | |||||
|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Total (n = 1651) | ||||||||
| Normal + High HGS | 1 | 1 | 1 | 1 | ||||
| NAFLD + High HGS | 1.297 (0.67–2.50) | 0.436 | 1.443 (0.74–2.81) | 0.281 | 1.455 (0.75–2.84) | 0.271 | 1.398 (0.70–2.76) | 0.341 |
| Normal + Low HGS | 3.062 (2.46–4.83) | <0.001 | 1.990 (1.38–2.87) | <0.001 | 2.017 (1.39–2.92) | <0.001 | 2.036 (1.40–2.97) | <0.001 |
| NAFLD + Low HGS | 4.489 (3.43–7.09) | <0.001 | 3.606 (2.46–5.29) | <0.001 | 3.581 (2.43–5.27) | <0.001 | 3.390 (2.23–5.15) | <0.001 |
| Non-obese (n = 1042) | ||||||||
| Normal + High HGS | 1 | 1 | 1 | 1 | ||||
| NAFLD + High HGS | 1.923 (0.42–8.73) | 0.397 | 1.881 (0.41–8.69) | 0.419 | 1.937 (0.42–8.97) | 0.398 | 1.674 (0.35–8.02) | 0.519 |
| Normal + Low HGS | 4.055 (2.62–6.27) | <0.001 | 2.339 (1.44–3.79) | 0.001 | 2.454 (1.51–4.00) | <0.001 | 2.480 (1.51–4.07) | <0.001 |
| NAFLD + Low HGS | 6.396 (2.72–15.07) | <0.001 | 4.160 (1.70–10.16) | 0.002 | 4.274 (1.74–10.48) | 0.002 | 3.856 (1.49–9.99) | 0.005 |
| Obese (n = 609) | ||||||||
| Normal + High HGS | 1 | 1 | 1 | 1 | ||||
| NAFLD + High HGS | 1.251 (0.68–2.31) | 0.473 | 1.619 (0.85–3.10) | 0.146 | 1.550 (0.80–2.99) | 0.285 | 1.536 (0.78–3.01) | 0.211 |
| Normal + Low HGS | 2.550 (1.36–4.77) | 0.003 | 1.533 (0.78–3.01) | 0.215 | 1.457 (0.73–2.90) | 0.191 | 1.398 (0.68–2.86) | 0.358 |
| NAFLD + Low HGS | 2.568 (1.46–4.51) | 0.001 | 2.247 (1.23–4.11) | 0.008 | 2.289 (1.25–4.19) | 0.007 | 2.192 (1.15–4.16) | 0.017 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, J.; Johnson, B.D.; Watt, K.D.; Kim, C.-H. Greater Muscular Strength Is Associated with a Lower Risk of Pulmonary Dysfunction in Individuals with Non-Alcoholic Fatty Liver Disease. J. Clin. Med. 2022, 11, 4151. https://doi.org/10.3390/jcm11144151
Cho J, Johnson BD, Watt KD, Kim C-H. Greater Muscular Strength Is Associated with a Lower Risk of Pulmonary Dysfunction in Individuals with Non-Alcoholic Fatty Liver Disease. Journal of Clinical Medicine. 2022; 11(14):4151. https://doi.org/10.3390/jcm11144151
Chicago/Turabian StyleCho, Jinkyung, Bruce D. Johnson, Kymberly D. Watt, and Chul-Ho Kim. 2022. "Greater Muscular Strength Is Associated with a Lower Risk of Pulmonary Dysfunction in Individuals with Non-Alcoholic Fatty Liver Disease" Journal of Clinical Medicine 11, no. 14: 4151. https://doi.org/10.3390/jcm11144151
APA StyleCho, J., Johnson, B. D., Watt, K. D., & Kim, C.-H. (2022). Greater Muscular Strength Is Associated with a Lower Risk of Pulmonary Dysfunction in Individuals with Non-Alcoholic Fatty Liver Disease. Journal of Clinical Medicine, 11(14), 4151. https://doi.org/10.3390/jcm11144151