
Association of Serum Lipid Level with Meibum Biosynthesis and Meibomian Gland Dysfunction: A Review

 and
and
Abstract
:1. Introduction
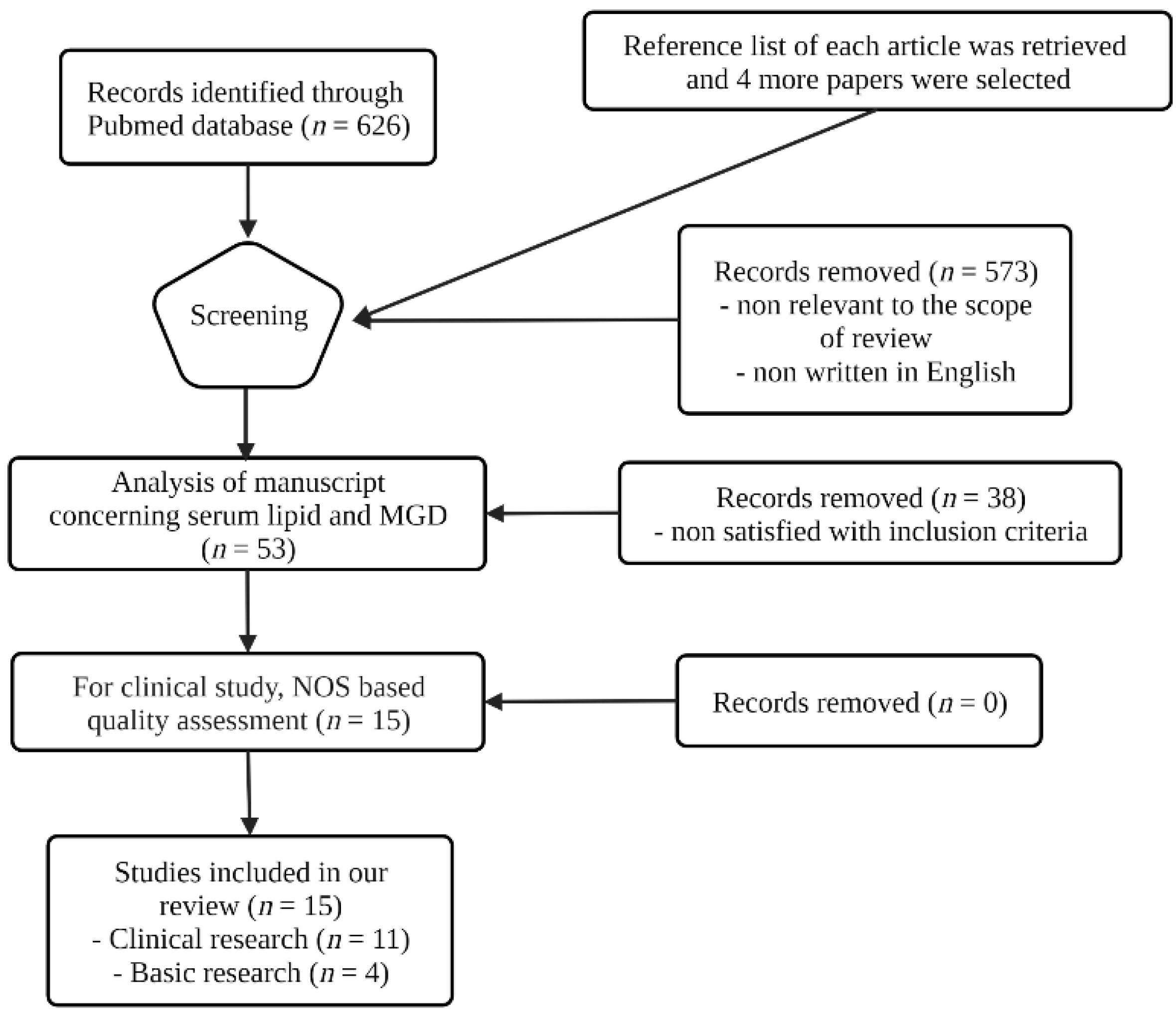
2. Sources and Methods of Literature Search
3. Research Results from Previous Studies
3.1. Clinical Research of Serum Lipid and MGD
3.2. Basic Research on Serum Lipids and MGD
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Knop, E.; Knop, N.; Millar, T.; Obata, H.; Sullivan, D.A. The international workshop on meibomian gland dysfunction: Report of the subcommittee on anatomy, physiology, and pathophysiology of the meibomian gland. Investig. Ophthalmol. Vis. Sci. 2011, 52, 1938–1978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nichols, K.K.; Foulks, G.N.; Bron, A.J.; Glasgow, B.J.; Dogru, M.; Tsubota, K.; Lemp, M.A.; Sullivan, D.A. The international workshop on meibomian gland dysfunction: Executive summary. Investig. Ophthalmol. Vis. Sci. 2011, 52, 1922–1929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willcox, M.D.P.; Argüeso, P.; Georgiev, G.A.; Holopainen, J.M.; Laurie, G.W.; Millar, T.J.; Papas, E.B.; Rolland, J.P.; Schmidt, T.A.; Stahl, U.; et al. TFOS DEWS II Tear Film Report. Ocul. Surf. 2017, 15, 366–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bründl, M.; Garreis, F.; Schicht, M.; Dietrich, J.; Paulsen, F. Characterization of the innervation of the meibomian glands in humans, rats and mice. Ann. Anat. 2021, 233, 151609. [Google Scholar] [CrossRef] [PubMed]
- Linton, R.G.; Curnow, D.H.; Riley, W.J. The meibomian glands: An investigation into the secretion and some aspects of the physiology. Br. J. Ophthalmol. 1961, 45, 718–723. [Google Scholar] [CrossRef] [Green Version]
- Nicolaides, N.; Kaitaranta, J.K.; Rawdah, T.N.; Macy, J.I.; Boswell, F.M., 3rd; Smith, R.E. Meibomian gland studies: Comparison of steer and human lipids. Investig. Ophthalmol. Vis. Sci. 1981, 20, 522–536. [Google Scholar]
- Butovich, I.A. The Meibomian puzzle: Combining pieces together. Prog. Retin. Eye Res. 2009, 28, 483–498. [Google Scholar] [CrossRef] [Green Version]
- Pucker, A.D.; Nichols, J.J. Analysis of meibum and tear lipids. Ocul. Surf. 2012, 10, 230–250. [Google Scholar] [CrossRef]
- Butovich, I.A. Tear film lipids. Exp. Eye Res. 2013, 117, 4–27. [Google Scholar] [CrossRef] [Green Version]
- Brown, S.H.; Kunnen, C.M.; Duchoslav, E.; Dolla, N.K.; Kelso, M.J.; Papas, E.B.; Lazon de la Jara, P.; Willcox, M.D.; Blanksby, S.J.; Mitchell, T.W. A comparison of patient matched meibum and tear lipidomes. Investig. Ophthalmol. Vis. Sci. 2013, 54, 7417–7424. [Google Scholar] [CrossRef]
- Butovich, I.A.; Wilkerson, A.; Yuksel, S. Depletion of Cholesteryl Esters Causes Meibomian Gland Dysfunction-Like Symptoms in a Soat1-Null Mouse Model. Int. J. Mol. Sci. 2021, 22, 1583. [Google Scholar] [CrossRef] [PubMed]
- Lam, S.M.; Tong, L.; Yong, S.S.; Li, B.; Chaurasia, S.S.; Shui, G.; Wenk, M.R. Meibum lipid composition in Asians with dry eye disease. PLoS ONE 2011, 6, e24339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelson, J.D.; Shimazaki, J.; Benitez-del-Castillo, J.M.; Craig, J.P.; McCulley, J.P.; Den, S.; Foulks, G.N. The international workshop on meibomian gland dysfunction: Report of the definition and classification subcommittee. Investig. Ophthalmol. Vis. Sci. 2011, 52, 1930–1937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bland, H.C.; Moilanen, J.A.; Ekholm, F.S.; Paananen, R.O. Investigating the Role of Specific Tear Film Lipids Connected to Dry Eye Syndrome: A Study on O-Acyl-ω-hydroxy Fatty Acids and Diesters. Langmuir 2019, 35, 3545–3552. [Google Scholar] [CrossRef]
- Klop, B.; Elte, J.W.; Cabezas, M.C. Dyslipidemia in obesity: Mechanisms and potential targets. Nutrients 2013, 5, 1218–1240. [Google Scholar] [CrossRef] [Green Version]
- Nikolic, D.; Castellino, G.; Banach, M.; Toth, P.P.; Ivanova, E.; Orekhov, A.N.; Montalto, G.; Rizzo, M. PPAR Agonists, Atherogenic Dyslipidemia and Cardiovascular Risk. Curr. Pharm. Des. 2017, 23, 894–902. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [Green Version]
- Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ott. Hosp. Res. Inst. 2011, 2, 1–12. [Google Scholar]
- Guliani, B.P.; Bhalla, A.; Naik, M.P. Association of the severity of meibomian gland dysfunction with dyslipidemia in Indian population. Indian J. Ophthalmol. 2018, 66, 1411–1416. [Google Scholar]
- Pinna, A.; Blasetti, F.; Zinellu, A.; Carru, C.; Solinas, G. Meibomian gland dysfunction and hypercholesterolemia. Ophthalmology 2013, 120, 2385–2389. [Google Scholar] [CrossRef]
- Braich, P.S.; Howard, M.K.; Singh, J.S. Dyslipidemia and its association with meibomian gland dysfunction. Int. Ophthalmol. 2016, 36, 469–476. [Google Scholar] [CrossRef]
- Chen, A.; Chen, H.T.; Chen, H.C.; Chen, Y.T.; Hwang, Y.H.; Sun, C.C.; Hsiao, C.H.; Ma, D.H.; Wu, W.C.; Lai, C.C. Asymptomatic Meibomian Gland Dysfunction and Cardiovascular Disease Risk Factors in a Middle-Aged Population in Taiwan—A Cross-sectional Analysis. Sci. Rep. 2017, 7, 4935. [Google Scholar] [CrossRef] [PubMed]
- Irfan, K.S.A.; Agrawal, A.; Singh, A.; Mittal, S.K.; Samanta, R. Association of Lipid Profile with Severity of Meibomian Gland Dysfunction. Nepal J. Ophthalmol. 2020, 12, 216–235. [Google Scholar] [CrossRef] [PubMed]
- Mussi, N.; Haque, W.; Robertson, D.M. The Association Between Risk Factors for Metabolic Syndrome and Meibomian Gland Disease in a Dry Eye Cohort. Clin. Ophthalmol. 2021, 15, 3821–3832. [Google Scholar] [CrossRef] [PubMed]
- Ha, M.; Song, J.; Park, S.; Han, K.; Hwang, H.S.; Kim, H.S.; Arita, R.; Na, K.S. Relationship between serum lipid level and meibomian gland dysfunction subtype in Korea using propensity score matching. Sci. Rep. 2021, 11, 16102. [Google Scholar] [CrossRef] [PubMed]
- Bukhari, A.A. Associations between the grade of meibomian gland dysfunction and dyslipidemia. Ophthalmic Plast. Reconstr. Surg. 2013, 29, 101–103. [Google Scholar] [CrossRef]
- Tulsyan, N.; Gupta, N.; Agrawal, N. Risk Factors Associated with Meibomian Gland Dysfunction: A Hospital Based Study. Nepal J. Ophthalmol. 2021, 13, 59–64. [Google Scholar] [CrossRef]
- Rajaram, S.; Haddad, E.H.; Mejia, A.; Sabaté, J. Walnuts and fatty fish influence different serum lipid fractions in normal to mildly hyperlipidemic individuals: A randomized controlled study. Am. J. Clin. Nutr. 2009, 89, 1657s–1663s. [Google Scholar] [CrossRef] [Green Version]
- Carrero, J.J.; Fonollá, J.; Marti, J.L.; Jiménez, J.; Boza, J.J.; López-Huertas, E. Intake of fish oil, oleic acid, folic acid, and vitamins B-6 and E for 1 year decreases plasma C-reactive protein and reduces coronary heart disease risk factors in male patients in a cardiac rehabilitation program. J. Nutr. 2007, 137, 384–390. [Google Scholar] [CrossRef] [Green Version]
- Demonty, I.; Chan, Y.M.; Pelled, D.; Jones, P.J. Fish-oil esters of plant sterols improve the lipid profile of dyslipidemic subjects more than do fish-oil or sunflower oil esters of plant sterols. Am. J. Clin. Nutr. 2006, 84, 1534–1542. [Google Scholar] [CrossRef] [Green Version]
- Kelley, D.S.; Siegel, D.; Vemuri, M.; Chung, G.H.; Mackey, B.E. Docosahexaenoic acid supplementation decreases remnant-like particle-cholesterol and increases the (n-3) index in hypertriglyceridemic men. J. Nutr. 2008, 138, 30–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macsai, M.S. The role of omega-3 dietary supplementation in blepharitis and meibomian gland dysfunction (an AOS thesis). Trans. Am. Ophthalmol. Soc. 2008, 106, 336–356. [Google Scholar] [PubMed]
- Sheppard, J.D., Jr.; Singh, R.; McClellan, A.J.; Weikert, M.P.; Scoper, S.V.; Joly, T.J.; Whitley, W.O.; Kakkar, E.; Pflugfelder, S.C. Long-term Supplementation With n-6 and n-3 PUFAs Improves Moderate-to-Severe Keratoconjunctivitis Sicca: A Randomized Double-Blind Clinical Trial. Cornea 2013, 32, 1297–1304. [Google Scholar] [CrossRef] [PubMed]
- Korb, D.R.; Blackie, C.A.; Finnemore, V.M.; Douglass, T. Effect of using a combination of lid wipes, eye drops, and omega-3 supplements on meibomian gland functionality in patients with lipid deficient/evaporative dry eye. Cornea 2015, 34, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, C.; Singh, S.; Chakma, P.; Jain, A.K. Effect of oral omega-3 Fatty Acid supplementation on contrast sensitivity in patients with moderate meibomian gland dysfunction: A prospective placebo-controlled study. Cornea 2015, 34, 637–643. [Google Scholar] [CrossRef] [Green Version]
- Pinna, A.; Piccinini, P.; Carta, F. Effect of oral linoleic and gamma-linolenic acid on meibomian gland dysfunction. Cornea 2007, 26, 260–264. [Google Scholar] [CrossRef]
- Oleñik, A.; Jiménez-Alfaro, I.; Alejandre-Alba, N.; Mahillo-Fernández, I. A randomized, double-masked study to evaluate the effect of omega-3 fatty acids supplementation in meibomian gland dysfunction. Clin. Interv. Aging 2013, 8, 1133–1138. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.W.; Rho, C.R.; Kim, J.; Xie, Y.; Prince, R.C.; Mustafa, K.; Potma, E.O.; Brown, D.J.; Jester, J.V. Eicosapentaenoic acid (EPA) activates PPARγ signaling leading to cell cycle exit, lipid accumulation, and autophagy in human meibomian gland epithelial cells (hMGEC). Ocul. Surf. 2020, 18, 427–437. [Google Scholar] [CrossRef]
- Butovich, I.A.; Bhat, N.; Wojtowicz, J.C. Comparative Transcriptomic and Lipidomic Analyses of Human Male and Female Meibomian Glands Reveal Common Signature Genes of Meibogenesis. Int. J. Mol. Sci. 2019, 20, 4539. [Google Scholar] [CrossRef] [Green Version]
- Wu, K.I.; Chen, C.Y.; Jou, T.S.; Jimmy Juang, J.M.; Lu, J.Y.; Wang, I.J. Effect of 3-Hydroxy-3-Methyl-Glutaryl-Coenzyme A Reductase Inhibitors on the Meibomian Gland Morphology in Patients with Dyslipidemia. Am. J. Ophthalmol. 2020, 219, 240–252. [Google Scholar] [CrossRef]
- Ooi, K.G.; Lee, M.H.; Burlutsky, G.; Gopinath, B.; Mitchell, P.; Watson, S. Association of dyslipidaemia and oral statin use, and dry eye disease symptoms in the Blue Mountains Eye Study. Clin. Exp. Ophthalmol. 2019, 47, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Maskin, S.L.; Tseng, S.C. Culture of rabbit meibomian gland using collagen gel. Investig. Ophthalmol. Vis. Sci. 1991, 32, 214–223. [Google Scholar]
- Richards, S.; Schirra, F.; Sullivan, D. Development of a defined, serum-free culture system for the maintenance of epithelial cells from the mouse meibomian gland. Investig. Ophthalmol. Vis. Sci. 2002, 43, 3150. [Google Scholar]
- Jester, J.V.; Potma, E.; Brown, D.J. PPARγ Regulates Mouse Meibocyte Differentiation and Lipid Synthesis. Ocul. Surf. 2016, 14, 484–494. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.; Hatton, M.P.; Khandelwal, P.; Sullivan, D.A. Culture, immortalization, and characterization of human meibomian gland epithelial cells. Investig. Ophthalmol. Vis. Sci. 2010, 51, 3993–4005. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.W.; Xie, Y.; Nguyen, P.Q.; Bui, V.T.; Huynh, K.; Kang, J.S.; Brown, D.J.; Jester, J.V. PPARγ regulates meibocyte differentiation and lipid synthesis of cultured human meibomian gland epithelial cells (hMGEC). Ocul. Surf. 2018, 16, 463–469. [Google Scholar] [CrossRef]
- Liu, Y.; Kam, W.R.; Ding, J.; Sullivan, D.A. Effect of azithromycin on lipid accumulation in immortalized human meibomian gland epithelial cells. JAMA Ophthalmol. 2014, 132, 226–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, X.; Liu, Y.; Kam, W.R.; Sullivan, D.A. Effect of brimonidine, an α2 adrenergic agonist, on human meibomian gland epithelial cells. Exp. Eye Res. 2018, 170, 20–28. [Google Scholar] [CrossRef]
- Hampel, U.; Krüger, M.; Kunnen, C.; Garreis, F.; Willcox, M.; Paulsen, F. In vitro effects of docosahexaenoic and eicosapentaenoic acid on human meibomian gland epithelial cells. Exp. Eye Res. 2015, 140, 139–148. [Google Scholar] [CrossRef]
- Liu, Y.; Kam, W.R.; Ding, J.; Sullivan, D.A. One man’s poison is another man’s meat: Using azithromycin-induced phospholipidosis to promote ocular surface health. Toxicology 2014, 320, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Ziemanski, J.F.; Wilson, L.; Barnes, S.; Nichols, K.K. Saturation of cholesteryl esters produced by human meibomian gland epithelial cells after treatment with rosiglitazone. Ocul. Surf. 2020, 20, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, D.A.; Liu, Y.; Kam, W.R.; Ding, J.; Green, K.M.; Shaffer, S.A.; Hatton, M.P.; Liu, S. Serum-induced differentiation of human meibomian gland epithelial cells. Investig. Ophthalmol. Vis. Sci. 2014, 55, 3866–3877. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Kam, W.R.; Sullivan, D.A. Influence of Omega 3 and 6 Fatty Acids on Human Meibomian Gland Epithelial Cells. Cornea 2016, 35, 1122–1126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asano, N.; Hampel, U.; Garreis, F.; Schröder, A.; Schicht, M.; Hammer, C.M.; Paulsen, F. Differentiation Patterns of Immortalized Human Meibomian Gland Epithelial Cells in Three-Dimensional Culture. Investig. Ophthalmol. Vis. Sci. 2018, 59, 1343–1353. [Google Scholar] [CrossRef]
- Butovich, I.A. Meibomian glands, meibum, and meibogenesis. Exp. Eye Res. 2017, 163, 2–16. [Google Scholar] [CrossRef]
- Sassa, T.; Tadaki, M.; Kiyonari, H.; Kihara, A. Very long-chain tear film lipids produced by fatty acid elongase ELOVL1 prevent dry eye disease in mice. FASEB J. 2018, 32, 2966–2978. [Google Scholar] [CrossRef] [Green Version]
- Butovich, I.A.; Wilkerson, A.; Bhat, N.; McMahon, A.; Yuksel, S. On the pivotal role of Elovl3/ELOVL3 in meibogenesis and ocular physiology of mice. FASEB J. 2019, 33, 10034–10048. [Google Scholar] [CrossRef]
- Miyamoto, M.; Sassa, T.; Sawai, M.; Kihara, A. Lipid polarity gradient formed by ω-hydroxy lipids in tear film prevents dry eye disease. eLife 2020, 9. [Google Scholar] [CrossRef]
- Widjaja-Adhi, M.A.K.; Silvaroli, J.A.; Chelstowska, S.; Trischman, T.; Bederman, I.; Sayegh, R.; Golczak, M. Deficiency in Acyl-CoA:Wax Alcohol Acyltransferase 2 causes evaporative dry eye disease by abolishing biosynthesis of wax esters. FASEB J. 2020, 34, 13792–13808. [Google Scholar] [CrossRef]
- McMahon, A.; Yuksel, S.; Bhat, N.; Pham, H.; Wilkerson, A.; Butovich, I.A. Inactivation of Awat2 in mice causes loss of wax ester lipids from meibum. Investig. Ophthalmol. Vis. Sci. 2020, 61, 2632. [Google Scholar]
- Sun, M.; Moreno, I.Y.; Dang, M.; Coulson-Thomas, V.J. Meibomian Gland Dysfunction: What Have Animal Models Taught Us? Int. J. Mol. Sci. 2020, 21, 8822. [Google Scholar] [CrossRef] [PubMed]
- Osada, J.; Joven, J.; Maeda, N. The value of apolipoprotein E knockout mice for studying the effects of dietary fat and cholesterol on atherogenesis. Curr. Opin. Lipidol. 2000, 11, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Bu, J.; Wu, Y.; Cai, X.; Jiang, N.; Jeyalatha, M.V.; Yu, J.; He, X.; He, H.; Guo, Y.; Zhang, M.; et al. Hyperlipidemia induces meibomian gland dysfunction. Ocul. Surf. 2019, 17, 777–786. [Google Scholar] [CrossRef] [PubMed]
- Miyake, H.; Oda, T.; Katsuta, O.; Seno, M.; Nakamura, M. Meibomian Gland Dysfunction Model in Hairless Mice Fed a Special Diet with Limited Lipid Content. Investig. Ophthalmol. Vis. Sci. 2016, 57, 3268–3275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Y.; Wu, J.; Bu, J.; Tang, L.; Yang, Y.; Ouyang, W.; Lin, X.; Liu, Z.; Huang, C.; Quantock, A.J.; et al. High-fat diet induces dry eye-like ocular surface damages in murine. Ocul. Surf. 2020, 18, 267–276. [Google Scholar] [CrossRef]
- Osae, E.A.; Steven, P.; Redfern, R.; Hanlon, S.; Smith, C.W.; Rumbaut, R.E.; Burns, A.R. Dyslipidemia and Meibomian Gland Dysfunction: Utility of Lipidomics and Experimental Prospects with a Diet-Induced Obesity Mouse Model. Int. J. Mol. Sci. 2019, 20, 3505. [Google Scholar] [CrossRef] [Green Version]
- Hargrave, A.; Courson, J.A.; Pham, V.; Landry, P.; Magadi, S.; Shankar, P.; Hanlon, S.; Das, A.; Rumbaut, R.E.; Smith, C.W.; et al. Corneal dysfunction precedes the onset of hyperglycemia in a mouse model of diet-induced obesity. PLoS ONE 2020, 15, e0238750. [Google Scholar] [CrossRef]
- Osae, E.A.; Bullock, T.; Chintapalati, M.; Brodesser, S.; Hanlon, S.; Redfern, R.; Steven, P.; Smith, C.W.; Rumbaut, R.E.; Burns, A.R. Obese Mice with Dyslipidemia Exhibit Meibomian Gland Hypertrophy and Alterations in Meibum Composition and Aqueous Tear Production. Int. J. Mol. Sci. 2020, 21, 8772. [Google Scholar] [CrossRef]
- Bagga, D.; Wang, L.; Farias-Eisner, R.; Glaspy, J.A.; Reddy, S.T. Differential effects of prostaglandin derived from omega-6 and omega-3 polyunsaturated fatty acids on COX-2 expression and IL-6 secretion. Proc. Natl. Acad. Sci. USA 2003, 100, 1751–1756. [Google Scholar] [CrossRef] [Green Version]
- Esteve, E.; Ricart, W.; Fernández-Real, J.M. Dyslipidemia and inflammation: An evolutionary conserved mechanism. Clin. Nutr. 2005, 24, 16–31. [Google Scholar] [CrossRef]
- Henrich, C.F.; Ramulu, P.Y.; Akpek, E.K. Association of dry eye and inflammatory systemic diseases in a tertiary care-based sample. Cornea 2014, 33, 819–825. [Google Scholar] [CrossRef] [PubMed]
- Liew, M.S.; Zhang, M.; Kim, E.; Akpek, E.K. Prevalence and predictors of Sjogren’s syndrome in a prospective cohort of patients with aqueous-deficient dry eye. Br. J. Ophthalmol. 2012, 96, 1498–1503. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, D.A.; Dana, R.; Sullivan, R.M.; Krenzer, K.L.; Sahin, A.; Arica, B.; Liu, Y.; Kam, W.R.; Papas, A.S.; Cermak, J.M. Meibomian Gland Dysfunction in Primary and Secondary Sjögren Syndrome. Ophthalmic Res. 2018, 59, 193–205. [Google Scholar] [CrossRef] [PubMed]
- Suhalim, J.L.; Parfitt, G.J.; Xie, Y.; De Paiva, C.S.; Pflugfelder, S.C.; Shah, T.N.; Potma, E.O.; Brown, D.J.; Jester, J.V. Effect of desiccating stress on mouse meibomian gland function. Ocul. Surf. 2014, 12, 59–68. [Google Scholar] [CrossRef] [Green Version]
- Botta, M.; Audano, M.; Sahebkar, A.; Sirtori, C.R.; Mitro, N.; Ruscica, M. PPAR Agonists and Metabolic Syndrome: An Established Role? Int. J. Mol. Sci. 2018, 19, 1197. [Google Scholar] [CrossRef] [Green Version]
- Nien, C.J.; Massei, S.; Lin, G.; Nabavi, C.; Tao, J.; Brown, D.J.; Paugh, J.R.; Jester, J.V. Effects of age and dysfunction on human meibomian glands. Arch. Ophthalmol. 2011, 129, 462–469. [Google Scholar] [CrossRef] [Green Version]
- Betteridge, D.J. Chicago, periscope and PROactive: CV risk modification in diabetes with pioglitazone. Fundam. Clin. Pharmacol. 2009, 23, 675–679. [Google Scholar] [CrossRef]
- Alghamdi, Y.A.; Mercado, C.; McClellan, A.L.; Batawi, H.; Karp, C.L.; Galor, A. Epidemiology of Meibomian Gland Dysfunction in an Elderly Population. Cornea 2016, 35, 731–735. [Google Scholar] [CrossRef] [Green Version]
- Jester, J.V.; Brown, D.J. Wakayama Symposium: Peroxisome proliferator-activated receptor-gamma (PPARγ) and meibomian gland dysfunction. Ocul. Surf. 2012, 10, 224–229. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Pinna et al. [20] | Braich et al. [21] | Chen et al. [22] | Irfan et al. [23] | Mussi et al. [24] | Ha et al. [25] | Guliani et al. [19] | Bukhari et al. [26] | Tulsyan et al. [27] | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Level of evidence | Level 3 | Level 3 | Level 3 | Level 3 | Level 3 | Level 3 | Level 3 | Level 3 | Level 3 | ||||||
| Design | Case-control study | Case-control study | Case-control study | Case-control study | Case-control study | Case-control study | Case-control study | Case-control study | Case-control study | ||||||
| Number of participants (case/control) | 60/63 | 109/115 | 199/89 | 58/58 | 163/136 | 95/475 | 90/90 | 132/104 | 237/163 | ||||||
| Year | 2013 | 2016 | 2017 | 2020 | 2021 | 2021 | 2018 | 2013 | 2021 | ||||||
| Results | |||||||||||||||
| Mean serum lipid Level 1n patients with MGD (compared to those without MGD) | Mean serum lipid Level 1n patients with moderate to severe MGD (compared to mild MGD) | ||||||||||||||
| Total cholesterol | Higher † | Higher | Higher | N/A | Lower (NS) | Lower (NS) | N/A | N/A | N/A | ||||||
| LDL | Higher | Higher † | Higher | N/A | Higher (NS) | Lower | N/A | N/A | N/A | ||||||
| TG | Higher | Higher | Higher | N/A | Higher (NS) | Lower (NS) | N/A | N/A | N/A | ||||||
| HDL | Higher | Higher | Lower | N/A | Lower (NS) | Higher | N/A | N/A | N/A | ||||||
| Prevalence of dyslipidemia * among patients with MGD (compared to those without MGD) | Prevalence of dyslipidemia * in patients with moderate to severe MGD (compared to mild MGD) | ||||||||||||||
| Gender | Female | Male | |||||||||||||
| Age | <45 | 45–64 | ≥65 | ||||||||||||
| Total cholesterol | N/A | Higher | N/A | Higher | Lower (NS) | Higher (NS) | - | - | - | Higher | N/A | Higher (NS) | |||
| LDL | N/A | Higher | N/A | Higher | Lower (NS) | Higher (NS) | - | Higher | Higher | Higher | Higher (NS) | Higher | |||
| TG | N/A | Higher | N/A | Higher | N/A | N/A | - | - | - | Higher | Higher (NS) | Higher (NS) | |||
| HDL | N/A | Lower (NS) | N/A | Higher (NS) | Lower (NS) | Higher (NS) | - | Higher | - | Higher | N/A | Higher (NS) | |||
| Factors impacting development of MGD | |||||||||||||||
| MGD grade | 1 | 2 | 3 | 4 | |||||||||||
| Total cholesterol | V | V | - | - | V | V | - | N/A | N/A | N/A | N/A | N/A | |||
| LDL | V | V | V | - | - | - | - | N/A | N/A | N/A | N/A | N/A | |||
| TG | - | V | V | - | - | V, | V | N/A | N/A | N/A | N/A | N/A | |||
| HDL | V | - | - | - | - | - | - | N/A | N/A | N/A | N/A | N/A | |||
| Author | Year | Level of Evidence | Study Design | Number of Patients | Results | ||||
|---|---|---|---|---|---|---|---|---|---|
| Case | Control | Lid Margin Abnormality | MG Expressibility | MG Quality | MG Morphology | ||||
| Oleñik et al. [37] | 2013 | Level 1 | Randomized, double-masked study | Omega-3 treatment group (n = 33) | Placebo group (n = 31) | Improved | Improved | ||
| Wu et al. [39] | 2020 | Level 2 | Prospective, nonrandomized study | Statin treatment group (n = 85) | Life style intervention group (n = 13) | Deteriorated | Deteriorated | Deteriorated | |
| Author | Year | Animal Model | MG Features | Other Defects |
|---|---|---|---|---|
| Bu et al. [63] | 2019 | Apolipoprotein E knockout mice (ApoE(−/−)) | Plugging of the meibomian gland orifice, duct dilation, and heteromorphic acinar morphology. | Present punctate corneal staining and signs of corneal damage |
| Miyake et al. [64] | 2016 | HR-1 hairless mice fed an HR-AD diet (a special diet with limited lipid content) | Plugging of the meibomian gland orifice and toothpaste-like meibum. | - |
| Osae et al. [68] | 2020 | C57BL/6 mice fed a high-fat diet | Hypertrophic change in meibomian gland and increased lipid saturation in meibum. | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoo, Y.-S.; Park, S.-K.; Hwang, H.-S.; Kim, H.-S.; Arita, R.; Na, K.-S. Association of Serum Lipid Level with Meibum Biosynthesis and Meibomian Gland Dysfunction: A Review. J. Clin. Med. 2022, 11, 4010. https://doi.org/10.3390/jcm11144010
Yoo Y-S, Park S-K, Hwang H-S, Kim H-S, Arita R, Na K-S. Association of Serum Lipid Level with Meibum Biosynthesis and Meibomian Gland Dysfunction: A Review. Journal of Clinical Medicine. 2022; 11(14):4010. https://doi.org/10.3390/jcm11144010
Chicago/Turabian StyleYoo, Young-Sik, Sun-Kyoung Park, Ho-Sik Hwang, Hyun-Seung Kim, Reiko Arita, and Kyung-Sun Na. 2022. "Association of Serum Lipid Level with Meibum Biosynthesis and Meibomian Gland Dysfunction: A Review" Journal of Clinical Medicine 11, no. 14: 4010. https://doi.org/10.3390/jcm11144010
APA StyleYoo, Y.-S., Park, S.-K., Hwang, H.-S., Kim, H.-S., Arita, R., & Na, K.-S. (2022). Association of Serum Lipid Level with Meibum Biosynthesis and Meibomian Gland Dysfunction: A Review. Journal of Clinical Medicine, 11(14), 4010. https://doi.org/10.3390/jcm11144010