Factors Affecting the Success of Endodontic Microsurgery: A Cone-Beam Computed Tomography Study


Abstract
:1. Introduction
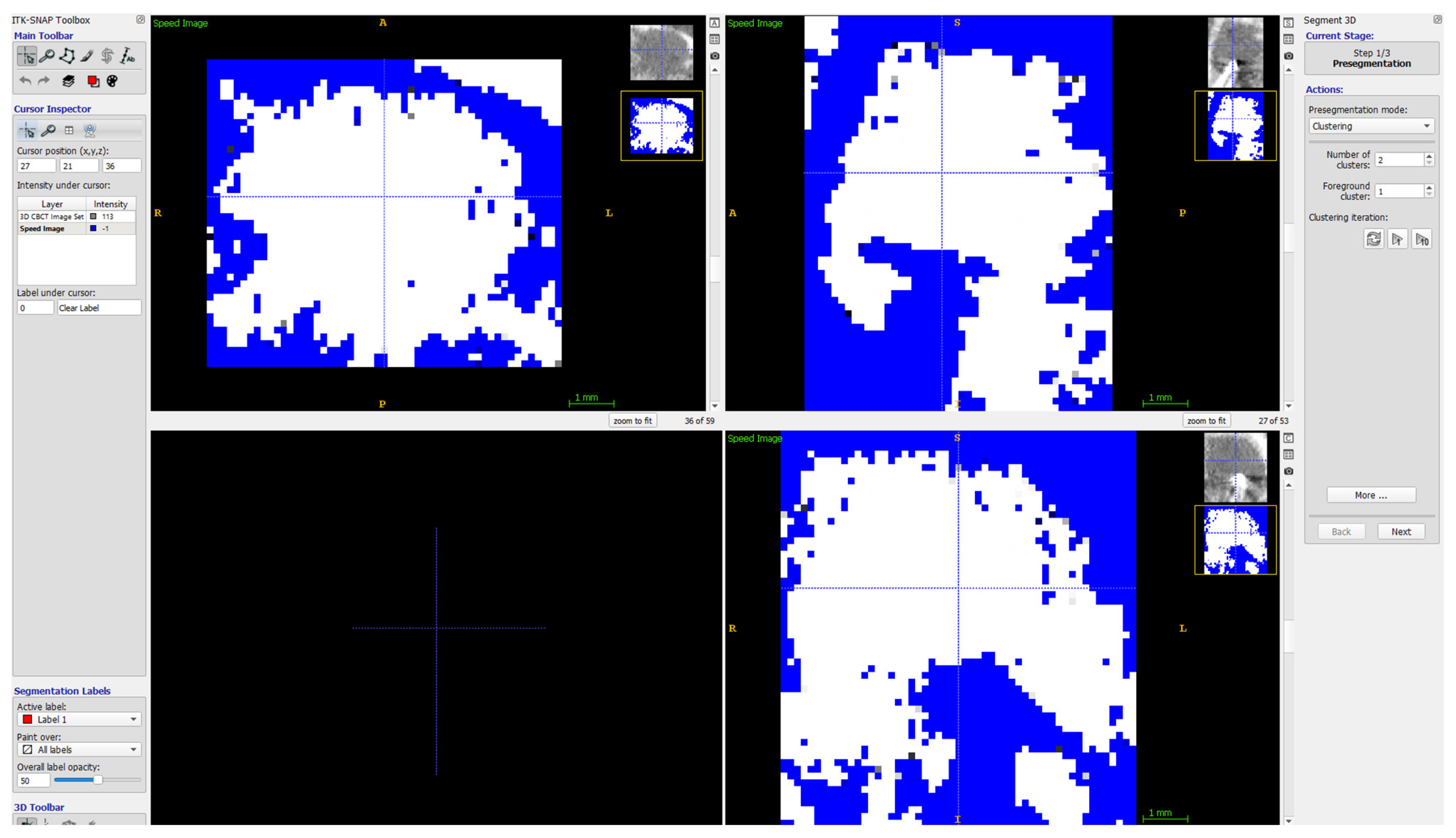
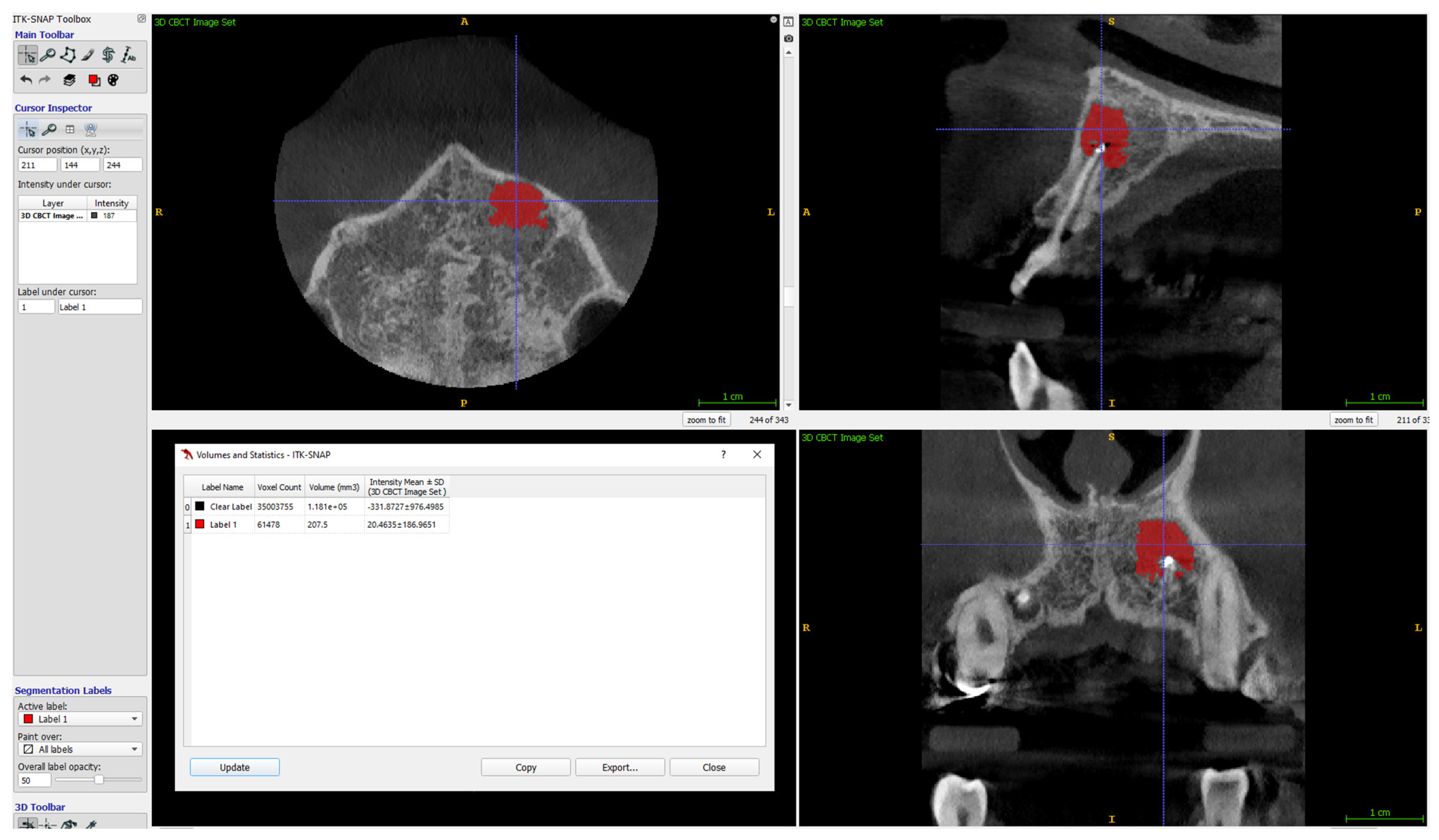
2. Materials and Methods
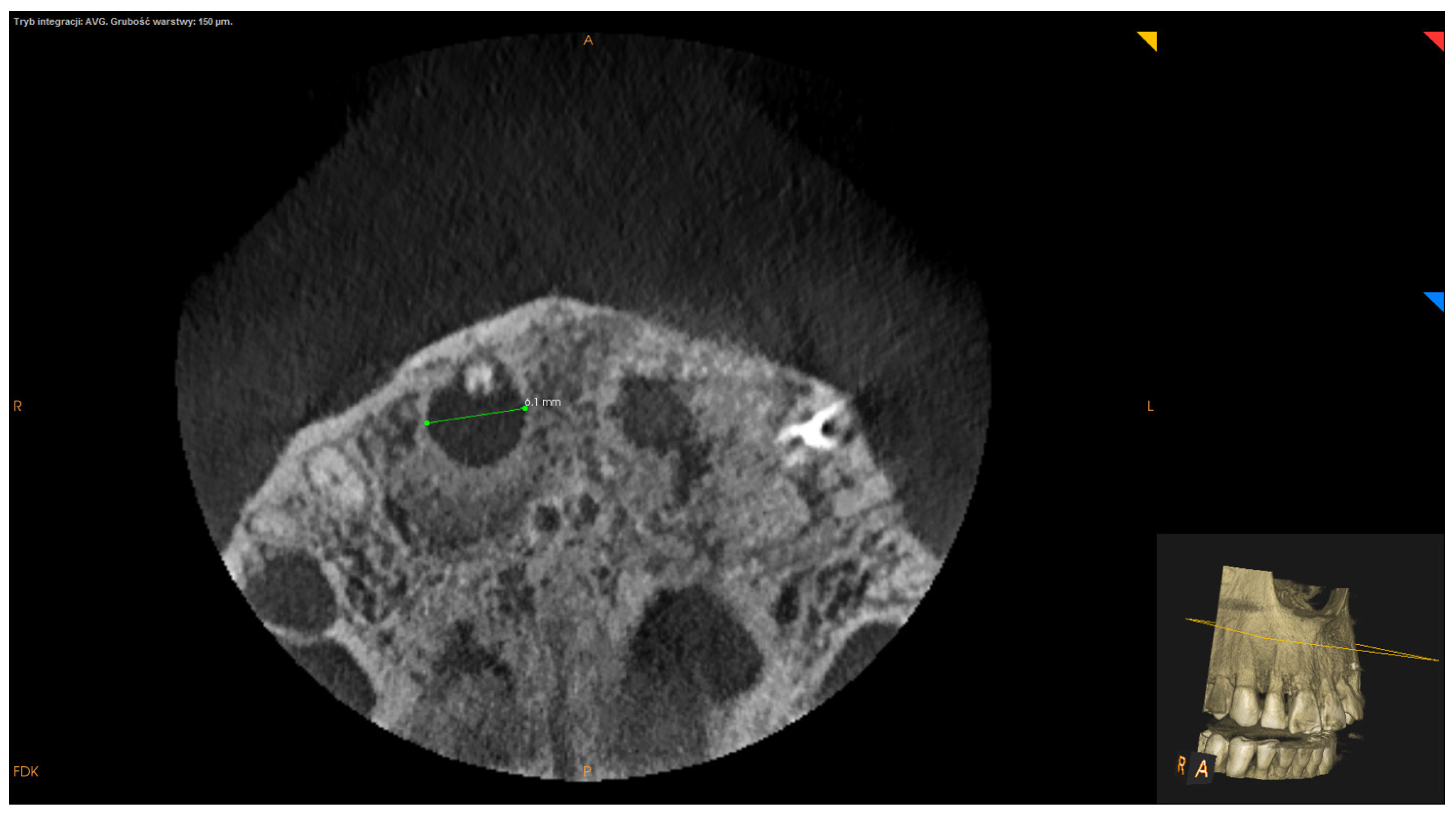
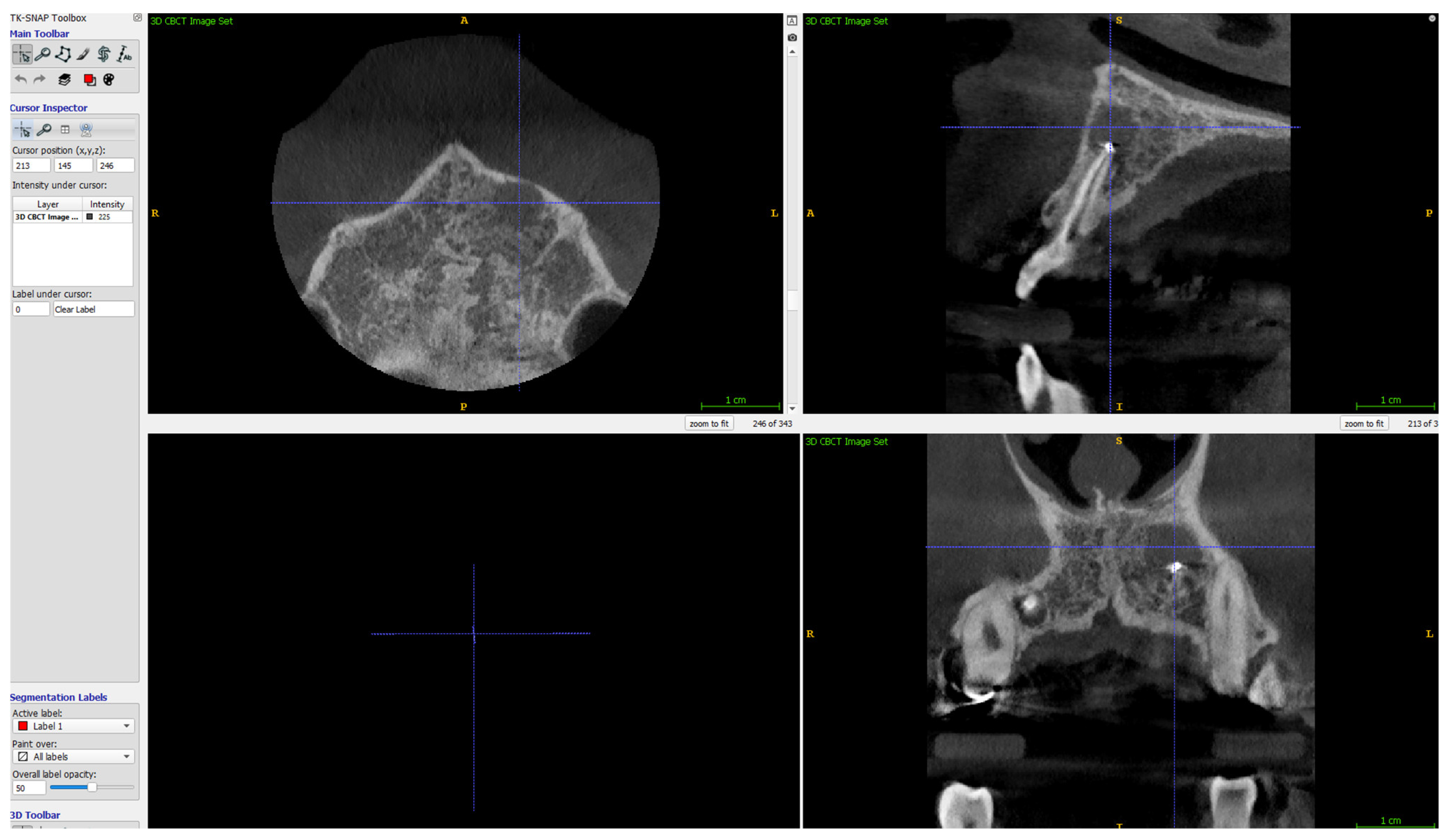
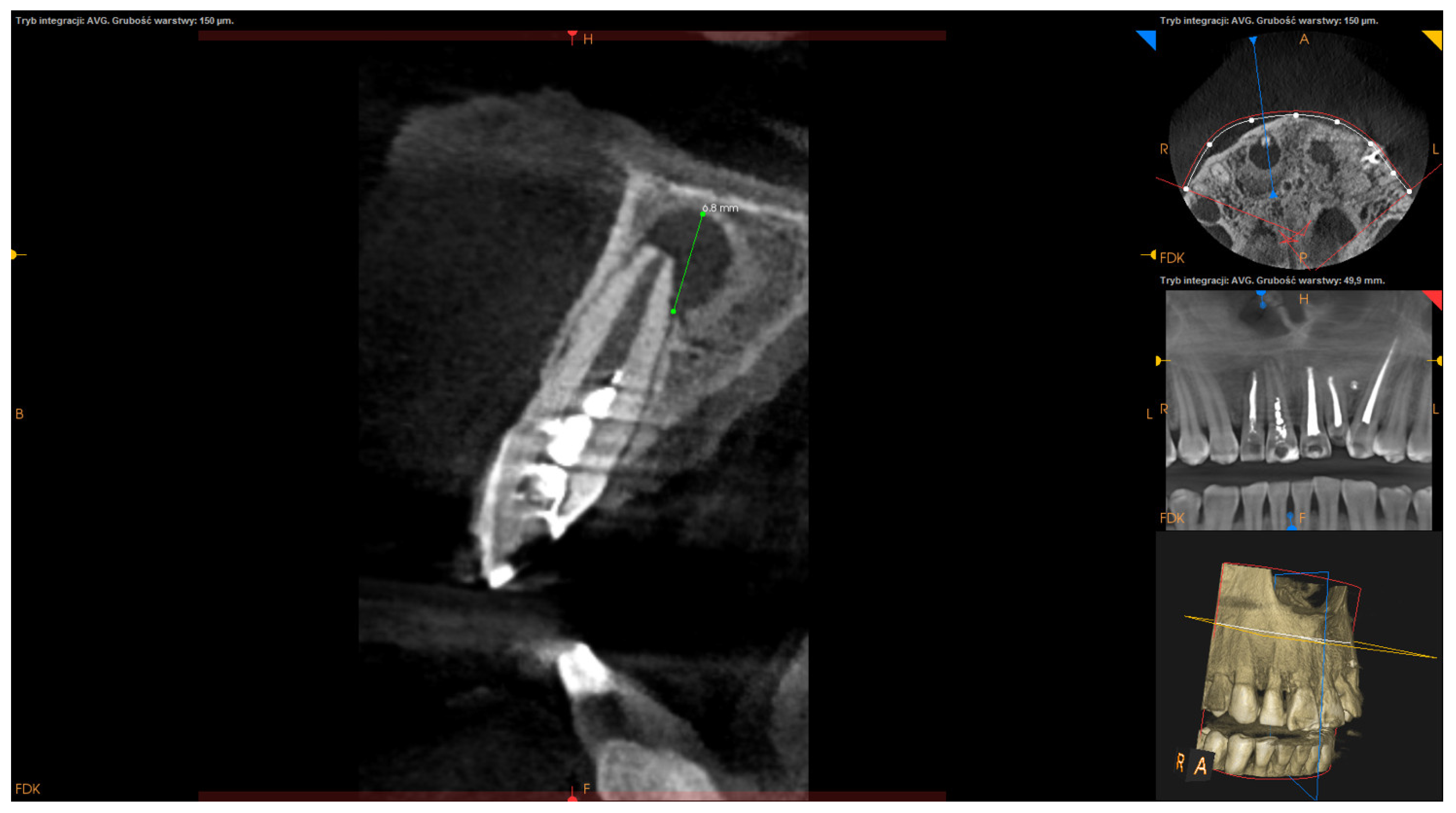
- Apicocoronal maximum diameter (measured in the sagittal section) (Figure 2);
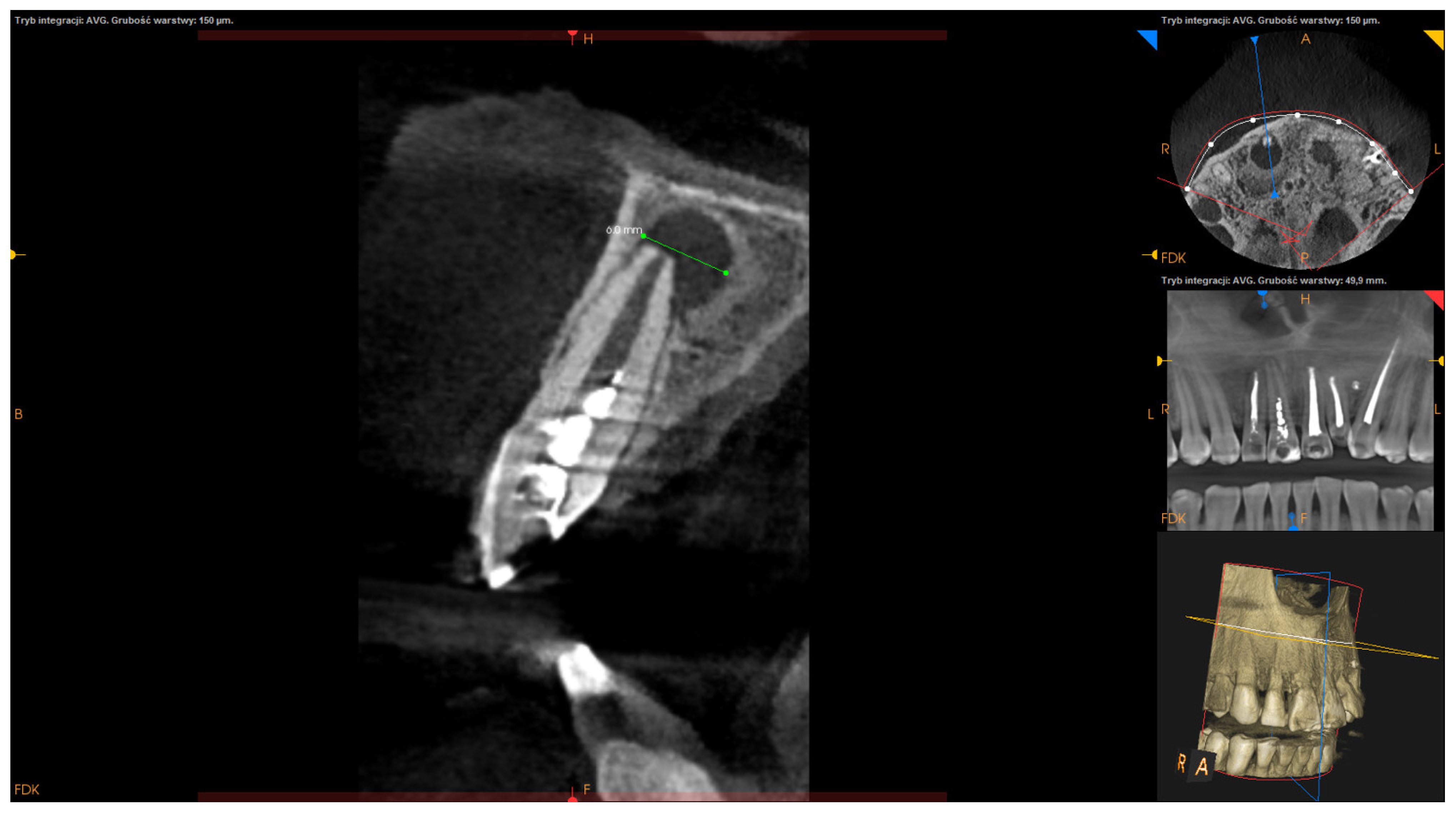
- Buccolingual maximum diameter (measured in the sagittal section) (Figure 3);
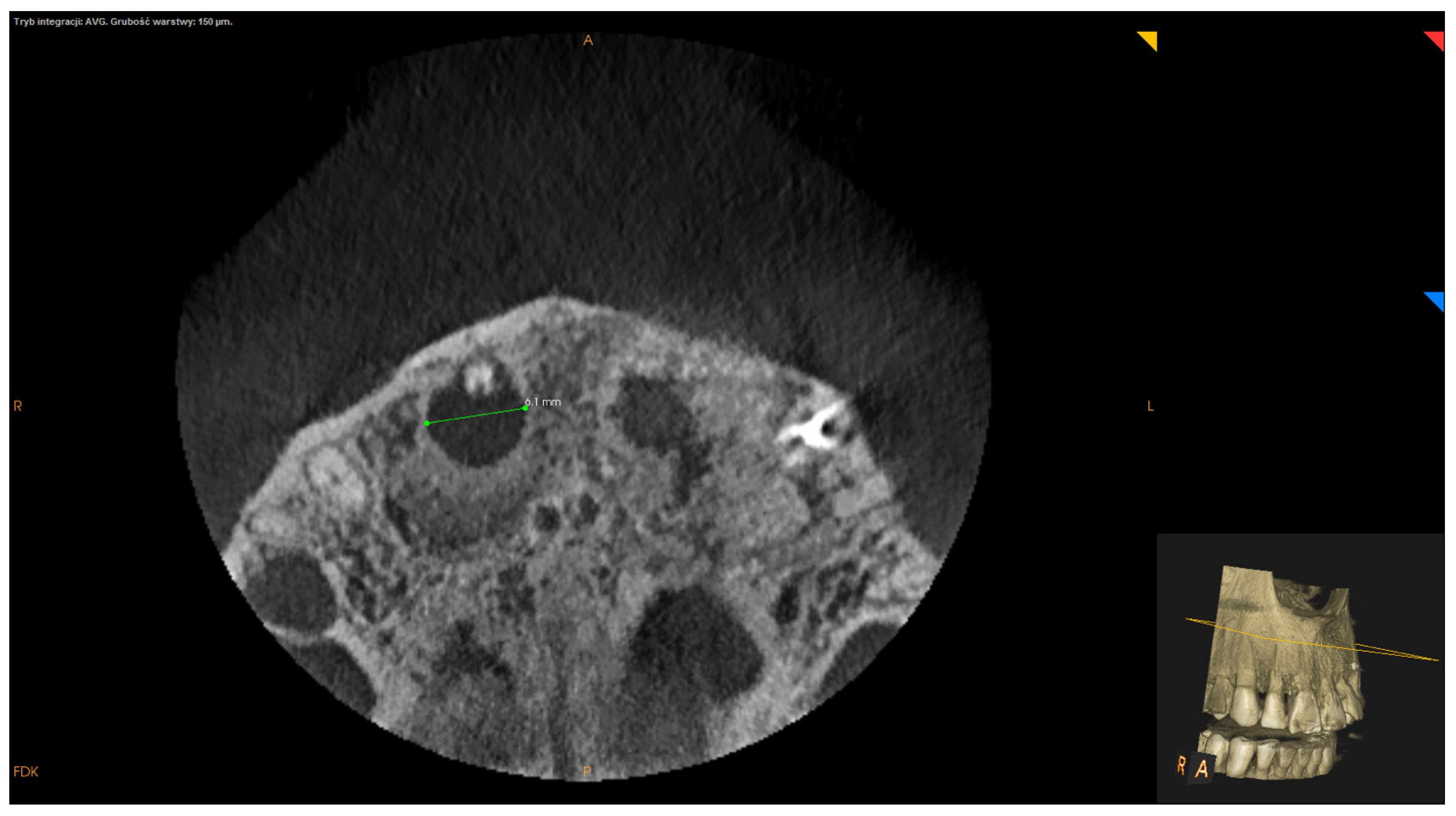
- Mesiodistal maximum diameter (measured in horizontal section) (Figure 4);
- Bone destruction pattern (rated in all sections);
- Presence/absence of cortical bone destruction;
- Height of buccal bone plate (measured in sagittal section);
- Apical extent of root canal filling;
- Presence/absence of communication with anatomical cavities;
- Type of lesion restriction (rated as diffused or demarcated).
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Eriksen, H.M.; Kirkebvang, L.L.; Petersson, K. Endodontic epidemiology and treatment outcome: General considerations. Endod. Top. 2002, 2, 1–9. [Google Scholar] [CrossRef]
- Siqueira, J.F., Jr.; Rocas, I.N. Clinical implications and microbiology of bacterial persistence after treatment procedures. J. Endod. 2008, 34, 1291–1301. [Google Scholar] [CrossRef] [PubMed]
- Kang, M.; Jung, H.I.; Song, M.; Kim, S.Y.; Kim, H.C.; Kim, E. Outcome of nonsurgical pretreatment and endodontic microsurgery; a meta-analysis. Clin. Oral Investig. 2015, 19, 569–582. [Google Scholar] [CrossRef] [PubMed]
- Tsesis, I.; Rosen, E.; Taschieri, S.; Strauss, Y.T.; Ceresoli, V.; Del Fabbro, M. Outcomes of surgical endodontic treatment performed by a modern technique; an updated meta-analysis of the literature. J. Endod. 2013, 39, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Rapp, E.L.; Brown, C.E., Jr.; Newton, C.W. An analysis of success and failure of apicoectomies. J. Endod. 1991, 17, 508–512. [Google Scholar] [CrossRef]
- von Arx, T.; Jenssen, S.S.; Hanni, S.; Friedman, S. Five-year longitudinal assessment of the prognosis of apical microsurgery. J. Endod. 2012, 38, 570–579. [Google Scholar] [CrossRef]
- von Arx, T.; Penarocha, M.; Jenssen, S.S. Prognostic factors in apical surgery with root-end filling: A meta-analysis. J. Endod. 2010, 36, 957–973. [Google Scholar] [CrossRef]
- Del Fabbro, M.; Taschieri, S.; Testori, T.; Rancetti, L.; Weinstein, R.L. Surgical versus non-surgical endodontic re-treatment for periradicular lesions. Cochrane Database Syst. Rev. 2007, 3, CD005511. [Google Scholar] [CrossRef]
- Lui, J.N.; Khin, M.M.; Krishnaswamy, G.; Chen, N.N. Prognostic factors realting to the outcome of endodontic microsurgery. J. Endod. 2014, 40, 1071–1076. [Google Scholar] [CrossRef]
- von Arx, T.; Jenssen, S.S.; Hanni, S. Clinical and radiogarphic assessment of various predictors for healing outcome 1 year after periapical surgery. J. Endod. 2007, 33, 123–128. [Google Scholar] [CrossRef]
- Rahbaran, S.; Gilthorpe, M.S.; Harrison, S.D.; Gulabivala, K. Comparison of clinical outcome of periapical surgery in endodontic and oral surgery units of a teaching dental hospital: A retrospective study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2001, 91, 700–709. [Google Scholar] [CrossRef] [PubMed]
- Wang, N.; Knight, K.; Dao, T.; Friedman, S. Treatment outcome in endodontics—The Toronto study. Phases I and II: Apical surgery. J. Endod. 2004, 30, 751–761. [Google Scholar] [CrossRef] [PubMed]
- Skoglund, A.; Persson, G. A follow-up study of apicoectomized teeth with total loss of buccal bone plate. Oral Surg. Oral Med. Oral Pathol. 1985, 59, 78–81. [Google Scholar] [CrossRef]
- Liao, W.C.; Lee, Y.L.; Tsai, Y.L.; Lin, H.J.; Chang, M.C.; Chang, S.F.; Chang, S.H.; Jeng, J.H. Outcome assessment of apical surgery: A study of 234 teeth. J. Form. Med. Assoc. 2019, 118, 1055–1061. [Google Scholar] [CrossRef] [PubMed]
- Song, M.; Jung, I.Y.; Lee, S.J.; Lee, C.Y.; Kim, E. Prognostic factors for clinical outcomes in endodontic microsurgery: Retrospective study. J. Endod. 2011, 37, 927–933. [Google Scholar] [CrossRef] [PubMed]
- Persson, G. Periapical surgery of molars. Int. J. Oral Surg. 1982, 11, 96–100. [Google Scholar] [CrossRef]
- Cheung, L.K.; Lam, J. Apicoectomy of posterior teeth—A clinical study. Aust. Dent. J. 1993, 38, 17–21. [Google Scholar] [CrossRef]
- Testori, T.; Capelli, M.; Milani, S.; Weinstein, R.L. Success and failure in periradicular surgery. A longitudinal retrospective analysis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1999, 87, 493–498. [Google Scholar] [CrossRef]
- Maddalone, M.; Gagliani, M. Periapical endodontic surgery: A 3 year follow-up study. Int. Endod. J. 2003, 36, 193–198. [Google Scholar] [CrossRef]
- von Arx, T.; Hanni, S.; Jenssen, S.S. Correlation of the bone defect dimensions with healing outcome one year after apical surgery. J. Endod. 2007, 33, 1044–1048. [Google Scholar] [CrossRef]
- Song, M.; Kim, S.G.; Shin, S.J.; Kim, H.C.; Kim, E. The influence of bone tissue deficiency on the outcome of endodontic microsurgery: A retrospective study. J. Endod. 2013, 39, 1341–1345. [Google Scholar] [CrossRef] [PubMed]
- Kreisler, M.; Gockel, R.; Aubell-Falkenberg, S.; Kreisler, T.; Weihe, C.; Filippi, A.; Kuhl, S.; Schultz, S.; d’Hoedt, B. Clinical outcome in periradicular surgery: Effect of patient- and tooth-related factors—A multi center study. Quintessence Int. 2013, 44, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Ku, H.; Nam, T.; Yoon, T.C.; Lee, C.Y.; Kim, E. Influence of size and volume of periapical lesions on the outcome of endodontic microsurgery: 3-dimensional analysis using cone-beam computed tomography. J. Endod. 2016, 42, 1196–1201. [Google Scholar] [CrossRef]
- Taschieri, S.; Del Fabbro, M.; Testori, T.; Weinstein, R. Efficacy of xenogeneic bone grafting with guided tissue regeneration in the management of bone defects after surgical endodontics. J. Oral Maxillofac. Surg. 2007, 65, 1121–1127. [Google Scholar] [CrossRef] [PubMed]
- Elnaghy, A.M. Influence of acidic environment on properties of Biodentine and white mineral trioxide aggregate: A comparative study. J. Endod. 2014, 40, 953–957. [Google Scholar] [CrossRef]
- Bader, G.; Lejeune, S. Prospective study of two retrograde endodontical preparations with and without the use of CO2 laser. Endod. Dent. Traumatol. 1998, 14, 75–78. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, T.; Zunker, P.; Dietrich, D.; Bernimoulin, J.P. Periapical and periodontal healing after osseous grafting and guided tissue regeneration treatment of apicomarginal defects in periradicular surgery: Results after 12 months. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2003, 95, 474–482. [Google Scholar] [CrossRef] [PubMed]
- Tsesis, I.; Rosen, E.; Tamse, A.; Taschieri, S.; Del Fabbro, M. Effect of guided tissue regeneration on the outcome of surgical treatment: A systematic review and meta-analysis. J. Endod. 2011, 37, 1039–1045. [Google Scholar] [CrossRef]
- Barnabe, P.F.; Gomes-Filho, J.E.; Cintra, L.T.; Moretto, M.J.; Lodi, C.S.; Nery, M.J.; Otoboni Filho, J.A.; Dezan, E., Jr. Histologic evaluation of the use of membrane, bone graft, and MTA in apical surgery. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 109, 309–314. [Google Scholar] [CrossRef]
- Garrett, K.; Kerr, M.; Hartwell, G.; O’Sullivan, S.; Mayer, P. The effect of a bioresorbable matrix barrier in endodontic surgery on the rate of periapical healing: An in vivo study. J. Endod. 2002, 28, 503–506. [Google Scholar] [CrossRef]
- Pecora, G.; De Leonardis, D.; Ibrahim, N.; Bovi, M.; Cornelini, R. The use of calcium sulphate in the surgical treatment of a “through & through” periradicular lesions. Int. Endod. J. 2001, 37, 1039–1045. [Google Scholar] [CrossRef]
- Sidiropoulos, K.; Roussou, K.; Intzes, L.; Economides, N. Guided tissue regeneration in surgical endodontic treatment: Case report and literature review. Balk. J. Dent. Med. 2019, 23, 102–107. [Google Scholar] [CrossRef] [Green Version]
- Schloss, T.; Sonntag, D.; Kohle, M.R.; Steuer, F.C. A comparison of 2- and 3-dimensional healing assessment after endodontic surgery using cone-beam computed tomographic volumes or periapical radiographs. J. Endod. 2017, 43, 1072–1079. [Google Scholar] [CrossRef]
- Yushkevich, P.A.; Piven, J.; Hazlett, H.C.; Smith, R.G.; Ho, S.; Gee, J.C.; Gerig, G. User-guided 3D active contour segmentation of anatomical structures: Significantly improved efficiency and reliability. Neuroimage 2006, 31, 1116–1128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rud, J.; Andreasen, J.; Jensen, J.M. Radiographic criteria for the assessment of healing after endodontic surgery. Int. J. Oral Surg. 1972, 1, 195–214. [Google Scholar] [CrossRef]
- Molven, O.; Halse, A.; Grung, B. Observer strategy and the radiographic classification on healing after endodontic surgery. Int. J. Oral Maxillofac. Surg. 1987, 16, 432–439. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing. Available online: http://www.R-project.org/ (accessed on 24 January 2020).
- McGraw, K.O.; Wong, S.P. Forming inferences about some interclass correlation coefficients. Psychol. Methods 1996, 1, 30–46. [Google Scholar] [CrossRef]
- Cohen, J. A coefficient of agreement for nominal scales. Educ. Psychol. Meas. 1960, 1, 37–46. [Google Scholar] [CrossRef]
- Shrout, P.E.; Fleiss, J.L. Interclass correlations: Uses in assessing rater reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef]
- McHugh, M. Interrater Reliability: The Kappa statistic. Biochem. Med. Cas. Hrvat. Drus. Med. Biokem. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Guimard, B.A.; Hoidal, M.J.; Mills, M.P.; Mellonig, J.T.; Nummikoski, P.V.; Mealey, B.L. Comparison of clinical, periapical radiograph, and cone-beam volume tomography measurement techniques for assessing bone level changes following regenerative periodontal theraphy. J. Periodontol. 2009, 80, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Kamburoglu, K.; Kibic, D.; Ozen, T.; Horasan, S. Accuracy of chemically created periodical lesion measurements using limited cone-beam computed tomography. Dentomaxillofac. Radiol. 2010, 39, 95–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, M.; Kim, S.G.; Lee, S.J.; Kim, B.; Kim, E. Prognostic factors of clinical outcomes in endodontic microsurgery: A prospective study. J. Endod. 2013, 39, 1491–1497. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.; Song, J.S.; Jung, I.Y.; Lee, S.J.; Kim, S. Prospective clinical study evaluating endodontic microsurgery outcomes for cases with lesions of endodontic origin compared with cases with lesions of combined periodontal-endodontic origin. J. Endod. 2008, 34, 546–551. [Google Scholar] [CrossRef] [PubMed]
- Song, M.; Kim, E. Success and failure of endodontic microsurgery. J. Korean Acad. Dent. 2011, 36, 465–476. [Google Scholar] [CrossRef] [Green Version]
- Villa-Machado, P.A.; Botero-Ramirez, X.; Tobon-Arroyave, S.I. Retrospective follow-up assessment of prognosis variables associated with the outcome of periradicular surgery. Int. Endod. J. 2013, 46, 1063–1076. [Google Scholar] [CrossRef]
- Nair, P.N. On the causes of persistent apical periodontitis: A review. Int. Endod. J. 2006, 39, 249–281. [Google Scholar] [CrossRef]
- Grung, B.; Molven, O.; Halse, A. Periapical surgery in a Norwegian county hospital: Follow-up findings of 477 teeth. J. Endod. 1990, 16, 411–417. [Google Scholar] [CrossRef]
- Lustmann, J.; Friedman, S.; Shaharabany, V. Relation of pre- and intraoperative factors to prognosis of posterior apical surgery. J. Endod. 1991, 17, 239–241. [Google Scholar] [CrossRef]
- Caliscan, M.K.; Tekin, U.; Kaval, M.E.; Solmaz, M.C. The outcome of apical microsurgery using MTA as a root-end filling material: 2- to 6-year follow-up study. Int. Endod. J. 2016, 49, 245–254. [Google Scholar] [CrossRef]
- Lin, L.; Chen, M.Y.; Ricucci, D.; Rosenberg, P.A. Guided tissue regeneration in apical surgery. J. Endod. 2010, 36, 618–625. [Google Scholar] [CrossRef] [PubMed]
- Wesson, C.M.; Gale, T.M. Molar apicoectomy with amalgam root-end filling: Results of a prospective study in two district general hospitals. Br. Dent. J. 2003, 195, 707–714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jesslen, P.; Zetterqvist, L.; Heimdahl, A. Long-term results of amalgam versus glass ionomer cement as apical sealant after apicoectomy. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1995, 79, 101–103. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | N = 89 | |
|---|---|---|
| Age (years) | mean ± SD | 44.25 ± 10.71 |
| median (range) | 45 (37–52) | |
| Gender | F | 45 (50.56%) |
| M | 44 (49.44%) | |
| Follow-up period [years] | mean ± SD | 2.75 ± 1.33 |
| median (range) | 3 (2–4) | |
| Preoperative activity of the lesion | symptomatic | 44 (49.44%) |
| asymptomatic | 45 (50.56%) | |
| Teeth group | anterior | 54 (60.67%) |
| premolars | 25 (28.09%) | |
| molars | 10 (11.24%) |
| Parameter | N = 89 | |
|---|---|---|
| volume of the lesion M ± SD: 475.51 ± 680.33 | <475.5 mm3 | 66 (74.16%) |
| >475.5 mm3 | 23 (25.84%) | |
| apicocoronal maximum diameter M ± SD: 8.93 ± 3.71 | <8.93 mm | 48 (53.93%) |
| >8.93 mm | 41 (46.07%) | |
| mesiodistal maximum diameter M ± SD: 8.86 ± 4.65 | <8.86 mm | 54 (60.67%) |
| >8.86 mm | 35 (39.33%) | |
| buccolingual maximum diameter M ± SD: 6.91 ± 2.43 | <6.91 mm | 48 (53.93%) |
| >6.91 mm | 41 (46.07%) | |
| bone destruction pattern | apical | 68 (76.40%) |
| apicomarginal | 21 (23.60%) | |
| cortical bone destruction | none | 32 (35.96%) |
| destruction of one of the cortical plates | 49 (55.06%) | |
| destruction of both cortical plates (through and through lesions) | 8 (8.99%) | |
| height of buccal bone plate | <3 mm | 10 (11.24%) |
| >3 mm | 79 (88.76%) | |
| apical extend of root canal filling | 0–2 mm short of apex | 43 (48.31%) |
| >2 mm short of apex | 16 (17.98%) | |
| beyond apex | 30 (33.71%) | |
| communication with anatomical cavities | present | 13 (14.61%) |
| absent (isolated lesions) | 76 (85.39%) | |
| type of lesion restriction | diffused | 44 (49.44%) |
| demarcated | 45 (50.56%) |
| Parameter | Success | OR (95% CI) | p-Value Univariate Logistic Regression | |
|---|---|---|---|---|
| gender | female (N = 45) | 41 (91.11%) | 1.00 | |
| male (N = 44) | 38 (86.36%) | 0.618 (0.162–2.36) | 0.481 | |
| age [years] | 0.939 (0.877–1.006) | 0.072 | ||
| preoperative activity of a lesion | non-active (N = 45) | 44 (97.78%) | 1.00 | |
| active (N = 44) | 35 (79.55%) | 0.088 (0.011–0.731) | 0.024 * | |
| teeth group | anterior (N = 54) | 49 (90.74%) | 1.00 | |
| premolars (N = 25) | 24 (96.00%) | 2.449 (0.271–22.133) | 0.425 | |
| molars (N = 10) | 6 (60.00%) | 0.153 (0.032–0.732) | 0.019 * | |
| follow-up period | years | 0.911 (0.556–1.492) | 0.71 | |
| apicocoronal maximum diameter [mm] | 0.85 (0.721–1.002) | 0.053 | ||
| <8.93 (N = 48) | 45 (93.75%) | 1.00 | ||
| >8.93 (N = 41) | 34 (82.93%) | 0.324 (0.078–1.345) | 0.121 | |
| mesiodistal maximum diameter | mm | 0.953 (0.835–1.088) | 0.475 | |
| <8.86 (N = 54) | 49 (90.74%) | 1.00 | ||
| >8.86 (N = 35) | 30 (85.71%) | 0.612 (0.164–2.292) | 0.466 | |
| buccolingual maximum diameter | mm | 0.824 (0.642–1.057) | 0.128 | |
| <6.91 (N = 48) | 44 (91.67%) | 1.00 | ||
| >6.91 (N = 41) | 35 (85.37%) | 0.53 (0.139–2.027) | 0.354 | |
| volume of a lesion | mm | 1 (0.999–1) | 0.435 | |
| <475.5 (N = 66) | 59 (89.39%) | 1.00 | ||
| >475.5 (N = 23) | 20 (86.96%) | 0.791 (0.187–3.353) | 0.75 | |
| bone destruction pattern | apical (N = 68) | 65 (95.59%) | 1.00 | |
| apicomarginal (N = 21) | 14 (66.67%) | 0.092 (0.021–0.402) | 0.001 * | |
| cortical bone destruction | none (N = 32) | 28 (87.50%) | 1.00 | |
| destruction of one of the cortical plates (N = 49) | 45 (91.84%) | 1.607 (0.372–6.948) | 0.525 | |
| destruction of two plates (N = 8) | 6 (75.00%) | 0.429 (0.063–2.902) | 0.385 | |
| height of buccal bone plate | <3 mm (N = 10) | 8 (80.00%) | 1.00 | |
| >3 mm (N = 79) | 71 (89.87%) | 2.219 (0.4–12.307) | 0.362 | |
| type of lesion restriction | diffused (N = 44) | 37 (84.09%) | 1.00 | |
| demarcated (N = 45) | 42 (93.33%) | 2.649 (0.638–10.989) | 0.18 | |
| communication with anatomical cavities | absent (isolated lesions) (N = 76) | 68 (89.47%) | 1.00 | |
| present (N = 13) | 11 (84.62%) | 0.647 (0.121–3.455) | 0.611 | |
| apical extend of root canal filling | 0–2 mm short of apex (N = 43) | 39 (90.70%) | 1.00 | |
| >2 mm short of apex (N = 16) | 12 (75.00%) | 0.308 (0.067–1.42) | 0.131 | |
| beyond apex (N = 30) | 28 (93.33%) | 1.436 (0.246–8.392) | 0.688 | |
| Parameter | OR (95% CI) | p-Value Multivariate Logistic Regression | |
|---|---|---|---|
| preoperative activity of a lesion | non-active | 1.00 | |
| active | 0.139 (0.011–1.721) | 0.124 | |
| tooth group | anterior | 1.00 | |
| premolars | 0.924 (0.064–13.314) | 0.954 | |
| molars | 0.047 (0.003–0.869) | 0.04 * | |
| bony destruction pattern | apical | 1.00 | |
| apicomarginal | 0.058 (0.006–0.55) | 0.013 * | |
| age | years | 0.919 (0.821–1.029) | 0.143 |
| apicocoronal maximum diameter | mm | 0.664 (0.477–0.926) | 0.016 * |
| Parameter | Success Rate | OR (95% Cl) | p-Value Univariate Logistic Regression | |
|---|---|---|---|---|
| apicomarginal lesions | without GTR (N = 14) | 7 (50.00%) | 1.00 | |
| with GTR (N = 7) | 6 (85.71%) | 6 (0.565–63.676) | 0.137 | |
| lesions of volume >475.5 mm3 | without GTR (N = 10) | 9 (90.00%) | 1.00 | |
| with GTR (N = 13) | 11 (84.62%) | 0.611 (0.047–7.88) | 0.706 | |
| “through and through” lesions | without GTR (N = 3) | 2 (66.67%) | 1.00 | |
| with GTR (N = 5) | 4 (80.00%) | 2 (0.078–51.593) | 0.676 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bieszczad, D.; Wichlinski, J.; Kaczmarzyk, T. Factors Affecting the Success of Endodontic Microsurgery: A Cone-Beam Computed Tomography Study. J. Clin. Med. 2022, 11, 3991. https://doi.org/10.3390/jcm11143991
Bieszczad D, Wichlinski J, Kaczmarzyk T. Factors Affecting the Success of Endodontic Microsurgery: A Cone-Beam Computed Tomography Study. Journal of Clinical Medicine. 2022; 11(14):3991. https://doi.org/10.3390/jcm11143991
Chicago/Turabian StyleBieszczad, Daniel, Jaroslaw Wichlinski, and Tomasz Kaczmarzyk. 2022. "Factors Affecting the Success of Endodontic Microsurgery: A Cone-Beam Computed Tomography Study" Journal of Clinical Medicine 11, no. 14: 3991. https://doi.org/10.3390/jcm11143991
APA StyleBieszczad, D., Wichlinski, J., & Kaczmarzyk, T. (2022). Factors Affecting the Success of Endodontic Microsurgery: A Cone-Beam Computed Tomography Study. Journal of Clinical Medicine, 11(14), 3991. https://doi.org/10.3390/jcm11143991