
Prediction of Intracranial Infection in Patients under External Ventricular Drainage and Neurological Intensive Care: A Multicenter Retrospective Cohort Study


Abstract
1. Introduction
2. Methods
2.1. Study Cohort and Data Acquisition
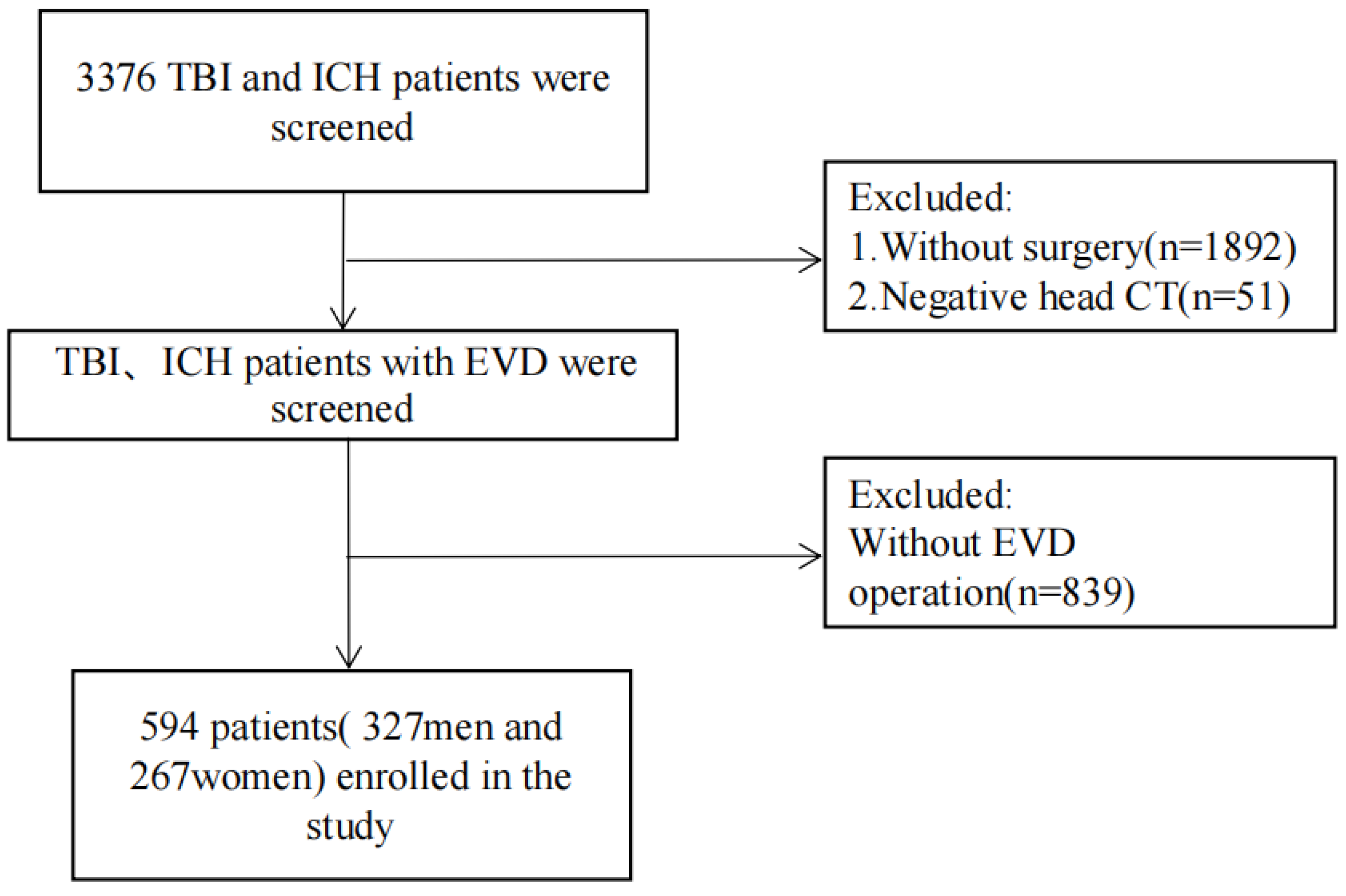
2.2. Inclusion and Exclusion Criteria
2.3. Definitions of EVD-Associated Infections and Length of EVD
2.4. Statistics
2.5. Feature Selection and Machine Learning Algorithms
2.6. Nomogram Construction
3. Results
3.1. Patients Characteristics
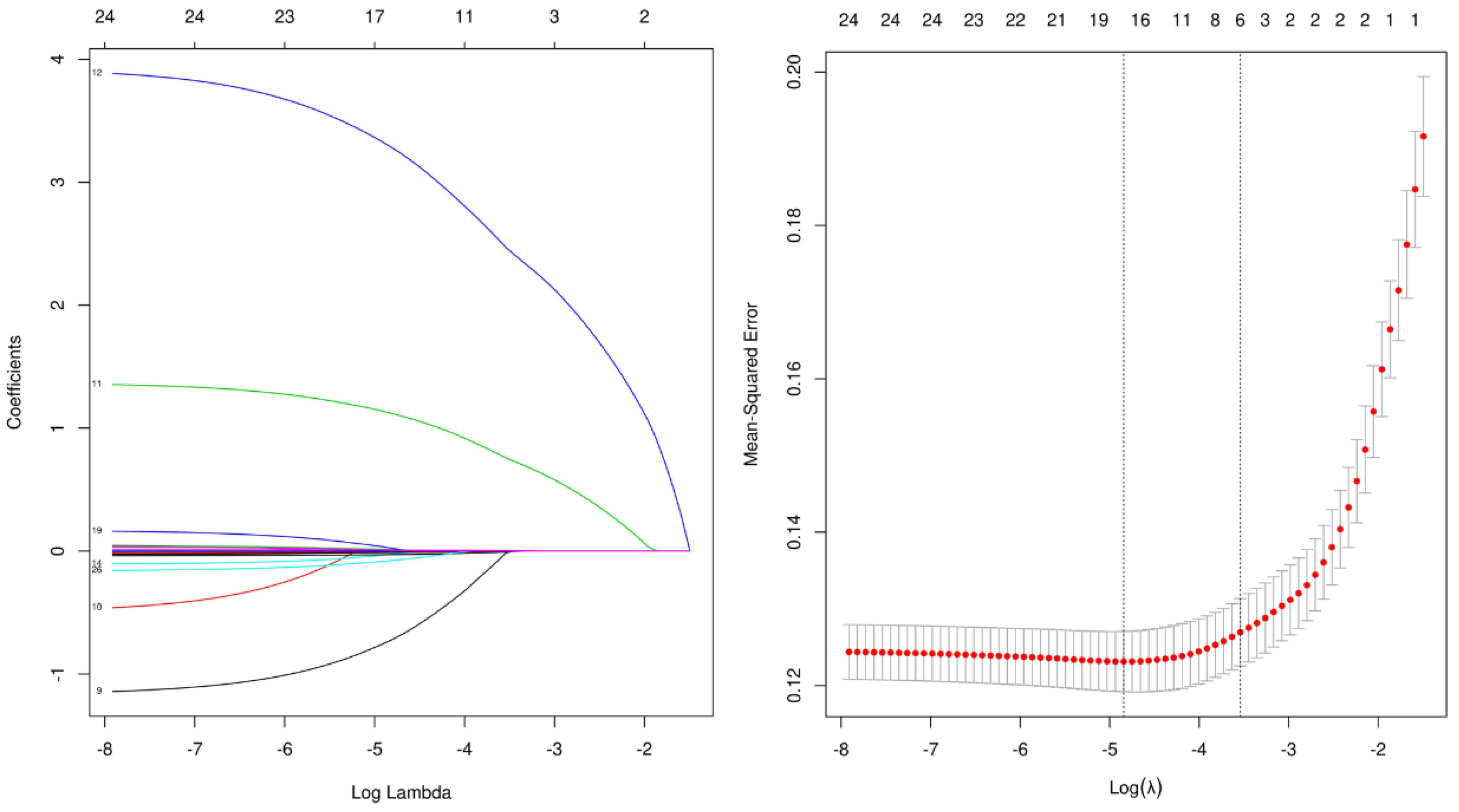
3.2. LASSO Regression and the Logistic Regression Model
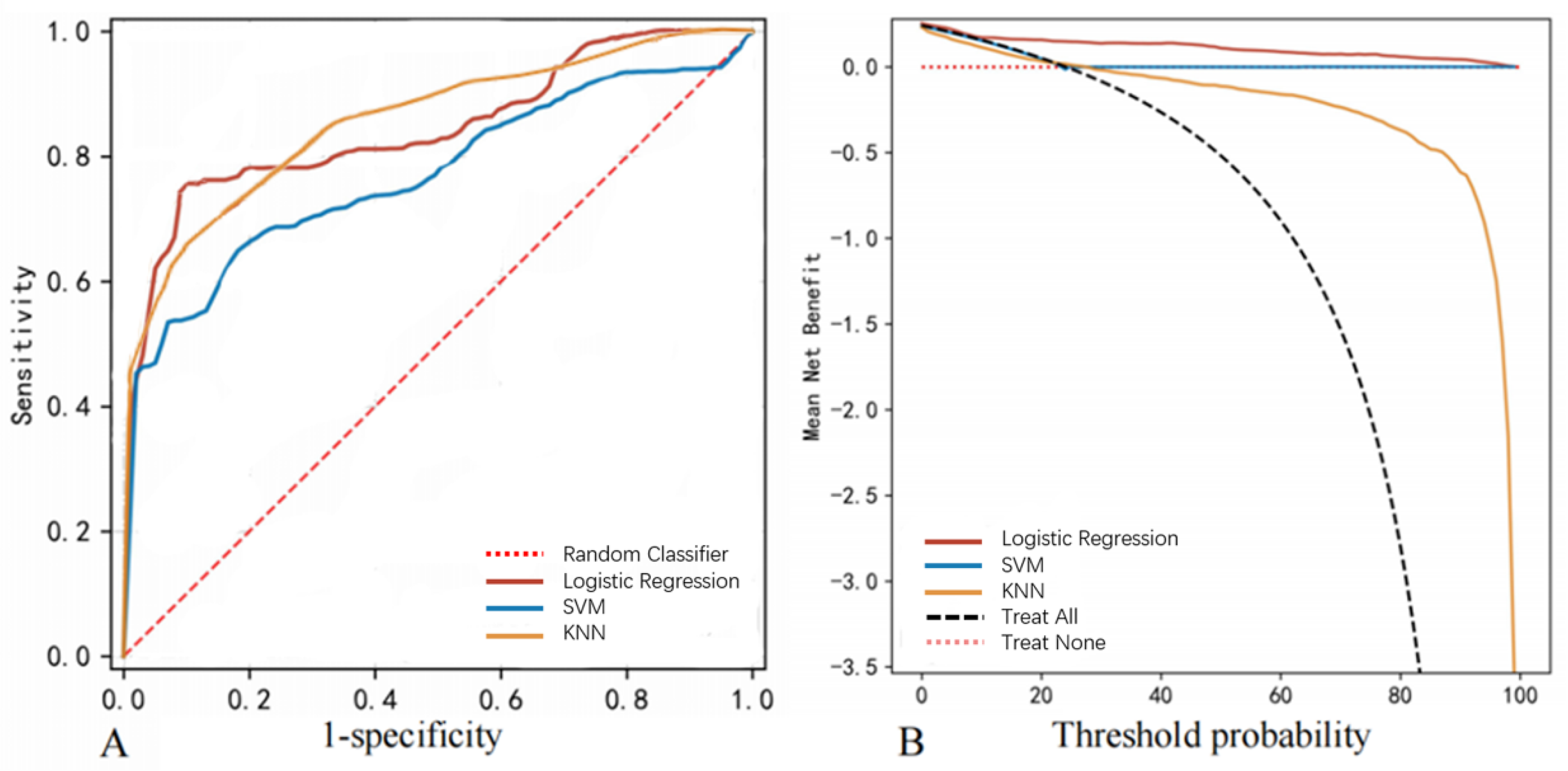
3.3. Models for EVD-Associated Infection Prediction
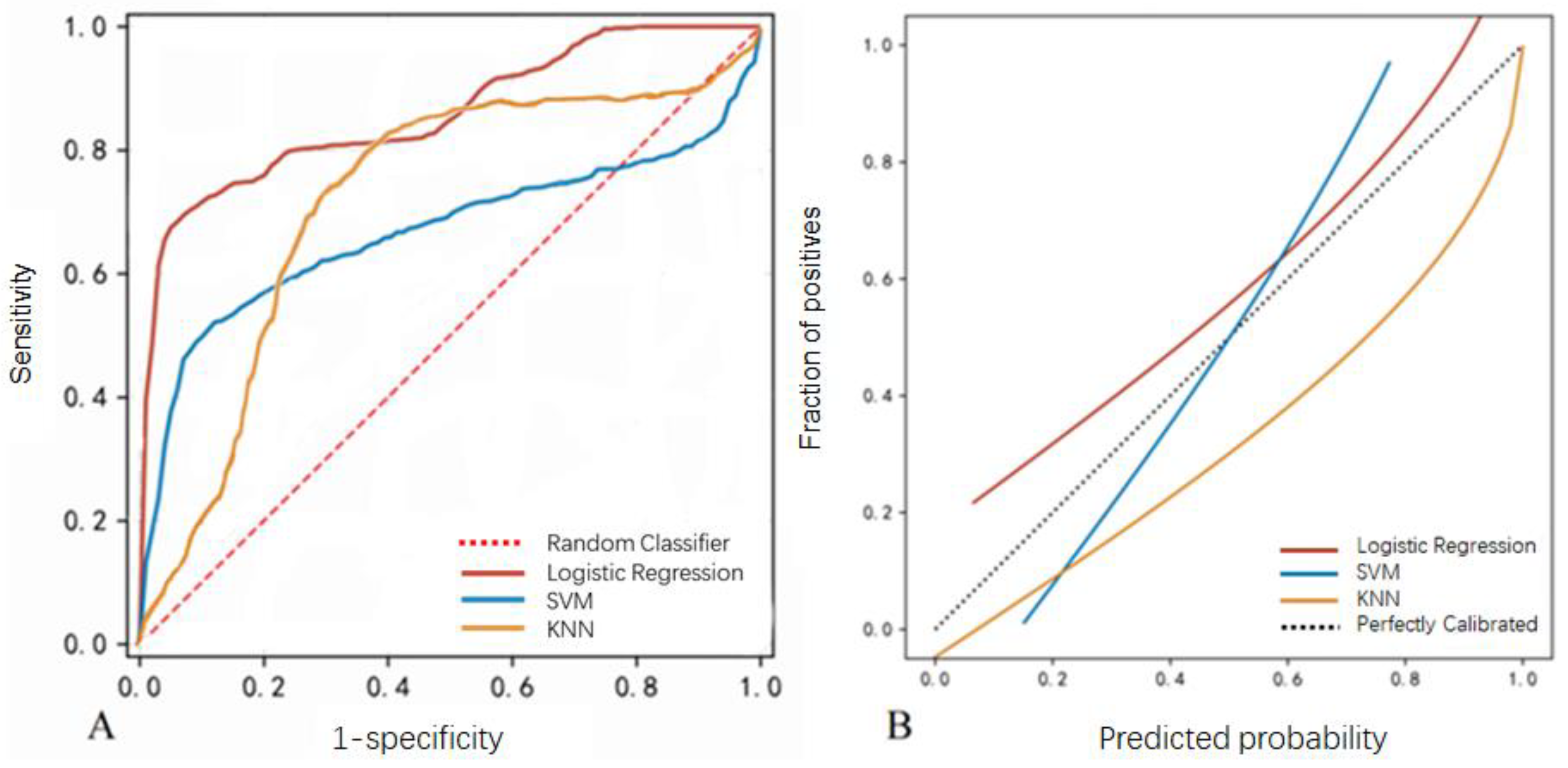
3.4. Model Validation
3.5. Nomogram Analysis for EVD-Associated Intracranial Infections Prediction
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Muralidharan, R. External ventricular drains: Management and complications. Surg. Neurol. Int. 2015, 6 (Suppl. S6), S271–S274. [Google Scholar] [CrossRef] [PubMed]
- Gu, J.C.; Wu, H.; Chen, X.Z.; Feng, J.F.; Gao, G.Y.; Jiang, J.Y.; Mao, Q. Intracranial Pressure during External Ventricular Drainage Weaning Is an Outcome Predictor of Traumatic Brain Injury. BioMed Res. Int. 2020, 2020, 8379134. [Google Scholar] [CrossRef] [PubMed]
- Chung, D.Y.; Mayer, S.A.; Rordorf, G.A. External Ventricular Drains after Subarachnoid Hemorrhage: Is Less More? Neurocrit Care 2018, 28, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Dey, M.; Jaffe, J.; Stadnik, A.; Awad, I.A. External ventricular drainage for intraventricular hemorrhage. Curr. Neurol. Neurosci. Rep. 2012, 12, 24–33. [Google Scholar] [CrossRef] [PubMed]
- Xia, D.; Jiang, X.; Li, Z.; Jin, Y.; Dai, Y. External ventricular drainage combined with continuous lumbar drainage in the treatment of ventricular hemorrhage. Clin. Risk. Manag. 2019, 15, 677–682. [Google Scholar] [CrossRef]
- Winkler, K.M.; Woernle, C.M.; Seule, M.; Held, U.; Bernays, R.L.; Keller, E. Antibiotic-impregnated versus silver-bearing external ventricular drainage catheters: Preliminary results in a randomized controlled trial. Neurocrit. Care 2013, 18, 161–165. [Google Scholar] [CrossRef]
- Chen, H.; Guo, X.; Xie, D.; Dong, X.; Niu, J.; Chen, G. A Clinical Study on the Use of Intraventricular Polymyxin B Supplemented by Continuous External Ventricular Drainage in the Treatment of Drug-Resistant Gram-Negative Bacilli Intracranial Infection. Infect. Drug Resist. 2020, 13, 2963–2970. [Google Scholar] [CrossRef]
- Kirmani, A.R.; Sarmast, A.H.; Bhat, A.R. Role of external ventricular drainage in the management of intraventricular hemorrhage; its complications and management. Surg. Neurol. Int. 2015, 6, 188. [Google Scholar]
- Wondafrash, M.; Tirsit, A. Prevalence of Ventriculostomy Related Infections and Associated Factors in Low Income Setup. Ethiop. J. Health Sci. 2021, 31, 1257–1266. [Google Scholar]
- Sun, C.; Du, H.; Yin, L.; He, M.; Tian, Y.; Li, H. Choice for the removal of bloody cerebrospinal fluid in postcoiling aneurysmal subarachnoid hemorrhage: External ventricular drainage or lumbar drainage? Turk. Neurosurg. 2014, 24, 737–744. [Google Scholar]
- Mo, R.; Shi, R.; Hu, Y.; Hu, F. Nomogram-Based Prediction of the Risk of Diabetic Retinopathy: A Retrospective Study. J. Diabetes Res. 2020, 2020, 7261047. [Google Scholar] [CrossRef] [PubMed]
- Chau, C.Y.C.; Craven, C.L.; Rubiano, A.M.; Adams, H.; Tulu, S.; Czosnyka, M.; Servadei, F.; Ercole, A.; Hutchinson, P.J.; Kolias, A.G. The Evolution of the Role of External Ventricular Drainage in Traumatic Brain Injury. J. Clin. Med. 2019, 8, 1422. [Google Scholar] [CrossRef] [PubMed]
- Woernle, C.M.; Burkhardt, J.K.; Bellut, D.; Krayenbuehl, N.; Bertalanffy, H. Do iatrogenic factors bias the placement of external ventricular catheters?—A single institute experience and review of the literature. Neurol. Med. Chir. 2011, 51, 180–186. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Karvouniaris, M.; Brotis, A.; Tsiakos, K.; Palli, E.; Koulenti, D. Current Perspectives on the Diagnosis and Management of Healthcare-Associated Ventriculitis and Meningitis. Infect. Drug Resist. 2022, 15, 697–721. [Google Scholar] [CrossRef] [PubMed]
- Qian, C.; Yu, X.; Chen, J.; Gu, C.; Wang, L.; Chen, G.; Dai, Y. Effect of the drainage of cerebrospinal fluid in patients with aneurismal subarachnoid hemorrhage: A meta-analysis. Medicine 2016, 95, e5140. [Google Scholar] [CrossRef]
- Sridhar, K.; Karmarkar, V. Peroral extrusion of ventriculoperitoneal shunt: Case report and review of literature. Neurol. India 2009, 57, 334–336. [Google Scholar] [CrossRef]
- Conen, A.; Raabe, A.; Schaller, K.; Fux, C.A.; Vajkoczy, P.; Trampuz, A. Management of neurosurgical implant-associated infections. Swiss Med. Wkly. 2020, 150, w20208. [Google Scholar] [CrossRef] [PubMed]
- Han, H.; Li, Y.; Liu, L.; Liu, N.; Wang, Y.; Zhang, M. The risk factors of intracranial infection in patients with intracerebral hemorrhage undergone hematoma puncture: What should we care. BMC Infect. Dis. 2020, 20, 949. [Google Scholar] [CrossRef]
- Zhao, J.; Zhao, X.; Yang, S.; Miao, S.; Liu, Y. Surgical treatment and operation time in human immunodeficiency virus-negative cryptococcal meningitis. Medicine 2020, 99, e22546. [Google Scholar] [CrossRef]
- Balachandran, V.P.; Gonen, M.; Smith, J.J.; DeMatteo, R.P. Nomograms in oncology: More than meets the eye. Lancet Oncol. 2015, 16, e173–e180. [Google Scholar] [CrossRef]
- Merry, E.; Thway, K.; Jones, R.L.; Huang, P.H. Predictive and prognostic transcriptomic biomarkers in soft tissue sarcomas. NPJ Precis. Oncol. 2021, 5, 17. [Google Scholar] [CrossRef] [PubMed]
- Mayhew, D.; Mendonca, V.; Murthy, B.V.S. A review of ASA physical status—Historical perspectives and modern developments. Anaesthesia 2019, 74, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Hurwitz, E.E.; Simon, M.; Vinta, S.R.; Zehm, C.F.; Shabot, S.M.; Minhajuddin, A.; Abouleish, A.E. Adding Examples to the ASA-Physical Status Classification Improves Correct Assignment to Patients. Anesthesiology 2017, 126, 614–622. [Google Scholar] [CrossRef] [PubMed]
- Prabhakar, H.; Sandhu, K.; Bhagat, H.; Durga, P.; Chawla, R. Current concepts of optimal cerebral perfusion pressure in traumatic brain injury. J. Anaesthesiol. Clin. Pharm. 2014, 30, 318–327. [Google Scholar]
- East, J.M.; Viau-Lapointe, J.; McCredie, V.A. Transfusion practices in traumatic brain injury. Curr. Opin. Anaesthesiol. 2018, 31, 219–226. [Google Scholar] [CrossRef]
- Suchdev, P.S.; Williams, A.M.; Mei, Z.; Flores-Ayala, R.; Pasricha, S.R.; Rogers, L.M.; Namaste, S.M. Assessment of iron status in settings of inflammation: Challenges and potential approaches. Am. J. Clin. Nutr. 2017, 106 (Suppl. S6), 1626s–1633s. [Google Scholar] [CrossRef]
- Griswold, D.P.; Fernandez, L.; Rubiano, A.M. Traumatic Subarachnoid Hemorrhage: A Scoping Review. J. Neurotrauma 2022, 39, 35–48. [Google Scholar] [CrossRef]
- Figueira Rodrigues Vieira, G.; Guedes Correa, J.F. Early computed tomography for acute post-traumatic diffuse axonal injury: A systematic review. Neuroradiology 2020, 62, 653–660. [Google Scholar] [CrossRef]
- Ziai, W.C.; Thompson, C.B.; Mayo, S.; McBee, N.; Freeman, W.D.; Dlugash, R.; Ullman, N.; Hao, Y.; Lane, K.; Awad, I.; et al. Clot Lysis: Evaluating Accelerated Resolution of Intraventricular Hemorrhage, I. Intracranial Hypertension and Cerebral Perfusion Pressure Insults in Adult Hypertensive Intraventricular Hemorrhage: Occurrence and Associations with Outcome. Crit. Care Med. 2019, 47, 1125–1134. [Google Scholar] [CrossRef]
- Luo, H.C.; Fu, Y.Q.; You, C.Y.; Liu, C.J.; Xu, F. Comparison of admission serum albumin and hemoglobin as predictors of outcome in children with moderate to severe traumatic brain injury: A retrospective study. Medicine 2019, 98, e17806. [Google Scholar] [CrossRef]
- Vasudevan, A.; Mukhopadhyay, A.; Li, J.; Yuen, E.G.; Tambyah, P.A. A prediction tool for nosocomial multi-drug Resistant Gram-Negative Bacilli infections in critically ill patients—Prospective observational study. BMC Infect. Dis. 2014, 14, 615. [Google Scholar] [CrossRef] [PubMed]
- Bjornson, A.; Tajsic, T.; Kolias, A.G.; Wells, A.; Naushahi, M.J.; Anwar, F.; Helmy, A.; Timofeev, I.; Hutchinson, P.J. A case series of early and late cranioplasty-comparison of surgical outcomes. Acta Neurochir. 2019, 161, 467–472. [Google Scholar] [CrossRef] [PubMed]
- Boles, A.; Kandimalla, R.; Reddy, P.H. Dynamics of diabetes and obesity: Epidemiological perspective. Biochim. Biophys. Acta Mol. Basis Dis. 2017, 1863, 1026–1036. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, M.; Chakraborty, S.; Pal, R. Diabetes self-management amid COVID-19 pandemic. Diabetes Metab. Syndr. 2020, 14, 351–354. [Google Scholar] [CrossRef] [PubMed]
- Berbudi, A.; Rahmadika, N.; Tjahjadi, A.I.; Ruslami, R. Type 2 Diabetes and its Impact on the Immune System. Curr. Diabetes Rev. 2020, 16, 442–449. [Google Scholar] [CrossRef]
- Daryabor, G.; Atashzar, M.R.; Kabelitz, D.; Meri, S.; Kalantar, K. The Effects of Type 2 Diabetes Mellitus on Organ Metabolism and the Immune System. Front. Immunol. 2020, 11, 1582. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | With EVD-Associated Intracranial Infections (n = 143) | Without EVD-Associated Intracranial Infections (n = 451) | p |
|---|---|---|---|
| Clinical characteristics | |||
| Gender (Male) | 77 (53.85%) | 262 (58.09%) | 0.36 |
| Age (years) | 54.08 (15.16) | 55.28 (14.38) | 0.39 |
| BMI | 23.22 (3.85) | 23.48 (3.64) | 0.48 |
| History of diabetes | 107 (74.83%) | 337 (74.72%) | <0.01 |
| ASA grades | 3.04 (0.94) | 2.25 (0.84) | <0.01 |
| BP on admission (mmHg) | 140.96 (12.30) | 142.12 (12.55) | 0.34 |
| GCS 3–8 (n, %) | 21 (14.69%) | 70 (15.52%) | 0.81 |
| GCS 9–12 (n, %) | 28 (19.58%) | 87 (19.29%) | 0.94 |
| GCS 13–15 (n, %) | 94 (65.73%) | 294 (65.19%) | 0.91 |
| Preoperative intubation (n, %) | 32 (22.38%) | 84 (18.63%) | 0.32 |
| Lopt (minutes) | 146.3 (92.44) | 126.44 (79.85) | 0.02 |
| Cases underwent operations in addition to EVD (n, %) | 62 (43.36%) | 175 (38.80%) | 0.33 |
| Diagnosis and complications | |||
| Hydrocephalus (n, %) | 17 (11.89%) | 56 (12.42%) | 0.87 |
| Spontaneous ICH (n, %) | 95 (66.43%) | 221 (49.00%) | <0.01 |
| Traumatic brain injury (n, %) | 62 (43.36%) | 143 (31.71%) | 0.01 |
| Skull fracture (n, %) | 41 (28.67%) | 136 (30.16%) | <0.01 |
| tSAH (n, %) | 69 (48.25%) | 146 (32.37%) | <0.01 |
| CSF leakage due to trauma (n, %) | 9 (6.29%) | 27 (5.99%) | <0.01 |
| Nonintracranial infections (n, %) | 12 (8.39%) | 28 (6.21%) | 0.36 |
| First laboratory tests | |||
| RBC (1012/L) | 4.49 (0.89) | 4.50 (0.83) | 0.88 |
| HB (g/L) | 75.28 (61.83) | 117.85 (32.26) | <0.01 |
| WBC (109/L) | 13.64 (4.24) | 12.88 (5.15) | 0.08 |
| NEUT (%) | 86.01 (6.21) | 83.83 (10.58) | <0.01 |
| PLT (109/L) | 200.86 (65.21) | 202.49 (68.66) | 0.8 |
| TBIL (μmol/L) | 12.28 (6.92) | 11.39 (6.84) | 0.18 |
| DBIL(μml/L) | 5.15 (2.91) | 4.94 (2.83) | 0.44 |
| ALT (U/L) | 43.17 (38.24) | 33.12 (23.60) | <0.01 |
| AST (U/L) | 43.23 (27.85) | 38.32 (29.57) | 0.15 |
| LDH (U/L) | 206.94 (69.11) | 205.53 (64.56) | 0.82 |
| HDL (mmol/L) | 1.93 (0.59) | 1.96 (0.62) | 0.62 |
| LDL (mmol/L) | 2.93 (1.15) | 2.97 (1.15) | 0.77 |
| Ch (μml/L) | 5.07 (1.18) | 5.03 (1.15) | 0.75 |
| Ab (g/L) | 33.27 (7.22) | 43.74 (4.62) | <0.01 |
| GLB (g/L) | 30.71 (6.62) | 32.02 (7.61) | 0.01 |
| BUN (mmol/L) | 6.09 (1.77) | 6.05 (1.76) | 0.79 |
| UA (mmol/L) | 261.83 (101.63) | 250.59 (94.69) | 0.23 |
| SCR (μmol/L) | 5.87 (1.21) | 6.03 (1.18) | 0.16 |
| Postoperative EVD monitoring | |||
| Length of EVD (days) | 9.15 (4.52) | 6.85 (3.48) | 0.045 |
| Number of CSF sampling (per week) | 3.07 (1.41) | 3.00 (1.41) | 0.62 |
| Leakage from EVD site (n, %) | 20 (13.99%) | 23 (5.10%) | <0.01 |
| Outcomes | |||
| ICU length of stays (days) | 14.29 (6.91) | 5.93 (2.96) | <0.01 |
| Hospital stays (days) | 24.49 (3.62) | 11.25 (3.75) | <0.01 |
| In-hospital mortality (n, %) | 47 (32.87%) | 26 (5.76%) | <0.01 |
| Models | Features | Weight |
|---|---|---|
| Logistic Regression | ASA grades | 0.37 |
| HB | 0.24 | |
| History of diabetes | 0.19 | |
| tSAH | 0.092 | |
| Lopt | 0.087 | |
| Ab | 0.068 | |
| SVM | HB | 0.31 |
| ASA grades | 0.29 | |
| Ab | 0.18 | |
| Lopt | 0.16 | |
| History of diabetes | 0.13 | |
| Length of EVD | 0.076 | |
| KNN | ASA grades | 0.37 |
| HB | 0.17 | |
| ALT | 0.16 | |
| Lopt | 0.14 | |
| Ab | 0.095 | |
| Leakage from EVD site | 0.075 |
| Classification Model | AUC | Cut-Off | Accuracy | Sensitivity | Specificity | Positive Predictive Value | Negative Predictive Value | F1 Score |
|---|---|---|---|---|---|---|---|---|
| Logistic regression | 0.846 (0.006) | 0.305 (0.016) | 0.870 (0.004) | 0.761 (0.010) | 0.970 (0.005) | 0.715 (0.011) | 0.921 (0.003) | 0.737 (0.008) |
| SVM | 0.730 (0.008) | 0.191 (0.100) | 0.792 (0.029) | 0.646 (0.059) | 0.845 (0.054) | 0.575 (0.097) | 0.879 (0.009) | 0.599 (0.018) |
| KNN | 0.845 (0.003) | 0.400 (0.001) | 0.887 (0.005) | 0.931 (0.014) | 0.817 (0.012) | 0.828 (0.021) | 0.901 (0.007) | 0.876 (0.012) |
| Classification Model | AUC | Cut-Off | Accuracy | Sensitivity | Specificity | Positive Predictive Value | Negative Predictive Value | F1 Score |
|---|---|---|---|---|---|---|---|---|
| Logistic regression | 0.847 (0.097) | 0.305 (0.016) | 0.869 (0.050) | 0.787 (0.145) | 0.923 (0.058) | 0.714 (0.094) | 0.924 (0.048) | 0.743 (0.101) |
| SVM | 0.677 (0.111) | 0.191 (0.100) | 0.758 (0.069) | 0.698 (0.174) | 0.875 (0.135) | 0.521 (0.140) | 0.856 (0.050) | 0.585 (0.122) |
| KNN | 0.844 (0.072) | 0.400 (0.000) | 0.829 (0.053) | 0.833 (0.136) | 0.747 (0.156) | 0.730 (0.170) | 0.859 (0.051) | 0.757 (0.100) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fu, P.; Zhang, Y.; Zhang, J.; Hu, J.; Sun, Y. Prediction of Intracranial Infection in Patients under External Ventricular Drainage and Neurological Intensive Care: A Multicenter Retrospective Cohort Study. J. Clin. Med. 2022, 11, 3973. https://doi.org/10.3390/jcm11143973
Fu P, Zhang Y, Zhang J, Hu J, Sun Y. Prediction of Intracranial Infection in Patients under External Ventricular Drainage and Neurological Intensive Care: A Multicenter Retrospective Cohort Study. Journal of Clinical Medicine. 2022; 11(14):3973. https://doi.org/10.3390/jcm11143973
Chicago/Turabian StyleFu, Pengfei, Yi Zhang, Jun Zhang, Jin Hu, and Yirui Sun. 2022. "Prediction of Intracranial Infection in Patients under External Ventricular Drainage and Neurological Intensive Care: A Multicenter Retrospective Cohort Study" Journal of Clinical Medicine 11, no. 14: 3973. https://doi.org/10.3390/jcm11143973
APA StyleFu, P., Zhang, Y., Zhang, J., Hu, J., & Sun, Y. (2022). Prediction of Intracranial Infection in Patients under External Ventricular Drainage and Neurological Intensive Care: A Multicenter Retrospective Cohort Study. Journal of Clinical Medicine, 11(14), 3973. https://doi.org/10.3390/jcm11143973