
Therapeutic Efficacy and Safety of Osteoinductive Factors and Cellular Therapies for Long Bone Fractures and Non-Unions: A Meta-Analysis and Systematic Review

 ,
,  ,
,  ,
,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Research Strategy
2.2. Inclusion Criteria and Study Selection
2.3. Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. Search Results
3.2. Clinical Application of Osteoinductive Factors
3.3. Statistical Results
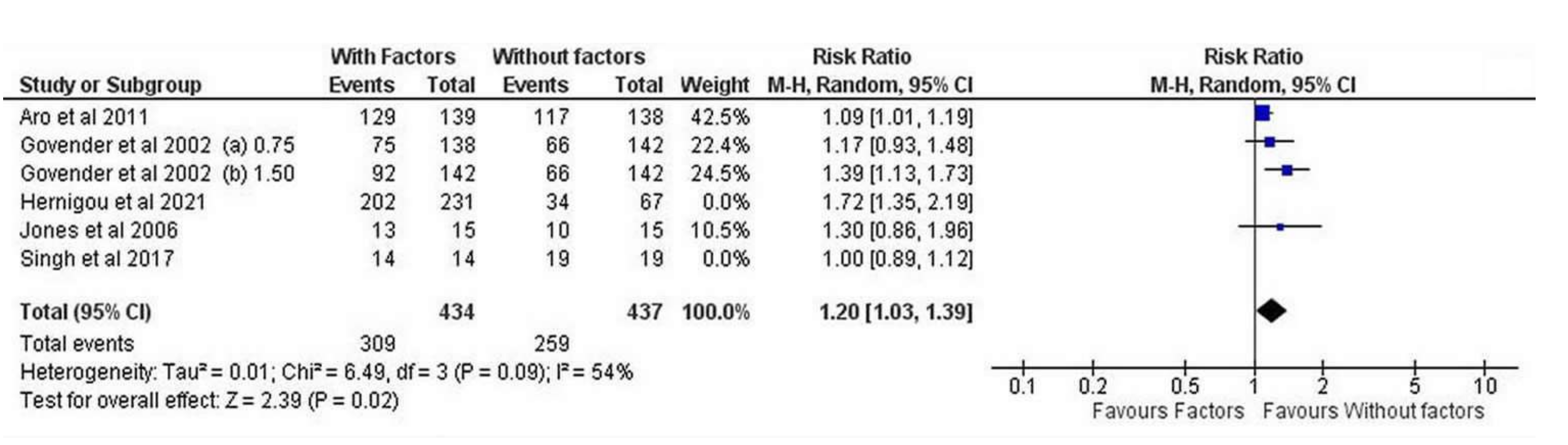
3.3.1. Overall Effectiveness
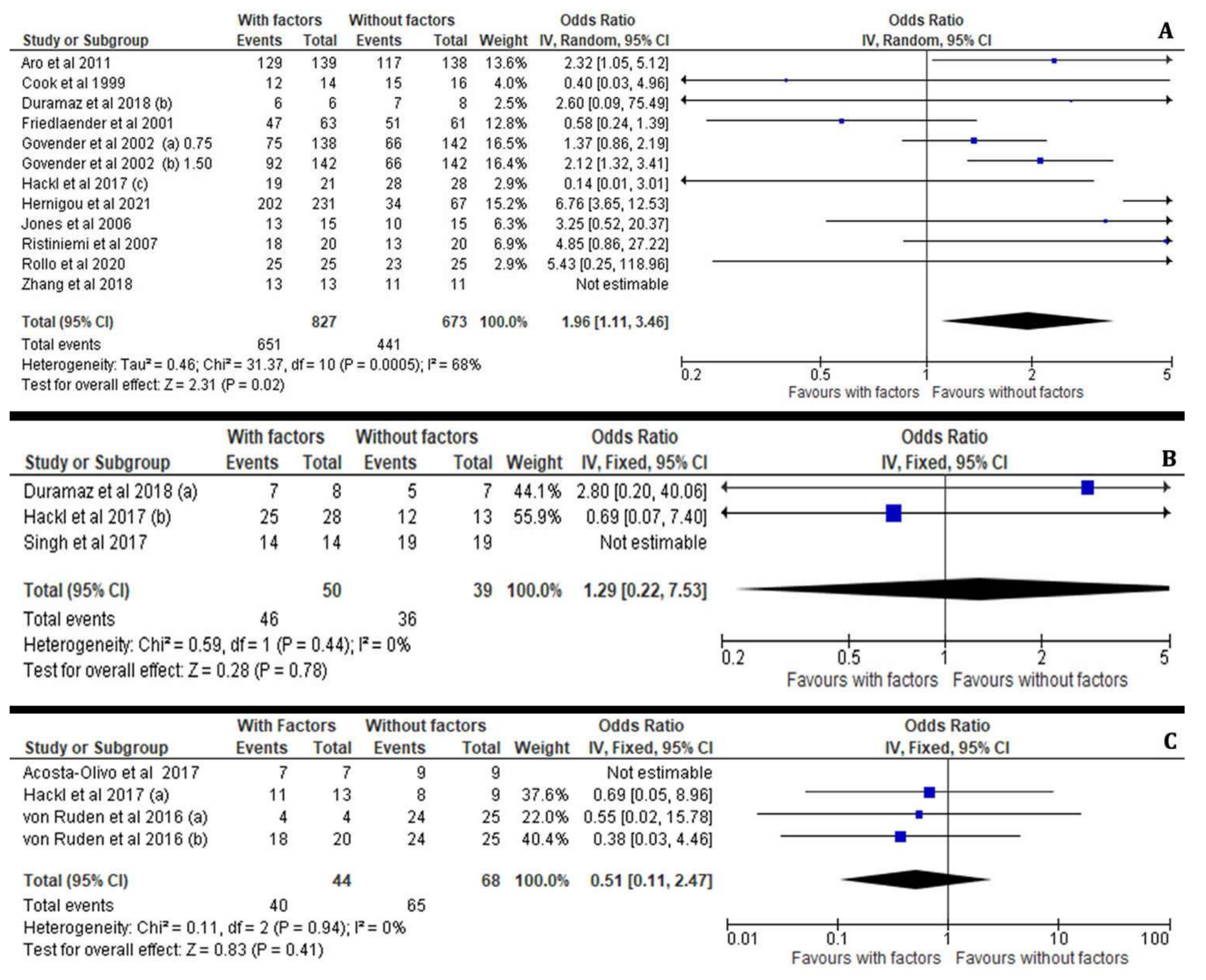
3.3.2. Subgroup Effectiveness Analysis (MCSs, PRP, BMP-7, BMP-2)
3.3.3. Persistent Non-Unions and Re-Fractures after the Application of Osteoinductive Growth Factors
3.3.4. Osteoinductive Factors, Fixation Technique and Fracture Location
4. Discussion
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
References
- Mock, C.; Cherian, M.N. The Global Burden of Musculoskeletal Injuries: Challenges and Solutions. Clin. Orthop. Relat. Res. 2008, 466, 2306–2316. [Google Scholar] [CrossRef]
- Meling, T.; Harboe, K.; Søreide, K. Incidence of traumatic long-bone fractures requiring in-hospital management: A prospective age- and gender-specific analysis of 4890 fractures. Injury 2009, 40, 1212–1219. [Google Scholar] [CrossRef]
- Nakase, T.; Kawai, H.; Yoshikawa, H. In Situ Grafting of Excised Fracture Callus Followed by Ilizarov External Fixation for Treatment of Nonunion After Open Fracture of Tibia. J. Trauma Inj. Infect. Crit. Care 2009, 66, 550–553. [Google Scholar] [CrossRef] [PubMed]
- Peters, R.M.; Claessen, F.M.; Doornberg, J.N.; Kolovich, G.P.; Diercks, R.L.; Bekerom, M.P.V.D. Union rate after operative treatment of humeral shaft nonunion—A systematic review. Injury 2015, 46, 2314–2324. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Szabo, R.M.; Marder, R.A. Epidemiology of humerus fractures in the United States: Nationwide emergency department sample, 2008. Arthritis Care Res. 2012, 64, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Rupp, M.; Biehl, C.; Budak, M.; Thormann, U.; Heiss, C.; Alt, V. Diaphyseal long bone nonunion—Types, aetiology, economics, and treatment recommendations. Int. Orthop. 2018, 42, 247–258. [Google Scholar] [CrossRef]
- Mills, L.A.; Aitken, S.A.; Simpson, A.H.R.W. The risk of non-union per fracture: Current myths and revised figures from a population of over 4 million adults. Acta Orthop. 2017, 88, 434–439. [Google Scholar] [CrossRef] [PubMed]
- Mills, L.A.; Simpson, A.H.R.W. The relative incidence of fracture non-union in the Scottish population (5.17 million): A 5-year epidemiological study. BMJ Open 2013, 3, e002276. [Google Scholar] [CrossRef] [PubMed]
- Hak, D.J.; Fitzpatrick, D.; Bishop, J.A.; Marsh, J.L.; Tilp, S.; Schnettler, R.; Simpson, H.; Alt, V. Delayed union and nonunions: Epidemiology, clinical issues, and financial aspects. Injury 2014, 45 (Suppl. S2), S3–S7. [Google Scholar] [CrossRef] [PubMed]
- Investigators SPERINPTF; Bhandari, M.; Guyatt, G.; Tornetta, P.; Schemitsch, E.H., 3rd; Swiontkowski, M.; Sanders, D.; Walter, S.D. Randomized trial of reamed and unreamed intramedullary nailing of tibial shaft fractures. J. Bone Jt. Surg. Am. 2008, 90, 2567–2578. [Google Scholar] [CrossRef] [PubMed]
- Canadian Orthopaedic Trauma Society. Nonunion following intramedullary nailing of the femur with and without reaming. Results of a multicenter randomized clinical trial. J. Bone Jt. Surg Am. 2006, 88, 2613–2623. [Google Scholar]
- Court-Brown, C.M. Reamed intramedullary tibial nailing: An overview and analysis of 1106 cases. J. Orthop. Trauma 2004, 18, 96–101. [Google Scholar] [CrossRef]
- Biz, C.; Crimì, A.; Fantoni, I.; Vigo, M.; Iacobellis, C.; Ruggieri, P. Functional outcome and complications after treatment of comminuted tibial fractures or deformities using Ilizarov bone transport: A single-center study at 15- to 30-year follow-up. Arch. Orthop. Trauma Surg. 2021, 141, 1825–1833. [Google Scholar] [CrossRef] [PubMed]
- Dumic-Cule, I.; Peric, M.; Kucko, L.; Grgurevic, L.; Pecina, M.; Vukicevic, S. Bone morphogenetic proteins in fracture repair. Int. Orthop. 2018, 42, 2619–2626. [Google Scholar] [CrossRef]
- Wu, S.; Quan, K.; Mei, J.; Dai, M.; Song, S. Cortical allograft strut augmented with platelet-rich plasma for the treatment of long bone non-union in lower limb—A pilot study. BMC Musculoskelet. Disord. 2022, 23, 512. [Google Scholar] [CrossRef] [PubMed]
- Andersen, C.; Wragg, N.M.; Shariatzadeh, M.; Wilson, S.L. The Use of Platelet-Rich Plasma (PRP) for the Management of Non-union Fractures. Curr. Osteoporos. Rep. 2021, 19, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Barrena, E.; Eguiluz, N.G.P.; García-Rey, E.; Hernández-Esteban, P.; Cordero-Ampuero, J.; Rubio-Suárez, J.C.; RE-BORNE and ORTHOUNION Research Consortia. Validation of a long bone fracture non-union healing score after treatment with mesenchymal stromal cells combined to biomaterials. Injury 2020, 51, S55–S62. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses. Ottawa Health Research Institute. 2000. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.htm (accessed on 15 October 2021).
- Oremus, M.; Wolfson, C.; Perrault, A.; Demers, L.; Momoli, F.; Moride, Y. Interrater Reliability of the Modified Jadad Quality Scale for Systematic Reviews of Alzheimer’s Disease Drug Trials. Dement. Geriatr. Cogn. Disord. 2001, 12, 232–236. [Google Scholar] [CrossRef]
- Hernigou, P.; Housset, V.; Dubory, A.; Rouard, H.; Auregan, J.C. Early injection of autologous bone marrow concentrates decreases infection risk and improves healing of acute severe open tibial fractures. Injury 2020, S0020-1383(20)31035-4. [Google Scholar] [CrossRef] [PubMed]
- Başdelioğlu, K.; Meriç, G.; Sargın, S.; Atik, A.; Ulusal, A.E.; Akseki, D. The effect of platelet-rich plasma on fracture healing in long-bone pseudoarthrosis. Eur. J. Orthop. Surg. Traumatol. 2020, 30, 1481–1486. [Google Scholar] [CrossRef]
- Rollo, G.; Bonura, E.M.; Falzarano, G.; Bisaccia, M.; Ribes Iborra, J.; Grubor, P.; Filipponi, M.; Pichierri, P.; Hitov, P.; Leonetti, D.; et al. Platet Rich Plasma or Hyperbaric Oxygen Therapy as callus accellerator in aseptic tibial non-union. Eval. Outcomes. Acta Biomed. 2020, 91, e2020188. [Google Scholar]
- Wang, X.; Chu, W.; Zhuang, Y.; Shi, D.; Tao, H.; Jin, C.; Dai, K.; Zhao, J.; Gan, Y. Bone Mesenchymal Stem Cell-Enriched β-Tricalcium Phosphate Scaffold Processed by the Screen-Enrich-Combine Circulating System Promotes Regeneration of Diaphyseal Bone Non-Union. Cell Transplant. 2018, 28, 212–223. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Xue, F.; Xiao, H.J. Ilizarov method in combination with autologous mesenchymal stem cells from iliac crest shows improved outcome in tibial non-union. Saudi J. Biol. Sci. 2016, 25, 819–825. [Google Scholar] [CrossRef]
- Duramaz, A.; Ursavaş, H.T.; Bilgili, M.G.; Bayrak, A.; Bayram, B.; Avkan, M.C. Platelet-rich plasma versus exchange intramedullary nailing in treatment of long bone oligotrophic nonunions. Eur. J. Orthop. Surg. Traumatol. 2018, 28, 131–137. [Google Scholar] [CrossRef]
- Singh, R.; Bleibleh, S.; Kanakaris, N.K.; Giannoudis, P.V. Upper limb non-unions treated with BMP-7: Efficacy and clinical results. Injury 2016, 47 (Suppl. S6), S33–S39. [Google Scholar] [CrossRef]
- Acosta-Olivo, C.; Garza-Borjon, A.; Simental-Mendia, M.; Vilchez-Cavazos, F.; Tamez-Mata, Y.; Peña-Martinez, V. Delayed union of humeral shaft fractures: Comparison of autograft with and without platelet-rich plasma treatment: A randomized, single blinded clinical trial. Arch. Orthop. Trauma Surg. 2017, 137, 1247–1252. [Google Scholar] [CrossRef]
- Hackl, S.; Hierholzer, C.; Friederichs, J.; Woltmann, A.; Bühren, V.; Von Rüden, C. Long-term outcome following additional rhBMP-7 application in revision surgery of aseptic humeral, femoral, and tibial shaft nonunion. BMC Musculoskelet. Disord. 2017, 18, 342. [Google Scholar] [CrossRef] [PubMed]
- Von Rüden, C.; Morgenstern, M.; Hierholzer, C.; Hackl, S.; Gradinger, F.L.; Woltmann, A.; Bühren, V.; Friederichs, J. The missing effect of human recombinant Bone Morphogenetic Proteins BMP-2 and BMP-7 in surgical treatment of aseptic forearm nonunion. Injury 2016, 47, 919–924. [Google Scholar] [CrossRef] [PubMed]
- Ghaffarpasand, F.; Shahrezaei, M.; Dehghankhalili, M. Effects of Platelet Rich Plasma on Healing Rate of Long Bone Non-union Fractures: A Randomized Double-Blind Placebo Controlled Clinical Trial. Bull. Emerg. Trauma 2016, 4, 134–140. [Google Scholar]
- Aro, H.T.; Govender, S.; Patel, A.D.; Hernigou, P.; De Gregorio, A.P.; Popescu, I.V.; Golden, J.D.; Christensen, J.; Valentin, A. Recombinant Human Bone Morphogenetic Protein-2: A Randomized Trial in Open Tibial Fractures Treated with Reamed Nail Fixation. J. Bone Jt. Surg. 2011, 93, 801–808. [Google Scholar] [CrossRef]
- Tressler, M.A.; Richards, J.E.; Sofianos, D.; Comrie, F.K.; Kregor, P.J.; Obremskey, W.T. Bone Morphogenetic Protein-2 Compared to Autologous Iliac Crest Bone Graft in the Treatment of Long Bone Nonunion. Orthopedics 2011, 34, e877–e884. [Google Scholar] [CrossRef] [PubMed]
- Ristiniemi, J.; Flinkkilä, T.; Hyvönen, P.; Lakovaara, M.; Pakarinen, H.; Jalovaara, P. RhBMP-7 accelerates the healing in distal tibial fractures treated by external fixation. J. Bone Jt. Surgery. Br. Vol. 2007, 89, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.L.; Bucholz, R.W.; Bosse, M.J.; Mirza, S.K.; Lyon, T.R.; Webb, L.X.; Pollak, A.N.; Golden, J.D.; Valentin-Opran, A. BMP-2 Evalu-ation in Surgery for Tibial Trauma-Allgraft (BESTT-ALL) Study Group. Recombinant human BMP-2 and allograft compared with autogenous bone graft for reconstruction of diaphyseal tibial fractures with cortical defects. A randomized, controlled trial. J. Bone Jt. Surg. Am. 2006, 88, 1431–1441. [Google Scholar]
- Govender, S.; Csimma, C.; Genant, H.K.; Valentin-Opran, A.; Amit, Y.; Arbel, R.; Aro, H.; Atar, D.; Bishay, M.; Borner, M.G.; et al. BMP-2 Evaluation in Sur-gery for Tibial Trauma (BESTT) Study Group. Recombinant human bone morphogenetic protein-2 for treatment of open tibial fractures: A prospective, controlled, randomized study of four hundred and fifty patients. J. Bone Jt. Surg. Am. 2002, 84, 2123–2134. [Google Scholar] [CrossRef]
- Friedlaender, G.E.; Perry, C.R.; Cole, J.D.; Cook, S.D.; Cierny, G.; Muschler, G.F.; Zych, G.A.; Calhoun, J.H.; LaForte, A.J.; Yin, S. Osteo-genic protein-1 (bone morphogenetic protein-7) in the treatment of tibial nonunions. J. Bone Jt. Surg. Am. 2001, 83 (Suppl. S1), S151. [Google Scholar] [CrossRef]
- Cook, D.S. Preclinical and Clinical Evaluation of Osteogenic Protein-1 (BMP-7) in bony sites. Preliminary Report: New technology. In Proceedings of the Annual Meeting of the California Orthopaedic Association, Olympic Valley, CA, USA, 14–15 May 1998. [Google Scholar]
- Bennett, M.H.; Stanford, R.E.; Turner, R. Hyperbaric oxygen therapy for promoting fracture healing and treating fracture non-union. Cochrane Database Syst. Rev. 2012, 11, CD004712. [Google Scholar]
- Kurdy, N.; Weiss, J.; Bate, A. Endothelial stimulating angiogenic factor in early fracture healing. Injury 1996, 27, 143–145. [Google Scholar] [CrossRef]
- Phillips, A.M. Overview of the fracture healing cascade. Injury 2005, 36 (Suppl. S3), S5–S7. [Google Scholar] [CrossRef]
- Lieberman, J.R.; Daluiski, A.; Einhorn, T.A. The role of growth factors in the repair of bone. Biology and clinical applications. J. Bone Jt. Surg. Am. 2002, 84, 1032–1044. [Google Scholar] [CrossRef]
- Grosso, A.; Burger, M.G.; Lunger, A.; Schaefer, D.J.; Banfi, A.; Di Maggio, N. It Takes Two to Tango: Coupling of Angiogenesis and Osteogenesis for Bone Regeneration. Front. Bioeng. Biotechnol. 2017, 5, 68. [Google Scholar] [CrossRef]
- Li, S.; Xing, F.; Luo, R.; Liu, M. Clinical Effectiveness of Platelet-Rich Plasma for Long-Bone Delayed Union and Nonunion: A Systematic Review and Meta-Analysis. Front. Med. 2022, 8, 771252. [Google Scholar] [CrossRef]
- Sandler, A.B.; Scanaliato, J.P.; Raiciulescu, S.; Nesti, L.; Dunn, J.C. Bone Morphogenic Protein for Upper Extremity Fractures: A Systematic Review. Hand 2021. [Google Scholar] [CrossRef]
- Dai, J.; Li, L.; Jiang, C.; Wang, C.; Chen, H.; Chai, Y. Bone Morphogenetic Protein for the Healing of Tibial Fracture: A Meta-Analysis of Randomized Controlled Trials. PLoS ONE 2015, 10, e0141670. [Google Scholar] [CrossRef]
- Killington, K.; Mafi, R.; Mafi, P.; Khan, W.S. A Systematic Review of Clinical Studies Investigating Mesenchymal Stem Cells for Fracture Non-Union and Bone Defects. Curr. Stem Cell Res. Ther. 2018, 13, 284–291. [Google Scholar] [CrossRef]
- Benn, A.; Hiepen, C.; Osterland, M.; Schütte, C.; Zwijsen, A.; Knaus, P. Role of bone morphogenetic proteins in sprouting an-giogenesis: Differential BMP receptor-dependent signaling pathways balance stalk vs. tip cell competence. FASEB J. 2017, 31, 4720–4733. [Google Scholar] [CrossRef]
- Chen, W.-C.; Chung, C.-H.; Lu, Y.-C.; Wu, M.-H.; Chou, P.-H.; Yen, J.-Y.; Lai, Y.-W.; Wang, G.-S.; Liu, S.-C.; Cheng, J.-K.; et al. BMP-2 induces angiogenesis by provoking integrin α6 expression in human endothelial progenitor cells. Biochem. Pharmacol. 2018, 150, 256–266. [Google Scholar] [CrossRef]
- Haubruck, P.; Tanner, M.C.; Vlachopoulos, W.; Hagelskamp, S.; Miska, M.; Ober, J.; Fischer, C.; Schmidmaier, G. Comparison of the clinical effectiveness of Bone Morphogenic Protein (BMP) -2 and -7 in the adjunct treatment of lower limb non-unions. Orthop. Traumatol. Surg. Res. 2018, 104, 1241–1248. [Google Scholar] [CrossRef]
- Conway, J.D.; Shabtai, L.; Bauernschub, A.; Specht, S.C. BMP-7 versus BMP-2 for the treatment of long bone non-union. Orthopedics 2014, 37, e1049–e1057. [Google Scholar] [CrossRef]
- Boraiah, S.; Paul, O.; Hawkes, D.; Wickham, M.; Lorich, D.G. Complications of recombinant human BMP-2 for treating complex tibial plateau fractures: A preliminary report. Clin. Orthop. Relat. Res. 2009, 467, 3257–3262. [Google Scholar] [CrossRef]
- Kostiv, R.E.; Matveeva, N.Y.; Kalinichenko, S.G. Localization of VEGF, TGF-β1, BMP-2, and Apoptosis Factors in Hyper-trophic Nonunion of Human Tubular Bones. Bull. Exp. Biol. Med. 2022, 173, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Gao, H.; Xing, D.; Liu, Z.; Zheng, J.; Xiong, Z.; Gong, M.; Liu, L. The effect of bone morphogenetic protein 2 composite materials combined with cannulated screws in treatment of acute displaced femoral neck fractures. Medicine 2020, 99, e18976. [Google Scholar] [CrossRef] [PubMed]
- Papanna, M.C.; Al-Hadithy, N.; Somanchi, B.V.; Sewell, M.D.; Robinson, P.M.; Khan, S.A.; Wilkes, R.A. The use of bone morphogenic protein-7 (OP-1) in the management of resistant non-unions in the upper and lower limb. Injury 2012, 43, 1135–1140. [Google Scholar] [CrossRef] [PubMed]
- Caterini, R.; Potenza, V.; Ippolito, E.; Farsetti, P. Treatment of recalcitrant atrophic non-union of the humeral shaft with BMP-7, autologous bone graft and hydroxyapatite pellets. Injury 2016, 47 (Suppl. S4), S71–S77. [Google Scholar] [CrossRef] [PubMed]
- Starman, J.S.; Bosse, M.J.; Cates, C.A.; Norton, H.J. Recombinant human bone morphogenetic protein-2 use in the off-label treatment of nonunions and acute fractures: A retrospective review. J. Trauma Acute Care Surg. 2012, 72, 676–681. [Google Scholar] [CrossRef]
- Kanakaris, N.; Lasanianos, N.; Calori, G.M.; Verdonk, R.; Blokhuis, T.; Cherubino, P.; De Biase, P.; Giannoudis, P. Application of bone morphogenetic proteins to femoral non-unions: A 4-year multicentre experience. Injury 2009, 40 (Suppl. S3), S54–S61. [Google Scholar] [CrossRef]
- Giannoudis, P.V.; Kanakaris, N.K.; Dimitriou, R.; Gill, I.; Kolimarala, V.; Montgomery, R.J. The Synergistic Effect of Autograft and BMP-7 in the Treatment of Atrophic Nonunions. Clin. Orthop. Relat. Res. 2009, 467, 3239–3248. [Google Scholar] [CrossRef]
- Kanakaris, N.K.; Calori, G.M.; Verdonk, R.; Burssens, P.; De Biase, P.; Capanna, R.; Vangosa, L.B.; Cherubino, P.; Baldo, F.; Ristiniemi, J.; et al. Application of BMP-7 to tibial non-unions: A 3-year multicenter experience. Injury 2008, 39, S83–S90. [Google Scholar] [CrossRef]
- Dimitriou, R.; Dahabreh, Z.; Katsoulis, E.; Matthews, S.; Branfoot, T.; Giannoudis, P. Application of recombinant BMP-7 on persistent upper and lower limb non-unions. Injury 2005, 36 (Suppl. S4), S51–S59. [Google Scholar] [CrossRef]
- Fuchs, T.; Stolberg-Stolberg, J.; Michel, P.A.; Garcia, P.; Amler, S.; Wähnert, D.; Raschke, M.J. Effect of Bone Morphogenetic Protein-2 in the Treatment of Long Bone Non-Unions. J. Clin. Med. 2021, 10, 4597. [Google Scholar] [CrossRef]
- Hoit, G.; Bonyun, M.; Nauth, A. Hardware considerations in infection and nonunion management: When and how to revise the fixation. OTA Int. 2020, 3, e055. [Google Scholar] [CrossRef] [PubMed]
- Watt, S.M.; Gullo, F.; van der Garde, M.; Markeson, D.; Camicia, R.; Khoo, C.P.; Zwaginga, J.J. The angiogenic properties of mes-enchymal stem/stromal cells and their therapeutic potential. Br. Med. Bull. 2013, 108, 25–53. [Google Scholar] [CrossRef] [PubMed]
- Pozzuoli, A.; Gardin, C.; Aldegheri, R.; Bressan, E.; Isola, M.; Calvo-Guirado, J.L.; Biz, C.; Arrigoni, A.; Feroni, L.; Zavan, B. Genetical stability and osteogenic ability of mesenchimal stem cells on demineralized bone matrices. J. Osseointegration 2015, 7, 2–7. [Google Scholar]
- González, M.A.; Gonzalez-Rey, E.; Rico, L.; Büscher, D.; Delgado, M. Treatment of experimental arthritis by inducing immune tolerance with human adipose-derived mesenchymal stem cells. Arthritis Care Res. 2009, 60, 1006–1019. [Google Scholar] [CrossRef]
- Bhattacharjee, A.; Kuiper, J.H.; Roberts, S.; Harrison, P.E.; Cassar-Pullicino, V.N.; Tins, B.; Bajada, S.; Rihardson, J.B. Pre-dictors of fracture healing in patients with recalcitrant nonunions treated with autologous culture expanded bone mar-row-derived mesenchymal stromal cells. J. Orthop. Res. 2018, 37, 1303–1309. [Google Scholar] [CrossRef]
- Dilogo, I.H.; Phedy, P.; Kholinne, E.; Djaja, Y.P.; Fiolin, J.; Kusnadi, Y.; Yulisa, N.D. Autologous mesenchymal stem cell implantation, hydroxyapatite, bone morphogenetic protein-2, and internal fixation for treating critical-sized defects: A translational study. Int. Orthop. 2019, 43, 1509–1519. [Google Scholar] [CrossRef]
- Chu, W.; Wang, X.; Gan, Y.; Zhuang, Y.; Shi, D.; Liu, F.; Sun, Y.; Zhao, J.; Tang, T.; Dai, K. Screen-enrich-combine circulating system to prepare MSC/β-TCP for bone repair in fractures with depressed tibial plateau. Regen. Med. 2019, 14, 555–569. [Google Scholar] [CrossRef]
- Giannotti, S.; Bottai, V.; Ghilardi, M.; Dell'Osso, G.; Fazzi, R.; Trombi, L.; Petrini, M.; Guido, G. Treatment of pseudoarthrosis of the upper limb using expanded mesenchymal stem cells: A pilot study. Eur. Rev. Med. Pharmacol. Sci. 2013, 17, 224–227. [Google Scholar]
- Intini, G. The use of platelet-rich plasma in bone reconstruction therapy. Biomaterials 2009, 30, 4956–4966. [Google Scholar] [CrossRef]
- Bielecki, T.; Gazdzik, T.S.; Szczepanski, T. Benefit of percutaneous injection of autologous platelet-leukocyte-rich gel in patients with delayed union and non-union. Eur. Surg. Res. 2008, 40, 289–296. [Google Scholar] [CrossRef]
- Malhotra, R.; Kumar, V.; Garg, B.; Singh, R.; Jain, V.; Coshic, P.; Chatterjee, K. Role of autologous platelet-rich plasma in treat-ment of long-bone nonunions: A prospective study. Musculoskelet Surg. 2015, 99, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Gołos, J.; Waliński, T.; Piekarczyk, P.; Kwiatkowski, K. Results of the use of platelet rich plasma in the treatment of delayed union of long bones. Ortop. Traumatol. Rehabil. 2014, 16, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Galasso, O.; Mariconda, M.; Romano, G.; Capuano, N.; Romano, L.; Iannò, B.; Milano, C. Expandable intramedullary nailing and platelet rich plasma to treat long bone non-unions. J. Orthop. Traumatol. 2008, 9, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Calori, G.M.; D’Avino, M.; Tagliabue, L.; Albisetti, W.; D’Imporzano, M.; Peretti, G. An Ongoing research for evaluation of treatment with BMPs or AGFs in long bone non-union: Protocol description and preliminary results. Injury 2006, 37 (Suppl. S3), S43–S50. [Google Scholar] [CrossRef] [PubMed]
- Thompson, W.R.; Rubin, C.T.; Rubin, J. Mechanical regulation of signaling pathways in bone. Gene 2012, 503, 179–193. [Google Scholar] [CrossRef]
- Paul, G.R.; Malhotra, A.; Müller, R. Mechanical Stimuli in the Local In Vivo Environment in Bone: Computational Approaches Linking Organ-Scale Loads to Cellular Signals. Curr. Osteoporos. Rep. 2018, 16, 395–403. [Google Scholar] [CrossRef]
- Böhm, A.M.; Dirckx, N.; Tower, R.J.; Peredo, N.; Vanuytven, S.; Theunis, K.; Nefyodova, E.; Cardoen, R.; Lindner, V.; Voet, T.; et al. Activation of Skeletal Stem and Progenitor Cells for Bone Regeneration Is Driven by PDGFRβ Signal-ing. Dev. Cell. 2019, 51, 236–254.e12. [Google Scholar] [CrossRef]
- Yao, Z.; Chen, P.; Fan, L.; Chen, P.; Zhang, X.; Yu, B. CCL2 is a critical mechano-responsive mediator in crosstalk between osteoblasts and bone mesenchymal stromal cells. FASEB J. 2021, 35, e21851. [Google Scholar] [CrossRef]
- Cheong, V.S.; Kadirkamanathan, V.; Dall’Ara, E. The Role of the Loading Condition in Predictions of Bone Adaptation in a Mouse Tibial Loading Model. Front. Bioeng. Biotechnol. 2021, 9, 67686. [Google Scholar]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author/Year/Country | Type of Study | Number of Open Fractures (n) | Number of Closed Fractures (n) | Number of Non-Unions (n) | Type of Osteosynthesis | Osteo-Inductive Factors Applied/Scaffolds | Patients Treated with Osteoinductive Growth Factors (n) | Patients Treated without Osteoinductive Growth Factors (n) | Median Follow-Up (Months) | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|
| Hernigou et al. 2021, France [21] | Prospective randomised cohort study | Open fractures (with gap less than 10 mm) Gustilo - Anderson Type II or III n = 231 treated with Bone marrow concentrate n = 67 control (no early graft) patients n = 76 treated with an early, standard of care, iliac bone graft | No | No | External fixation/Ilizarov | Bone marrow with mesenchymal stem cells (MSCs) | n = 231 Bone marrow group (MSCs) | n = 67 (control group = no early graft) n = 76 (standard iliac bone graft) | 09 | Bone union in: 50.7% Control group 86.8% Iliac Bone graft group 87.4% Bone marrow group (MSCs) |
| Başdelioğlu et al. 2020, Turkey [22] | Retrospective study | n = 1 in PPR group n = 1 in the control group | n = 13 in PRP group n = 09 in the control group | n = 14 in the PRP group n = 10 in the control group | ORIF: n = 7 PRP n = 4 not PRP IMN: PRP n = 3 not PRP n = 1 ILIZAROV: n = 1 PRP n = 1 not PRP CAST: n = 1 PRP n = 2 not PRP BANDAGE: n = 1 PRP, n = 0 not PRP | Autologous platelet-rich plasma (PRP), autologous bone graft allograft | n = 14 | n = 10 | 03 | Fracture healing in both groups Statistically significant difference in time healing (5.3 months in PRP group and 11.3 in control group) No complications |
| Rollo et al. 2020, Italy [23] | Retrospective study | No | n = 50 | n = 50 Type B according ASAMI tibial non union | External fixation/Ilizarov | PRP or Hyperbaric Oxygen Therapy (HOT) | n = 25 with PRP | n = 25 with HOT | 12 | Ilizarov technique plus PRP (or HOT) does not improve the functional outcomes but allows a more rapid healing of the regenerated bone |
| Wang et al. 2019, China [24] | Retrospective case control study | N/A | N/A | n = 50 Humerus: 5 Radius/ulna:3 Femur: 23 Tibia/fibula: 19 | ORIF | Mesenchymal stem cells (MSC), β-tricalcium phosphate scaffolds, autologous bone graft | n = 30 | n = 20 | 09 | Healing of bone defects in 45 pts (success rate: 90%) |
| Zhang et al. 2018, China [25] | Prospective randomised cohort study | N/A | N/A | n = 24 Infected tibial non-union fractures Non-union gap between 3 and 12 cm | External fixation/Ilizarov | Autologous mesenchymal stem cells (MSC) | n = 13 | n = 11 | 16 | Significant decrease in union time and hospitalisation period in the MSC group |
| Duramaz et al. 2018, Turkey [26] | Retrospective study | N/A | N/A | n = 29 Long bone oligotrophic non-unions | Femur: n = 8 PRP, n = 7 IMN exchange Tibia: n = 6 PRP, n = 8 IMN exchange | PRP | n = 14 | n = 15 | 09 | Percutaneous PRP application significantly affected union rate, but without significant difference compared to exchange intramedullary nailing. PRP remains a minimal invasive technique instead of exchange intramedullary nailing. |
| Singh et al. 2018, UK [27] | Prospective randomised cohort study | n = 31 | n = 11 | n = 42 Non-union of the upper limb bones Radius and ulna (n = 25), humerus (n = 14), clavicle (n = 3) | n = 31 had operative interventions (ORIF) n = 11 non-operative | rhBMP-7 autologous bone graft | n = 14 | n = 19 | 12–36 | Healing of non-union in 40 pts, Partial union in 2 pts DASH score: 33.7 Heterotopic bone formation in 2 pts |
| Acosta-Olivo et al. 2017, Mexico [28] | Prospective randomised cohort study | N/A | N/A | n = 16 Delayed union of diaphyseal humeral fractures | Locking compression plate (LCP) fixation | iliac crest autograft using platelet-rich plasma (PRP) | n = 08 | n = 08 | 09 | PRP promotes earlier bone consolidation (19.9 weeks compared to 25.4 weeks in control group) |
| Hackl et al. 2017, Germany [29] | Retrospective comparative study | N/A | N/A | n = 112 Treatment of aseptic diaphyseal Non-union humerus: 19 femur: 37 tibia: 47 | Locking compression plate (LCP) fixation | Recombinant human Bone Morphogenetic Protein-7 (rhBMP-7) | n = 62 with rhBMP-7 | n = 50 | 12 | Aseptic diaphyseal non-union in humerus, femur, and tibia healed irrespectively of additional rhBMP-7 application. |
| Von Ruden et al. 2016, Germany [30] | Prospective randomised cohort study | N/A | N/A | n = 49 Aseptic diaphyseal ulnar and/or radial shaft non-union | Compression plating (ORIF) | With or without human recombinant Bone Morphogenetic Proteins BMP-2 and BMP-7 | BMP-2 (n = 4) BMP-7 (n = 20) | n = 25 | 06–54 (Median 15) | Atrophic/oligotrophic forearm non-union healed irrespective of additional application of BMP combined with autologous bone grafting. |
| Ghaffarpasand et al. 2016, Iran [31] | Prospective randomised double-blind placebo controlled trial | N/A | N/A | Long bone non-union fracture Hypertrophic PRP: n = 23 Placebo: n = 25 Oligotrophic PRP: n = 9 Placebo: n = 11 Atrophic PRP: n = 5 Placebo: n = 2 Femur PRP: n = 16 Placebo: n = 19 Tibia PRP: n = 14 Placebo: n = 12 Humerus PRP: n = 6 Placebo: n = 5 Ulna PRP: n = 1 Placebo: n = 2 | IMN or ORIF along with autologous bone graft. | PRP | n = 37 5 mL PRP | n = 38 5 mL normal saline (placebo) | 09 | Healing rate significantly higher in the PRP group compared to placebo (81.1% vs. 55.3%; p = 0.025). Limb shortening significantly higher in the placebo group (2.61 ± 1.5 vs. 1.88 ± 1.2 mm; p = 0.030). The PRP group had lower pain scores (p = 0.003) and shorter healing duration (p = 0.046). |
| Aro et al. 2011, Finland [32] | Prospective randomised cohort study | n = 277 Open tibial fractures Gustilo–Anderson Type IIIB | No | No | Reamed IMN | rhBMP-2, bovine derived collagen type-I | n = 139 | n = 138 | Healed fracture at 13 and 20 weeks | Healing was not accelerated in the BMP-2 group Deep infections were more common in the BMP-2 group |
| Tressler et al. 2011, USA [33] | Retrospective study | N/A | N/A | n = 93 Long bone fractures: femur, tibia, and humerus | External fixation/Ilizarov: rhBMP-2: n = 2 autograft: n = 3 ORIF: rhBMP-2: n = 4 autograft: n = 29 IMN: rhBMP-2: n = 13 autograft: n = 35 Nonoperative: rhBMP-2: n = 0 autograft: n = 7 | rhBMP-2 mixed with cancellous allograft vs compared iliac crest autograft | n = 19 | n = 74 | 20.0 ± 17.7 | No statistical difference in the rate of healing between treatment groups (rhBMP-2 = 68.4% vs Control = 85.1%, p = 0.09) rhBMP-2 may be a suitable alternative to autologous iliac bone graft, with shorter operative time and reduced intraoperative blood loss |
| Ristiniemi et al. 2007, Finland [34] | Prospective randomised cohort study | n = 04 Distal tibial fractures | n = 36 Distal tibial fractures | All fractures united | External fixation/ Ilizarov | rhBMP-7, bovine collagen | n = 20 | n = 20 | 12 | Healing of fractures in all pts, Delayed healing in 2 pts Time healing and external fixation application of the BMP-7 group was significantly shorter |
| Jones et al. 2006, USA [35] | Prospective randomised cohort study | n = 27 (24: Gustilo–Anderson type-IIIA or IIIB) Diaphyseal tibial fracture with residual defect | n = 03 Diaphyseal tibial fracture with residual defect | No | IMN or External fixation/Ilizarov | 1st Group (n = 15): autologous bone graft 2nd Group (n = 15): rhBMP-2 with cancellous bone chips allograft soaked on absorbable collagen sponge | n = 15 | n = 15 | 12 | Similar healing rates between the groups Deep infections in 4 pts (n = 1 of 1st group and n = 3 of the 2nd group), without immunological reactions |
| Govender et al. 2002, Multicentre study [36] | Prospective randomised cohort study | n = 450 Open tibial shaft fractures | No | No | Reamed and undreamed IMN | rhBMP-2, bovine derived collagen type-I | n = 300 | n = 150 | 12 | The rhBMP-2 group showed accelerated wound and fracture healing and reduction in frequency of secondary operations and infection rates |
| Friedlaender et al. 2001 USA [37] | Prospective randomised comparative cohort study | n = 115 | n = 09 | n = 124 Non-union of the tibia | IMN | rhBMP-7 (n = 124) bovine derived collagen type-I (n = 63) autologous bone graft (n = 61) | n = 63 | n = 61 | 24 | Healing of non-union in 104 pts, Consolidation rate similar between the groups, without deep infection or allergic reactions |
| Cook et al. 1999, USA [38] | Prospective randomised cohort study | N/A | N/A | n = 30 n = 31 Tibial non-union | Reamed IMN | BMP-7 or autologous iliac crest bone | n = 14 (15 non-union) | n = 16 | 09 | Similar healing characteristics between BMP-7 application and autologous iliac crest bone. Advantages of BMP-7:
|
| Author/Year/Country | Type of Study | Indications/Surgical Interventions | Osteoinductive Growth Factor Applied/Scaffolds | Patients Treated with Osteoinductive Growth Factors (n) | Median Follow-Up (Months) | Outcome |
|---|---|---|---|---|---|---|
| Haubruck et al. 2018, Germany [39] | Retrospective comparative cohort study | Non-union of the long bones of the lower limbs one (n = 58) or two stage (n = 98) procedures with plates (n = 85), IMN (n = 65), external fixation (n = 4), lag screws (n = 2) | rhBMP-2 (n = 46), rhBMP-7 (n = 110) autologous bone graft PMMA cement spacer with gentamycin | 156 (F/M: 68/82) | 12 | Pts with rhBMP-2 showed a statistically higher consolidation rate |
| Caterini et al. 2016, Italy [40] | Prospective cohort study | Atrophic non-union of the humeral shaft/internal fixation with compression plate | rhBMP-7, autologous bone graft hydroxyapatite pellets | 12 (F/M: 8/4) | 7.3 | Healing of non-union in all pts, without humeral clinical instability |
| Conway et al. 2014, USA [41] | Retrospective comparative cohort study | Non-union of the long bones (n = 214 limbs) Tibia (n = 78), femur (n = 66), humerus (n = 70) | rhBMP-2, rhBMP-7, autologous bone graft, allograft | 175 (F/M: 81/94) | 17 | Healing was increased in the BMP-2 group (93%) Time healing was reduced in the BMP-2 group Complication rates were lower in the BMP-2 group |
| Starman et al. 2012, USA [42] | Retrospective cohort study | Acute (n = 35) and aseptic and septic non-union (n = 81) fractures of the femur (n = 62), tibia (n = 45), fibula (n = 2), clavicle (n = 1), humerus (n = 5), ulna (n = 1) | rhBMP-2, without graft (n = 31), autologous bone graft (n = 13), allograft (n = 67), allograft and autograft (n = 05) | 116 (F/M:49/67) | 11 | Healing of non-union in 76 pts, revision surgery in 30 pts |
| Papanna et al. 2012 UK [43] | Retrospective cohort study | Persistent non-unions of the upper and lower limbs femur (n = 9), tibia (n = 21), foot and ankle (n = 5), clavicle (n = 3), humerus (n = 10), ulna and radius (n = 4) | rhBMP-7, bovine derived collagen type-I, tri-calcium phosphate crystals | 52 (F/M:22/30) | 13.9 | Clinical and radiological union in 48 pts, Joint stiffness (n = 3) Synostosis (tibiofibular, n = 1) Post-traumatic OA (n = 1) Without deep infection or allergic reactions |
| Kanakaris et al. 2009, UK [44] | Prospective cohort study | Atrophic, aseptic non-union of the femur (22 closed, 08 open) /Intramedullary Nailing (n = 17), ORIF (n = 10), Ilizarov circular frame (n = 3) | rhBMP-7, autologous bone graft | 30 (F/M:8/22) | 30 | Healing of non-union in 26 pts, Revision surgery in 04 pts, without deep infection or allergic reactions |
| Giannoudis et al. 2009, UK [45] | Retrospective cohort study | Atrophic, aseptic non-union of long bones (humeral:07, femoral:19, tibial:19, 31 closed 14 open) /Intramedullary Nailing, ORIF | rhBMP-7, autologous bone graft | 45 (F/M:13/32) | 24.8 | Healing of non-union in all pts, Median pain VAS:9, without deep infection or allergic reactions |
| Kanakaris et al. 2008, UK [46] | Retrospective and Prospective cohort study | Atrophic, aseptic non-union of the tibia (39 closed- 29 open) Intramedullary Nailing (n = 26), ORIF (n = 33), External Fixation (n = 8), non-operatively (n = 1) | rhBMP-7, autologous bone graft | 68 (F/M:18/50) | 18 | Healing of non-union in 61 pts, revision surgery in 07 pts, median health VAS: 8.2, without deep infection or allergic reactions |
| Dimitriou et al. 2005, UK [47] | Prospective randomised cohort study | Persistent non-unions of the upper and lower limbs Tibial (n = 10), femoral (n = 8), humeral (n = 3), ulnar (n = 3), patellar (n = 1), clavicular (n = 1) treated with IMN or ORIF | 1st Group (n = 9): rhBMP-7 autologous bone graft injection of bone marrow 2nd Group (n = 15): rhBMP-7 | 25 (F/M: 06/19) | 15.3 | Healing of non-union in 24 pts, without deep infection or allergic reactions |
| Bhattacharjee et al. 2019, UK [48] | Prospective cohort study | Severe recalcitrant atrophic (n = 29) and hypertrophic (n = 06) Non-union of the tibia (n = 16) and femur (n = 19) | Mesenchymal stem cells (MSC), Hydroxyapatite, tricalcium phosphate, calcium phosphate, serum | 35 (F/M: 14/21) | 30 | Healing of bone defects in 21 pts (success rate: 60%) Significant increase of quality of health index (Eq5D) Sepsis in n = 1 pt. |
| Dilogo et al. 2019 Indonesia [49] | Prospective experimental study | Critical size bony defects with previously failed surgical attempts | Mesenchymal stem cells (MSC), Hydroxyapatite, rhBMP-2 | 06 (F/M: 02/04) | 19 | Healing of bone defects in all pts |
| Chu et al. 2018, China [50] | Retrospective comparative cohort study | Depressed tibial plateau fractures | Mesenchymal stem cells (MSC), β-tricalcium phosphate scaffolds | 39 (F/M: /24/15) | 30.5 | Healing of bone defects in all pts |
| Giannotti et al. 2013, Italy [51] | Prospective experimental study | Atrophic pseudarthrosis of the upper limb | Mesenchymal stem cells (MSC) embedded in fibrin clot, autologous bone graft, homologous bone chips, synthetic bone chips | 08 (F/M: 4/4) | 76 | Healing of non-union in all pts One pt had a 2nd intervention Without allergic reactions, deep infections, ectopic neo-formations or neoplastic transformations Absence of re-fracture |
| Malhotra et al. 2015, India [52] | Prospective cohort study | Non-union of the long bones Tibia (n = 35), femur (n = 30), humerus (n = 11), radius and ulna (n = 18) | Autologous platelet-rich plasma (PRP) | 94 (F/M: 28/66) | 3 | Healing of non-union in 82 pts |
| Golos et al. 2014, Poland [53] | Retrospective cohort study | Delayed union of the long bones | Autologous platelet-rich plasma (PRP) | 132 (F/M: 53/79) | - | Healing of non-union in 108 pts |
| Galasso et al. 2008, Italy [54] | Prospective cohort study | Atrophic aseptic diaphyseal non-unions of long bones (humeral:03, femoral:08, tibial:11), Expandable Intramedullary Nailing | Autologous platelet-rich plasma (PRP) | 22 (F/M:09/13) | 13 | Healing of non-union in all pts Mean time to union: 21.5 weeks One pt suffered moderate pain and limitation of the abduction Without complications like haematomas, infections, delayed wound healing |
| Author Year | Representativeness of the Exposed Cohort | Selection of the Nonexposed Cohort | Ascertainment of Exposure | Demonstration That Outcome of Interest Was Not Present at Start of the Study | Comparability of Cohorts on the Basis of the Design or Analysis | Assessment of the Outcome | Follow up Long Enough for Outcomes * | Adequacy of Follow-Up of Cohort ** | Total | Quality |
|---|---|---|---|---|---|---|---|---|---|---|
| Hernigou et al. 2021, France [21] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 09 | Good |
| Basdelioglu et al. 2020, Turkey [22] | 1 | 1 | 1 | 1 | 2 | 1 | 0 | 0 | 08 | Good |
| Rollo et al. 2020, Italy [23] | 1 | 1 | 1 | 1 | 2 | 1 | 0 | 0 | 08 | Good |
| Wang et al. 2019, China [24] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 09 | Good |
| Zhang et al. 2018, China [25] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 09 | Good |
| Duramaz et al. 2018, Turkey [26] | 1 | 1 | 1 | 1 | 2 | 1 | 0 | 1 | 08 | Good |
| Singh et al. 2018, UK [27] | 1 | 1 | 1 | 1 | 2 | 1 | 0 | 0 | 07 | Good |
| Acosta-Olivo et al. 2017, Mexico [28] | 1 | 1 | 1 | 1 | 2 | 1 | 0 | 0 | 07 | Good |
| Hackl et al. 2017, Germany [29] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 09 | Good |
| Von Ruden et al. 2016, Germany [30] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 09 | Good |
| Ghaffarpasand et al. 2016, Iran [31] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 09 | Good |
| Aro et al. 2011, Finland [32] | 1 | 1 | 1 | 1 | 2 | 1 | 0 | 1 | 08 | Good |
| Tressler et al. 2011, USA [33] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 09 | Good |
| Ristiniemi et al. 2007, Finland [34] | 1 | 1 | 1 | 1 | 2 | 1 | 0 | 1 | 08 | Good |
| Jones et al. 2006, USA [35] | 1 | 1 | 1 | 1 | 2 | 1 | 0 | 0 | 07 | Good |
| Govender et al. 2002, Multicentre study [36] | 1 | 1 | 1 | 1 | 2 | 1 | 0 | 0 | 07 | Good |
| Friedlaender et al. 2001, USA [37] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 07 | Good |
| Cook et al. 1999, USA [38] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 07 | Good |
| Author(s) Year | Randomization | Concealment of Allocation | Double Blinding | Total Withdrawals and Dropouts | Total | Quality |
|---|---|---|---|---|---|---|
| Hernigou et al., 2021, France [21] | ** | * | * | ** | 06 | Good |
| Basdelioglu et al., 2020, Turkey [22] | * | * | * | * | 04 | Good |
| Rollo et al., 2020, Italy [23] | * | * | * | * | 04 | Good |
| Wang et al., 2019, China [24] | ** | * | * | ** | 06 | Good |
| Zhang et al., 2018, China [25] | ** | * | * | * | 05 | Good |
| Duramaz et al., 2018, Turkey [26] | ** | * | * | ** | 06 | Good |
| Singh et al., 2018, UK [27] | * | * | * | * | 04 | Good |
| Acosta-Olivo et al., 2017, Mexico [28] | * | * | * | * | 04 | Good |
| Hackl et al., 2017, Germany [29] | ** | * | * | ** | 06 | Good |
| Von Ruden et al., 2016, Germany [30] | ** | * | * | ** | 06 | Good |
| Ghaffarpasand et al., 2016, Iran [31] | ** | * | * | ** | 06 | Good |
| Aro et al., 2011, Finland [32] | ** | * | * | ** | 06 | Good |
| Tressler et al., 2011, USA [33] | * | * | * | * | 04 | Good |
| Ristiniemi et al., 2007, Finland [34] | * | * | * | * | 04 | Good |
| Jones et al., 2006, USA [35] | ** | * | * | ** | 06 | Good |
| Govender et al., 2002, Multicentre study [36] | * | * | * | * | 04 | Good |
| Friedlaender et al., 2001, USA [37] | ** | * | * | * | 05 | Good |
| Cook et al., 1999, USA [38] | * | * | * | * | 04 | Good |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaspiris, A.; Hadjimichael, A.C.; Vasiliadis, E.S.; Papachristou, D.J.; Giannoudis, P.V.; Panagiotopoulos, E.C. Therapeutic Efficacy and Safety of Osteoinductive Factors and Cellular Therapies for Long Bone Fractures and Non-Unions: A Meta-Analysis and Systematic Review. J. Clin. Med. 2022, 11, 3901. https://doi.org/10.3390/jcm11133901
Kaspiris A, Hadjimichael AC, Vasiliadis ES, Papachristou DJ, Giannoudis PV, Panagiotopoulos EC. Therapeutic Efficacy and Safety of Osteoinductive Factors and Cellular Therapies for Long Bone Fractures and Non-Unions: A Meta-Analysis and Systematic Review. Journal of Clinical Medicine. 2022; 11(13):3901. https://doi.org/10.3390/jcm11133901
Chicago/Turabian StyleKaspiris, Angelos, Argyris C. Hadjimichael, Elias S. Vasiliadis, Dionysios J. Papachristou, Peter V. Giannoudis, and Elias C. Panagiotopoulos. 2022. "Therapeutic Efficacy and Safety of Osteoinductive Factors and Cellular Therapies for Long Bone Fractures and Non-Unions: A Meta-Analysis and Systematic Review" Journal of Clinical Medicine 11, no. 13: 3901. https://doi.org/10.3390/jcm11133901
APA StyleKaspiris, A., Hadjimichael, A. C., Vasiliadis, E. S., Papachristou, D. J., Giannoudis, P. V., & Panagiotopoulos, E. C. (2022). Therapeutic Efficacy and Safety of Osteoinductive Factors and Cellular Therapies for Long Bone Fractures and Non-Unions: A Meta-Analysis and Systematic Review. Journal of Clinical Medicine, 11(13), 3901. https://doi.org/10.3390/jcm11133901