
Carpal Tunnel Syndrome and Ulnar Nerve Entrapment Are Associated with Impaired Psychological Health in Adults as Appraised by Their Increased Use of Psychotropic Medication



Abstract
:1. Introduction
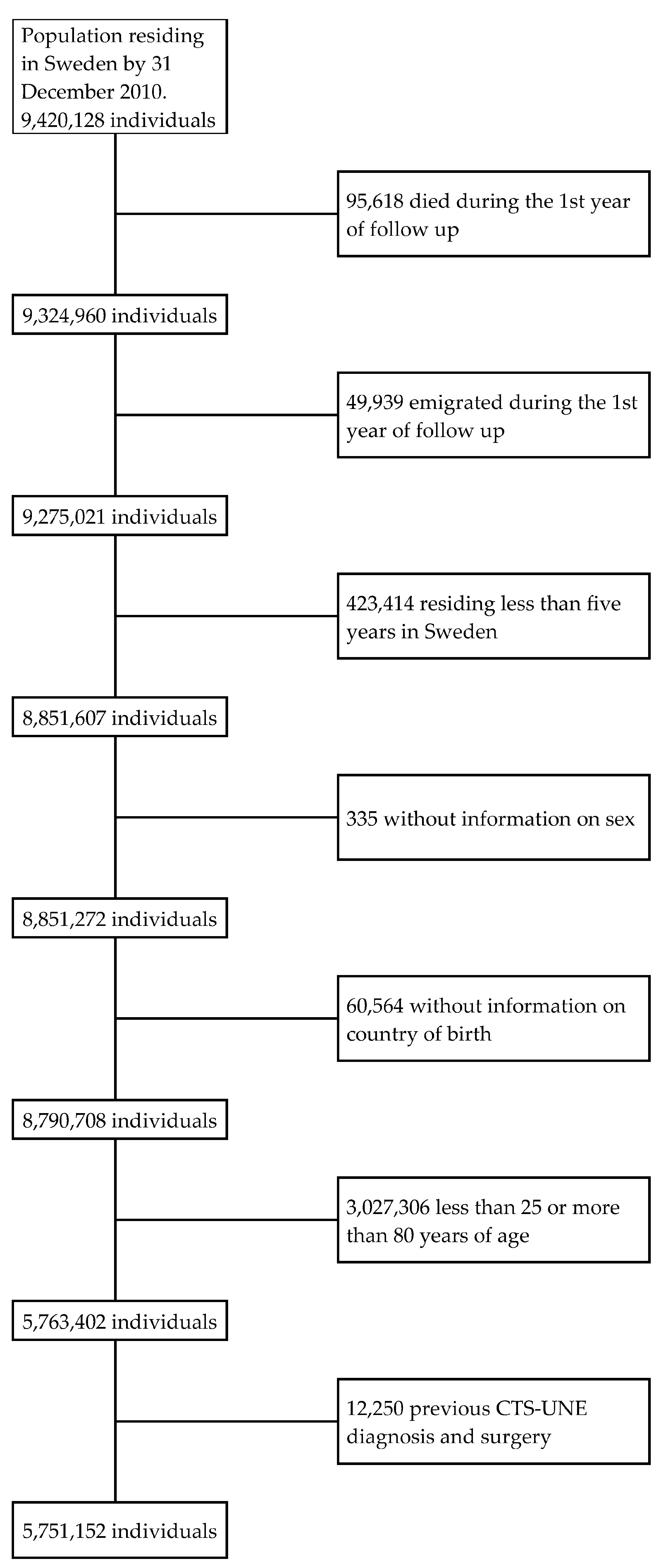
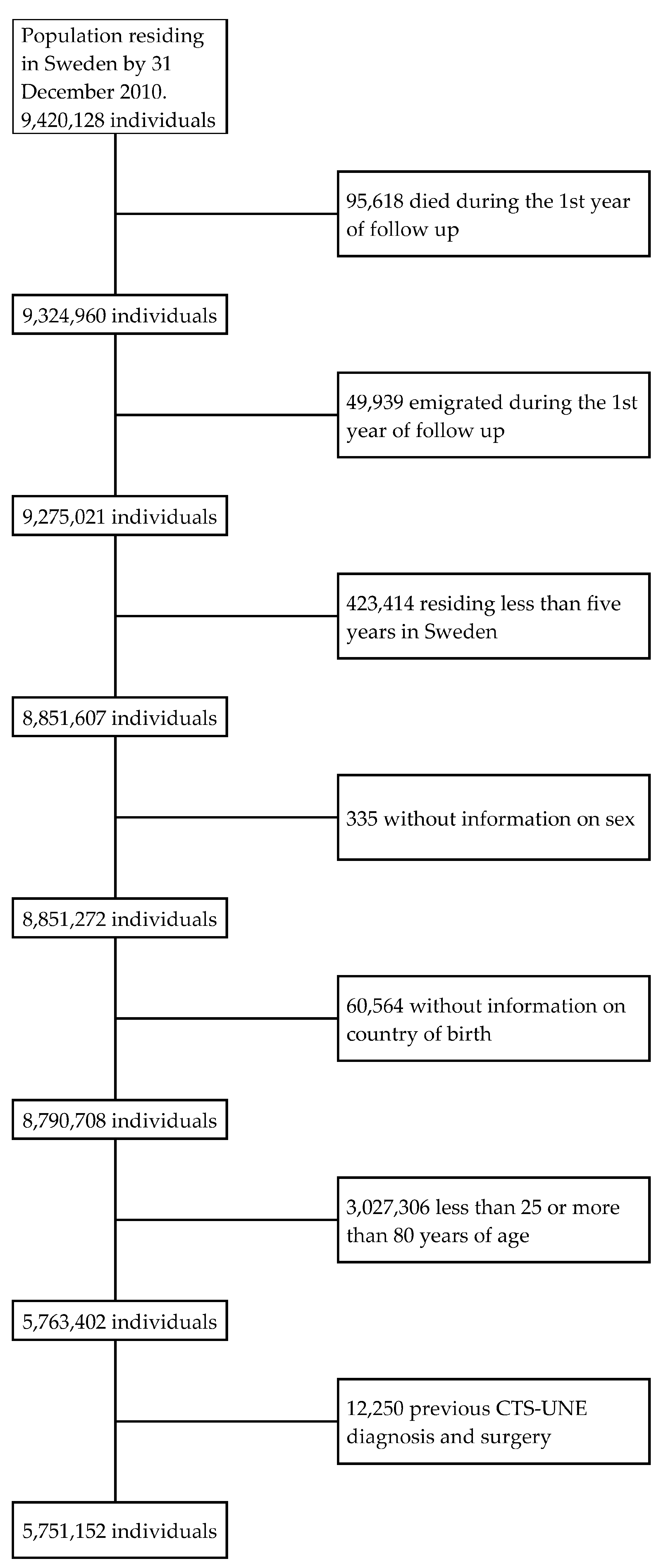
2. Population & Methods
2.1. Databases
2.2. Assessment of Variables
2.3. Statistical Analyses
3. Results
3.1. Demographic and Socioeconomic Characteristics of the Population
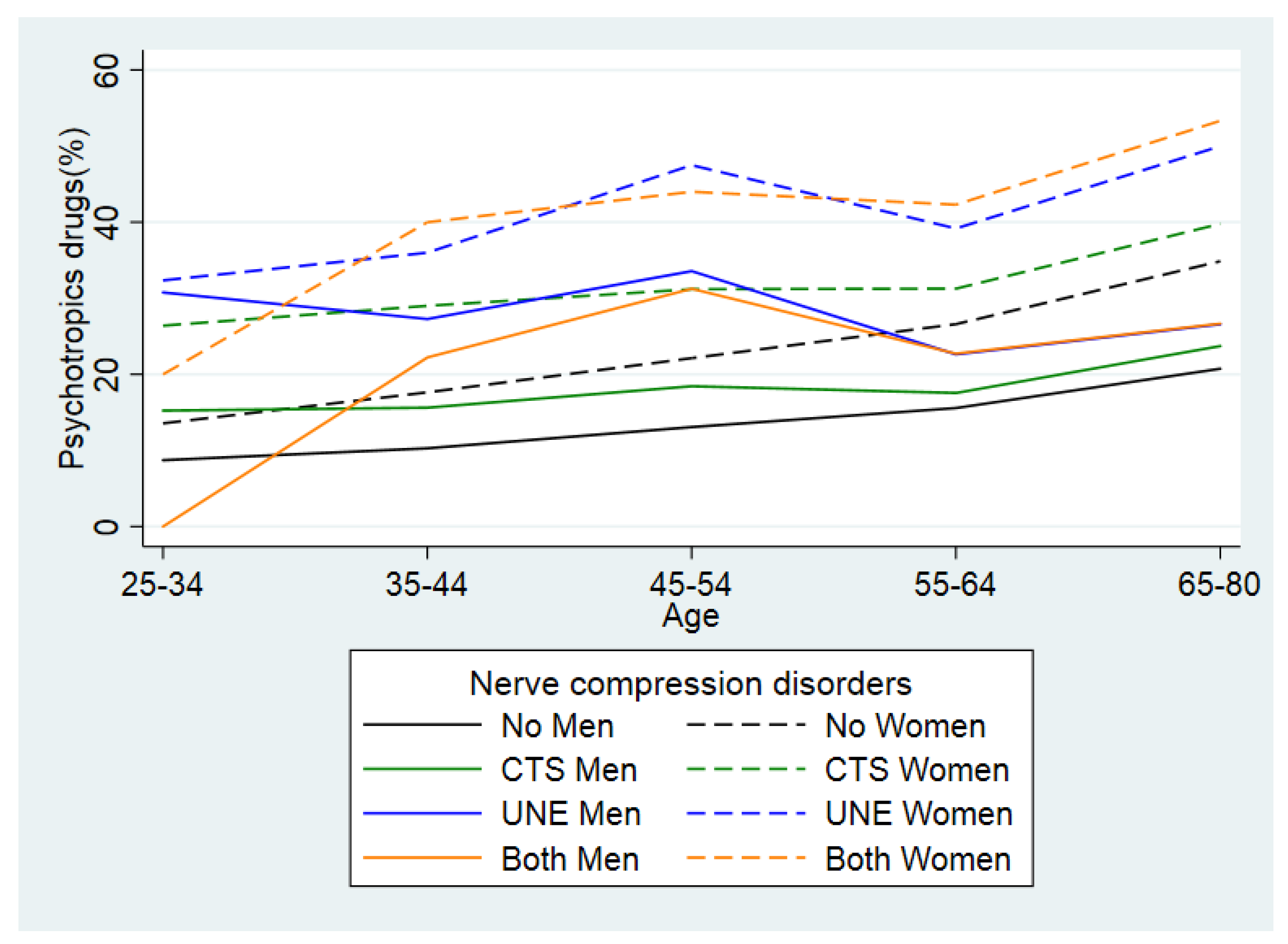
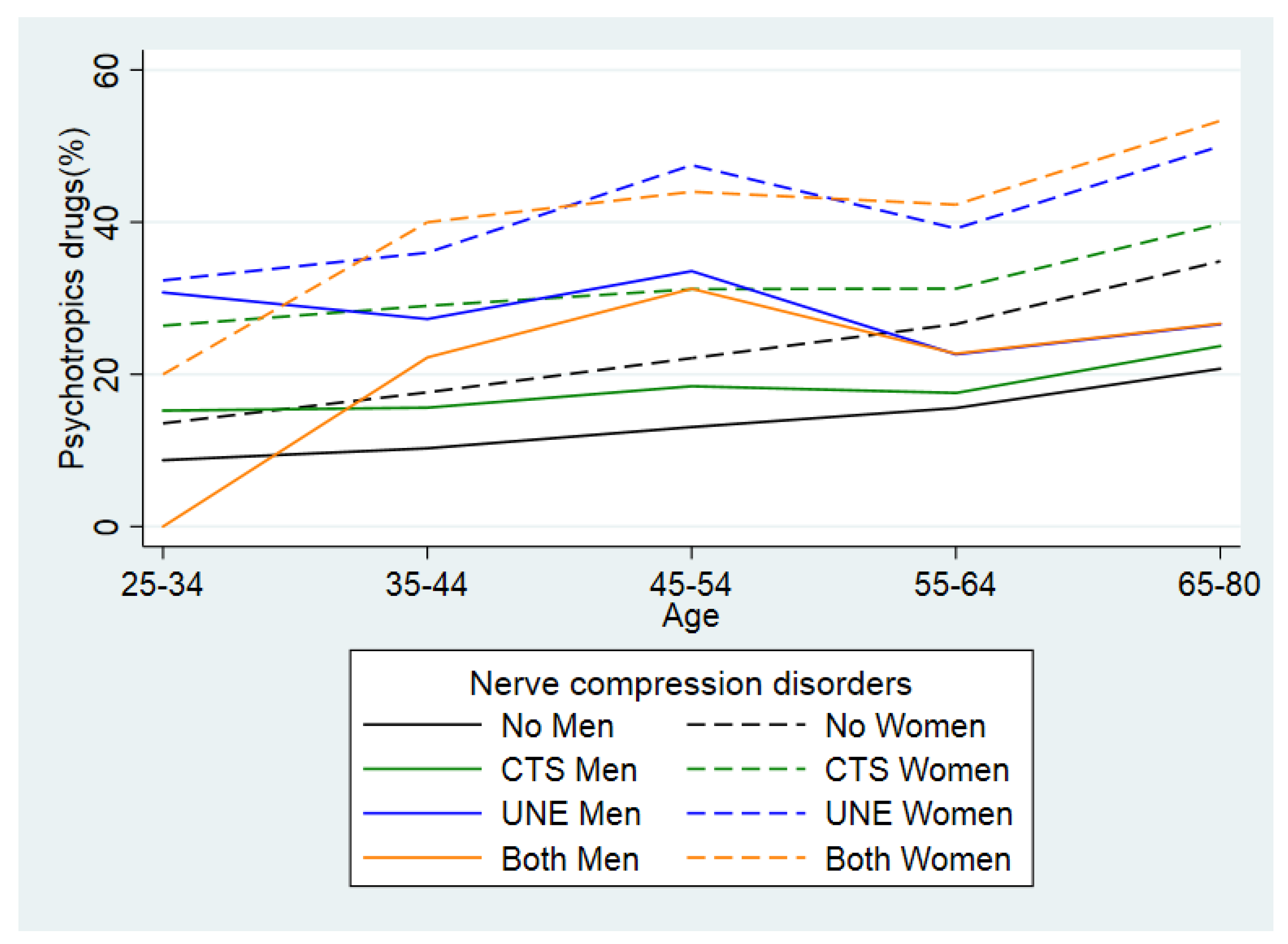
3.2. Use of Psychotropic Medication
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bartels, R.H.; Verbeek, A.L. Risk factors for ulnar nerve compression at the elbow: A case control study. Acta Neurochir. 2007, 149, 669–674; discussion 674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giostad, A.; Nyman, E. Patient Characteristics in Ulnar Nerve Compression at the Elbow at a Tertiary Referral Hospital and Predictive Factors for Outcomes of Simple Decompression versus Subcutaneous Transposition of the Ulnar Nerve. Biomed. Res. Int. 2019, 2019, 5302462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anker, I.; Zimmerman, M.; Andersson, G.S.; Jacobsson, H.; Dahlin, L.B. Outcome and predictors in simple decompression of ulnar nerve entrapment at the elbow. Hand Microsurg. 2018, 7, 24–32. [Google Scholar] [CrossRef]
- Giostad, A.; Rantfors, R.; Nyman, T.; Nyman, E. Enrollment in Treatment at a Specialized Pain Management Clinic at a Tertiary Referral Center after Surgery for Ulnar Nerve Compression: Patient Characteristics and Outcome. J. Hand Surg. Glob. Online 2021, 3, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Hulkkonen, S.; Lampainen, K.; Auvinen, J.; Miettunen, J.; Karppinen, J.; Ryhänen, J. Incidence and operations of median, ulnar and radial entrapment neuropathies in Finland: A nationwide register study. J. Hand Surg. 2020, 45, 226–230. [Google Scholar] [CrossRef]
- Pourmemari, M.H.; Heliovaara, M.; Viikari-Juntura, E.; Shiri, R. Carpal tunnel release: Lifetime prevalence, annual incidence, and risk factors. Muscle Nerve 2018, 58, 497–502. [Google Scholar] [CrossRef]
- Mollestam, K.; Englund, M.; Atroshi, I. Association of clinically relevant carpal tunnel syndrome with type of work and level of education: A general-population study. Sci. Rep. 2021, 11, 19850. [Google Scholar] [CrossRef]
- Jenkins, P.J.; Watts, A.C.; Duckworth, A.D.; McEachan, J.E. Socioeconomic deprivation and the epidemiology of carpal tunnel syndrome. J. Hand Surg. 2012, 37E, 123–129. [Google Scholar] [CrossRef]
- Zimmerman, M.; Hall, E.; Carlsson, K.S.; Nyman, E.; Dahlin, L.B. Socioeconomic factors predicting outcome in surgically treated carpal tunnel syndrome: A national registry-based study. Sci. Rep. 2021, 11, 2581. [Google Scholar] [CrossRef]
- Goodson, J.T.; DeBerard, M.S.; Wheeler, A.J.; Colledge, A.L. Occupational and biopsychosocial risk factors for carpal tunnel syndrome. J. Occup. Environ. Med. 2014, 56, 965–972. [Google Scholar] [CrossRef] [Green Version]
- Brodeur, P.G.; Patel, D.D.; Licht, A.H.; Loftus, D.H.; Cruz, A.I., Jr.; Gil, J.A. Demographic Disparities amongst Patients Receiving Carpal Tunnel Release: A Retrospective Review of 92,921 Patients. Plast. Reconstr. Surg. Glob. Open 2021, 9, e3959. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Earp, B.E.; Blazar, P. Association of Economic Well-Being with Comorbid Conditions in Patients Undergoing Carpal Tunnel Release. J. Hand Surg. Am. 2021. [Google Scholar] [CrossRef]
- Zimmerman, M.; Nyman, E.; Steen Carlsson, K.; Dahlin, L.B. Socioeconomic Factors in Patients with Ulnar Nerve Compression at the Elbow: A National Registry-Based Study. Biomed. Res. Int. 2020, 2020, 5928649. [Google Scholar] [CrossRef] [PubMed]
- Hulkkonen, S.; Auvinen, J.; Miettunen, J.; Karppinen, J.; Ryhanen, J. Smoking is associated with ulnar nerve entrapment: A birth cohort study. Sci. Rep. 2019, 9, 9450. [Google Scholar] [CrossRef] [PubMed]
- Johnson, N.A.; Darwin, O.; Chasiouras, D.; Selby, A.; Bainbridge, C. The effect of social deprivation on the incidence rate of carpal and cubital tunnel syndrome surgery. J. Hand Surg. 2021, 46, 265–269. [Google Scholar] [CrossRef]
- Fernandez-de-Las-Penas, C.; de-la-Llave-Rincon, A.I.; Cescon, C.; Barbero, M.; Arias-Buria, J.L.; Falla, D. Influence of Clinical, Psychological, and Psychophysical Variables on Long-term Treatment Outcomes in Carpal Tunnel Syndrome: Evidence from a Randomized Clinical Trial. Pain Pract. 2019, 19, 644–655. [Google Scholar] [CrossRef] [PubMed]
- Jansen, M.C.; van der Oest, M.J.W.; de Haas, N.P.; Selles Ph, D.R.; Zuidam Md Ph, D.J.; Hand-Wrist Study, G. The Influence of Illness Perception and Mental Health on Return to Work After Carpal Tunnel Release Surgery. J. Hand Surg. Am. 2021, 46, 748–757. [Google Scholar] [CrossRef]
- Psouni, E.; Perez Vicente, R.; Dahlin, L.B.; Merlo, J. Psychotropic drug use as indicator of mental health in adolescents affected by a plexus injury at birth: A large population-based study in Sweden. PLoS ONE 2018, 13, e0193635. [Google Scholar] [CrossRef]
- Nilsson, S.; Merlo, J.; Lyberg-Ahlander, V.; Psouni, E. Psychotropic drug use in adolescents born with an orofacial cleft: A population-based study. BMJ Open 2015, 5, e005306. [Google Scholar] [CrossRef] [Green Version]
- Johnson, N.A.; Darwin, O.; Chasiouras, D.; Selby, A.; Bainbridge, C. The association between surgery for carpal and cubital tunnel syndrome: Analysis of incidence and risk factors within a geographical area. J. Hand Surg. 2021, 46, 260–264. [Google Scholar] [CrossRef]
- Statistics Sweden. MIS 2012:1, SSYK 2012 Swedish Standard Classification of Occupations 2012. Available online: https://www.scb.se/contentassets/c9d055b6f2114b62bd23c33602b56da5/ov9999_2012a01_br_x70br1201.pdf (accessed on 1 January 2022).
- Barros, A.J.; Hirakata, V.N. Alternatives for logistic regression in cross-sectional studies: An empirical comparison of models that directly estimate the prevalence ratio. BMC Med. Res. Methodol. 2003, 3, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pepe, M.S.; Janes, H.; Longton, G.; Leisenring, W.; Newcomb, P. Limitations of the odds ratio in gauging the performance of a diagnostic, prognostic, or screening marker. Am. J. Epidemiol. 2004, 159, 882–890. [Google Scholar] [CrossRef] [PubMed]
- Hosmer, D.W.; Lemeshow, S. Applied Logistic Regression, 2nd ed.; Wiley: New York, NY, USA, 2000. [Google Scholar]
- Jerosch-Herold, C.; Houghton, J.; Blake, J.; Shaikh, A.; Wilson, E.C.; Shepstone, L. Association of psychological distress, quality of life and costs with carpal tunnel syndrome severity: A cross-sectional analysis of the PALMS cohort. BMJ Open 2017, 7, e017732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCallum, L.M.; Damms, N.A.; Sarrigiannis, P.G.; Zis, P. Anxiety and depression in patients with suspected carpal tunnel syndrome—A case-controlled study. Brain Behav. 2019, 9, e01342. [Google Scholar] [CrossRef] [Green Version]
- Zimmerman, M.; Gottsäter, A.; Dahlin, L.B. Carpal Tunnel Syndrome and Diabetes-A Comprehensive Review. J. Clin. Med. 2022, 11, 1674. [Google Scholar] [CrossRef]
- Rydberg, M.; Zimmerman, M.; Gottsater, A.; Nilsson, P.M.; Melander, O.; Dahlin, L.B. Diabetes mellitus as a risk factor for compression neuropathy: A longitudinal cohort study from southern Sweden. BMJ Open Diabetes Res. Care 2020, 8, e001298. [Google Scholar] [CrossRef] [Green Version]
- Sun, P.O.; Walbeehm, E.T.; Selles, R.W.; Slijper, H.P.; Ulrich, D.J.O.; Porsius, J.T.; Hand Wrist Study, G. Patient Mindset and the Success of Carpal Tunnel Release. Plast. Reconstr. Surg. 2021, 147, 66e–75e. [Google Scholar] [CrossRef]
- Mahdi, A.; Halleberg-Nyman, M.; Wretenberg, P. Preoperative psychological distress no reason to delay total knee arthroplasty: A register-based prospective cohort study of 458 patients. Arch. Orthop. Trauma Surg. 2020, 140, 1809–1818. [Google Scholar] [CrossRef]
- Mahdi, A.; Nyman, M.H.; Wretenberg, P. How do orthopaedic surgeons inform their patients before knee arthroplasty surgery? A cross-sectional study. BMC Musculoskelet. Disord. 2018, 19, 414. [Google Scholar] [CrossRef]
- Mahdi, A. Psychological Distress and Contentment after Primary Total Knee Replacement. Ph.D. Thesis, Örebro University, Örebro, Sweden, 2020. [Google Scholar]
- Moradi, F. No integration without health. Lakartidningen 2013, 110, 1046. [Google Scholar]
- Graetz, V.; Rechel, B.; Groot, W.; Norredam, M.; Pavlova, M. Utilization of health care services by migrants in Europe-a systematic literature review. Br. Med. Bull. 2017, 121, 5–18. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Nerve Compression Disorders | ||||
|---|---|---|---|---|
| None | CTS | UNE | Both | |
| Study sample | 5,740,385 | 9728 | 890 | 149 |
| (99.81) | (0.17) | (0.02) | (0.00) | |
| Psychotropic drugs | 1,072,677 | 2,732 | 305 | 53 |
| (18.69) | (28.08) | (34.27) | (35.57) | |
| Age (years) | ||||
| 25–34 | 997,168 | 803 | 73 | 6 |
| (17.37) | (8.25) | (8.20) | (4.03) | |
| 35–44 | 1,183,624 | 1689 | 188 | 24 |
| (20.62) | (17.36) | (21.12) | (16.11) | |
| 45–54 | 1,165,714 | 2522 | 260 | 41 |
| (20.31) | (25.93) | (29.21) | (27.52) | |
| 55–64 | 1,147,095 | 2205 | 234 | 41 |
| (19.98) | (22.67) | (26.29) | (32.21) | |
| 65–80 | 1,246,784 | 2509 | 135 | 30 |
| (21.72) | (25.79) | (15.17) | (20.13) | |
| Men | 2,865,465 | 3149 | 483 | 63 |
| (49.92) | (32.37) | (54.27) | (42.28) | |
| Income | ||||
| Low | 1,309,528 | 2520 | 236 | 31 |
| (22.81) | (25.90) | (26.52) | (20.81) | |
| Middle | 2,038,179 | 3646 | 351 | 57 |
| (35.51) | (37.48) | (39.44) | (38.26) | |
| High | 2,392,678 | 3562 | 303 | 61 |
| (41.68) | (36.62) | (34.04) | (40.94) | |
| Immigrant | 778,468 | 1150 | 118 | 24 |
| (13.56) | (11.82) | (13.26) | (16.11) | |
| Occupational qualification level | ||||
| Low | 329,645 | 804 | 68 | 15 |
| (5.74) | (8.26) | (7.64) | (10.07) | |
| Middle-low | 2,611,706 | 5469 | 525 | 73 |
| (45.50) | (56.22) | (58.99) | (48.99) | |
| Middle-high | 980,117 | 1300 | 94 | 28 |
| (17.07) | (13.36) | (10.56) | (18.79) | |
| High | 1,267,169 | 1326 | 115 | 18 |
| (22.07) | (13.63) | (12.92) | (12.08) | |
| Missing | 551,748 | 829 | 88 | 15 |
| (9.61) | (8.52) | (9.4889) | (10.07) | |
| Previous psychotropic use | 1,608,486 | 3993 | 440 | 80 |
| (28.02) | (41.05) | (49.44) | (53.69) | |
| Model 1 | Model 2 | |
|---|---|---|
| PR (95% CI) | PR (95% CI) | |
| Nerve compression disorders | ||
| Ref | Ref |
| 1.50 (1.45–1.56) | 1.06 (1.02–1.10) |
| 1.83 (1.64–2.05) | 1.16 (1.04–1.29) |
| 1.90 (1.45–2.49) | 1.08 (0.83–1.42) |
| Age (years) | ||
| Ref | |
| 1.12 (1.11–1.13) | |
| 1.20 (1.19–1.21) | |
| 1.30 (1.29–1.31) | |
| 1.49 (1.48–1.50) | |
| Men | Ref | |
| 1.15 (1.15–1.16) | |
| Income | ||
| 1.07 (1.07–1.08) | |
| 1.07 (1.06–1.07) | |
| Ref | |
| Native | Ref | |
| 0.89 (0.89–0.90) | |
| Occupational qualification level | ||
| 1.06 (1.05–1.07) | |
| 1.04 (1.03–1.04) | |
| 1.00 (1.00–1.01) | |
| Ref | |
| 1.27 (1.26–1.42) | |
| Previous psychotropic drugs use | ||
| 15.59 (15.50–15.67) | |
| AUC | 0.501 | 0.885 |
| Nerve Compression Disorders | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age (Years) | None | CTS | UNE | Both | ||||||||
| N | AR | ARD | N | AR | ARD (95% CI) | N | AR | ARD (95% CI) | N | AR | ARD (95% CI) | |
| 25–34 | 997,168 | 11.09 | Ref. | 803 | 23.66 | 12.57 (9.63–15.51) | 73 | 31.51 | 20.42 (9.76–31.07) | 6 | 16.67 | 5.58 (−24.24–35.40) |
| 35–44 | 1,183,624 | 13.90 | Ref | 1689 | 25.46 | 11.55 (9.48–13.36) | 188 | 31.92 | 18.01 (11.35–24.68) | 24 | 33.33 | 19.43 (0.57–38.29) |
| 45–54 | 1,162,714 | 17.54 | Ref | 2522 | 27.87 | 10.33 (8.25–12.09) | 260 | 40.00 | 22.46 (16.50–28.41) | 41 | 39.02 | 21.48 (6.55–34.42) |
| 55–64 | 1,147,095 | 21.10 | Ref | 2205 | 26.49 | 5.39 (3.54–7.23) | 234 | 29.49 | 8.39 (2.55–14.23) | 48 | 33.33 | 12.24 (−1.10–25.57) |
| 65–80 | 1,246,784 | 28.15 | Ref | 2509 | 32.88 | 4.73 (2.89–6.57) | 135 | 36.30 | 8.15 (0.03–16.26) | 30 | 40.01 | 11.85 (−5.68–29.38) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dahlin, L.B.; Perez, R.; Nyman, E.; Zimmerman, M.; Merlo, J. Carpal Tunnel Syndrome and Ulnar Nerve Entrapment Are Associated with Impaired Psychological Health in Adults as Appraised by Their Increased Use of Psychotropic Medication. J. Clin. Med. 2022, 11, 3871. https://doi.org/10.3390/jcm11133871
Dahlin LB, Perez R, Nyman E, Zimmerman M, Merlo J. Carpal Tunnel Syndrome and Ulnar Nerve Entrapment Are Associated with Impaired Psychological Health in Adults as Appraised by Their Increased Use of Psychotropic Medication. Journal of Clinical Medicine. 2022; 11(13):3871. https://doi.org/10.3390/jcm11133871
Chicago/Turabian StyleDahlin, Lars B., Raquel Perez, Erika Nyman, Malin Zimmerman, and Juan Merlo. 2022. "Carpal Tunnel Syndrome and Ulnar Nerve Entrapment Are Associated with Impaired Psychological Health in Adults as Appraised by Their Increased Use of Psychotropic Medication" Journal of Clinical Medicine 11, no. 13: 3871. https://doi.org/10.3390/jcm11133871
APA StyleDahlin, L. B., Perez, R., Nyman, E., Zimmerman, M., & Merlo, J. (2022). Carpal Tunnel Syndrome and Ulnar Nerve Entrapment Are Associated with Impaired Psychological Health in Adults as Appraised by Their Increased Use of Psychotropic Medication. Journal of Clinical Medicine, 11(13), 3871. https://doi.org/10.3390/jcm11133871