
Risk Factors for Prolonged Mechanical Ventilation and Delayed Extubation Following Bimaxillary Orthognathic Surgery: A Single-Center Retrospective Cohort Study

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Setting, and Participants
2.2. Anesthesia, Postoperative Care, and ICU Therapy
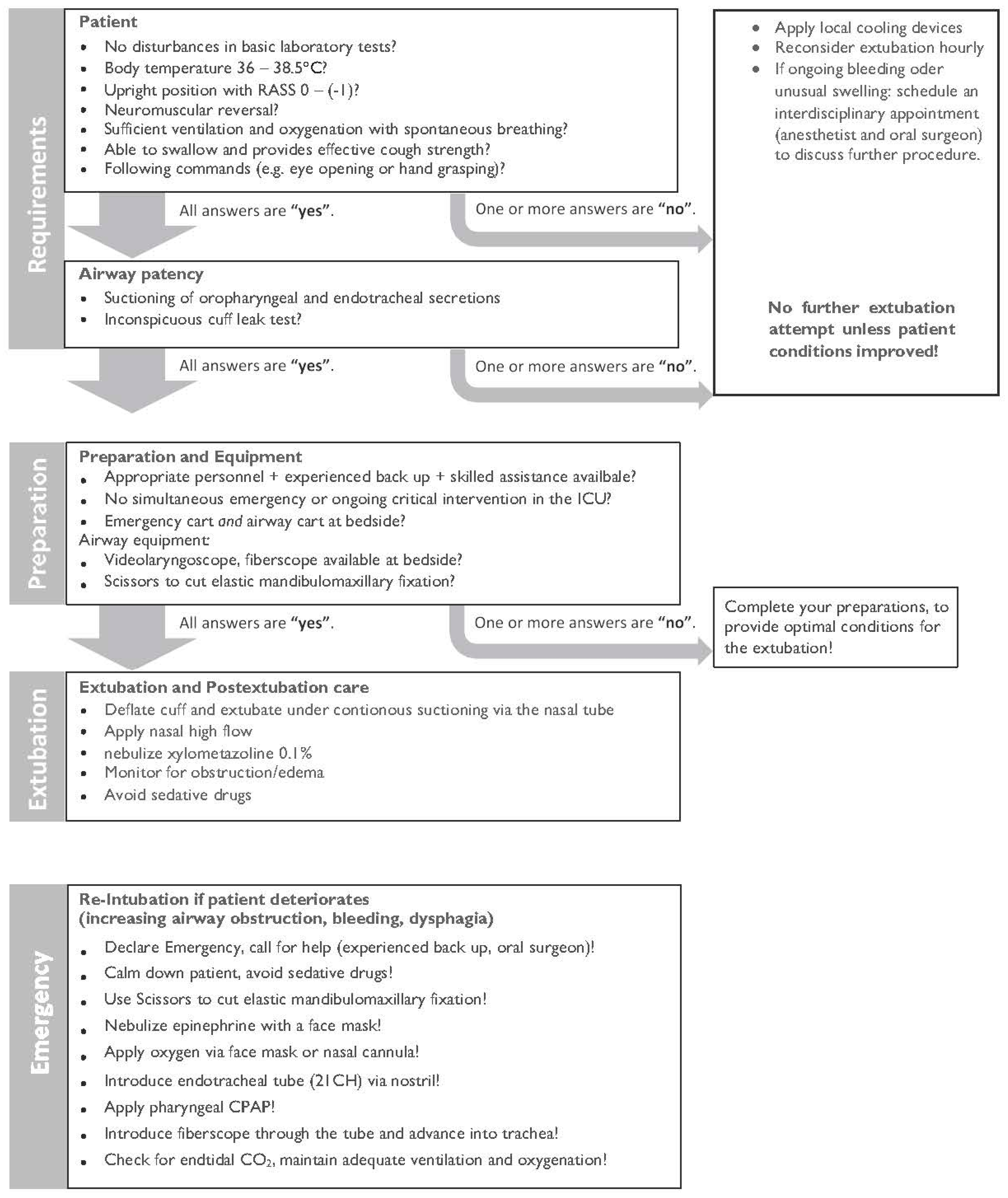
2.3. Surgical Protocol
2.4. Data Collection
2.5. Data Analyses
3. Results
3.1. Preoperative Variables
3.2. Anesthesia and Operative Variables
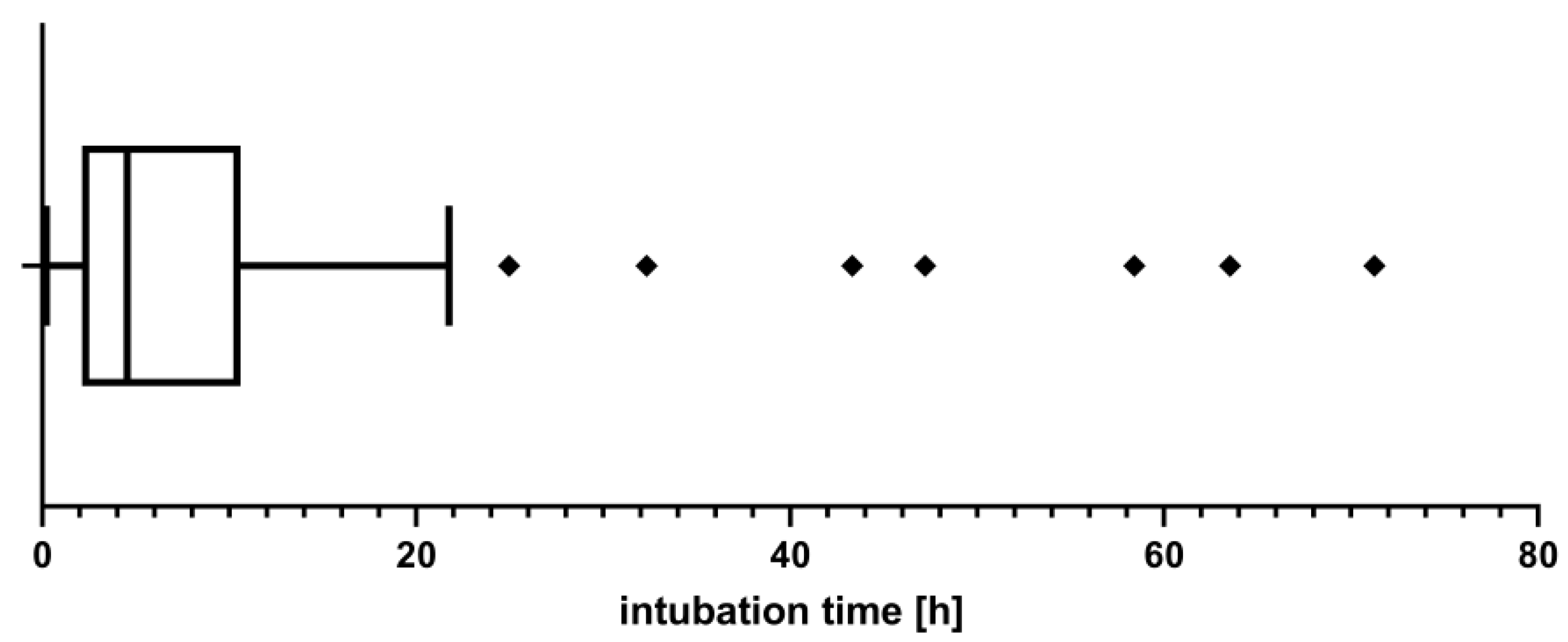
3.3. Time of Mechanical Ventilation in the ICU
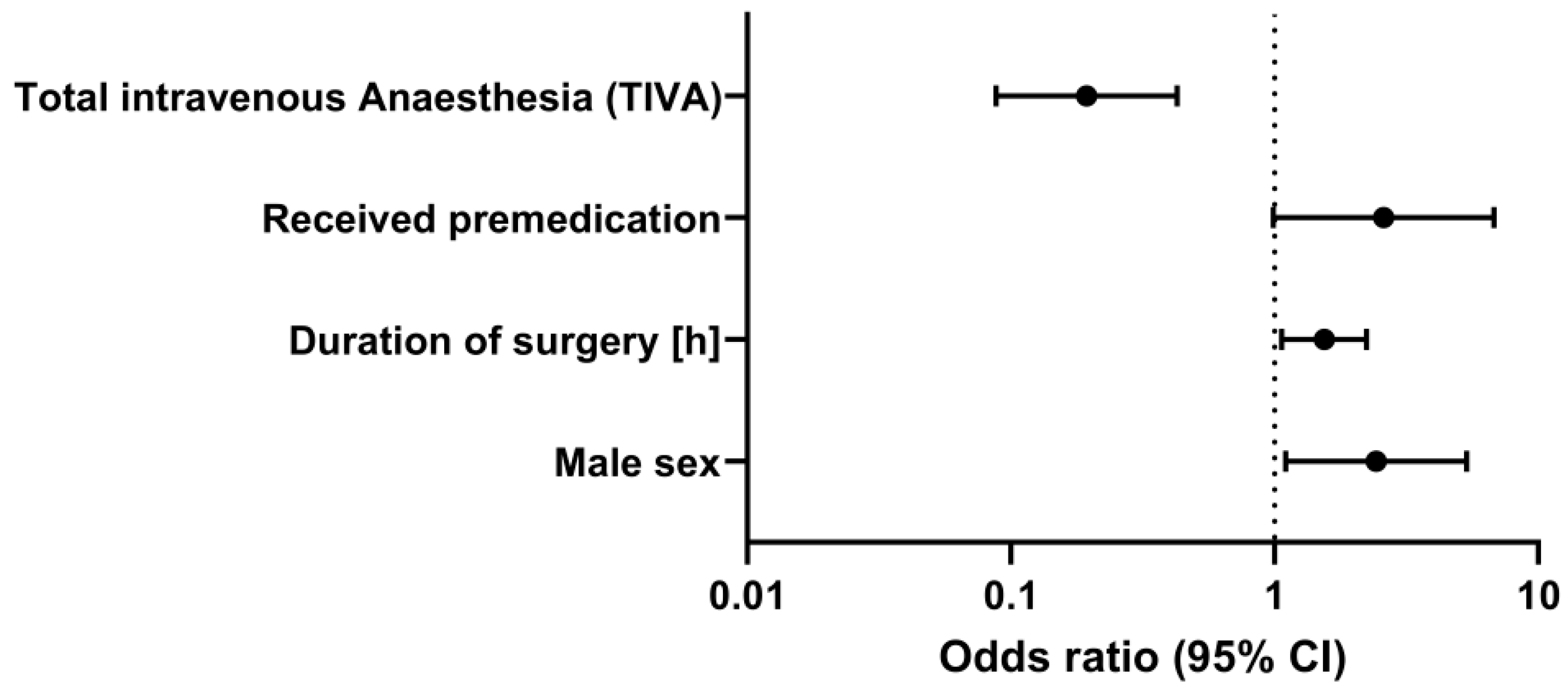
3.4. Statistical Analysis of Risk Factors and Outcome Variables
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cascone, P.; di Paolo, C.; Leonardi, R.; Pedulla, E. Temporomandibular disorders and orthognathic surgery. J. Craniofac. Surg. 2008, 19, 687–692. [Google Scholar] [CrossRef] [PubMed]
- Gottsauner-Wolf, S.; Laimer, J.; Bruckmoser, E. Posterior Airway Changes Following Orthognathic Surgery in Obstructive Sleep Apnea. J. Oral Maxillofac. Surg. 2018, 76, 1093.e1–1093.e21. [Google Scholar] [CrossRef] [PubMed]
- Tepecik, T.; Ertas, U.; Akgun, M. Effects of bimaxillary orthognathic surgery on pharyngeal airway and respiratory function at sleep in patients with class III skeletal relationship. J. Craniomaxillofac. Surg. 2018, 46, 645–653. [Google Scholar] [CrossRef] [PubMed]
- Eshghpour, M.; Mianbandi, V.; Samieirad, S. Intra- and Postoperative Complications of Le Fort I Maxillary Osteotomy. J. Craniofac. Surg. 2018, 29, e797–e803. [Google Scholar] [CrossRef]
- Posnick, J.C.; Choi, E.; Chavda, A. Operative Time, Airway Management, Need for Blood Transfusions, and In-Hospital Stay for Bimaxillary, Intranasal, and Osseous Genioplasty Surgery: Current Clinical Practices. J. Oral Maxillofac. Surg. 2016, 74, 590–600. [Google Scholar] [CrossRef]
- Kantar, R.S.; Cammarata, M.J.; Rifkin, W.J.; Alfonso, A.R.; DeMitchell-Rodriguez, E.M.; Noel, D.Y.; Greenfield, J.; Levy-Lambert, D.; Rodriguez, E.D. Bimaxillary Orthognathic Surgery Is Associated with an Increased Risk of Early Complications. J. Craniofac. Surg. 2019, 30, 352–357. [Google Scholar] [CrossRef]
- Brasileiro, B.F.; van Sickels, J.E. Nasal Alar Pressure Ulcer After Orthognathic Surgery: Clinical Presentation and Preventive Recommendations. J. Craniofac. Surg. 2019, 30, e533–e535. [Google Scholar] [CrossRef]
- Pacheco-Lopez, P.C.; Berkow, L.C.; Hillel, A.T.; Akst, L.M. Complications of airway management. Respir. Care 2014, 59, 1006–1019; discussion 19–21. [Google Scholar] [CrossRef]
- Shinn, J.R.; Kimura, K.S.; Campbell, B.R.; Sun Lowery, A.; Wootten, C.T.; Garrett, C.G.; Francis, D.O.; Hillel, A.T.; Du, L.; Casey, J.D.; et al. Incidence and Outcomes of Acute Laryngeal Injury After Prolonged Mechanical Ventilation. Crit. Care Med. 2019, 47, 1699–1706. [Google Scholar] [CrossRef]
- Alpha, C.; O’Ryan, F.; Silva, A.; Poor, D. The incidence of postoperative wound healing problems following sagittal ramus osteotomies stabilized with miniplates and monocortical screws. J. Oral Maxillofac. Surg. 2006, 64, 659–668. [Google Scholar] [CrossRef]
- Posnick, J.C.; Choi, E.; Chavda, A. Surgical Site Infections Following Bimaxillary Orthognathic, Osseous Genioplasty, and Intranasal Surgery: A Retrospective Cohort Study. J. Oral Maxillofac. Surg. 2017, 75, 584–595. [Google Scholar] [CrossRef] [PubMed]
- Zijderveld, S.A.; Smeele, L.E.; Kostense, P.J.; Tuinzing, D.B. Preoperative antibiotic prophylaxis in orthognathic surgery: A randomized, double-blind, and placebo-controlled clinical study. J. Oral Maxillofac. Surg. 1999, 57, 1403–1406; discussion 6–7. [Google Scholar] [CrossRef]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M.; STROBE Initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Epidemiology 2007, 18, 805–835. [Google Scholar] [CrossRef]
- Semper-Hogg, W.; Fuessinger, M.A.; Dirlewanger, T.W.; Cornelius, C.P.; Metzger, M.C. The influence of dexamethasone on postoperative swelling and neurosensory disturbances after orthognathic surgery: A randomized controlled clinical trial. Head Face Med. 2017, 13, 19. [Google Scholar] [CrossRef] [PubMed]
- Ely, E.W.; Truman, B.; Shintani, A.; Thomason, J.W.; Wheeler, A.P.; Gordon, S.; Francis, J.; Speroff, T.; Gautam, S.; Margolin, R.; et al. Monitoring sedation status over time in ICU patients: Reliability and validity of the Richmond Agitation-Sedation Scale (RASS). JAMA 2003, 289, 2983–2991. [Google Scholar] [CrossRef] [PubMed]
- Schmutz, A.; Dieterich, R.; Kalbhenn, J.; Voss, P.; Loop, T.; Heinrich, S. Protocol based evaluation for feasibility of extubation compared to clinical scoring systems after major oral cancer surgery safely reduces the need for tracheostomy: A retrospective cohort study. BMC Anesthesiol. 2018, 18, 43. [Google Scholar] [CrossRef] [PubMed]
- Al-Moraissi, E.A.; Perez, D.; Ellis, E., 3rd. Do patients with malocclusion have a higher prevalence of temporomandibular disorders than controls both before and after orthognathic surgery? A systematic review and meta-analysis. J. Craniomaxillofac. Surg. 2017, 45, 1716–1723. [Google Scholar] [CrossRef]
- Zaroni, F.M.; Cavalcante, R.C.; Joao da Costa, D.; Kluppel, L.E.; Scariot, R.; Rebellato, N.L.B. Complications associated with orthognathic surgery: A retrospective study of 485 cases. J. Craniomaxillofac. Surg. 2019, 47, 1855–1860. [Google Scholar] [CrossRef]
- Olate, S.; Sigua, E.; Asprino, L.; de Moraes, M. Complications in Orthognathic Surgery. J. Craniofac. Surg. 2018, 29, e158–e161. [Google Scholar] [CrossRef]
- Thiem, D.G.E.; Schneider, D.; Hammel, M.; Saka, B.; Frerich, B.; Al-Nawas, B.; Kämmerer, P.W. Complications or rather side effects? Quantification of patient satisfaction and complications after orthognathic surgery-a retrospective, cross-sectional long-term analysis. Clin. Oral Investig. 2021, 25, 3315–3327. [Google Scholar] [CrossRef]
- Riekert, M.; Kreppel, M.; Schier, R.; Zoller, J.E.; Rempel, V.; Schick, V.C. Postoperative complications after bimaxillary orthognathic surgery: A retrospective study with focus on postoperative ventilation strategies and posterior airway space (PAS). J. Craniomaxillofac. Surg. 2019, 47, 1848–1854. [Google Scholar] [CrossRef] [PubMed]
- Nuotto, E.J.; Korttila, K.T.; Lichtor, J.L.; Ostman, P.L.; Rupani, G. Sedation and recovery of psychomotor function after intravenous administration of various doses of midazolam and diazepam. Anesth. Analg. 1992, 74, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Conway, A.; Rolley, J.; Sutherland, J.R. Midazolam for sedation before procedures. Cochrane Database Syst. Rev. 2016, 2018, CD009491. [Google Scholar] [CrossRef] [PubMed]
- Fredman, B.; Lahav, M.; Zohar, E.; Golod, M.; Paruta, I.; Jedeikin, R. The effect of midazolam premedication on mental and psychomotor recovery in geriatric patients undergoing brief surgical procedures. Anesth. Analg. 1999, 89, 1161–1166. [Google Scholar] [CrossRef]
- Mohammadi, F.; Marashi, M.; Tavakoli, I.; Khakbaz, O. Effects of oral clonidine premedication on hemodynamic status in bimaxillary orthognathic surgery: A double-blind randomized clinical trial. J. Craniomaxillofac. Surg. 2016, 44, 436–439. [Google Scholar] [CrossRef] [PubMed]
- Sezen, G.; Demiraran, Y.; Seker, I.S.; Karagoz, I.; Iskender, A.; Ankarali, H.; Ersoy, O.; Ozlu, O. Does premedication with dexmedetomidine provide perioperative hemodynamic stability in hypertensive patients? BMC Anesthesiol. 2014, 14, 113. [Google Scholar] [CrossRef]
- Kollef, M.H.; O’Brien, J.D.; Silver, P. The impact of gender on outcome from mechanical ventilation. Chest 1997, 111, 434–441. [Google Scholar] [CrossRef]
- Vezzani, A.; Mergoni, M.; Orlandi, P.; Corradi, F.; Volpi, A.; Zasa, M. Gender differences in case mix and outcome of critically ill patients. Gend. Med. 2011, 8, 32–39. [Google Scholar] [CrossRef]
- Mahmood, K.; Eldeirawi, K.; Wahidi, M.M. Association of gender with outcomes in critically ill patients. Crit. Care 2012, 16, R92. [Google Scholar] [CrossRef]
- Daniel, C.R.; de Matos, C.A.; de Meneses, J.B.; Bucoski, S.C.M.; Fréz, A.; Mora, C.T.R.; Ruaro, J.A. Mechanical ventilation and mobilization: Comparison between genders. J. Phys. Ther. Sci. 2015, 27, 1067–1070. [Google Scholar] [CrossRef][Green Version]
- Schraag, S.; Pradelli, L.; Alsaleh, A.J.O.; Bellone, M.; Ghetti, G.; Chung, T.L.; Westphal, M.; Rehberg, S. Propofol vs. inhalational agents to maintain general anaesthesia in ambulatory and in-patient surgery: A systematic review and meta-analysis. BMC Anesthesiol. 2018, 18, 162. [Google Scholar] [CrossRef] [PubMed]
- Anastasian, Z.H.; Gaudet, J.G.; Levitt, L.C.; Mergeche, J.L.; Heyer, E.J.; Berman, M.F. Factors that correlate with the decision to delay extubation after multilevel prone spine surgery. J. Neurosurg. Anesthesiol. 2014, 26, 167–171. [Google Scholar] [CrossRef] [PubMed]
- Sharma, V.; Rao, V.; Manlhiot, C.; Boruvka, A.; Fremes, S.; Wasowicz, M. A derived and validated score to predict prolonged mechanical ventilation in patients undergoing cardiac surgery. J. Thorac. Cardiovasc. Surg. 2017, 153, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Margraf, A.; Ludwig, N.; Zarbock, A.; Rossaint, J. Systemic Inflammatory Response Syndrome After Surgery: Mechanisms and Protection. Anesth. Analg. 2020, 131, 1693–1707. [Google Scholar] [CrossRef] [PubMed]
- Politis, C.; Kunz, S.; Schepers, S.; Vrielinck, L.; Lambrichts, I. Obstructive airway compromise in the early postoperative period after orthognathic surgery. J. Craniofac. Surg. 2012, 23, 1717–1722. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Entire Cohort | n = 195 |
|---|---|
| Age in years, median (IQR) | 23.0 (8) |
| BMI, median (IQR) | 23.1 (5) |
| Gender | |
| Male, n (%) | 88 (45.1) |
| Female, n (%) | 107 (54.9) |
| ASA classification, n (%) | |
| - I and II | 186 (95.4) |
| - III–V | 9 (4.6) |
| Mallampati grading, n (%) | |
| - 1 and 2 | 151 (77.4) |
| - 3 or higher | 15 (7.7) |
| - Mallampati missing | 29 (14.9) |
| Preexisting comorbidities, n (%) | |
| - Hypertension | 6 (3.1) |
| - Allergic asthma | 24 (12.3) |
| - COPD | 2 (1.0) |
| - Hypothyroidism | 9 (4.6) |
| - Depression | 10 (5.1) |
| - Smoker | 27 (13.8) |
| Entire Cohort | n = 195 |
|---|---|
| Received premedication | 125 (64.1%) |
| Intraoperative comedication, n (%) | |
| - Parecoxib | 30 (15.4) |
| - Metamizole | 15 (7.7) |
| - Tranexamic acid | 19 (9.7) |
| Preoperative dexamethasone, n (%) | |
| - None | 16 (8.2) |
| - 4 mg | 10 (5.1) |
| - 8 mg | 4 (2.1) |
| - 16 mg | 20 (10.3) |
| - 20 mg | 83 (42.6) |
| - 40 mg | 49 (25.1) |
| - 44 mg | 6 (3.1) |
| - 80 mg | 6 (3.1) |
| - 84 mg | 1 (0.5) |
| Intraoperative blood loss (mL), median (IQR) | 300 (280) |
| Intraoperative fluid intake (mL), median (IQR) | 1700 (1550) |
| Anesthesia maintenance, n (%) | |
| - Balanced anesthesia | 60 (30.8) |
| - Total intravenous anesthesia | 135 (69.2) |
| Time intervals (min), median (IQR) | |
| - Contact anesthesia until the start of surgical preparation | 30 (15) |
| - Length of operation | 238 (95) |
| - Mechanical ventilation until ICU arrival | 330 (106) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schwer, C.I.; Roth, T.; Gass, M.; Rothweiler, R.; Loop, T.; Metzger, M.C.; Kalbhenn, J. Risk Factors for Prolonged Mechanical Ventilation and Delayed Extubation Following Bimaxillary Orthognathic Surgery: A Single-Center Retrospective Cohort Study. J. Clin. Med. 2022, 11, 3829. https://doi.org/10.3390/jcm11133829
Schwer CI, Roth T, Gass M, Rothweiler R, Loop T, Metzger MC, Kalbhenn J. Risk Factors for Prolonged Mechanical Ventilation and Delayed Extubation Following Bimaxillary Orthognathic Surgery: A Single-Center Retrospective Cohort Study. Journal of Clinical Medicine. 2022; 11(13):3829. https://doi.org/10.3390/jcm11133829
Chicago/Turabian StyleSchwer, Christian I., Teresa Roth, Mathieu Gass, René Rothweiler, Torsten Loop, Marc C. Metzger, and Johannes Kalbhenn. 2022. "Risk Factors for Prolonged Mechanical Ventilation and Delayed Extubation Following Bimaxillary Orthognathic Surgery: A Single-Center Retrospective Cohort Study" Journal of Clinical Medicine 11, no. 13: 3829. https://doi.org/10.3390/jcm11133829
APA StyleSchwer, C. I., Roth, T., Gass, M., Rothweiler, R., Loop, T., Metzger, M. C., & Kalbhenn, J. (2022). Risk Factors for Prolonged Mechanical Ventilation and Delayed Extubation Following Bimaxillary Orthognathic Surgery: A Single-Center Retrospective Cohort Study. Journal of Clinical Medicine, 11(13), 3829. https://doi.org/10.3390/jcm11133829