
Serum Calcification Propensity T50 Associates with Disease Severity in Patients with Pseudoxanthoma Elasticum

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Patient Data Collection
2.2. Assessment of PXE Disease Severity
2.3. Measurement of cIMT, cfPWV and Total Body CT Calcium Score
2.4. Measurement of Serum Calcification Propensity T50
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics and Serum T50 in PXE Patients
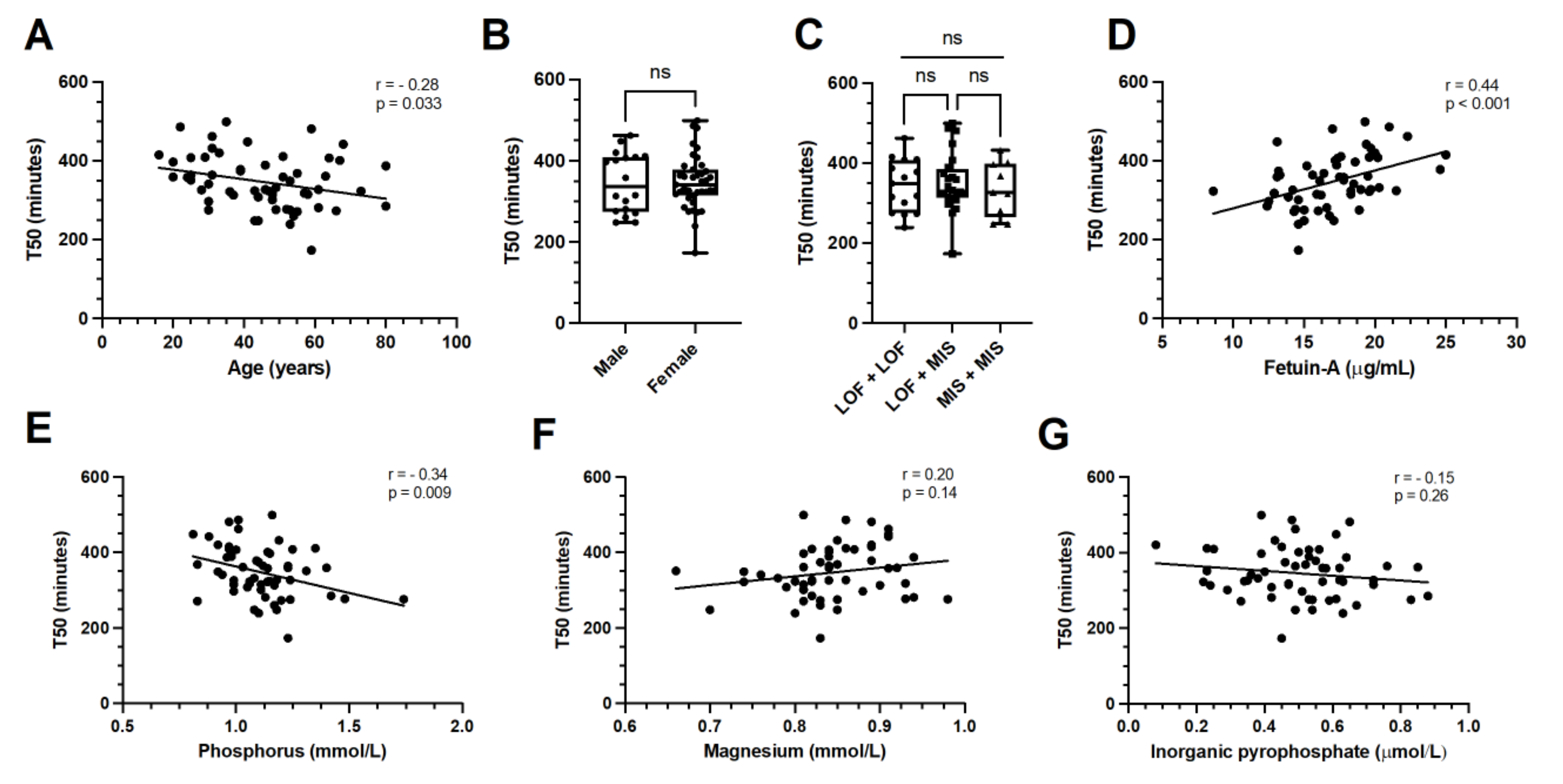
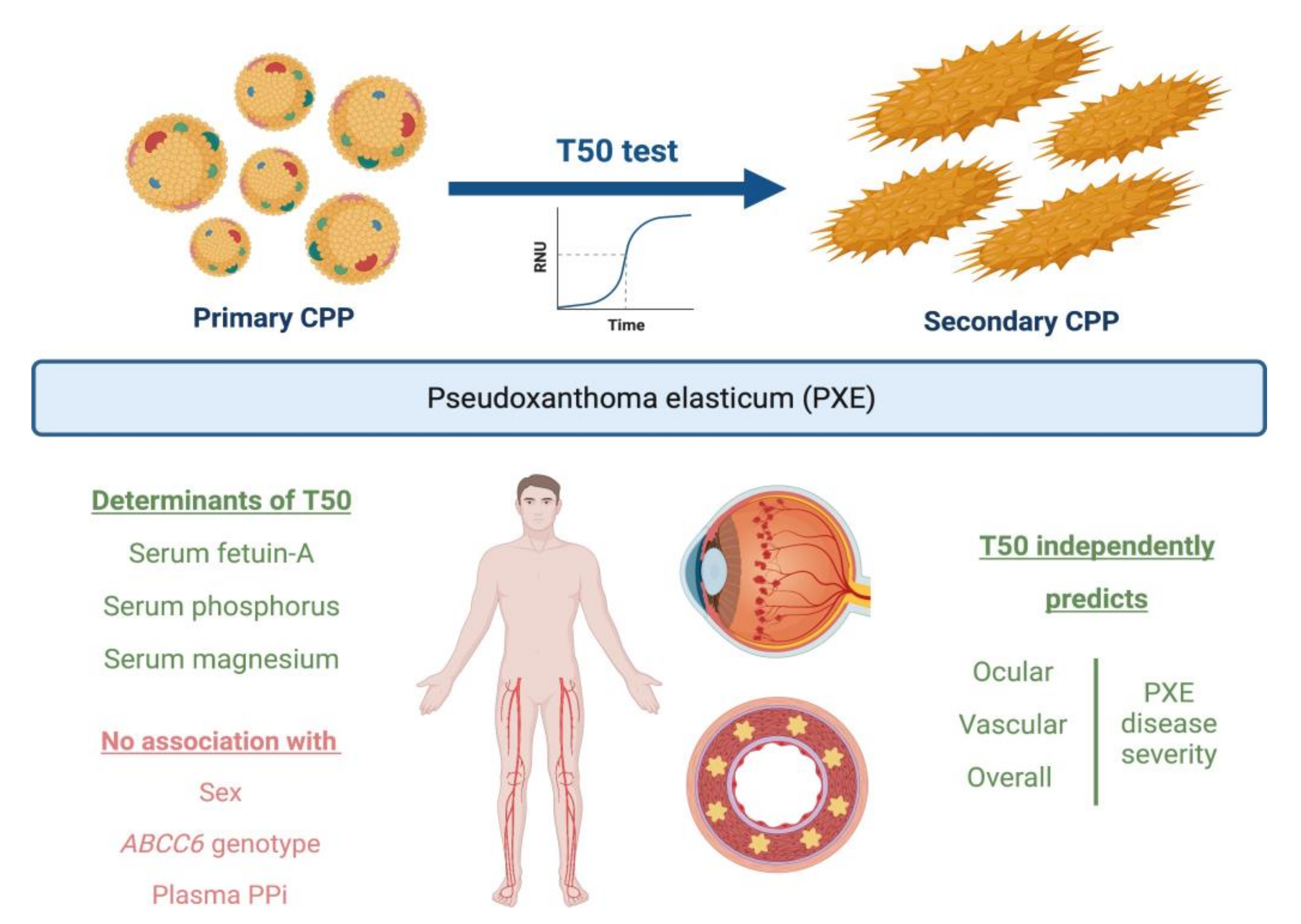
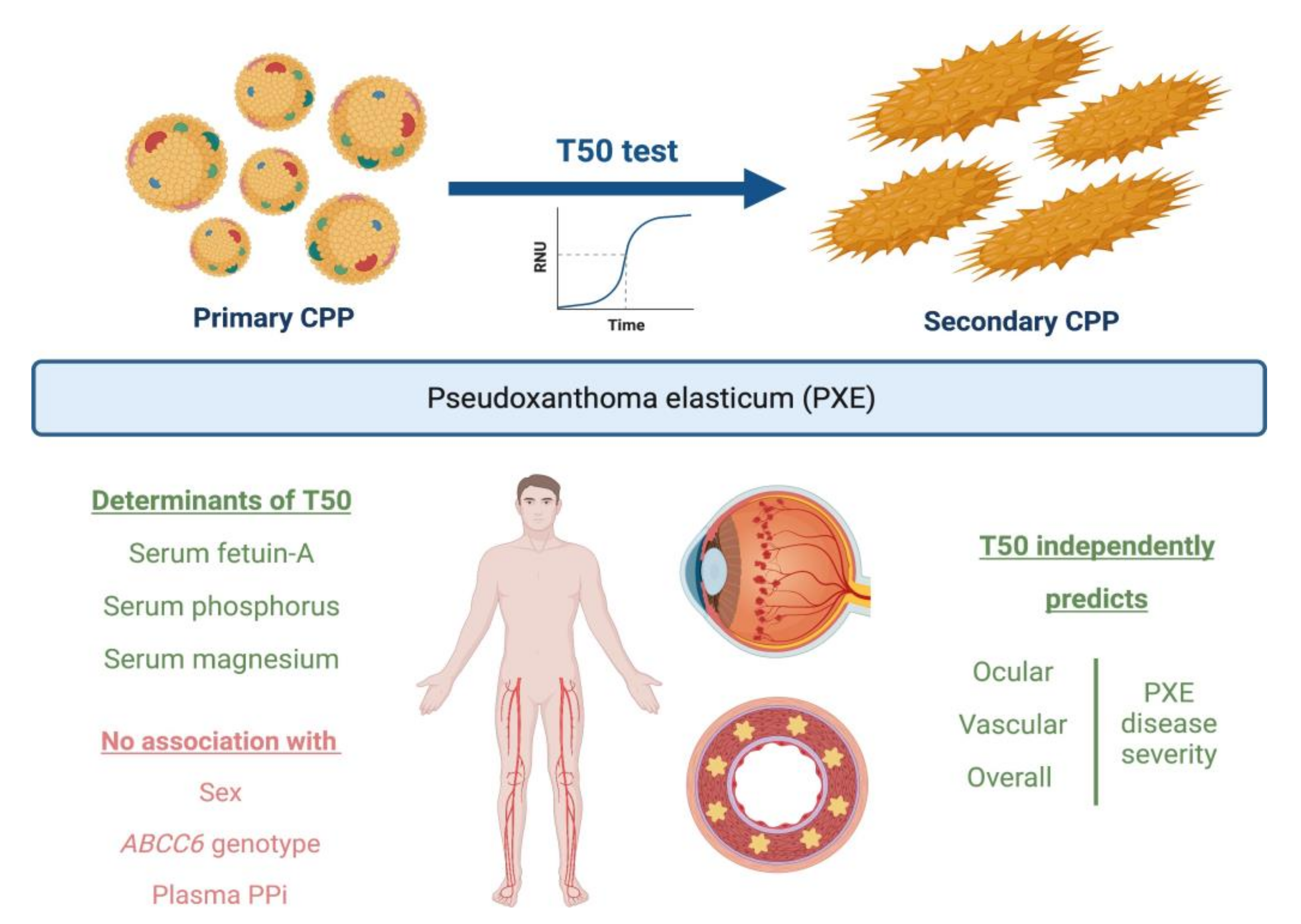
3.2. Determinants of Serum T50 in PXE Patients
3.3. Associations of Serum T50 with PXE Disease Severity
3.4. Associations of Serum T50 with Vascular Ultrasound Measurements and CT Calcium Score in PXE
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- De Vilder, E.Y.; Vanakker, O.M. From variome to phenome: Pathogenesis, diagnosis and management of ectopic mineralization disorders. World J. Clin. Cases 2015, 3, 556–574. [Google Scholar] [CrossRef] [PubMed]
- Rashdan, N.A.; Rutsch, F.; Kempf, H.; Váradi, A.; Lefthériotis, G.; MacRae, V.E. New perspectives on rare connective tissue calcifying diseases. Curr. Opin. Pharmacol. 2016, 28, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Lanzer, P.; Hannan, F.M.; Lanzer, J.D.; Janzen, J.; Raggi, P.; Furniss, D.; Schuchardt, M.; Thakker, R.; Fok, P.W.; St Hilaire, C.; et al. Medial Arterial Calcification: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2021, 78, 1145–1165. [Google Scholar] [CrossRef] [PubMed]
- Poornima, I.G.; Mackey, R.H.; Allison, M.A.; Manson, J.E.; Carr, J.J.; LaMonte, M.J.; Chang, Y.; Kuller, L.H.; Rossouw, J.; Ludlam, S.; et al. Coronary Artery Calcification (CAC) and Post-Trial Cardiovascular Events and Mortality within the Women’s Health Initiative (WHI) Estrogen-Alone Trial. J. Am. Heart Assoc. 2017, 6, e006887. [Google Scholar] [CrossRef] [Green Version]
- Luscher, T.F.; Creager, M.A.; Beckman, J.A.; Cosentino, F. Diabetes and vascular disease: Pathophysiology, clinical consequences, and medical therapy: Part II. Circulation 2003, 108, 1655–1661. [Google Scholar] [CrossRef]
- Chen, J.; Budoff, M.J.; Reilly, M.P.; Yang, W.; Rosas, S.E.; Rahman, M.; Zhang, X.; Roy, J.A.; Lustigova, E.; Nessel, L.; et al. Coronary Artery Calcification and Risk of Cardiovascular Disease and Death among Patients with Chronic Kidney Disease. JAMA Cardiol. 2017, 2, 635–643. [Google Scholar] [CrossRef] [Green Version]
- Silaghi, C.N.; Ilyés, T.; Van Ballegooijen, A.J.; Crăciun, A.M. Calciprotein Particles and Serum Calcification Propensity: Hallmarks of Vascular Calcifications in Patients with Chronic Kidney Disease. J. Clin. Med. 2020, 9, 1287. [Google Scholar] [CrossRef]
- Pasch, A. Novel assessments of systemic calcification propensity. Curr. Opin. Nephrol. Hypertens. 2016, 25, 278–284. [Google Scholar] [CrossRef]
- Pasch, A.; Jahnen-Dechent, W.; Smith, E.R. Phosphate, Calcification in Blood, and Mineral Stress: The Physiologic Blood Mineral Buffering System and Its Association with Cardiovascular Risk. Int. J. Nephrol. 2018, 2018, 9182078. [Google Scholar] [CrossRef]
- Pasch, A.; Farese, S.; Gräber, S.; Wald, J.; Richtering, W.; Floege, J.; Jahnen-Dechent, W. Nanoparticle-based test measures overall propensity for calcification in serum. J. Am. Soc. Nephrol. 2012, 23, 1744–1752. [Google Scholar] [CrossRef]
- Van Dijk, P.R.; Hop, H.; Waanders, F.; Mulder, U.J.; Pasch, A.; Hillebrands, J.-L.; van Goor, H.; Bilo, H.J. Serum calcification propensity in type 1 diabetes associates with mineral stress. Diabetes Res. Clin. Pract. 2019, 158, 107917. [Google Scholar] [CrossRef]
- Mencke, R.; van der Vaart, A.; Pasch, A.; Harms, G.; Waanders, F.; Bilo, H.J.G.; van Goor, H.; Hillebrands, J.-L.; van Dijk, P.R. Serum calcification propensity is associated with HbA1c in type 2 diabetes mellitus. BMJ Open Diabetes Res. Care 2021, 9, e002016. [Google Scholar] [CrossRef]
- Bielesz, B.; Reiter, T.; Marculescu, R.; Gleiss, A.; Bojic, M.; Kieweg, H.; Cejka, D. Calcification Propensity of Serum is Independent of Excretory Renal Function. Sci. Rep. 2017, 7, 17941. [Google Scholar] [CrossRef] [Green Version]
- Eelderink, C.; te Velde-Keyzer, C.A.; Frenay AR, S.; Vermeulen, E.A.; Bachtler, M.; Aghagolzadeh, P.; van Dijk, P.R.; Gansevoort, R.T.; Vervloet, M.G.; Hillebrands, J.L.; et al. Serum Calcification Propensity and the Risk of Cardiovascular and All-Cause Mortality in the General Population: The PREVEND Study. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 1942–1951. [Google Scholar] [CrossRef]
- Bundy, J.D.; Cai, X.; Mehta, R.C.; Scialla, J.J.; De Boer, I.H.; Hsu, C.-Y.; Go, A.S.; Dobre, M.A.; Chen, J.; Rao, P.S.; et al. Serum Calcification Propensity and Clinical Events in CKD. Clin. J. Am. Soc. Nephrol. 2019, 14, 1562–1571. [Google Scholar] [CrossRef]
- Dahle, D.O.; Åsberg, A.; Hartmann, A.; Holdaas, H.; Bachtler, M.; Jenssen, T.G.; Dionisi, M.; Pasch, A. Serum Calcification Propensity Is a Strong and Independent Determinant of Cardiac and All-Cause Mortality in Kidney Transplant Recipients. Am. J. Transpl. 2016, 16, 204–212. [Google Scholar] [CrossRef] [Green Version]
- Bressendorff, I.; Hansen, D.; Schou, M.; Silver, B.; Pasch, A.; Bouchelouche, P.; Pedersen, L.; Rasmussen, L.M.; Brandi, L. Oral Magnesium Supplementation in Chronic Kidney Disease Stages 3 and 4: Efficacy, Safety, and Effect on Serum Calcification Propensity—A Prospective Randomized Double-Blinded Placebo-Controlled Clinical Trial. Kidney Int. Rep. 2017, 2, 380–389. [Google Scholar] [CrossRef] [Green Version]
- Ter Meulen, K.J.; Dekker, M.J.E.; Pasch, A.; Broers, N.J.H.; Van Der Sande, F.M.; Van Der Net, J.B.; Konings, C.J.A.M.; Gsponer, I.M.; Bachtler, M.D.N.; Gauly, A.; et al. Citric-acid dialysate improves the calcification propensity of hemodialysis patients: A multicenter prospective randomized cross-over trial. PLoS ONE 2019, 14, e0225824. [Google Scholar] [CrossRef] [Green Version]
- De Vilder, E.Y.; Hosen, M.J.; Vanakker, O.M. The ABCC6 Transporter as a Paradigm for Networking from an Orphan Disease to Complex Disorders. BioMed Res. Int. 2015, 2015, 648569. [Google Scholar] [CrossRef] [Green Version]
- Scheffer, G.L.; Hu, X.; Pijnenborg, A.C.L.M.; Wijnholds, J.; Bergen, A.A.B.; Scheper, R.J. MRP6 (ABCC6) detection in normal human tissues and tumors. Lab. Investig. 2002, 82, 515–518. [Google Scholar] [CrossRef]
- Verschuere, S.; Van Gils, M.; Nollet, L.; Vanakker, O.M. From membrane to mineralization: The curious case of the ABCC6 transporter. FEBS Lett. 2020, 594, 4109–4133. [Google Scholar] [CrossRef]
- Finger, R.P.; Charbel Issa, P.; Ladewig, M.S.; Götting, C.; Szliska, C.; Scholl, H.P.; Holz, F.G. Pseudoxanthoma elasticum: Genetics, clinical manifestations and therapeutic approaches. Surv. Ophthalmol. 2009, 54, 272–285. [Google Scholar] [CrossRef]
- Campens, L.; Vanakker, O.M.; Trachet, B.; Segers, P.; Leroy, B.P.; De Zaeytijd, J.; Voet, D.; De Paepe, A.; De Backer, T.; De Backer, J. Characterization of cardiovascular involvement in pseudoxanthoma elasticum families. Arterioscler. Thromb. Vasc. Biol. 2013, 33, 2646–2652. [Google Scholar] [CrossRef] [Green Version]
- Kauw, F.; Kranenburg, G.; Kappelle, L.J.; Hendrikse, J.; Koek, H.L.; Visseren, F.L.; Mali, W.P.; de Jong, P.A.; Spiering, W. Cerebral disease in a nationwide Dutch pseudoxanthoma elasticum cohort with a systematic review of the literature. J. Neurol. Sci. 2017, 373, 167–172. [Google Scholar] [CrossRef]
- Visseren, F.L.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Williams, B.; et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef]
- Sánchez-Tévar, A.M.; García-Fernández, M.; Murcia-Casas, B.; Rioja-Villodres, J.; Carrillo, J.L.; Camacho, M.; Van Gils, M.; Sánchez-Chaparro, M.A.; Vanakker, O.; Valdivielso, P. Plasma inorganic pyrophosphate and alkaline phosphatase in patients with pseudoxanthoma elasticum. Ann. Transl. Med. 2019, 7, 798. [Google Scholar] [CrossRef]
- Hosen, M.J.; Van Nieuwerburgh, F.; Steyaert, W.; Deforce, D.; Martin, L.; Leftheriotis, G.; De Paepe, A.; Coucke, P.J.; Vanakker, O.M. Efficiency of exome sequencing for the molecular diagnosis of pseudoxanthoma elasticum. J. Investig. Dermatol. 2015, 135, 992–998. [Google Scholar] [CrossRef] [Green Version]
- Verschuere, S.; Navassiolava, N.; Martin, L.; Nevalainen, P.I.; Coucke, P.J.; Vanakker, O.M. Reassessment of causality of ABCC6 missense variants associated with pseudoxanthoma elasticum based on Sherloc. Genet. Med. 2020, 23, 131–139. [Google Scholar] [CrossRef]
- Boraldi, F.; Murro, V.; Lofaro, F.; Mucciolo, D.; Costa, S.; Pavese, L.; Quaglino, D. Phenotypic Features and Genetic Findings in a Cohort of Italian Pseudoxanthoma Elasticum Patients and Update of the Ophthalmologic Evaluation Score. J. Clin. Med. 2021, 10, 2710. [Google Scholar] [CrossRef]
- Agatston, A.S.; Janowitz, W.R.; Hildner, F.J.; Zusmer, N.R.; Viamonte, M., Jr.; Detrano, R. Quantification of coronary artery calcium using ultrafast computed tomography. J. Am. Coll. Cardiol. 1990, 15, 827–832. [Google Scholar] [CrossRef] [Green Version]
- Ziegler, S.G.; Ferreira, C.R.; MacFarlane, E.G.; Riddle, R.C.; Tomlinson, R.E.; Chew, E.Y.; Martin, L.; Sergienko, E.; Pinkerton, A.B.; Dietz, H.C.; et al. Ectopic calcification in pseudoxanthoma elasticum responds to inhibition of tissue-nonspecific alkaline phosphatase. Sci. Transl. Med. 2017, 9, eaal1669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nollet, L.; Van Gils, M.; Willaert, A.; Coucke, P.J.; Vanakker, O.M. Minocycline attenuates excessive DNA damage response and reduces ectopic calcification in pseudoxanthoma elasticum. J. Investig. Dermatol. 2021, 142, 1629–1638. [Google Scholar] [CrossRef] [PubMed]
- Bouderlique, E.; Nollet, L.; Letavernier, E.; Vanakker, O.M. Minocycline Counteracts Ectopic Calcification in a Murine Model of Pseudoxanthoma Elasticum: A Proof-of-Concept Study. Int. J. Mol. Sci. 2022, 23, 1838. [Google Scholar] [CrossRef] [PubMed]
- Smith, E.R.; Ford, M.L.; Tomlinson, L.; Bodenham, E.; McMahon, L.P.; Farese, S.; Rajkumar, C.; Holt, S.; Pasch, A. Serum calcification propensity predicts all-cause mortality in predialysis CKD. J. Am. Soc. Nephrol. 2014, 25, 339–348. [Google Scholar] [CrossRef] [PubMed]
- Hendig, D.; Schulz, V.; Arndt, M.; Szliska, C.; Kleesiek, K.; Götting, C. Role of serum fetuin-A, a major inhibitor of systemic calcification, in pseudoxanthoma elasticum. Clin. Chem. 2006, 52, 227–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, Q.; Dibra, F.; Lee, M.D.; Oldenburg, R.; Uitto, J. Overexpression of fetuin-a counteracts ectopic mineralization in a mouse model of pseudoxanthoma elasticum (Abcc6−/−). J. Investig. Dermatol. 2010, 130, 1288–1296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, Q.; Li, Q.; Uitto, J. Aberrant mineralization of connective tissues in a mouse model of pseudoxanthoma elasticum: Systemic and local regulatory factors. J. Investig. Dermatol. 2007, 127, 1392–1402. [Google Scholar] [CrossRef] [Green Version]
- LaRusso, J.; Li, Q.; Jiang, Q.; Uitto, J. Elevated dietary magnesium prevents connective tissue mineralization in a mouse model of pseudoxanthoma elasticum (Abcc6−/−). J. Investig. Dermatol. 2009, 129, 1388–1394. [Google Scholar] [CrossRef] [Green Version]
- Kupetsky-Rincon, E.A.; Li, Q.; Uitto, J. Magnesium reduces carotid intima-media thickness in a mouse model of pseudoxanthoma elasticum: A novel treatment biomarker. Clin. Transl. Sci. 2012, 5, 259–264. [Google Scholar] [CrossRef]
- Rose, S.; On, S.J.; Fuchs, W.; Chen, C.; Phelps, R.; Kornreich, D.; Haddican, M.; Singer, G.; Wong, V.; Lebwohl, M.; et al. Magnesium supplementation in the treatment of pseudoxanthoma elasticum: A randomized trial. J. Am. Acad. Dermatol. 2019, 81, 263–265. [Google Scholar] [CrossRef] [Green Version]
- Jansen, R.S.; Duijst, S.; Mahakena, S.; Sommer, D.; Szeri, F.; Váradi, A.; Plomp, A.; Bergen, A.A.; Oude Elferink, R.P.J.; van de Wetering, K.; et al. ABCC6-mediated ATP secretion by the liver is the main source of the mineralization inhibitor inorganic pyrophosphate in the systemic circulation-brief report. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 1985–1989. [Google Scholar] [CrossRef] [Green Version]
- Kiss, N.; Fésűs, L.; Bozsányi, S.; Szeri, F.; Van Gils, M.; Szabó, V.; Nagy, A.I.; Hidvégi, B.; Szipőcs, R.; Martin, L.; et al. Nonlinear optical microscopy is a novel tool for the analysis of cutaneous alterations in pseudoxanthoma elasticum. Lasers Med. Sci. 2020, 35, 1821–1830. [Google Scholar] [CrossRef]
- Farkas, K.; Bozsányi, S.; Plázár, D.; Bánvölgyi, A.; Fésűs, L.; Anker, P.; Zakariás, S.; Lihacova, I.; Lihachev, A.; Lange, M.; et al. Autofluorescence Imaging of the Skin Is an Objective Non-Invasive Technique for Diagnosing Pseudoxanthoma Elasticum. Diagnostics 2021, 11, 260. [Google Scholar] [CrossRef]
- Germain, D.; Boutouyrie, P.; Laloux, B.; Laurent, S. Arterial remodeling and stiffness in patients with pseudoxanthoma elasticum. Arterioscler. Thromb. Vasc. Biol. 2003, 23, 836–841. [Google Scholar] [CrossRef] [Green Version]
- Kranenburg, G.; Visseren, F.L.; de Borst, G.J.; de Jong, P.A.; Spiering, W. Arterial stiffening and thickening in patients with pseudoxanthoma elasticum. Atherosclerosis 2018, 270, 160–165. [Google Scholar] [CrossRef]
- Pruijm, M.; Lu, Y.; Megdiche, F.; Piskunowicz, M.; Milani, B.; Stuber, M.; Bachtler, M.; Vogt, B.; Michel, B.; Pasch, A. Serum calcification propensity is associated with renal tissue oxygenation and resistive index in patients with arterial hypertension or chronic kidney disease. J. Hypertens. 2017, 35, 2044–2052. [Google Scholar] [CrossRef]
- Sequí-Domínguez, I.; Cavero-Redondo, I.; Álvarez-Bueno, C.; Pozuelo-Carrascosa, D.P.; De Arenas-Arroyo, S.N.; Martínez-Vizcaíno, V. Accuracy of Pulse Wave Velocity Predicting Cardiovascular and All-Cause Mortality. A Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 2080. [Google Scholar] [CrossRef]
- Aghagolzadeh, P.; Bachtler, M.; Bijarnia, R.; Jackson, C.; Smith, E.R.; Odermatt, A.; Radpour, R.; Pasch, A. Calcification of vascular smooth muscle cells is induced by secondary calciprotein particles and enhanced by tumor necrosis factor-α. Atherosclerosis 2016, 251, 404–414. [Google Scholar] [CrossRef] [Green Version]
- Smith, E.R.; Hanssen, E.; McMahon, L.P.; Holt, S.G. Fetuin-A-containing calciprotein particles reduce mineral stress in the macrophage. PLoS ONE 2013, 8, e60904. [Google Scholar] [CrossRef] [Green Version]
- Tiemann, J.; Wagner, T.; Lindenkamp, C.; Plümers, R.; Faust, I.; Knabbe, C.; Hendig, D. Linking ABCC6 Deficiency in Primary Human Dermal Fibroblasts of PXE Patients to p21-Mediated Premature Cellular Senescence and the Development of a Proinflammatory Secretory Phenotype. Int. J. Mol. Sci. 2020, 21, 9665. [Google Scholar] [CrossRef]
- Bojic, M.; Koller, L.; Cejka, D.; Niessner, A.; Bielesz, B. Propensity for Calcification in Serum Associates with 2-Year Cardiovascular Mortality in Ischemic Heart Failure with Reduced Ejection Fraction. Front. Med. 2021, 8, 672348. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| All | T50 Tertile 1 (<316 min) | T50 Tertile 2 (316–368 min) | T50 Tertile 3 (>368 min) | Tertile Comp. p Value | Correlation Coefficient | Correlation p Value | |
|---|---|---|---|---|---|---|---|
| Number of participants, n | 57 | 19 | 19 | 19 | |||
| Age (years) | 45.2 ± 15.7 | 50.7 ± 12.0 | 43 ± 15.5 | 41.9 ± 18.3 | 0.17 | −0.28 | 0.033 * |
| Sex, % female (n) | 68.4 (39) | 52.6 (10) | 94.7 (18) | 57.9 (11) | 0.010 * | −0.01 | 0.94 |
| Current smoking, % (n) | 14.0 (8) | 15.8 (3) | 21.1 (4) | 5.3 (1) | 0.36 | −0.16 | 0.25 |
| Arterial hypertension, % (n) | 17.5 (10) | 21.1 (4) | 15.8 (3) | 15.8 (3) | 0.89 | −0.03 | 0.85 |
| Hypercholesterolemia, % (n) | 56.1 (32) | 52.6 (10) | 68.4 (13) | 47.4 (9) | 0.40 | −0.06 | 0.64 |
| Diabetes mellitus, % (n) | 1.8 (1) | 5.3 (1) | 0 (0) | 0 (0) | 0.36 | −0.17 | 0.20 |
| Body mass index (BMI) (kg/m2) | 25.4 ± 5.0 | 25.3 ± 5.8 | 26.1 ± 4.7 | 24.9 ± 4.6 | 0.78 | −0.15 | 0.26 |
| Serum calcium (mmol/L) | 2.38 ± 0.11 | 2.38 ± 0.10 | 2.38 ± 0.11 | 2.37 ± 0.13 | 0.90 | 0.004 | 0.98 |
| Serum magnesium (mmol/L) | 0.84 ± 0.06 | 0.84 ± 0.06 | 0.82 ± 0.07 | 0.87 ± 0.04 | 0.051 | 0.20 | 0.14 |
| Serum phosphorus (mmol/L) | 1.12 ± 0.17 | 1.18 ± 0.20 | 1.12 ± 0.14 | 1.05 ± 0.13 | 0.043 * | −0.34 | 0.009 * |
| Serum creatinine (mg/dL) | 0.82 ± 0.15 | 0.81 ± 0.18 | 0.78 ± 0.13 | 0.87 ± 0.15 | 0.26 | 0.13 | 0.35 |
| eGFR (ml/min/1.73 m2) | 95.4 ± 20.2 | 94.5 ± 18.0 | 95.8 ± 23.5 | 96.0 ± 20.0 | 0.97 | 0.11 | 0.41 |
| Serum alkaline phosphatase (U/L) | 70.5 ± 19.2 | 69.0 ± 16.4 | 71.4 ± 19.7 | 71.1 ± 21.9 | 0.92 | 0.09 | 0.50 |
| Serum fetuin-A (µg/mL) | 17.0 ± 3.1 | 15.3 ± 1.7 | 16.8 ± 3.2 | 18.8 ± 3.2 | 0.001 * | 0.44 | <0.001 * |
| Plasma inorganic pyrophosphate (PPi) (µmol/L) | 0.50 ± 0.16 | 0.53 ± 0.17 | 0.51 ± 0.17 | 0.46 ± 0.15 | 0.35 | −0.15 | 0.26 |
| Phenodex score | |||||||
| Skin (S) | 2 (1.5–2) | 2 (2–2) | 2 (2–2) | 2 (1–2) | 0.69 | −0.11 | 0.40 |
| Eye (E) | 2 (2–3) | 3 (2–3) | 2 (2–2.5) | 2 (2–2) | 0.041 * | −0.47 | <0.001 * |
| Vascular (V) | 1 (0–1) | 1 (1–1) | 0 (0–1) | 0 (0–1) | 0.093 | −0.38 | 0.003 * |
| Cardiac (C) | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0.35 | −0.12 | 0.36 |
| Gastrointestinal (G) | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0 (0–0) | NA | NA | NA |
| Renal (R) | 0 (0–1) | 0 (0–1) | 0 (0–0.5) | 0 (0–0.75) | 0.67 | −0.09 | 0.51 |
| Cumulative (Cu) | 5 (4–7) | 6.5 (6–7) | 5 (4–5.5) | 4 (3.25–5) | 0.014 * | −0.47 | <0.001 * |
| ABCC6 genotype | 0.93 | −0.03 | 0.86 | ||||
| LOF + missense, % (n) | 42.1 (24) | 36.8 (7) | 52.6 (10) | 36.8 (7) | NA | NA | NA |
| Missense + missense, % (n) | 15.8 (9) | 15.8 (3) | 15.8 (3) | 15.8 (3) | NA | NA | NA |
| LOF + LOF, % (n) | 26.3 (15) | 31.6 (6) | 15.8 (3) | 31.6 (6) | NA | NA | NA |
| Other (single or splice), % (n) | 15.8 (9) | 15.8 (3) | 15.8 (3) | 15.8 (3) | NA | NA | NA |
| cIMT (mm) (n = 16) | 0.64 ± 0.12 | 0.75 ± 0.13 | 0.63 ± 0.11 | 0.56 ± 0.08 | 0.068 | −0.57 | 0.022 * |
| cfPWV (m/s) (n = 14) | 8.7 ± 2.4 | 11.2 ± 1.8 | 9.0 ± 2.5 | 7.0 ± 1.08 | 0.11 | −0.61 | 0.020 * |
| CT calcium score (Agatston units) (n = 14) | 542 (4–2189) | 1091 (496–4537) | 524 (260–5001) | 2 (0–724) | 0.45 | −0.45 | 0.10 |
| Unstandardized Coefficients | Standardized Coefficients | T Value | p Value | ||
|---|---|---|---|---|---|
| Beta | SE | Beta | |||
| T50 (final model) | |||||
| (Constant) | 107.4 | 125.0 | |||
| Serum fetuin-A | 8.67 | 2.49 | 0.40 | 3.49 | <0.001 * |
| Serum phosphorus | −132.1 | 46.8 | −0.32 | −2.82 | 0.007 * |
| Serum magnesium | 283.9 | 130.7 | 0.25 | 2.17 | 0.034 * |
| Model summary | R | Adjusted R2 | ANOVA: F value | ANOVA: p value | |
| 0.58 | 0.30 | 8.80 | <0.001 * | ||
| Phenodex Eye (Final Model) | Parameter Estimates | p Value | Model Fitting | ||
| Estimate | SE | Chi-square | p Value | ||
| 33.4 | <0.001 * | ||||
| Age | 0.084 | 0.026 | 0.001 * | ||
| T50 | −0.014 | 0.006 | 0.013 * | ||
| Serum fetuin-A | −0.25 | 0.13 | 0.044 * | ||
| Phenodex Vascular (Final Model) | Parameter Estimates | p Value | Model Fitting | ||
| Estimate | SE | Chi-square | p value | ||
| 11.3 | 0.004 * | ||||
| Arterial hypertension | 1.42 | 0.69 | 0.039 * | ||
| T50 | −0.010 | 0.004 | 0.013 * | ||
| Phenodex Cumulative (Final Model) | Parameter Estimates | p Value | Model Fitting | ||
| Estimate | SE | Chi-square | p value | ||
| 16.2 | 0.001 * | ||||
| Age | 0.025 | 0.017 | 0.15 | ||
| Serum fetuin-A | −0.11 | 0.088 | 0.23 | ||
| T50 | −0.010 | 0.004 | 0.016 * | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nollet, L.; Van Gils, M.; Fischer, S.; Campens, L.; Karthik, S.; Pasch, A.; De Zaeytijd, J.; Leroy, B.P.; Devos, D.; De Backer, T.; et al. Serum Calcification Propensity T50 Associates with Disease Severity in Patients with Pseudoxanthoma Elasticum. J. Clin. Med. 2022, 11, 3727. https://doi.org/10.3390/jcm11133727
Nollet L, Van Gils M, Fischer S, Campens L, Karthik S, Pasch A, De Zaeytijd J, Leroy BP, Devos D, De Backer T, et al. Serum Calcification Propensity T50 Associates with Disease Severity in Patients with Pseudoxanthoma Elasticum. Journal of Clinical Medicine. 2022; 11(13):3727. https://doi.org/10.3390/jcm11133727
Chicago/Turabian StyleNollet, Lukas, Matthias Van Gils, Suzanne Fischer, Laurence Campens, Swapna Karthik, Andreas Pasch, Julie De Zaeytijd, Bart P. Leroy, Daniel Devos, Tine De Backer, and et al. 2022. "Serum Calcification Propensity T50 Associates with Disease Severity in Patients with Pseudoxanthoma Elasticum" Journal of Clinical Medicine 11, no. 13: 3727. https://doi.org/10.3390/jcm11133727
APA StyleNollet, L., Van Gils, M., Fischer, S., Campens, L., Karthik, S., Pasch, A., De Zaeytijd, J., Leroy, B. P., Devos, D., De Backer, T., Coucke, P. J., & Vanakker, O. M. (2022). Serum Calcification Propensity T50 Associates with Disease Severity in Patients with Pseudoxanthoma Elasticum. Journal of Clinical Medicine, 11(13), 3727. https://doi.org/10.3390/jcm11133727