
Integrated Cognitive Rehabilitation Home-Based Protocol to Improve Cognitive Functions in Multiple Sclerosis Patients: A Randomized Controlled Study




Abstract
:1. Introduction
2. Materials and Methods
2.1. Neuropsychological Assessments
2.1.1. California Verbal Learning Test (CVLT) and Brief Visuospatial Memory Test (BVMTR)
2.1.2. Numerical Stroop
2.1.3. Wisconsin Card Sorting Test (WCST)
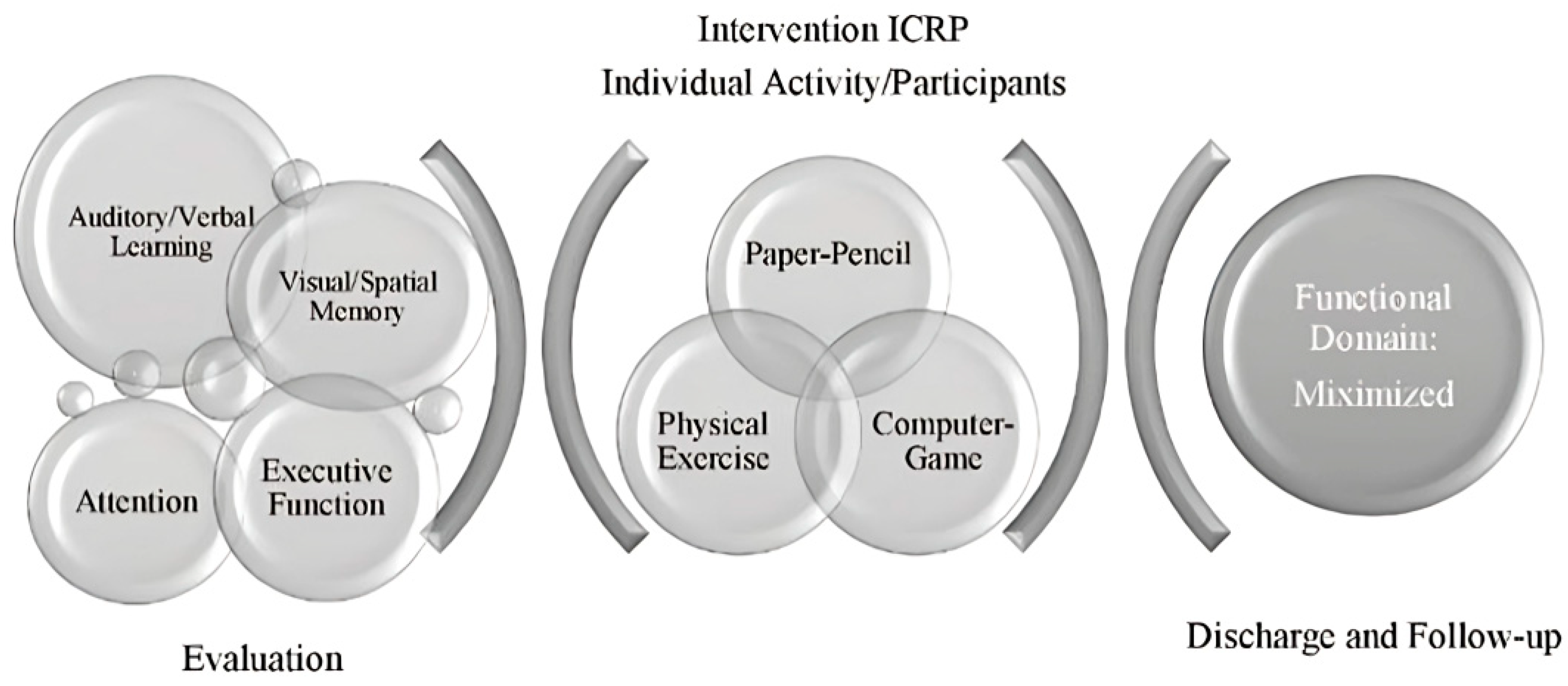
2.2. Integrated Cognitive Rehabilitation Program (ICRP)
2.2.1. General Considerations
2.2.2. Paper-Pencil
2.2.3. Computer-Game
2.2.4. Physical Exercise Intervention
2.3. Statistical Analysis
3. Results
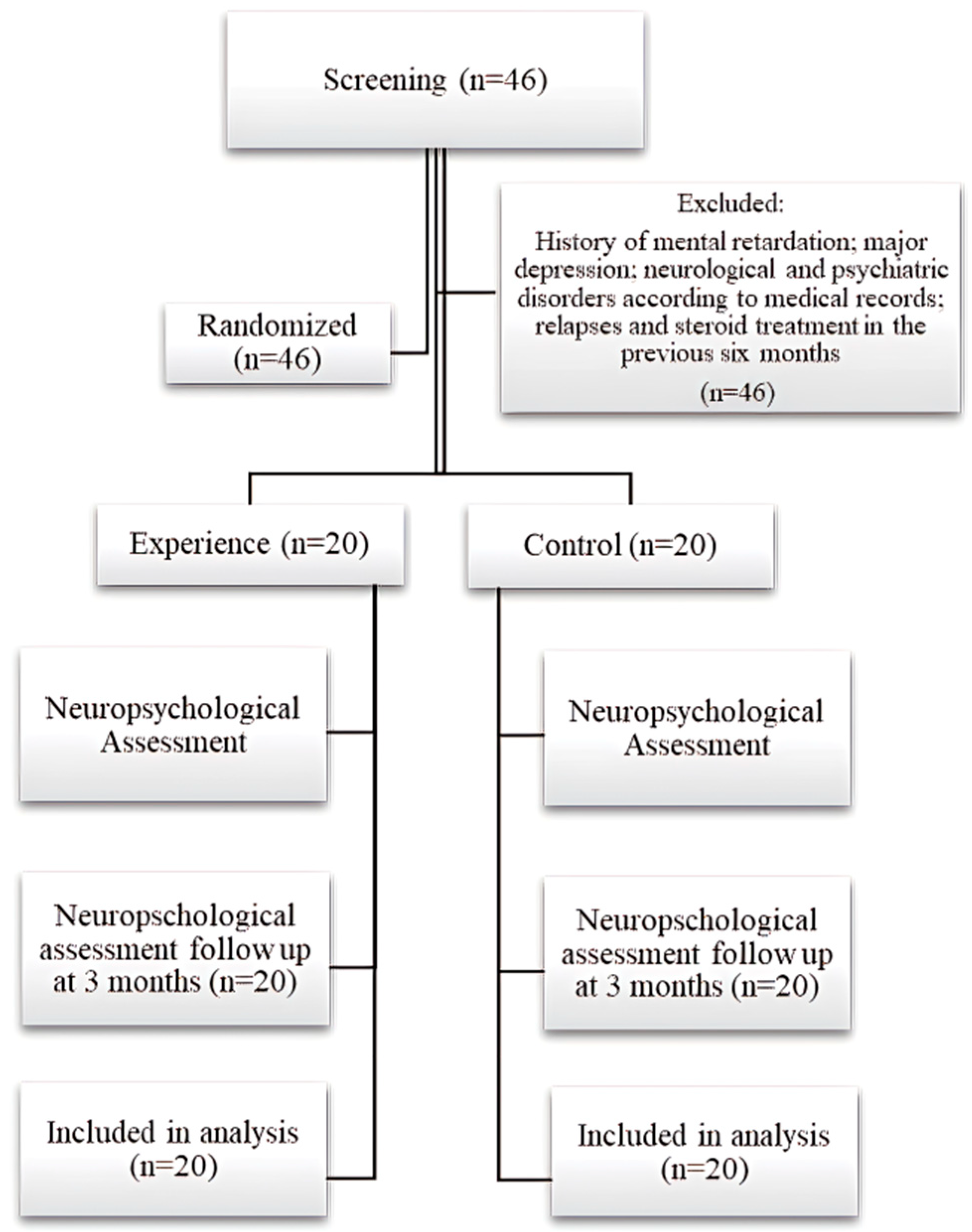
3.1. Characteristics of the Sample
3.1.1. Comparison of Demographic and Clinical Characteristics at Baseline (Pretreatment)
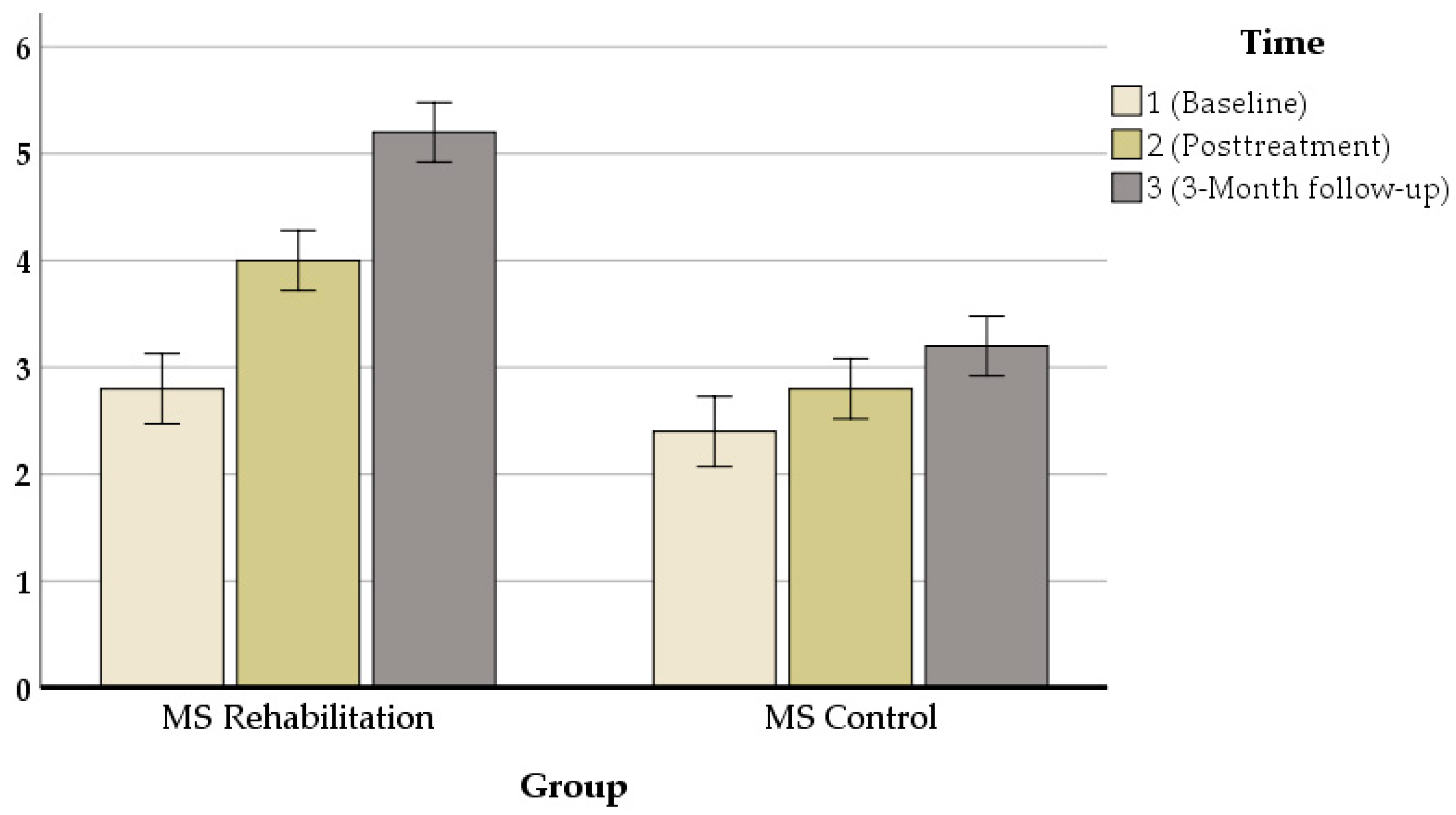
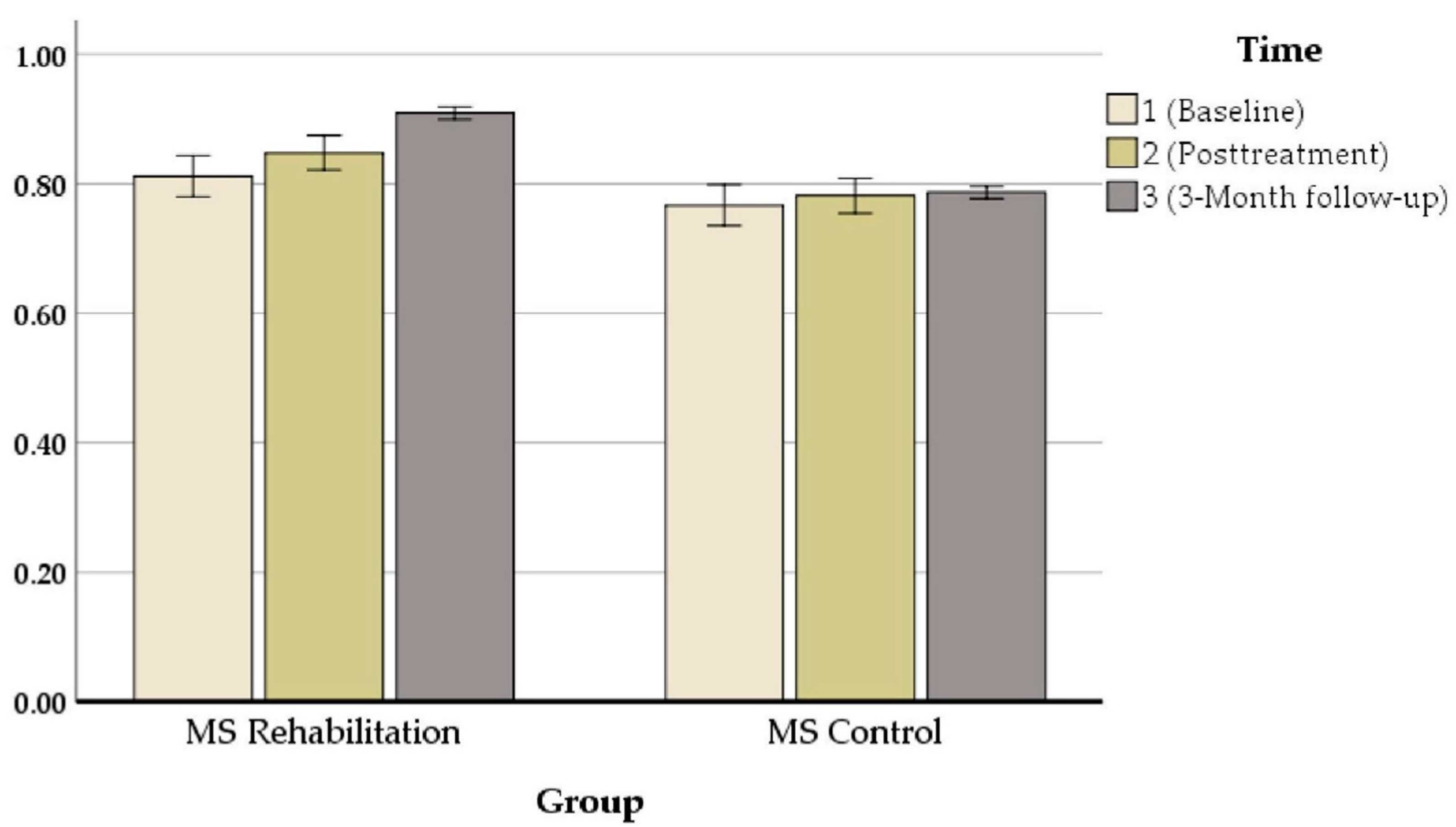
3.1.2. Comparison of Neuropsychological Test Performance for the ICRP MS-Experimental Group between Baseline, Posttreatment, and at 3-Month Follow-Up
3.1.3. Comparison of Neuropsychological Test Performance for the MS Standard Care Control Group between Baseline and Posttreatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hadoush, H.; Alawneh, A.; Kassab, M.; Al-Wardat, M.; Al-Jarrah, M. Effectiveness of non-pharmacological rehabilitation interventions in pain management in patients with multiple sclerosis: Systematic review and meta-analysis. Neurorehabilitation, 2022; preprint. [Google Scholar] [CrossRef] [PubMed]
- Hauser, S.L.; Cree, B.A.C. Treatment of Multiple Sclerosis: A Review. Am. J. Med. 2020, 133, 1380–1390.e2. [Google Scholar] [CrossRef] [PubMed]
- Dobson, R.; Giovannoni, G. Multiple sclerosis—A review. Eur. J. Neurol. 2019, 26, 27–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeLuca, G.C.; Yates, R.L.; Beale, H.; Morrow, S.A. Cognitive impairment in multiple sclerosis: Clinical, radiologic, and pathologic insights. Brain Pathol. 2015, 25, 79–98. [Google Scholar] [CrossRef]
- Glasner, P.; Sabisz, A.; Chylińska, M.; Komendziński, J.; Wyszomirski, A.; Karaszewski, B. Retinal nerve fiber and ganglion cell complex layer thicknesses mirror brain atrophy in patients with relapsing-remitting multiple sclerosis. Restor. Neurol. Neurosci. 2022, 40, 35–42. [Google Scholar] [CrossRef]
- Hämäläinen, P.; Rosti-Otajärvi, E. Cognitive impairment in MS: Rehabilitation approaches. Acta Neurol. Scand. 2016, 134, 8–13. [Google Scholar] [CrossRef] [Green Version]
- Niino, M.; Miyazaki, Y. Cognitive Impairment in Multiple Sclerosis. Brain Nerve 2020, 72, 509–515. [Google Scholar] [CrossRef]
- Planche, V.; Gibelin, M.; Cregut, D.; Pereira, B.; Clavelou, P. Cognitive impairment in a population-based study of patients with multiple sclerosis: Differences between late relapsing-remitting, secondary progressive and primary progressive multiple sclerosis. Eur. J. Neurol. 2016, 23, 282–289. [Google Scholar] [CrossRef]
- Ruano, L.; Portaccio, E.; Goretti, B.; Niccolai, C.; Severo, M.; Patti, F.; Cilia, S.; Gallo, P.; Grossi, P.; Ghezzi, A.; et al. Age and disability drive cognitive impairment in multiple sclerosis across disease subtypes. Mult. Scler. J. 2016, 23, 1258–1267. [Google Scholar] [CrossRef] [Green Version]
- Dackovic, J.; Pekmezovic, T.; Mesaros, S.; Dujmovic, I.; Stojsavljevic, N.; Martinovic, V.; Drulovic, J. The Rao’s Brief Repeatable Battery in the study of cognition in different multiple sclerosis phenotypes: Application of normative data in a Serbian population. Neurol. Sci. 2016, 37, 1475–1481. [Google Scholar] [CrossRef]
- Longoni, G.; Rocca, M.A.; Pagani, E.; Riccitelli, G.C.; Colombo, B.; Rodegher, M.; Falini, A.; Comi, G.; Filippi, M. Deficits in memory and visuospatial learning correlate with regional hippocampal atrophy in MS. Anat. Embryol. 2015, 220, 435–444. [Google Scholar] [CrossRef] [PubMed]
- Balsimelli, S.; Mendes, M.F.; Bertolucci, P.H.; Tilbery, C.P. Attention impairment associated with relapsing-remitting multiple sclerosis patients with mild incapacity. Arq. Neuropsiquiatr. 2007, 65, 262–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wuerfel, E.; Weddige, A.; Hagmayer, Y.; Jacob, R.; Wedekind, L.; Stark, W.; Gärtner, J. Cognitive deficits including executive functioning in relation to clinical parameters in paediatric MS patients. PLoS ONE 2018, 13, e0194873. [Google Scholar] [CrossRef] [PubMed]
- De Meo, E.; Portaccio, E.; Giorgio, A.; Ruano, L.; Goretti, B.; Niccolai, C.; Patti, F.; Chisari, C.G.; Gallo, P.; Grossi, P.; et al. Identifying the Distinct Cognitive Phenotypes in Multiple Sclerosis. JAMA Neurol. 2021, 78, 414. [Google Scholar] [CrossRef]
- Sehanovic, A.; Smajlovic, D.; Tupkovic, E.; Ibrahimagic, O.C.; Kunic, S.; Dostovic, Z.; Zoletic, E.; Pasic, Z. Cognitive Disorders in Patients with Multiple Sclerosis. Mater. Socio Med. 2020, 32, 191–195. [Google Scholar] [CrossRef]
- Paul, F. Pathology and MRI: Exploring cognitive impairment in MS. Acta Neurol. Scand. 2016, 134, 24–33. [Google Scholar] [CrossRef]
- Campanholo, K.; Pitombeira, M.; Rimkus, C.; Mendes, M.; Apóstolos-Pereira, S.; Filho, G.B.; Callegaro, D.; Buchpiguel, C.; Duran, F.; Faria, D.D.P. Myelin imaging measures as predictors of cognitive impairment in MS patients: A hybrid PET-MRI study. Mult. Scler. Relat. Disord. 2021, 57, 103331. [Google Scholar] [CrossRef]
- Riccitelli, G.C.; Pagani, E.; Meani, A.; Valsasina, P.; Preziosa, P.; Filippi, M.; Rocca, M.A. Cognitive impairment in benign multiple sclerosis: A multiparametric structural and functional MRI study. J. Neurol. 2020, 267, 3508–3517. [Google Scholar] [CrossRef]
- Nasios, G.; Bakirtzis, C.; Messinis, L. Cognitive Impairment and Brain Reorganization in MS: Underlying Mechanisms and the Role of Neurorehabilitation. Front. Neurol. 2020, 11, 147. [Google Scholar] [CrossRef]
- Khan, F.; Amatya, B. Rehabilitation in Multiple Sclerosis: A Systematic Review of Systematic Reviews. Arch. Phys. Med. Rehabil. 2017, 98, 353–367. [Google Scholar] [CrossRef]
- Amatya, B.; Khan, F.; Galea, M. Rehabilitation for people with multiple sclerosis: An overview of Cochrane Reviews. Cochrane Database Syst. Rev. 2019, 1, CD012732. [Google Scholar] [CrossRef] [PubMed]
- Bonavita, S.; Sacco, R.; Della Corte, M.; Esposito, S.; Sparaco, M.; D’Ambrosio, A.; Docimo, R.; Bisecco, A.; Lavorgna, L.; Corbo, D.; et al. Computer-aided cognitive rehabilitation improves cognitive performances and induces brain functional connectivity changes in relapsing remitting multiple sclerosis patients: An exploratory study. J. Neurol. 2014, 262, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Zuber, P.; Tsagkas, C.; Papadopoulou, A.; Gaetano, L.; Huerbin, M.; Geiter, E.; Altermatt, A.; Parmar, K.; Ettlin, T.; Schuster-Amft, C.; et al. Efficacy of inpatient personalized multidisciplinary rehabilitation in multiple sclerosis: Behavioural and functional imaging results. J. Neurol. 2020, 267, 1744–1753. [Google Scholar] [CrossRef] [PubMed]
- McGinley, M.P.; Goldschmidt, C.H.; Rae-Grant, A.D. Diagnosis and Treatment of Multiple Sclerosis: A Review. JAMA 2021, 325, 765–779. [Google Scholar] [CrossRef] [PubMed]
- Lenehan, P.; Deane, F.P.; Wolstencroft, K.; Kelly, P.J. Coherence between goals and therapeutic homework of clients engaging in recovery-oriented support. Psychiatr. Rehabil. J. 2019, 42, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Shatil, E.; Metzer, A.; Horvitz, O.; Miller, A. Home-based personalized cognitive training in MS patients: A study of adherence and cognitive performance. NeuroRehabilitation 2010, 26, 143–153. [Google Scholar] [CrossRef]
- Stuifbergen, A.; Becker, H.; Morgan, S.; Morrison, J.; Perez, F. Home-Based Computer-Assisted Cognitive Training: Feasibility and Perceptions of People with Multiple Sclerosis. Int. J. MS Care 2011, 13, 189–198. [Google Scholar] [CrossRef]
- Feinstein, A.; On behalf of the CogEx Research Team; Amato, M.P.; Brichetto, G.; Chataway, J.; Chiaravalloti, N.; Dalgas, U.; DeLuca, J.; Feys, P.; Filippi, M.; et al. Study protocol: Improving cognition in people with progressive multiple sclerosis: A multi-arm, randomized, blinded, sham-controlled trial of cognitive rehabilitation and aerobic exercise (COGEx). BMC Neurol. 2020, 20, 204. [Google Scholar] [CrossRef]
- Filippi, M.; Riccitelli, G.; Mattioli, F.; Capra, R.; Stampatori, C.; Pagani, E.; Valsasina, P.; Copetti, M.; Falini, A.; Comi, G.; et al. Multiple Sclerosis: Effects of Cognitive Rehabilitation on Structural and Functional MR Imaging Measures—An Explorative Study. Radiology 2012, 262, 932–940. [Google Scholar] [CrossRef]
- Péran, P.; Nemmi, F.; Dutilleul, C.; Finamore, L.; Caravasso, C.F.; Troisi, E.; Iosa, M.; Sabatini, U.; Grasso, M.G. Neuroplasticity and brain reorganization associated with positive outcomes of multidisciplinary rehabilitation in progressive multiple sclerosis: A fMRI study. Mult. Scler. Relat. Disord. 2020, 42, 102127. [Google Scholar] [CrossRef]
- Lublin, F.D.; Reingold, S.C.; Cohen, J.A.; Cutter, G.R.; Sørensen, P.S.; Thompson, A.J.; Wolinsky, J.S.; Balcer, L.J.; Banwell, B.; Barkhof, F.; et al. Defining the clinical course of multiple sclerosis: The 2013 revisions. Neurology 2014, 83, 278–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rilo, O.; Peña, J.; Ojeda, N.; Rodríguez-Antigüedad, A.; Mendibe-Bilbao, M.; Gómez-Gastiasoro, A.; DeLuca, J.; Chiaravalloti, N.; Ibarretxe-Bilbao, N. Integrative group-based cognitive rehabilitation efficacy in multiple sclerosis: A randomized clinical trial. Disabil. Rehabil. 2016, 40, 208–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inojosa, H.; Schriefer, D.; Ziemssen, T. Clinical outcome measures in multiple sclerosis: A review. Autoimmun. Rev. 2020, 19, 102512. [Google Scholar] [CrossRef]
- Benedict, R.H.B.; Amato, M.P.; Boringa, J.; Brochet, B.; Foley, F.; Fredrikson, S.; Hamalainen, P.; Hartung, H.; Krupp, L.; Penner, I.; et al. Brief International Cognitive Assessment for MS (BICAMS): International standards for validation. BMC Neurol. 2012, 12, 55. [Google Scholar] [CrossRef] [Green Version]
- Dadon, G.; Henik, A. Adjustment of control in the numerical Stroop task. Mem. Cogn. 2017, 45, 891–902. [Google Scholar] [CrossRef] [Green Version]
- Kopp, B.; Lange, F.; Steinke, A. The Reliability of the Wisconsin Card Sorting Test in Clinical Practice. Assessment 2019, 28, 248–263. [Google Scholar] [CrossRef]
- Barbarulo, A.M.; Lus, G.; Signoriello, E.; Trojano, L.; Grossi, D.; Esposito, M.; Costabile, T.; Lanzillo, R.; Saccà, F.; Morra, V.B.; et al. Integrated Cognitive and Neuromotor Rehabilitation in Multiple Sclerosis: A Pragmatic Study. Front. Behav. Neurosci. 2018, 12, 196. [Google Scholar] [CrossRef]
- Fleeman, J.A.; Stavisky, C.; Carson, S.; Dukelow, N.; Maier, S.; Coles, H.; Wager, J.; Rice, J.; Essaff, D.; Scherer, M. Integrating cognitive rehabilitation: A preliminary program description and theoretical review of an interdisciplinary cognitive rehabilitation program. NeuroRehabilitation 2015, 37, 471–486. [Google Scholar] [CrossRef]
- Faria, A.L.; Pinho, M.S.; Badia, S.B.I. A comparison of two personalization and adaptive cognitive rehabilitation approaches: A randomized controlled trial with chronic stroke patients. J. Neuroeng. Rehabil. 2020, 17, 78. [Google Scholar] [CrossRef]
- Messinis, L.; Nasios, G.; Kosmidis, M.; Zampakis, P.; Malefaki, S.; Ntoskou, K.; Nousia, A.; Bakirtzis, C.; Grigoriadis, N.; Gourzis, P.; et al. Efficacy of a Computer-Assisted Cognitive Rehabilitation Intervention in Relapsing-Remitting Multiple Sclerosis Patients: A Multicenter Randomized Controlled Trial. Behav. Neurol. 2017, 2017, 15919841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centonze, D.; Leocani, L.; Feys, P. Advances in physical rehabilitation of multiple sclerosis. Curr. Opin. Neurol. 2020, 33, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Field, A. Discovering Statistics Using IBM SPSS Statistics, 4th ed.; SAGE Publications: London, UK, 2013. [Google Scholar]
- Pallant, J. SPSS Survival Manual: A Step by Step Guide to Data Analysis Using IBM SPSS; Routledge: Oxfordshire, UK, 2020. [Google Scholar]
- Ghahfarrokhi, M.M.; Banitalebi, E.; Negaresh, R.; Motl, R.W. Home-Based Exercise Training in Multiple Sclerosis: A Systematic Review with Implications for Future Research. Mult. Scler. Relat. Disord. 2021, 55, 103177. [Google Scholar] [CrossRef] [PubMed]
- Harand, C.; Daniel, F.; Mondou, A.; Chevanne, D.; Creveuil, C.; Defer, G. Neuropsychological management of multiple sclerosis: Evaluation of a supervised and customized cognitive rehabilitation program for self-used at home (SEPIA): Protocol for a randomized controlled trial. Trials 2019, 20, 614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson, J.C.; Ely, E.W.; Morey, M.C.; Anderson, V.M.; Denne, L.B.; Clune, J.; Siebert, C.S.; Archer, K.R.; Torres, R.; Janz, D.; et al. Cognitive and physical rehabilitation of intensive care unit survivors. Crit. Care Med. 2012, 40, 1088–1097. [Google Scholar] [CrossRef] [Green Version]
- Gómez-Gastiasoro, A.; Peña, J.; Ibarretxe-Bilbao, N.; Lucas-Jiménez, O.; Díez-Cirarda, M.; Rilo, O.; Montoya-Murillo, G.; Zubiaurre-Elorza, L.; Ojeda, N. A Neuropsychological Rehabilitation Program for Cognitive Impairment in Psychiatric and Neurological Conditions: A Review That Supports Its Efficacy. Behav. Neurol. 2019, 2019, 4647134. [Google Scholar] [CrossRef]
- Campbell, J.; Langdon, D.; Cercignani, M.; Rashid, W. A Randomised Controlled Trial of Efficacy of Cognitive Rehabilitation in Multiple Sclerosis: A Cognitive, Behavioural, and MRI Study. Neural Plast. 2016, 2016, 4292585. [Google Scholar] [CrossRef]
- Prosperini, L.; Di Filippo, M. Beyond clinical changes: Rehabilitation-induced neuroplasticity in MS. Mult. Scler. 2019, 25, 1348–1362. [Google Scholar] [CrossRef]
- Prosperini, L.; Piattella, M.C.; Giannì, C.; Pantano, P. Functional and Structural Brain Plasticity Enhanced by Motor and Cognitive Rehabilitation in Multiple Sclerosis. Neural Plast. 2015, 2015, 481574. [Google Scholar] [CrossRef] [Green Version]
- Sandroff, B.M.; Motl, R.W.; Reed, W.R.; Barbey, A.K.; Benedict, R.H.B.; DeLuca, J. Integrative CNS Plasticity with Exercise in MS: The PRIMERS (PRocessing, Integration of Multisensory Exercise-Related Stimuli) Conceptual Framework. Neurorehabil Neural Repair 2018, 32, 847–862. [Google Scholar] [CrossRef]
- Sandroff, B.M.; Jones, C.D.; Baird, J.F.; Motl, R.W. Systematic Review on Exercise Training as a Neuroplasticity-Inducing Behavior in Multiple Sclerosis. Neurorehabil. Neural Repair 2020, 34, 575–588. [Google Scholar] [CrossRef] [PubMed]
- Landmeyer, N.C.; Bürkner, P.-C.; Wiendl, H.; Ruck, T.; Hartung, H.-P.; Holling, H.; Meuth, S.G.; Johnen, A. Disease-modifying treatments and cognition in relapsing-remitting multiple sclerosis. Neurology 2020, 94, e2373–e2383. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Experimental Group (n = 20) | Control Group (n = 20) | U/x2 | df | p | |
|---|---|---|---|---|---|---|
| Sex | Mean (SD) (95% CI) | 1.3 ± 0.47 | 1.2 ± 0.41 | 149.00 | 39 | 0.988 |
| Female (%) | 14 (70) | 16 (80) | ||||
| Male (%) | 6 (30) | 4 (20) | ||||
| Age years | Mean (SD) (95% CI) | 34.15 ± 8.36 | 31.85 ± 8.25 | 0.512 | 1 | 0.774 |
| 18–30 (%) | 7 (35) | 10 (50) | ||||
| 31–43 (%) | 9 (45) | 7 (35) | ||||
| 44–56 (%) | 4 (20) | 3 (15) | ||||
| Disease duration years | Mean (SD) (95% CI) | 7.6 ± 4.32 | 7.8 ± 2.28 | 4.489 | 1 | 0.106 |
| 2–8 (%) | 15 (75) | 14 (70) | ||||
| 9–14 (%) | 3 (15) | 3 (15) | ||||
| 15–21 (%) | 2 (10) | 3 (15) | ||||
| History of MS disease in the family | Mean (SD) (95% CI) | 1.3 ± 0.47 | 1.2 ± 0.41 | 208.00 | 39 | 0.072 |
| With history (%) | 6 (30) | 4 (20) | ||||
| Without history (%) | 14 (70) | 16 (80) | ||||
| Phenotypes of MS | Mean (SD) (95% CI) | 1.75 ± 0.85 | 1.5 ± 0.82 | 4.305 | 1 | 0.116 |
| Relapsing-remitting (RRMS) (%) | 10 (50) | 14 (70) | ||||
| Primary-progressive MS (PPMS) (%) | 5 (25) | 2 (10) | ||||
| Secondary-progressive (SPMS) (%) | 5 (25) | 4 (20) | ||||
| Disease-modifying therapies (DMTs) | Interferon β-1b (%) | 4 (20) | 5 (25) | 190.00 | 39 | 0.892 |
| Glatiramer acetate (%) | 6 (30) | 5 (25) | ||||
| Ocrelizumab (%) | 10 (50) | 10 (50) | ||||
| Measure | Time Period | Experimental Group | Control Group | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| CVLT | T0 | 3/37 | 0/413 | 3/10 | 0/391 |
| T1 | 3/68 | 0/418 | 3/33 | 0/395 | |
| T2 | 6/75 | 0/827 | 3/75 | 0/401 | |
| BVMTR | T0 | 2/80 | 0/89 | 2/40 | 0/50 |
| T1 | 4 | 0/77 | 2/80 | 0/41 | |
| T2 | 5/20 | 0/76 | 3/20 | 0/41 | |
| Attention | T0 | 0/42 | 0/22 | 0/49 | 0/27 |
| T1 | 0/62 | 0/15 | 0/50 | 0/27 | |
| T2 | 0/88 | 0/08 | 0/52 | 0/28 | |
| Executive Function | T0 | 0/81 | 0/09 | 0/76 | 0/03 |
| T1 | 0/84 | 0/07 | 0/78 | 0/03 | |
| T2 | 0/90 | 0/007 | 0/78 | 0/02 | |
| Value | f | p-Value | Effect Size | Observed Power | ||
|---|---|---|---|---|---|---|
| CVLT | Time | 0.363 | 66.681 | 0.000 | 0.637 | 1 |
| Time × group | 0.494 | 38.816 | 0.000 | 0.505 | 1 | |
| BVMTR | Time | 0.089 | 389.120 | 0.000 | 0.911 | 1 |
| Time × group | 0.281 | 97.280 | 0.000 | 0.719 | 1 | |
| Attention | Time | 0.276 | 48.623 | 0.000 | 0.724 | 1 |
| Time × group | 0.339 | 36.124 | 0.000 | 0.661 | 1 | |
| Executive Function | Time | 0.328 | 37.913 | 0.000 | 0.672 | 1 |
| Time × group | 0.697 | 8.005 | 0.001 | 0.302 | 0.95 |
| Baseline | Posttreatment | 3-Month Follow-Up | Baseline versus Posttreatment p-Values | Effect Size (r) | Baseline versus Follow-Up p-Values | ||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | Median | Mean | Median | Mean | Median | ||||
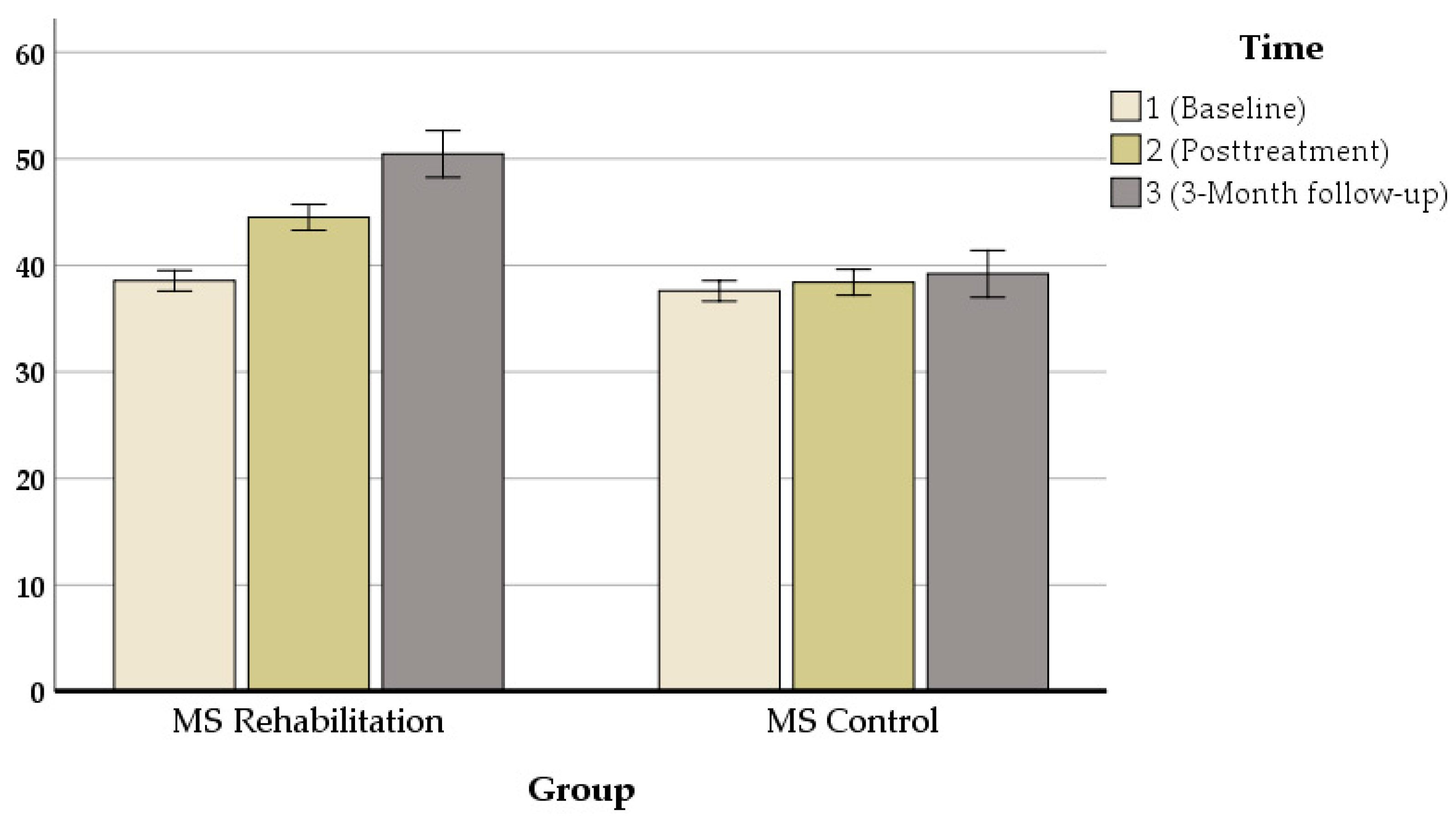
| CVLT | 38.55 | 38 | 44.50 | 43.50 | 50.45 | 48.50 | 0.000 *** | 0.996 | 0.000 |
| BVMTR | 2.80 | 2.50 | 4 | 3.75 | 5.20 | 5 | 0.000 *** | 0.996 | 0.000 |
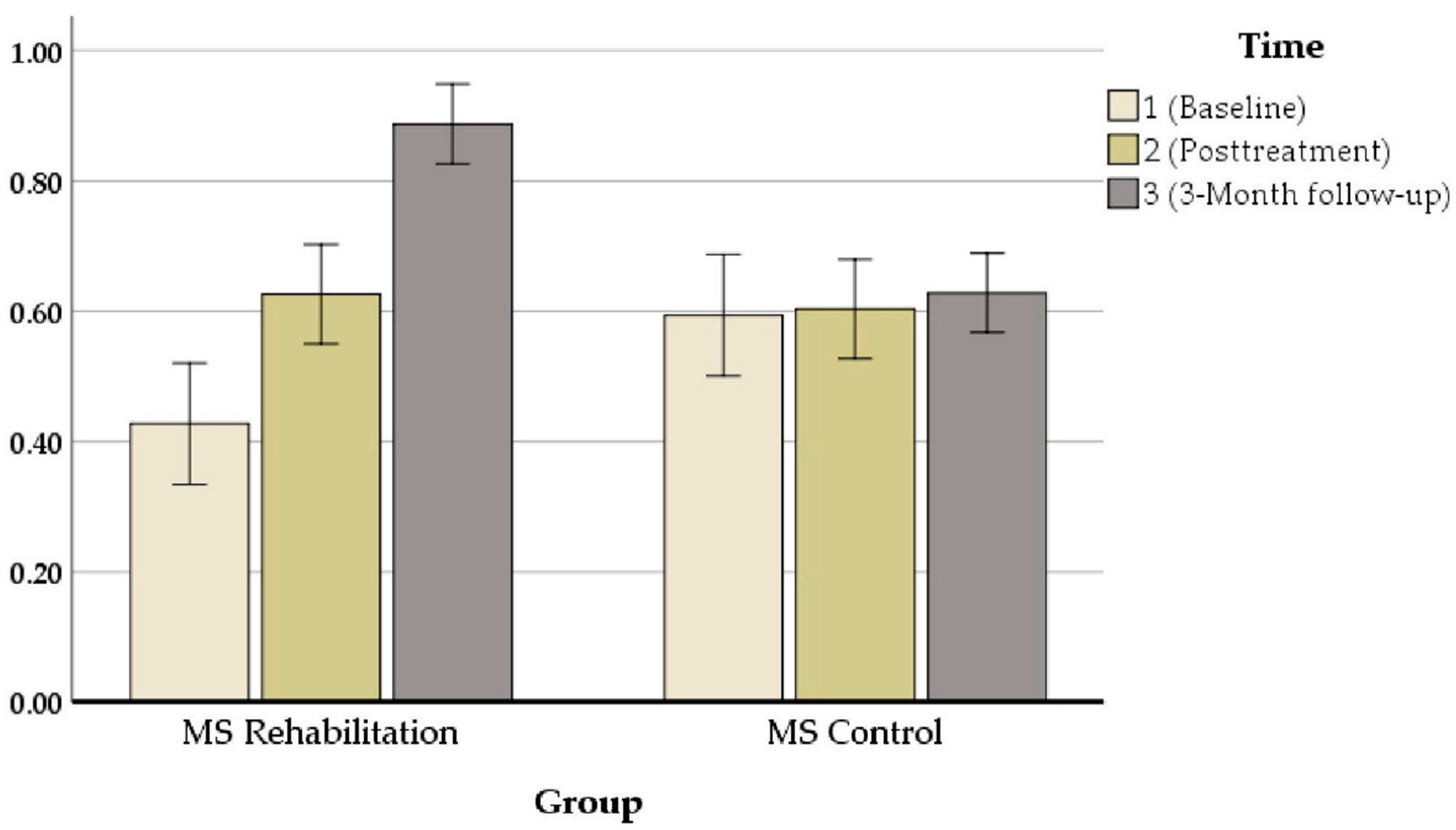
| Attention | 0.427 | 0.445 | 0.626 | 0.670 | 0.887 | 0.90 | 0.000 *** | 0.944 | 0.000 |
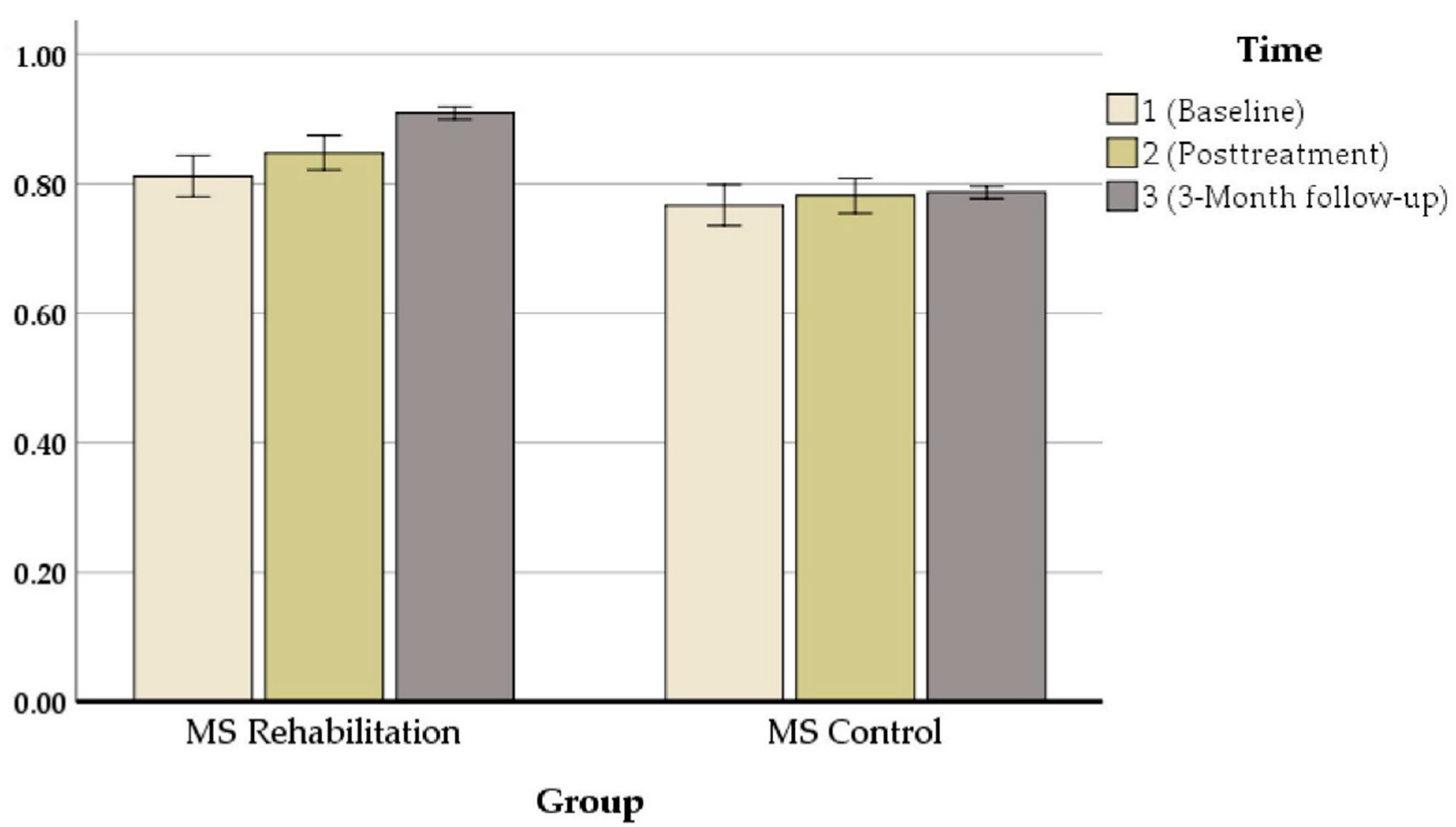
| Executive Function | 0.811 | 0.840 | 0.847 | 0.875 | 0.909 | 0.910 | 0.000 *** | 0.997 | 0.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sharbafshaaer, M.; Trojsi, F.; Bonavita, S.; Azimi, A. Integrated Cognitive Rehabilitation Home-Based Protocol to Improve Cognitive Functions in Multiple Sclerosis Patients: A Randomized Controlled Study. J. Clin. Med. 2022, 11, 3560. https://doi.org/10.3390/jcm11123560
Sharbafshaaer M, Trojsi F, Bonavita S, Azimi A. Integrated Cognitive Rehabilitation Home-Based Protocol to Improve Cognitive Functions in Multiple Sclerosis Patients: A Randomized Controlled Study. Journal of Clinical Medicine. 2022; 11(12):3560. https://doi.org/10.3390/jcm11123560
Chicago/Turabian StyleSharbafshaaer, Minoo, Francesca Trojsi, Simona Bonavita, and Amirreza Azimi. 2022. "Integrated Cognitive Rehabilitation Home-Based Protocol to Improve Cognitive Functions in Multiple Sclerosis Patients: A Randomized Controlled Study" Journal of Clinical Medicine 11, no. 12: 3560. https://doi.org/10.3390/jcm11123560
APA StyleSharbafshaaer, M., Trojsi, F., Bonavita, S., & Azimi, A. (2022). Integrated Cognitive Rehabilitation Home-Based Protocol to Improve Cognitive Functions in Multiple Sclerosis Patients: A Randomized Controlled Study. Journal of Clinical Medicine, 11(12), 3560. https://doi.org/10.3390/jcm11123560