
Bridge Nodes between Personality Traits and Alcohol-Use Disorder Criteria: The Relevance of Externalizing Traits of Risk Taking, Callousness, and Irresponsibility

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Measures
2.3. Procedure
2.4. Data Analysis
3. Results
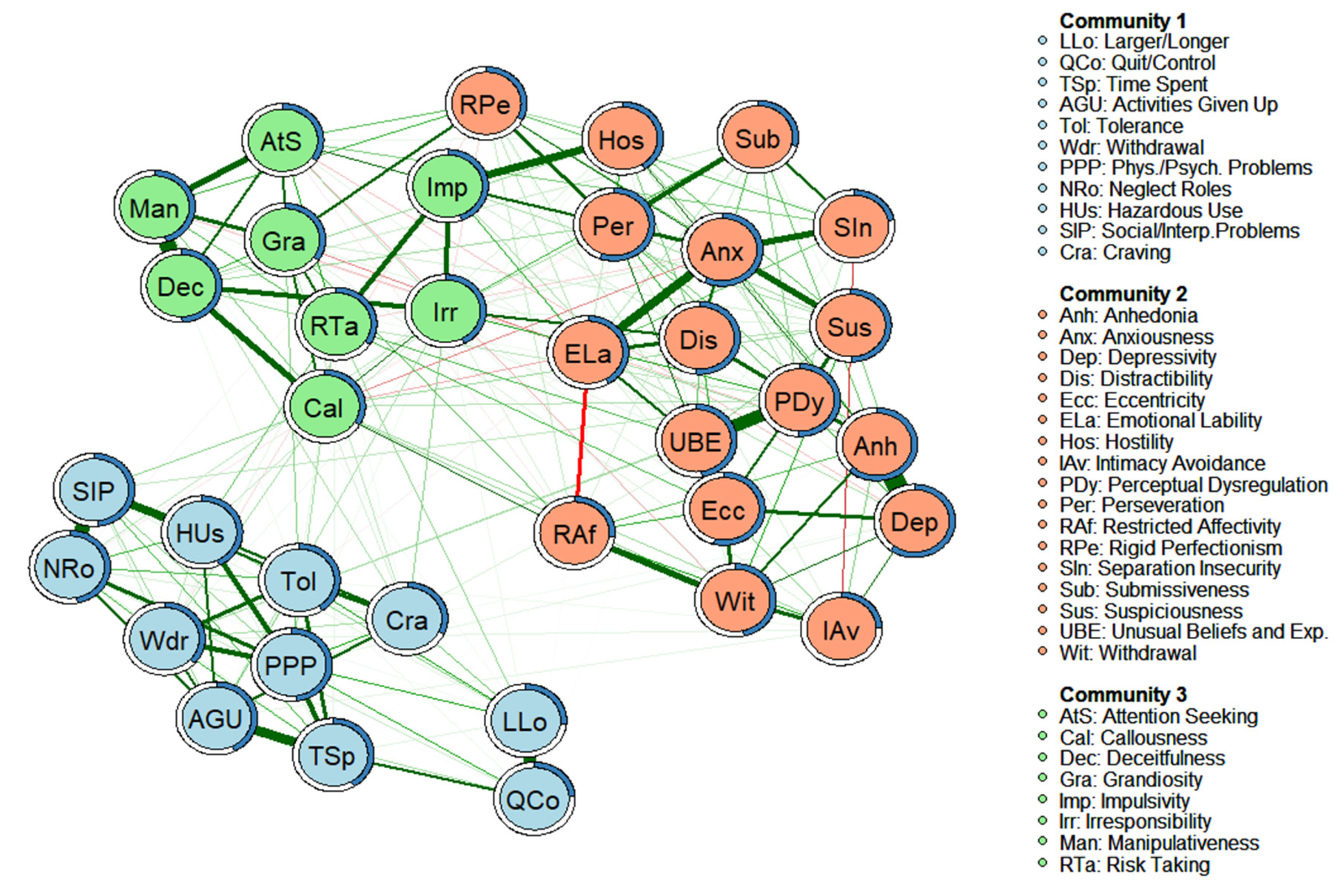
3.1. Network Structure with AMPD Personality Facets and AUD Criteria, and Invariance According to Gender
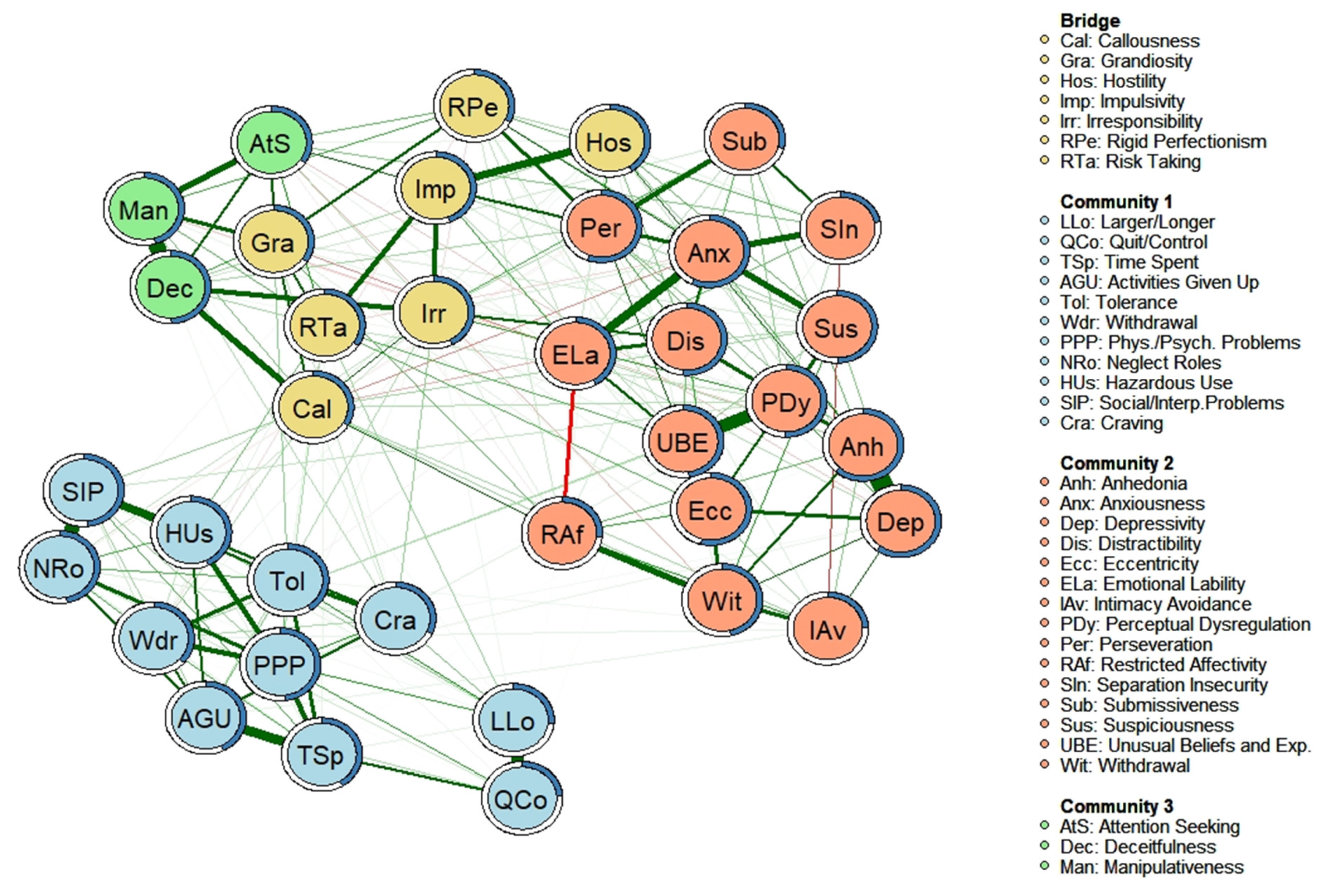
3.2. “Bridging Nodes” between AUD Criteria and Personality Facets
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Global Status Report on Alcohol and Health; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Kapoor, M.; Wang, J.; Farris, S.; Liu, Y.; McClintick, J.; Gupta, I.; Goate, A. Analysis of whole genome-transcriptomic organization in brain to identify genes associated with alcoholism. Transl. Psychiatry 2019, 9, 89. [Google Scholar] [CrossRef] [PubMed]
- Pearson, M.; Hustad, J. Personality and alcohol-related outcomes among mandated college students: Descriptive norms, injunctive norms, and college-related alcohol beliefs as mediatiors. Addit. Behav. 2014, 39, 879–884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwako, L.; Schawandt, M.; Ramchandani, V.; Diazgranados, N.; Koob, G.; Volkow, N.; Blanco, C.; Goldman, D. Neurofunctional domains derived from deep behavioral phenotyping in alcohol use disorder. Am. J. Psychiatry 2019, 176, 744–753. [Google Scholar] [CrossRef] [PubMed]
- Cavicchioli, M.; Ramella, P.; Movalli, M.; Prudenziati, F.; Vassena, G.; Simone, G.; Maffei, C. DSM-5 maladaptive personality domains among treatment-seeking individuals with alcohol use disorder: The role of deshinibition and negative affectivity. Subst. Use Misuse 2020, 55, 1746–1758. [Google Scholar] [CrossRef] [PubMed]
- Trull, T.J.; Jahng, S.; Tomko, R.L.; Wood, P.K.; Sher, K.J. Revised NESARC personality disorder diagnoses: Gender, prevalence, and comorbidity with substance dependence disorders. J. Personal. Disord. 2010, 24, 412–426. [Google Scholar] [CrossRef]
- Grant, B.; Goldstein, R.B.; Saha, T.; Chou, P.; Jung, J.; Zhang, H.; Hasin, D. Epidemiology of DSM-5 Alcohol Use Disorder: Results from the National Epidemiologic Survey on Alcohol and Related Conditions III. JAMA Psychiatry 2015, 72, 757–766. [Google Scholar] [CrossRef] [Green Version]
- Guy, K.; Newton-Howes, G.; Ford, H.; Williman, J.; Foulds, J. The prevalence of comorbid alcohol use disorder in the presence of personality disorder: Systematic review and explanatory modelling. Personal. Ment. Health 2018, 12, 216–228. [Google Scholar] [CrossRef]
- Trull, T.J.; Solham, M.B.; Brown, W.C.; Tomko, R.L.; Schaefer, L.; Jahng, S. Substance Use Disorders and Personality Disorders; Sher, K., Ed.; Oxford Handbook of Substance Use Disorders; Oxford University Press: New York, NY, USA, 2016. [Google Scholar]
- Malouf, J.M.; Thirsteinsson, E.; Rooke, S.; Chutte, N. Alcohol involvement and the Five-Factor Model of personality: A meta-analysis. J. Drug Educ. 2007, 37, 277–294. [Google Scholar] [CrossRef]
- Kotov, R.; Gamez, W.; Schimidt, F.; Watson, D. Linking “Big” Personality traits to anxiety, depressive, and substance use disorders: A meta-analysis. Psychol. Bull. 2010, 136, 768–821. [Google Scholar] [CrossRef]
- Hakulinen, C.; Elovainio, M.; Batty, G.D.; Virtanen, M.; Kivimäki, M.; Jokela, M. Personality and alcohol consumption: Pooled analysis of 72,949 adults from eight cohort studies. Drug Alcohol Depend. 2015, 151, 110–114. [Google Scholar] [CrossRef] [Green Version]
- Moraleda, E.; Ramírez-lopez, J.; Fernández-Calderón, F.; Lozano, O.M.; Díaz-Batanero, C. Personality traits among the variuos profiles of substance use disorder patients: New evidence using the DSM-5 Section III Framework. Eur. Addict. Res. 2019, 25, 238–247. [Google Scholar] [CrossRef] [PubMed]
- Ronningstam, E.; Keng, S.L.; Ridolfi, M.E.; Arbabi, M.; Grenyer, B. Cultural aspects in symptomatology, assessment and treatment of personality disorders. Curr. Psychiatry Rep. 2018, 20, 22. [Google Scholar] [CrossRef] [PubMed]
- Contreras, A.; Nieto, I.; Valiente, C.; Espinosa, R.; Vazquez, C. The study of psychopathology from the network analysis perspective: A systematic review. Psychother. Psychosom. 2019, 88, 71–83. [Google Scholar] [CrossRef] [PubMed]
- Borsboom, D. A network theory of mental disorders. World Psychiatry 2017, 16, 5–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borsboom, D.; Cramer, A.O.J. Network analysis: An integrative approach to the structure of psychopathology. Annu. Rev. Clin. Psychol. 2013, 9, 91–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boccaletti, S.; Latora, V.; Moreno, Y.; Chavez, M.; Hwang, D.U. Complex networks: Structure and dynamics. Phys. Rep. 2006, 424, 175–308. [Google Scholar] [CrossRef]
- Kendler, K.S.; Zachar, P.; Craver, C. What kinds of things are psychiatric disorders? Psychol. Med. 2011, 41, 1143–1150. [Google Scholar] [CrossRef] [Green Version]
- Anker, J.J.; Forbes, M.K.; Almquist, Z.W.; Menk, J.S.; Thuras, P.; Unruh, A.S.; Kushner, M.G. A network approach to modeling comorbid internalizing and alcohol use disorders. J. Abnorm. Psychol. 2017, 126, 325–339. [Google Scholar] [CrossRef]
- Maples, J.L.; Carter, N.T.; Few, L.R.; Crego, C.; Gore, W.L.; Samuel, D.B.; Williamson, R.L.; Lynam, D.R.; Widiger, T.A.; Markon, K.E.; et al. Testing whether the DSM-5 personality disorder trait model can be measured with a reduced set of items: An item response theory investigation of the Personality Inventory for DSM-5. Psychol. Assess. 2015, 27, 1195–1210. [Google Scholar] [CrossRef]
- Díaz-Batanero, C.; Ramírez-López, J.; Domínguez-Salas, S.; Fernández-Calderón, F.; Lozano, O.M. Personality inventory for DSM-5 Short Form (PID-5-SF): Reliability, factorial structure and relationship with functional impairment in dual diagnosis patients. Assessment 2019, 26, 853–866. [Google Scholar] [CrossRef]
- American Educational Research Association; American Psychological Association; National Council on Measurement in Education. Standards for Educational and Psychological Testing; American Educational Research Association: Washington DC, USA, 2014. [Google Scholar]
- Dacosta-Sánchez, D.; Fernández-Calderón, F.; González-Ponce, B.; Díaz-Batanero, C.; Lozano, O.M. Severity of substance use disorder: Utility as an outcome in clinical settings. Alcohol. Clin. Exp. Res. 2019, 43, 869–876. [Google Scholar] [CrossRef] [PubMed]
- González-Sainz, F.; Lozano, O.M.; Vélez-Moreno, A.; Ramírez, J.L. Manual de la Escala de Gravedad de la Dependencia de Sustancias; Servicio de Publicaciones de la Universidad de Huelva: Huelva, Spain, 2014. [Google Scholar]
- Miele, G.M.; Carpenter, K.M.; Cockerham, M.S.; Trautman, K.D.; Blaine, J.; Hasin, D.S. Substance Dependence Severity Scale (SDSS): Reliability and validity of a clinician-administered interview for DSM-IV substance use disorders. Drug Alcohol Depend. 2000, 59, 63–75. [Google Scholar] [CrossRef]
- Friedman, J.; Hastie, T.; Tibshirani, R. Sparse inverse covariance estimation with the graphical lasso. Biostatistics 2008, 9, 432–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.; Chen, Z. Extended bayesian information criteria for model selection with large model spaces. Biometrika 2008, 95, 759–771. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Lafferty, J.; Wasserman, L. The nonparanormal: Semiparametric estimation of high dimensional undirected graphs. J. Mach. Learn. Res. 2009, 10, 2295–2328. [Google Scholar]
- Fruchterman, T.M.J.; Reingold, E.M. Graph drawing by force-directed placement. Softw. Pract. Exp. 1991, 21, 1129–1164. [Google Scholar] [CrossRef]
- Epskamp, S.; Borsboom, D.; Fried, E.I. Estimating psychological networks and their accuracy: A tutorial paper. Behav. Res. Methods 2018, 50, 195–212. [Google Scholar] [CrossRef] [Green Version]
- Pons, P.; Latapy, M. Computing Communities in Large Networks Using Random Walks. In Computer and Information Sciences—ISCIS; Yolum, P., Güngör, T., Gürgen, F., Özturan, C., Eds.; Springer: Berlin/Heidelberg, Germany, 2005; pp. 284–293. [Google Scholar]
- Robinaugh, D.J.; Millner, A.J.; McNally, R.J. Identifying highly influential nodes in the complicated grief network. J. Abnorm. Psychol. 2016, 125, 747–757. [Google Scholar] [CrossRef] [Green Version]
- Haslbeck, J.M.B.; Waldorp, L.J. How well do network models predict observations? On the importance of predictability in network models. Behav. Res. Methods 2018, 50, 853–861. [Google Scholar] [CrossRef] [Green Version]
- Letina, S.; Blanken, T.; Deserno, M.; Borsboom, D. Expanding network analysis tools in psychological networks: Minimal spanning trees, participation coefficients, and motif analysis applied to a network of 26 psychological attributes. Complexity 2019, 2019, 9424605. [Google Scholar] [CrossRef]
- Jones, P. Networktools: Tools for Identifying Important Nodes in Networks. R Package Version 1.4.0. Available online: https://cran.r-project.org/package=networktools (accessed on 3 June 2022).
- Jones, P.; Ma, R.; McNally, R.J. Bridge Centrality: A network approach to understanding comorbidity. Multivar. Behav. Res. 2019, 56, 353–367. [Google Scholar] [CrossRef] [PubMed]
- van Borkulo, C.D.; Boschloo, L.; Kossakowski, J.J.; Tio, P.; Schoevers, R.A.; Borsboom, D.; Waldorp, L.J. Comparing network structures on three aspects: A permutation test. Psychol. Methods 2022. [Google Scholar] [CrossRef] [PubMed]
- Korkmaz, S.; Göksüük, D.; Zararsiz, G. MVN: An R package for assessing multivariate normality. R J. 2014, 6, 151–162. [Google Scholar] [CrossRef] [Green Version]
- Csardi, G.; Nepusz, T. The Igraph Software Package for Complex Network Research. InterJournal Complex Systems 1695. 2006. Available online: http://igraph.org (accessed on 3 June 2022).
- Epskamp, S.; Cramer, A.; Waldorp, L.; Schimittmann, V.; Borsboom, D. qgraph: Network visualizations of relationships in psychometric data. J. Stat. Softw. 2012, 48, 1–18. [Google Scholar] [CrossRef] [Green Version]
- De Clercq, B.; Fruyt, F.; De Bolle, M.; Van Hiel, A.; Markon, K.E.; Krueger, R.F. The hierarchical structure and construct validity of the PID-5 trait measure in adolescence. J. Personal. 2014, 82, 158–169. [Google Scholar] [CrossRef]
- Díaz-Batanero, C.; Aluja, A.; Sayans-Jiménez, -P.; Baillés, E.; Fernández-Calderón, F.; Peri, J.M.; Vall Lozano, O.M.; Gutiérrez, F. Alterntive DSM-5 Model for personality disorders through the lens of an empirical network model. Assessment 2021, 28, 773–787. [Google Scholar] [CrossRef]
- Wright, A.G.; Thomas, K.M.; Hopwood, C.J.; Markon, K.E.; Pincus, A.L.; Krueger, R.F. The hierarchical structure of DSM-5 pathological personality traits. J. Abnorm. Psychol. 2012, 121, 951–957. [Google Scholar] [CrossRef] [Green Version]
- Kotov, R.; Krueger, R.; Watson, D.; Achenbach, T.M.; Althoff, R.; Bagby, R.; Zimmerman, M. The Hierarchical Taxonomy of Psychopathology (HiTOP): A dimensional alternative to traditional nosologies. J. Abnorm. Psychol. 2017, 126, 454–477. [Google Scholar] [CrossRef] [Green Version]
- Baggio, S.; Sapin, M.; Khazaal, Y.; Studer, J.; Wolff, H.; Gmel, G. Comorbidity of symptoms of alcohol and cannabis use disorders among a population-based sample of simultaneous users. Insight from a network perspective. Int. J. Environ. Res. Public Health 2018, 15, 2893. [Google Scholar] [CrossRef] [Green Version]
- Rhemtulla, M.; Fried, E.I.; Aggen, S.H.; Tuerlinckx, F.; Kendler, K.S.; Borsboom, D. Network analysis of substance abuse and dependence symptoms. Drug Alcohol Depend. 2016, 161, 230–237. [Google Scholar] [CrossRef] [Green Version]
- Sanchez-Garcia, M.; de la Rosa-Cáceres, A.; Díaz-Batanero, C.; Fernández-Calderón, F.; Lozano, O.M. Cocaine use disorder criteria in a clinical sample: An analysis using item response theory, factor and network analysis. Am. J. Drug Alcohol Abus 2021. [Google Scholar] [CrossRef] [PubMed]
- Widiger, T.A.; McCabe, G.A. The Alternative Model of Personality Disorders (AMPD) from the perspective of the Five-Factor Model. Psychopathology 2020, 53, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Freeman, C.; Wiers, C.; Sloan, M.; Zehra, A.; Ramirez, V.; Wang, G.; Volkow, N. Emotion recognition biases in alcohol use disorder. Alcohol. Clin. Exp. Res. 2018, 42, 1541–1547. [Google Scholar] [CrossRef] [PubMed]
- Pabst, A.; Peyroux, E.; Rolland, B.; Timary, P.; Maurage, P. Hostile attributional bias in severe alcohol use disorder. J. Psychiatr. Res. 2020, 129, 176–180. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- Choate, A.; Gorey, C.; Rappaport, L.; Wiernik, B.; Bornovalova, M. Alternative model of personality disorders traits predict residential addictions treatment completion. Drug Alcohol Depend. 2021, 228, 109011. [Google Scholar] [CrossRef]
- Gómez-Bujedo, J.; Lozano, O.M.; Pérez-Moreno, P.J.; Lorca-Marín, J.A.; Fernández-Calderón, F.; Díaz-Batanero, C.; Moraleda-Barreno, E. Personality traits and impulsivity task among substance use disorder patients: Their relations and links with retention in treatment. Front. Psychiatry 2020, 11, 566240. [Google Scholar] [CrossRef]
- Mezquita, L.; Bravo, A.J.; Ortet, G.; Pilatti, A.; Rearson, M.R.; Ibañez, M.I. Cross-cultural examination of different personality pathways to alcohol use and misuse in emerging adulthood. Drug Alcohol Depend. 2018, 19, 193–200. [Google Scholar] [CrossRef]
- Rhem, J.; Room, R. The cultural aspect: How to measure and interpret epidemiological data on alcohol-use disorders across cultures. Nord. Stud. Alcohol Drugs 2017, 34, 330–341. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Sociodemographic Characteristics | n | % |
|---|---|---|
| Gender | ||
| Male | 495 | 50.3 |
| Female | 490 | 49.7 |
| Education level | ||
| Did not complete primary education | 17 | 1.7 |
| Primary education | 52 | 5.3 |
| Secondary education | 533 | 54.1 |
| University studies | 383 | 38.9 |
| Employment status | ||
| Employed | 569 | 57.8 |
| Unemployed | 416 | 42.2 |
| n | % Sample Patients (n = 243) | % All Sample (n = 985) | |
|---|---|---|---|
| Neurodevelopmental Disorders | 5 | 2.06 | 0.51 |
| Schizophrenia Spectrum and Other Psychotic Disorders | 21 | 8.64 | 2.13 |
| Bipolar and Related Disorders | 11 | 4.53 | 1.12 |
| Depressive Disorders | 94 | 38.68 | 9.54 |
| Anxiety Disorders | 88 | 36.21 | 8.93 |
| Obsessive-Compulsive and Related Disorders | 6 | 2.47 | 0.61 |
| Trauma- and Stressor-Related Disorders | 76 | 31.28 | 7.72 |
| Dissociative Disorders | 2 | 0.82 | 0.20 |
| Somatic Symptom and Related Disorders | 2 | 0.82 | 0.20 |
| Feeding and Eating Disorders | 4 | 1.65 | 0.41 |
| Substance-Related and Addictive Disorders | 10 | 4.12 | 1.02 |
| Personality Disorders | 25 | 10.29 | 2.54 |
| Nodes | Strength | Expected Influence 1 | Expected Influence 2 | Bridge Strength | Bridge Expected Influence 1 | Bridge Expected Influence 2 | R2 | PC | PR |
|---|---|---|---|---|---|---|---|---|---|
| Personality Facets of Alternative Model of Personality Disorder | |||||||||
| Anhedonia | 1.67 | 1.48 | 1.50 | −1.00 | −1.14 | −1.02 | 0.62 | 0.00 | 0.61 |
| Anxiousness | 1.94 | 1.43 | 1.20 | −0.82 | −1.33 | −1.00 | 0.57 | 0.01 | 0.71 |
| Attention Seeking | −0.21 | −0.57 | −0.64 | 0.32 | −0.39 | −0.14 | 0.34 | 0.11 | 0.45 |
| Callousness | 0.40 | −0.24 | −0.32 | 2.21 | 1.34 | 1.25 | 0.33 | 0.29 | 0.86 |
| Deceitfulness | 0.83 | 1.03 | 0.97 | −0.33 | −0.09 | 0.49 | 0.50 | 0.02 | 0.58 |
| Depressivity | 0.91 | 0.82 | 1.10 | −0.89 | −1.04 | −1.00 | 0.60 | 0.00 | 0.59 |
| Distractibility | 0.35 | 0.61 | 0.75 | −0.18 | 0.04 | −0.12 | 0.51 | 0.15 | 0.64 |
| Eccentricity | 1.04 | 1.20 | 1.24 | −0.46 | −0.22 | −0.08 | 0.54 | 0.05 | 0.67 |
| Emotional Lability | 1.08 | −1.46 | −1.19 | 0.20 | −1.06 | −1.25 | 0.41 | 0.09 | 0.86 |
| Grandiosity | 0.12 | −0.10 | −0.26 | 1.36 | 0.95 | 0.83 | 0.34 | 0.25 | 0.49 |
| Hostility | −0.93 | −0.46 | −0.26 | 0.77 | 1.05 | 0.63 | 0.40 | 0.53 | 0.51 |
| Impulsivity | 0.16 | 0.47 | 0.41 | 2.49 | 2.85 | 2.84 | 0.44 | 0.50 | 0.37 |
| Intimacy Avoidance | −1.75 | −2.09 | −2.01 | −0.60 | −0.37 | −0.53 | 0.24 | 0.04 | 0.28 |
| Irresponsibility | 0.63 | 0.69 | 0.73 | 2.77 | 2.91 | 3.01 | 0.42 | 0.37 | 1 |
| Manipulativeness | 0.39 | 0.25 | 0.22 | 0.02 | −0.27 | −0.11 | 0.45 | 0.04 | 0.40 |
| Perceptual Dysreg. | 0.61 | 0.84 | 0.95 | 0.60 | 0.88 | 0.83 | 0.50 | 0.09 | 0.90 |
| Perseveration | 1.51 | 1.51 | 1.57 | 0.34 | 0.49 | 0.47 | 0.56 | 0.15 | 0.97 |
| Restricted Affectivity | −0.49 | −1.75 | −1.72 | 0.29 | 0.43 | 0.15 | 0.27 | 0.18 | 0.35 |
| Rigid Perfectionism | −0.75 | −0.68 | −0.70 | 0.96 | 0.75 | 0.60 | 0.33 | 0.38 | 0.48 |
| Risk Taking | −0.17 | −0.02 | 0.02 | 1.43 | 1.47 | 1.82 | 0.35 | 0.23 | 0.67 |
| Separation Insecurity | −1.58 | −2.15 | −2.15 | −0.53 | −0.57 | −0.72 | 0.22 | 0.05 | 0.20 |
| Submissiveness | −1.84 | −1.28 | −1.28 | −0.42 | −0.28 | −0.32 | 0.29 | 0.11 | 0.17 |
| Suspiciousness | 0.34 | 0.61 | 0.77 | −0.40 | −0.17 | −0.15 | 0.50 | 0.04 | 0.85 |
| Unusual Bel. and Exp. | −0.02 | 0.31 | 0.38 | −0.05 | 0.21 | 0.30 | 0.48 | 0.05 | 0.48 |
| Withdrawal | 0.27 | 0.20 | 0.06 | −0.56 | −0.82 | −0.74 | 0.46 | 0.03 | 0.39 |
| Alcohol-Use Disorders | |||||||||
| Larger/Longer | −1.54 | −0.97 | −1.23 | −0.78 | −0.55 | −0.69 | 0.27 | 0.02 | 0.15 |
| Quit/Control | −2.24 | −1.59 | −1.75 | −1.14 | −0.97 | −1.07 | 0.24 | 0.00 | 0 |
| Time spent | −0.36 | 0.03 | 0.01 | −1.08 | −0.88 | −0.88 | 0.41 | 0.00 | 0.31 |
| Activities given up | 0.05 | 0.37 | 0.23 | −0.74 | −0.52 | −0.53 | 0.43 | 0.02 | 0.36 |
| Tolerance | 0.12 | 0.36 | 0.22 | −0.56 | −0.44 | −0.43 | 0.41 | 0.00 | 0.61 |
| Withdrawal | −0.61 | −0.35 | −0.26 | −0.15 | −0.12 | −0.21 | 0.37 | 0.03 | 0.56 |
| Phys./Psych.Problems | 1.07 | 1.23 | 0.99 | −0.79 | −0.57 | −0.54 | 0.48 | 0.00 | 0.55 |
| Neglect roles | 0.06 | 0.19 | 0.28 | −0.81 | −0.85 | −0.81 | 0.47 | 0.02 | 0.60 |
| Hazardous use | −0.18 | 0.18 | 0.21 | −0.56 | −0.32 | −0.35 | 0.43 | 0.02 | 0.27 |
| Social/Interp.Prob. | 0.18 | 0.48 | 0.50 | −0.66 | −0.43 | −0.49 | 0.48 | 0.01 | 0.38 |
| Craving | −1.07 | −0.57 | −0.54 | −0.22 | 0.03 | −0.04 | 0.32 | 0.04 | 0.44 |
| All Sample | Men | Women | Cohen’s d | |
|---|---|---|---|---|
| PID-5 Subscales | ||||
| Anhedonia | 6.78 (3.24) | 6.18 (2.71) | 7.38 (3.60) | 0.38 |
| Anxiousness | 8.60 (3.38) | 7.81 (3.17) | 9.41 (3.39) | 0.49 |
| Attention Seeking | 5.88 (2.50) | 6.04 (2.55) | 5.72 (2.44) | 0.13 |
| Callousness | 4.75 (1.50) | 4.90 (1.69) | 4.59 (1.26) | 0.34 |
| Deceitfulness | 5.24 (2.00) | 5.40 (2.16) | 5.08 (1.81) | 0.16 |
| Depressivity | 5.88 (2.91) | 5.39 (2.36) | 6.38 (3.31) | 0.34 |
| Distractibility | 7.97 (3.42) | 7.40 (3.27) | 8.54 (3.48) | 0.34 |
| Eccentricity | 7.11 (3.39) | 6.89 (3.28) | 7.34 (3.48) | 0.13 |
| Emotional Lability | 9.21 (3.14) | 8.28 (2.85) | 10.13 (3.15) | 0.62 |
| Grandiosity | 5.50 (2.12) | 5.74 (2.32) | 5.25 (1.88) | 0.23 |
| Hostility | 6.95 (2.85) | 6.35 (2.69) | 7.54 (2.88) | 0.43 |
| Impulsivity | 6.47 (2.91) | 6.10 (2.79) | 6.85 (3.02) | 0.26 |
| Intimacy Avoidance | 6.26 (3.26) | 5.99 (2.76) | 6.54 (3.66) | 0.17 |
| Irresponsibility | 5.51 (1.91) | 5.52 (2.01) | 5.50 (1.80) | 0.01 |
| Manipulativeness | 5.62 (2.13) | 5.72 (2.18) | 5.51 (2.08) | 0.10 |
| Perceptual Dysregulation | 5.32 (2.20) | 5.21 (2.13) | 5.44 (2.25) | 0.10 |
| Perseveration | 7.31 (2.96) | 6.88 (2.79) | 7.75 (3.07) | 0.30 |
| Restricted Affectivity | 7.35 (2.66) | 7.67 (2.68) | 7.03 (2.59) | 0.24 |
| Rigid Perfectionism | 8.06 (3.12) | 7.84 (3.05) | 8.27 (3.19) | 0.14 |
| Risk Taking | 5.40 (2.23) | 5.51 (2.30) | 5.29 (2.14) | 0.10 |
| Separation Insecurity | 7.90 (3.26) | 7.78 (3.26) | 8.03 (3.26) | 0.08 |
| Submissiveness | 6.94 (2.82) | 6.63 (2.56) | 7.25 (3.02) | 0.22 |
| Suspiciousness | 6.69 (2.57) | 6.50 (2.51) | 6.88 (2.63) | 0.15 |
| Unusual Beliefs and Exp. | 5.92 (2.67) | 5.63 (2.45) | 6.21 (2.84) | 0.22 |
| Withdrawal | 6.98 (2.93) | 6.86 (2.86) | 7.09 (3.00) | 0.08 |
| Alcohol-Use Disorder criteria | ||||
| Larger/Longer | 0.17 (0.17) | 0.20 (0.40) | 0.14 (0.35) | 0.16 |
| Quit/Control | 0.19 (0.23) | 0.25 (0.43) | 0.13 (0.33) | 0.31 |
| Time spent | 0.05 (0.20) | 0.06 (0.24) | 0.04 (0.20) | 0.09 |
| Activities given up | 0.04 (0.38) | 0.05 (0.22) | 0.03 (0.17) | 0.10 |
| Tolerance | 0.05 (0.39) | 0.07 (0.25) | 0.03 (0.18) | 0.18 |
| Withdrawal | 0.05 (0.22) | 0.06 (0.24) | 0.04 (0.20) | 0.09 |
| Phys/Psych.Problems | 0.08 (0.20) | 0.09 (0.28) | 0.06 (0.24) | 0.12 |
| Neglect roles | 0.03 (0.22) | 0.04 (0.21) | 0.02 (0.13) | 0.11 |
| Hazardous use | 0.06 (0.22) | 0.08 (0.27) | 0.03 (0.18) | 0.21 |
| Social/Interp.Problems | 0.04 (0.26) | 0.05 (0.22) | 0.03 (0.18) | 0.10 |
| Craving | 0.06 (0.24) | 0.07 (0.26) | 0.05 (0.22) | 0.08 |
| Scales | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Callousness | 1 | 0.45 | 0.31 | 0.29 | 0.49 | 0.25 | 0.36 | 0.14 | 0.13 | 0.25 | 0.27 | 0.31 | 0.32 | 0.26 | 0.31 | 0.29 | 0.33 | 0.31 |
| 2. Grandiosity | 0.12 | 1 | 0.29 | 0.29 | 0.36 | 0.39 | 0.43 | 0.13 | 0.12 | 0.20 | 0.21 | 0.29 | 0.23 | 0.19 | 0.20 | 0.26 | 0.26 | 0.29 |
| 3. Hostility | 0.01 | - | 1 | 0.57 | 0.42 | 0.41 | 0.38 | 0.13 | 0.08 | 0.18 | 0.20 | 0.18 | 0.23 | 0.21 | 0.19 | 0.19 | 0.21 | 0.19 |
| 4. Impulsivity | - | - | 0.20 | 1 | 0.53 | 0.31 | 0.53 | 0.13 | 0.08 | 0.21 | 0.25 | 0.19 | 0.23 | 0.23 | 0.20 | 0.20 | 0.21 | 0.17 |
| 5. Irresponsibility | 0.12 | - | 0.00 | 0.16 | 1 | 0.23 | 0.43 | 0.23 | 0.13 | 0.28 | 0.35 | 0.29 | 0.31 | 0.33 | 0.34 | 0.35 | 0.32 | 0.34 |
| 6. Rigid Perfectionism | - | 0.12 | 0.04 | 0.13 | −0.02 | 1 | 0.33 | 0.04 | 0.06 | 0.08 | 0.08 | 0.07 | 0.07 | 0.10 | 0.05 | 0.13 | 0.13 | 0.13 |
| 7. Risk taking | 0.03 | 0.12 | - | 0.18 | - | - | 1 | 0.25 | 0.18 | 0.27 | 0.28 | 0.30 | 0.31 | 0.35 | 0.29 | 0.35 | 0.30 | 0.30 |
| 8. Larger/longer | - | - | - | - | - | - | 0.05 | 1 | 0.48 | 0.35 | 0.28 | 0.39 | 0.30 | 0.42 | 0.34 | 0.36 | 0.34 | 0.34 |
| 9. Quit/control | - | - | - | - | - | - | - | 0.27 | 1 | 0.39 | 0.33 | 0.32 | 0.29 | 0.40 | 0.32 | 0.29 | 0.29 | 0.25 |
| 10. Time Spent | - | - | - | - | - | - | 0.01 | 0.19 | 0.23 | 1 | 0.58 | 0.52 | 0.48 | 0.55 | 0.48 | 0.46 | 0.50 | 0.40 |
| 11. Activities given up | - | - | - | - | 0.04 | - | - | - | - | 0.20 | 1 | 0.49 | 0.50 | 0.50 | 0.53 | 0.52 | 0.51 | 0.48 |
| 12. Tolerance | - | - | - | - | - | - | 0.02 | 0.04 | - | 0.22 | 0.09 | 1 | 0.51 | 0.52 | 0.51 | 0.44 | 0.53 | 0.48 |
| 13. Withdrawal | 0.03 | - | 0.01 | - | 0.02 | - | 0.04 | 0.08 | - | 0 | 0.10 | 0.19 | 1 | 0.55 | 0.49 | 0.45 | 0.46 | 0.41 |
| 14. Phys./Psych.Problems | - | - | - | - | - | - | 0.01 | 0.08 | 0.05 | 0.12 | 0.05 | 0.05 | 0.20 | 1 | 0.57 | 0.57 | 0.54 | 0.48 |
| 15. Neglect roles | 0.05 | - | - | - | 0.01 | 0.02 | - | - | - | 0.02 | 0.22 | 0.11 | 0.11 | 0.09 | 1 | 0.54 | 0.66 | 0.42 |
| 16. Hazardous use | 0.01 | - | - | - | - | - | 0.04 | 0.10 | - | 0.04 | 0.05 | 0.02 | - | 0.17 | 0.13 | 1 | 0.59 | 0.48 |
| 17. Social/Interp.Problems | - | 0.02 | - | - | - | - | 0.01 | - | - | 0.05 | 0.06 | 0.10 | 0.09 | 0.11 | 0.25 | 0.21 | 1 | 0.42 |
| 18. Craving | 0.03 | 0.02 | - | - | 0.05 | - | - | 0.10 | 0.05 | - | - | 0.27 | 0.08 | 0.11 | 0.01 | 0.06 | 0.04 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De la Rosa-Cáceres, A.; Narvaez-Camargo, M.; Blanc-Molina, A.; Romero-Pérez, N.; Dacosta-Sánchez, D.; González-Ponce, B.M.; Parrado-González, A.; Torres-Rosado, L.; Mancheño-Velasco, C.; Lozano-Rojas, Ó.M. Bridge Nodes between Personality Traits and Alcohol-Use Disorder Criteria: The Relevance of Externalizing Traits of Risk Taking, Callousness, and Irresponsibility. J. Clin. Med. 2022, 11, 3468. https://doi.org/10.3390/jcm11123468
De la Rosa-Cáceres A, Narvaez-Camargo M, Blanc-Molina A, Romero-Pérez N, Dacosta-Sánchez D, González-Ponce BM, Parrado-González A, Torres-Rosado L, Mancheño-Velasco C, Lozano-Rojas ÓM. Bridge Nodes between Personality Traits and Alcohol-Use Disorder Criteria: The Relevance of Externalizing Traits of Risk Taking, Callousness, and Irresponsibility. Journal of Clinical Medicine. 2022; 11(12):3468. https://doi.org/10.3390/jcm11123468
Chicago/Turabian StyleDe la Rosa-Cáceres, Ana, Marta Narvaez-Camargo, Andrea Blanc-Molina, Nehemías Romero-Pérez, Daniel Dacosta-Sánchez, Bella María González-Ponce, Alberto Parrado-González, Lidia Torres-Rosado, Cinta Mancheño-Velasco, and Óscar Martín Lozano-Rojas. 2022. "Bridge Nodes between Personality Traits and Alcohol-Use Disorder Criteria: The Relevance of Externalizing Traits of Risk Taking, Callousness, and Irresponsibility" Journal of Clinical Medicine 11, no. 12: 3468. https://doi.org/10.3390/jcm11123468
APA StyleDe la Rosa-Cáceres, A., Narvaez-Camargo, M., Blanc-Molina, A., Romero-Pérez, N., Dacosta-Sánchez, D., González-Ponce, B. M., Parrado-González, A., Torres-Rosado, L., Mancheño-Velasco, C., & Lozano-Rojas, Ó. M. (2022). Bridge Nodes between Personality Traits and Alcohol-Use Disorder Criteria: The Relevance of Externalizing Traits of Risk Taking, Callousness, and Irresponsibility. Journal of Clinical Medicine, 11(12), 3468. https://doi.org/10.3390/jcm11123468