
The Role of ABO Blood Type in Patients with SARS-CoV-2 Infection: A Systematic Review

 ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Strategy and Selection Criteria
2.2. Selection of Studies and Data Extraction
2.3. Assessment of Risk of Bias in Included Studies
2.4. Data Synthesis
3. Results
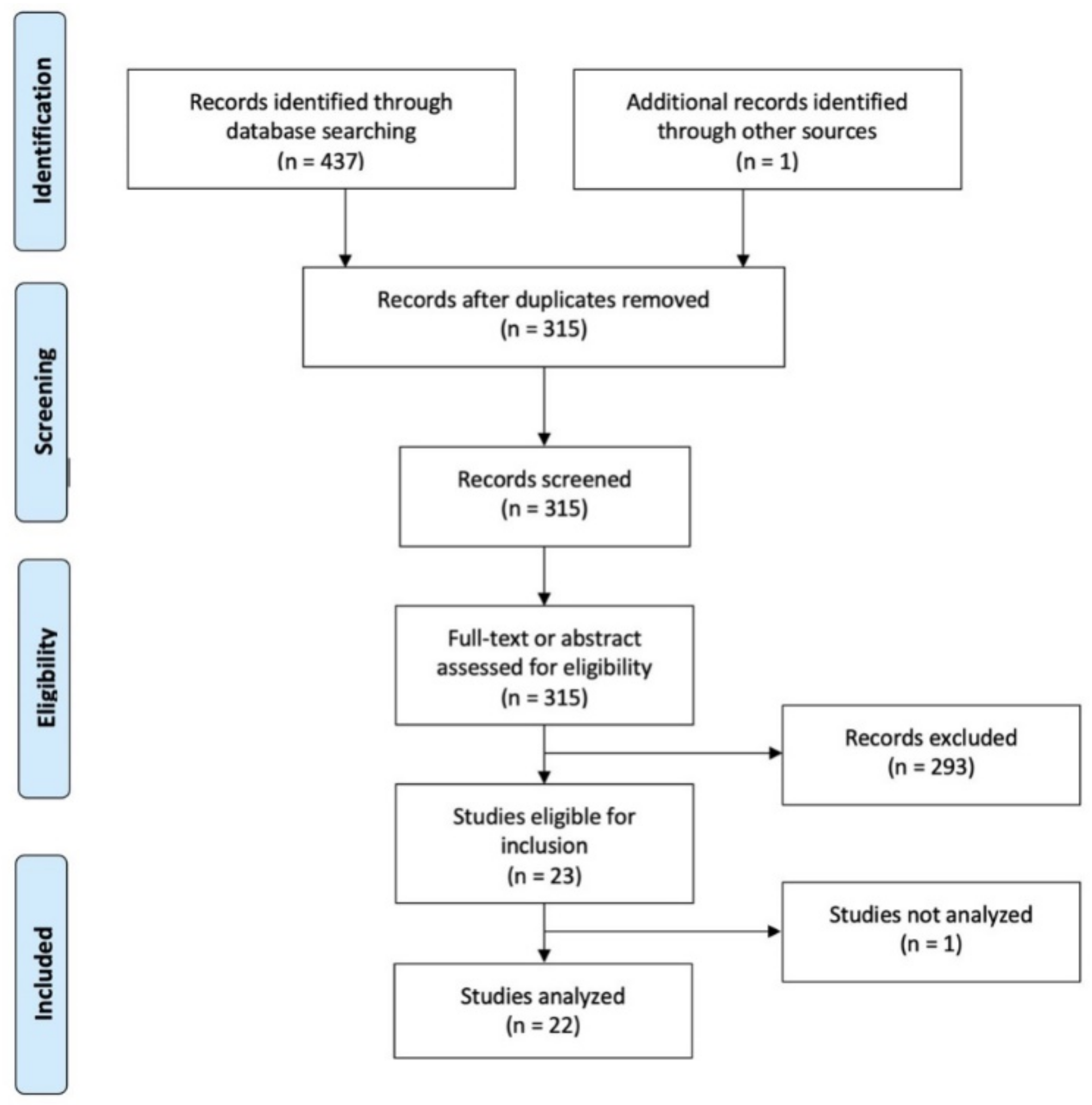
3.1. Search Outcomes
3.2. Characteristics of the Included Studies
3.3. Assessment of Risk of Bias
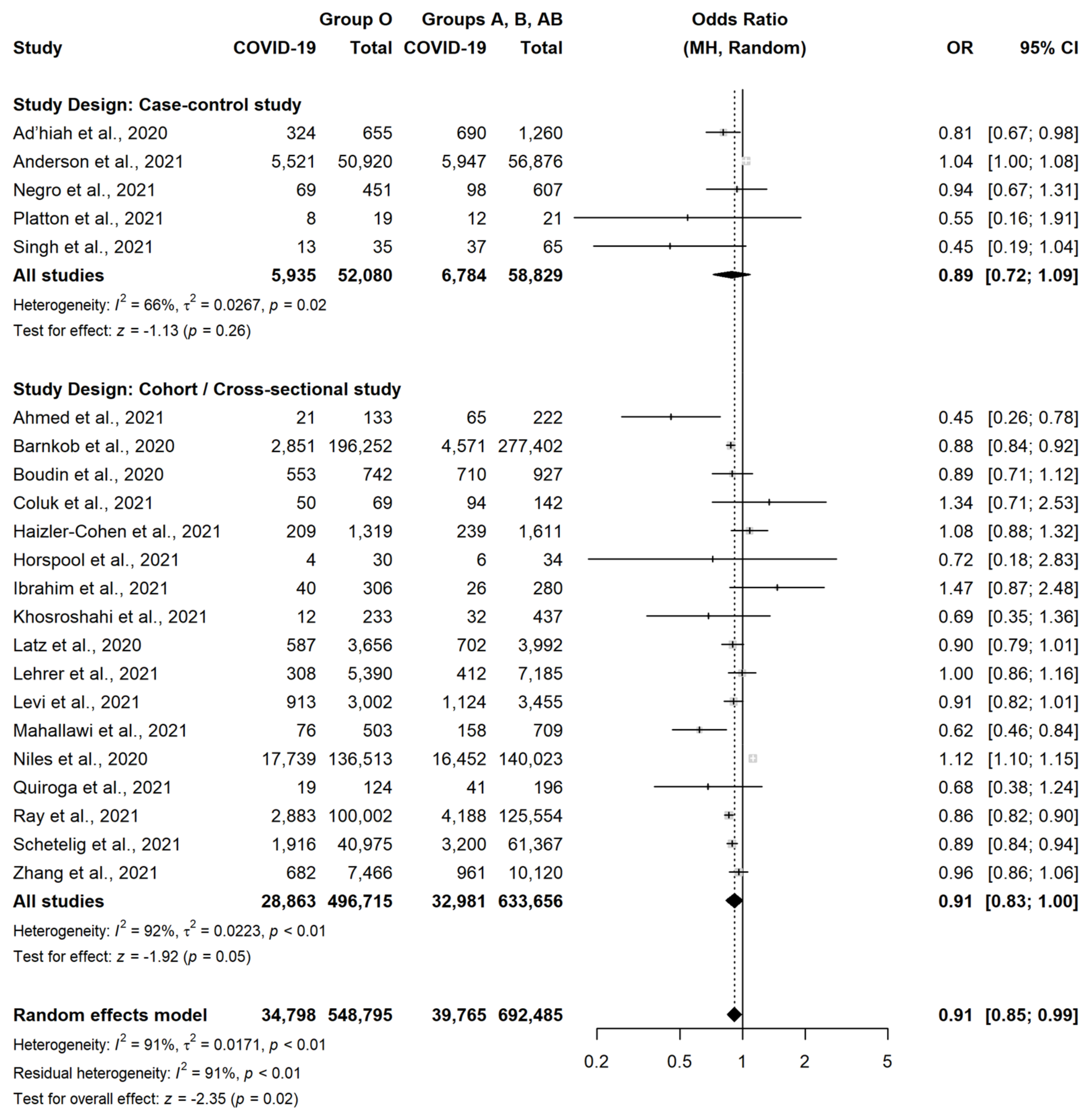
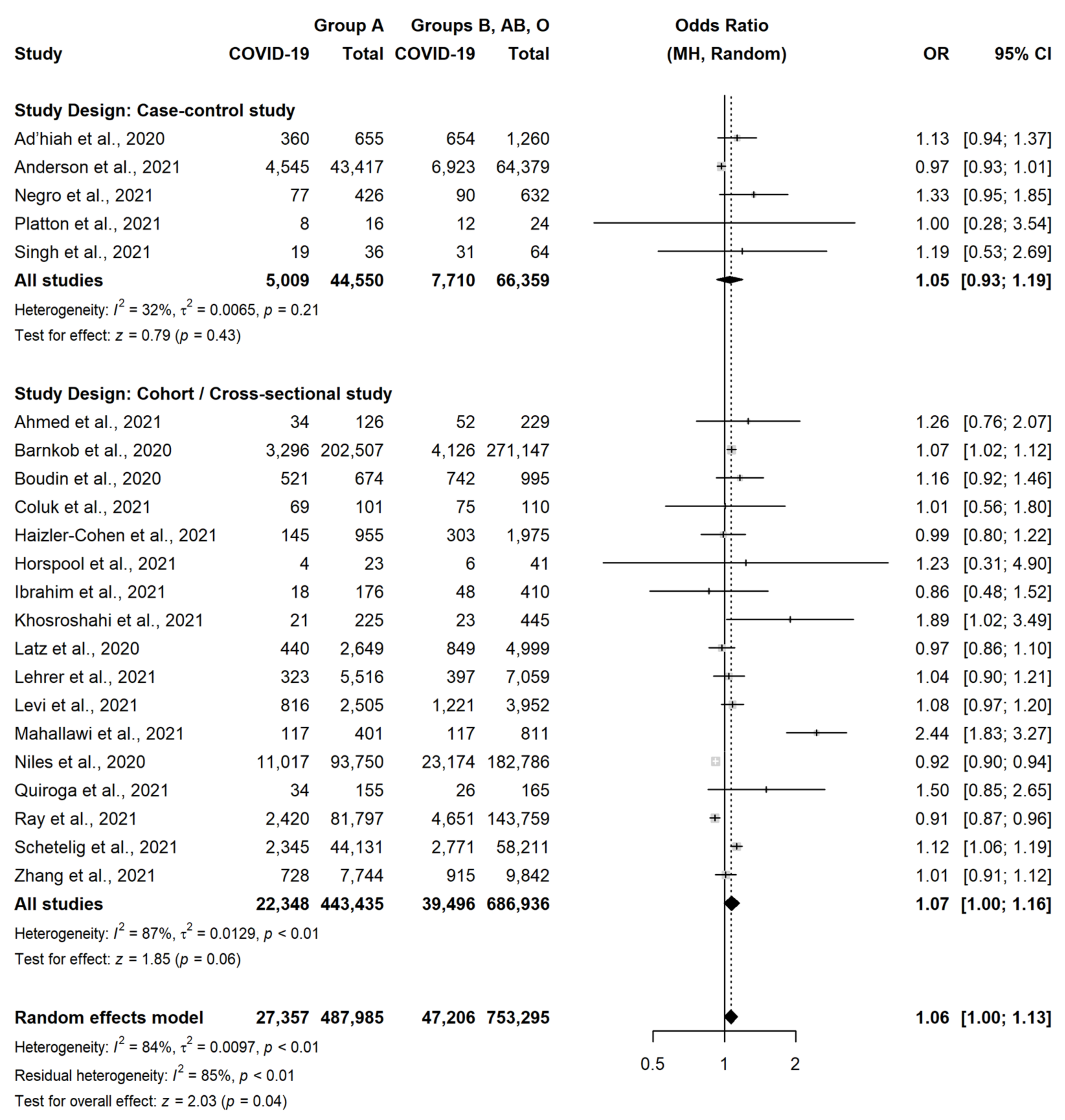
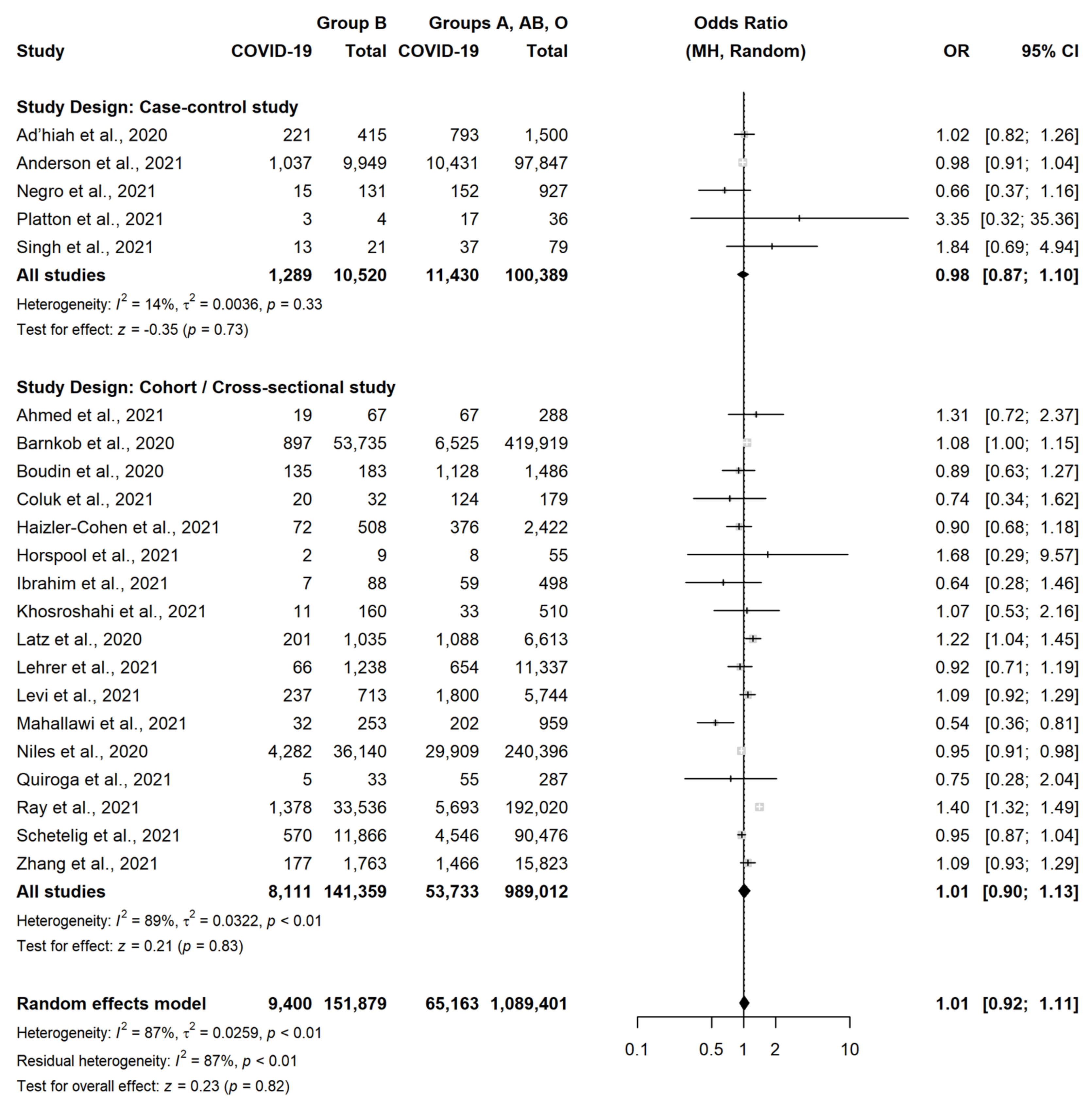
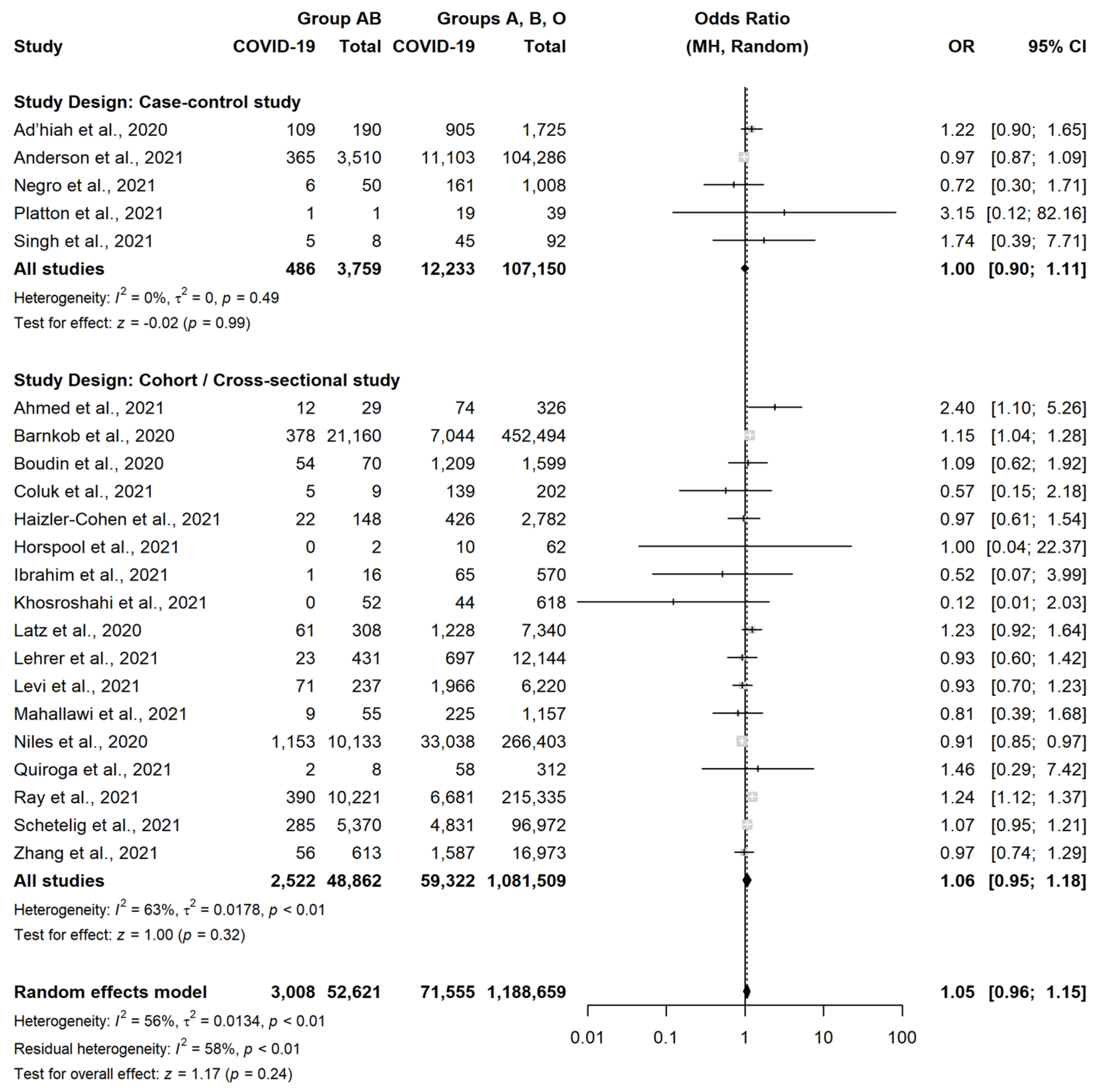
3.4. Association between Blood Groups and SARS-CoV-2 Infection
4. Discussion
4.1. Summary of Main Results
4.2. Overall Completeness and Applicability of Evidence
4.3. Potential Biases in the Review Process
4.4. Context for This Review
4.5. Agreements and Disagreements with Other Systematic Reviews
4.6. Implications for Practice
4.7. Implications for Research
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). Weekly Epidemiological Update on COVID-19. Available online: https://www.who.int/publications/m/item/weekly-operational-update-on-covid-19---22-february-2021 (accessed on 22 February 2022).
- Zhou, P.; Yang, X.L.; Wang, X.G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.R.; Zhu, Y.; Li, B.; Huang, C.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [Green Version]
- Li, M.Y.; Li, L.; Zhang, Y.; Wang, X.S. Expression of the SARS-CoV-2 cell receptor gene ACE2 in a wide variety of human tissues. Infect. Dis. Poverty 2020, 9, 45. [Google Scholar] [CrossRef] [PubMed]
- Zizza, A.; Recchia, V.; Aloisi, A.; Guido, M. Clinical features of COVID-19 and SARS epidemics. A literature review. J. Prev. Med. Hyg. 2021, 62, E13–E24. [Google Scholar] [PubMed]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Wang, Y.; Chen, Y.; Qin, Q. Unique epidemiological and clinical features of the emerging 2019 novel coronavirus pneumonia (COVID-19) implicate special control measures. J. Med. Virol. 2020, 92, 568–576. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Diagnostic Tests for SARS-CoV-2. Interim Guidance. 2020. Available online: https://www.who.int/publications/i/item/diagnostic-testing-for-sars-cov-2 (accessed on 2 December 2021).
- Winter, A.K.; Hegde, S.T. The important role of serology for COVID-19 control. Lancet Infect. Dis. 2020, 20, 758–759. [Google Scholar] [CrossRef]
- Mercer, T.R.; Salit, M. Testing at scale during the COVID-19 pandemic. Nat. Rev. Genet. 2021, 22, 415–426. [Google Scholar] [CrossRef]
- Sciomer, S.; Moscucci, F.; Magrì, D.; Badagliacca, R.; Piccirillo, G.; Agostoni, P. SARS-CoV-2 spread in Northern Italy: What about the pollution role? Environ. Monit. Assess. 2020, 192, 325. [Google Scholar] [CrossRef]
- Cai, H. Sex difference and smoking predisposition in patients with COVID-19. Lancet Respir. Med. 2020, 8, e20. [Google Scholar] [CrossRef]
- Chung, R.Y.; Dong, D.; Li, M.M. Socioeconomic gradient in health and the covid-19 outbreak. BMJ 2020, 369, m1329. [Google Scholar] [CrossRef] [Green Version]
- Zhao, J.; Yang, Y.; Huang, H.; Li, D.; Gu, D.; Lu, X.; Zhang, Z.; Liu, L.; Liu, T.; Liu, Y.; et al. Relationship Between the ABO Blood Group and the Coronavirus Disease 2019 (COVID-19) Susceptibility. Clin. Infect. Dis. 2021, 73, 328–331. [Google Scholar] [CrossRef] [PubMed]
- Göker, H.; Aladağ Karakulak, E.; Demiroğlu, H.; Ayaz Ceylan, Ç.M.; Büyükaşik, Y.; Inkaya, A.Ç.; Aksu, S.; Sayinalp, N.; Haznedaroğlu, I.C.; Uzun, Ö.; et al. The effects of blood group types on the risk of COVID-19 infection and its clinical outcome. Turkish J. Med. Sci. 2020, 50, 679–683. [Google Scholar] [CrossRef] [PubMed]
- Abdollahi, A.; Mahmoudi-Aliabadi, M.; Mehrtash, V.; Jafarzadeh, B.; Salehi, M. The novel coronavirus SARS-CoV-2 vulnerability association with ABO/Rh blood types. Iran J. Pathol. 2020, 15, 156–160. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 8. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0; The Cochrane Collaboration: Chichester, UK, 2011. [Google Scholar]
- Negro, P.; Congedo, M.; Zizza, A.; Guido, M.; Sacquegna, G.; Pulito, G.; Lobreglio, G. Role of ABO blood system in COVID-19: Findings from a southern Italian study. Transfus. Med. 2021; online ahead of print. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Robertson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality if Nonrandomised Studies in Meta-Analyses. Available online: https://ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 2 September 2021).
- Reeves, B.C.; Deeks, J.J.; Higgins, J.P.T.; Shea, B.; Tugwell, P.; Wells, G.A.; on behalf of the Cochrane Non-Randomised Studies Methods Group. Chapter 13: Including non-randomised studies. In Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0; Higgins, J.P.T., Green, S., Eds.; The Cochrane Collaboration: Chichester, UK, 2011. [Google Scholar]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials. 1987, 7, 177–188. [Google Scholar] [CrossRef]
- Ad’hiah, A.H.; Allami, R.H.; Mohsin, R.H.; Abdullah, M.H.; AL-Sa’ady, A.J.R.; Alsudan, M.Y. Evaluating of the association between ABO blood groups and coronavirus disease 2019 (COVID-19) in Iraqi patients. Egypt. J. Med. Hum. Genet. 2020, 21, 50. [Google Scholar] [CrossRef]
- Anderson, J.L.; May, H.T.; Knight, S.; Bair, T.L.; Muhlestein, J.B.; Knowlton, K.U.; Horne, B.D. Association of Sociodemographic Factors and Blood Group Type with Risk of COVID-19 in a US Population. JAMA Netw. Open 2021, 4, e217429. [Google Scholar] [CrossRef]
- Platton, S.; Mendes, N.; Booth, C.; Lancut, J.; Lee, K.; Regan, F.; Green, L. Positive direct antiglobulin tests in patients with COVID-19. Transfusion 2021, 61, 333–334. [Google Scholar] [CrossRef]
- Singh, N.; Buckley, T.; Shertz, W. Placental Pathology in COVID-19: Case Series in a Community Hospital Setting. Cureus 2021, 13, e12522. [Google Scholar]
- Ahmed, I.; Quinn, L.; Tan, B.K. COVID-19 and the ABO blood group in pregnancy: A tale of two multiethnic cities. Int. J. Lab. Hematol. 2021, 43, e45–e47. [Google Scholar] [CrossRef] [PubMed]
- Barnkob, M.B.; Pottegård, A.; Støvring, H.; Haunstrup, T.M.; Homburg, K.; Larsen, R.; Hansen, M.B.; Titlestad, K.; Aagaard, B.; Møller, B.K.; et al. Reduced prevalence of SARS-CoV-2 infection in ABO blood group O. Blood Adv. 2020, 4, 4990–4993. [Google Scholar] [CrossRef] [PubMed]
- Boudin, L.; Janvier, F.; Bylicki, O.; Dutasta, F. ABO blood groups are not associated with risk of acquiring the SARS-CoV-2 infection in young adults. Haematologica 2020, 105, 2841–2843. [Google Scholar] [CrossRef] [PubMed]
- Coluk, Y.; Hizli, O.; Gunaydın, S.; Yildirim, G.; Baysal, E.; OzgenHergul, G. Association of blood subgroups with PCR test positivity and lung involvement in patients with COVID-19. Cureus 2021, 13, e14172. [Google Scholar] [CrossRef] [PubMed]
- Haizler-Cohen, L.; Collins, A.; Moncada, K.; Davidov, A.; Fruhman, G. ABO and Rh blood groups and SARS-CoV-2 susceptibility in pregnancy. Am. J. Obstet. Gynecol. 2021, 224, S383. [Google Scholar] [CrossRef]
- Horspool, A.M.; Kieffer, T.; Russ, B.P.; DeJong, M.A.; Wolf, M.A.; Karakiozis, J.M.; Hickey, B.J.; Fagone, P.; Tacker, D.H.; Bevere, J.R.; et al. Interplay of Antibody and Cytokine Production Reveals CXCL13 as a Potential Novel Biomarker of Lethal SARS-CoV-2 Infection. mSphere 2021, 6, e01324-20. [Google Scholar] [CrossRef]
- Ibrahim, S.A.; Boudova, S.; Rouse, C.E.; Shanks, A.L.; Reinhardt, J.; Scifres, C. ABO blood group, rhesus type and risk of COVID-19 in pregnant women. Am. J. Obstet. Gynecol. 2021, 224, S605. [Google Scholar] [CrossRef]
- Tayebi Khosroshahi, H.; Mardomi, A.; Niknafs, B.; Farnood, F.; Shekarchi, M.; Salehi, S.; FadaeiHaggi, T. Current status of COVID-19 among hemodialysis patients in the East Azerbaijan Province of Iran. Hemodial. Int. 2021, 25, 214–219. [Google Scholar] [CrossRef]
- Kolin, D.A.; Kulm, S.; Christos, P.J.; Elemento, O. Clinical, regional, and genetic characteristics of Covid-19 patients from UK Biobank. PLoS ONE 2020, 15, e0241264. [Google Scholar] [CrossRef]
- Latz, C.A.; DeCarlo, C.; Boitano, L.; Png, C.Y.M.; Patell, R.; Conrad, M.F.; Eagleton, M.; Dua, A. Blood type and outcomes in patients with COVID-19. Ann. Hematol. 2020, 99, 2113–2118. [Google Scholar] [CrossRef]
- Lehrer, S.; Rheinstein, P.H. ABO blood groups, COVID-19 infection and mortality. Blood Cells Mol. Dis. 2021, 89, 102571. [Google Scholar] [CrossRef] [PubMed]
- Levi, J.E.; Telles, P.R.; Scrivani, H.; Campana, G. Lack of association between ABO blood groups and susceptibility to SARS-CoV-2 infection. Vox. Sang. 2021, 116, 251–252. [Google Scholar] [CrossRef] [PubMed]
- Mahallawi, W.H.; Al-Zalabani, A.H. The seroprevalence of SARS-CoV-2 IgG antibodies among asymptomatic blood donors in Saudi Arabia. Saudi J. Biol. Sci. 2021, 28, 1697–1701. [Google Scholar] [CrossRef] [PubMed]
- Niles, J.K.; Karnes, H.E.; Dlott, J.S.; Kaufman, H.W. Association of ABO/Rh with SARS-CoV-2 positivity: The role of race and ethnicity in a female cohort. Am. J. Hematol. 2021, 96, E23–E26. [Google Scholar] [CrossRef]
- Quiroga, B.; Sánchez-Álvarez, E.; Ortiz, A.; de Sequera, P. Spanish Society of Nephrology Suboptimal personal protective equipment and SARS-CoV-2 infection in Nephrologists: A Spanish national survey. Clin. Kidney J. 2021, 14, 1216–1221. [Google Scholar] [CrossRef]
- Ray, J.G.; Schull, M.J.; Vermeulen, M.J.; Park, A.L. Association Between ABO and Rh Blood Groups and SARS-CoV-2 Infection or Severe COVID-19 Illness: A Population-Based Cohort Study. Ann. Intern. Med. 2021, 174, 308–315. [Google Scholar] [CrossRef]
- Schetelig, J.; Baldauf, H.; Wendler, S.; Heidenreich, F.; Real, R.; Kolditz, M.; Rosner, A.; Dalpke, A.; de With, K.; Lange, V.; et al. Blood group A epitopes do not facilitate entry of SARS-CoV-2. J. Intern. Med. 2021, 290, 223–226. [Google Scholar] [CrossRef]
- Zhang, J.; Pellicori, P.; Schutte, R.; Cleland, J.G. The association between blood groups and COVID-19 infection: A study from the UK Biobank. J. Intern. Med. 2021, 289, 747–748. [Google Scholar] [CrossRef]
- Nordgren, J.; Svensson, L. Genetic Susceptibility to Human Norovirus Infection: An Update. Viruses 2019, 11, 226. [Google Scholar] [CrossRef] [Green Version]
- Lebiush, M.; Rannon, L.; Kark, J.D. The relationship between epidemic influenza (A(H1N1) and ABO blood group. J. Hyg. 1981, 87, 139–146. [Google Scholar] [CrossRef]
- Siransy, L.K.; Nanga, Z.Y.; Zaba, F.S.; Tufa, N.Y.; Dasse, S.R. ABO/Rh Blood Groups and Risk of HIV Infection and Hepatitis B Among Blood Donors of Abidjan, Côte D’ivoire. Eur. J. Microbiol. Immunol. 2015, 5, 205–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, Y.; Cheng, G.; Chui, C.H.; Lau, F.Y.; Chan, P.K.; Ng, M.H.; Sung, J.J.; Wong, R.S. ABO blood group and susceptibility to severe acute respiratory syndrome. JAMA 2005, 293, 1450–1451. [Google Scholar] [PubMed]
- Gérard, C.; Maggipinto, G.; Minon, J.M. COVID-19 and ABO blood group: Another viewpoint. Br. J. Haematol. 2020, 190, e93–e94. [Google Scholar] [CrossRef] [PubMed]
- Arend, P. Why blood group A individuals are at risk whereas blood group O individuals are protected from SARS-CoV-2 (COVID-19) infection: A hypothesis regarding how the virus invades the human body via ABO(H) blood group-determining carbohydrates. Immunobiology 2021, 226, 152027. [Google Scholar] [CrossRef]
- Guillon, P.; Clément, M.; Sébille, V.; Rivain, J.G.; Chou, C.F.; Ruvoën-Clouet, N.; Le Pendu, J. Inhibition of the interaction between the SARS-CoV spike protein and its cellular receptor by anti-histo-blood group antibodies. Glycobiology 2008, 18, 1085–1093. [Google Scholar] [CrossRef] [Green Version]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy region, Italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [Green Version]
- Hussain, A.; Mahawar, K.; Xia, Z.; Yang, W.; El-Hasani, S. Obesity and mortality of COVID-19. Meta-analysis. Obes. Res. Clin. Pract. 2020, 14, 295–300. [Google Scholar] [CrossRef]
- Wu, B.B.; Gu, D.Z.; Yu, J.N.; Yang, J.; Shen, W.Q. Association between ABO blood groups and COVID-19 infection, severity and demise: A systematic review and meta-analysis. Infect. Genet. Evol. 2020, 84, 104485. [Google Scholar] [CrossRef]
- Pourali, F.; Afshari, M.; Alizadeh-Navaei, R.; Javidnia, J.; Moosazadeh, M.; Hessami, A. Relationship between blood group and risk of infection and death in COVID-19: A live meta-analysis. New Microbes New Infect. 2020, 37, 100743. [Google Scholar] [CrossRef]
- Liu, N.; Zhang, T.; Ma, L.; Zhang, H.; Wang, H.; Wei, W.; Pei, H.; Li, H. The impact of ABO blood group on COVID-19 infection risk and mortality: A systematic review and meta-analysis. Blood Rev. 2021, 48, 100785. [Google Scholar] [CrossRef]
- Li, J.; Wang, X.; Chen, J.; Cai, Y.; Deng, A.; Yang, M. Association between ABO blood groups and risk of SARS-CoV-2 pneumonia. Br. J. Haematol. 2020, 190, 24–27. [Google Scholar] [CrossRef] [PubMed]
- Golinelli, D.; Boetto, E.; Maietti, E.; Fantini, M.P. The association between ABO blood group and SARS-CoV-2 infection: A meta-analysis. PLoS ONE 2020, 15, e0239508. [Google Scholar] [CrossRef] [PubMed]
- Franchini, M.; Cruciani, M.; Mengoli, C.; Marano, G.; Candura, F.; Lopez, N.; Pati, I.; Pupella, S.; De Angelis, V. ABO blood group and COVID-19: An updated systematic literature review and meta-analysis. Blood Transfus. 2021, 19, 317–326. [Google Scholar] [PubMed]
- Gutiérrez-Valencia, M.; Leache, L.; Librero, J.; Jericó, C.; Enguita Germán, M.; García-Erce, J.A. ABO blood group and risk of COVID-19 infection and complications: A systematic review and meta-analysis. Transfusion 2021, 62, 493–505. [Google Scholar] [CrossRef] [PubMed]
- Kabrah, S.M.; Kabrah, A.M.; Flemban, A.F.; Abuzerr, S. Systematic review and meta-analysis of the susceptibility of ABO blood group to COVID-19 infection. Transfus. Apher. Sci. 2021, 60, 103169. [Google Scholar] [CrossRef] [PubMed]
- Gallian, P.; Pastorino, B.; Morel, P.; Chiaroni, J.; Ninove, L.; de Lamballerie, X. Lower prevalence of antibodies neutralizing SARS-CoV-2 in group O French blood donors. Antiviral. Res. 2020, 181, 104880. [Google Scholar] [CrossRef]
- Franchini, M.; Glingani, C.; Del Fante, C.; Capuzzo, M.; Di Stasi, V.; Rastrelli, G.; Vignozzi, L.; De Donno, G.; Perotti, C. The protectiveeffect of O bloodtypeagainst SARS-CoV-2 infection. Vox. Sang. 2021, 116, 249–250. [Google Scholar] [CrossRef] [PubMed]
- Ahn, E.; Kang, H. Introduction to systematic review and meta-analysis. Korean J. Anesthesiol. 2018, 71, 103–112. [Google Scholar] [CrossRef] [Green Version]
- McVey, J.; Baker, D.; Parti, R.; Berg, R.; Gudino, M.; Teschner, W. Anti-A and anti-B titers in donor plasma, plasma pools, and immunoglobulin final products. Transfusion 2015, 55, S98–S104. [Google Scholar] [CrossRef]
- Liu, Y.J.; Chen, W.; Wu, K.W.; Broadberry, R.E.; Lin, M. The development of ABO isohemagglutinins in Taiwanese. Hum. Hered. 1996, 46, 181–184. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Country | Study Period | Study Design | Participants Included in This Review § | SARS-CoV-2 Positive Patients | SARS-CoV-2 Negative Patients | Gender (M) | Age (Years) | Diagnostic Test |
|---|---|---|---|---|---|---|---|---|---|
| Ad’hiah et al., 2020 [22] | Iraq | 31 May to 31 July 2020 | Case-control | 1915 | Hospitalized patients | Blood donors | 58.3% | Mean age 39.6 | PCR |
| Ahmed I et al., 2021 [26] | UK | 24 April to 6 May 2020 | Cohort/Cross-sectional | 355 | Pregnant women | Pregnant women | 0.0% | Mean age 30.8 | PCR |
| Anderson JL et al., 2021 [23] | USA | 3 March to 2 November 2020 | Case-control | 107,796 | General population | General population | 23.1% | Mean age 42.0 | PCR |
| Barnkob MB et al., 2020 [27] | Denmark | 27 February to 30 July 2020 | Cohort/Cross-sectional | 473,654 | General population | General population | 29.0% | ≥60 years: 35.2% 1 | PCR |
| Boudin L et al., 2020 [28] | France | 28 February to 13 April 2020 | Cohort/Cross-sectional | 1669 | Crewmembers | Crewmembers | 87.0% a | Median age 28.0 | PCR |
| Coluk Y et al., 2021 [29] | Turkey | NR | Cohort/Cross-sectional | 211 | General population | General population | NR | Subjects > 18 years | PCR |
| Haizler-Cohen L et al., 2021 [30] | USA | 27 May to 28 August 2020 | Cohort/Cross-sectional | 2930 | Pregnant women | Pregnant women | 0.0% | Women of reproductive age | Antibody |
| Horspool A et al., 2021 [31] | USA | NR | Cohort/Cross-sectional | 64 | Hospitalized patients | Hospitalized patients | 56.3% | Range: 15–92 | Antibody |
| Ibrahim SA et al., 2021 [32] | USA | 1 March to 31 May 2020 | Cohort/Cross-sectional | 586 | Pregnant women | Pregnant women | 0.0% | Women of reproductive age | PCR or antigen |
| Khosroshahi HT et al., 2021 [33] | Iran | Until 1 July 2020 | Cohort/Cross-sectional | 670 | Haemodialysis patients | Haemodialysis patients | 64.5% | Range: 19–88 | PCR |
| Kolin DA et al., 2020 [34] | UK | 16 March to 18 May 2020 | Cohort/Cross-sectional | 4811 | General population | General population | 53.8% 1 | Range: 40–69 | PCR |
| Latz CA et al., 2020 [35] | USA | 6 March to 16 April 2020 | Cohort/Cross-sectional | 7648 | General population | General population | 32.4% 1 | Subjects > 18 years | PCR or antigen |
| Lehrer S et al., 2021 [36] | UK | 16 March to 26 April 2020 | Cohort/Cross-sectional | 12,575 | Community volunteers | Community volunteers | 47.8% | Range: 40–70 | PCR |
| Levi JE et al., 2021 [37] | Brazil | Until 22 June 2020 | Cohort/Cross-sectional | 6457 | General population | General population | NR | NR | PCR and/or antibody |
| Mahallawi AH et al., 2021 [38] | Saudi Arabia | Mid-May to mid-July, 2020 | Cohort/Cross-sectional | 1212 | Blood donors | Blood donors | 100.0% | Range: 18–64 | Antibody |
| Negro P et al., 2021 [18] | Italy | 28 February to 23 April 2020 | Case-control | 1058 | General population | General population | 46.2% | Range: 1–100 | PCR |
| Niles JK et al., 2020 [39] | USA | March to July 2020 | Cohort/Cross-sectional | 276,536 | Pregnant women at the time of ABO testing | Pregnant women at the time of ABO testing | 0.0% | Median age 34.4 | RNA NAAT |
| Platton S et al., 2021 [24] | UK | NR | Case-control | 40 | Hospitalized patients in critical care unit | Hospitalized patients in critical care unit | 82.5% | Range: 22–78 | PCR |
| Quiroga B et al., 2021 [40] | Spain | Until 1 November 2020 | Cohort/Cross-sectional | 320 | Nephrologists | Nephrologists | 33.6% b | Mean age 46.0 | Self-reported |
| Ray JG et al., 2021 [41] | Canada | 15 January to 30 June 2020 | Cohort/Cross-sectional | 225,556 | General population | General population | 29.1% | Mean age 54.0 | PCR |
| Schetelig J et al., 2021 [42] | Germany | January to September 2020 | Cohort/Cross-sectional | 102,342 | Stem cell Donors | Stem cell Donors | 29.8% c | Range: 18–61 | PCR |
| Singh N et al., 2021 [25] | USA | 1 April to 30 June 2020 | Case-control | 100 | Pregnant women | Pregnant women | 0.0% | Range: 17–42 | PCR or antigen |
| Zhang J et al., 2021 [43] | UK | By 24 August 2020 | Cohort/Cross-sectional | 17,586 | Community volunteers | Community volunteers | 48.0% | Range: 38–73 | PCR |
| Study | Blood Group A | Blood Group B | Blood Group AB | Blood Group O | Overall | ||||
|---|---|---|---|---|---|---|---|---|---|
| Risk | Pos./Tot. | Risk | Pos./Tot. | Risk | Pos./Tot. | Risk | Pos./Tot. | Risk | |
| Ahmed et al., 2021 [26] | 27.0% | 34/126 | 28.4% | 19/67 | 41.4% | 12/29 | 15.8% | 21/133 | 24.2% |
| Barnkob et al., 2020 [27] | 1.6% | 3296/202,507 | 1.7% | 897/53,735 | 1.8% | 378/21,160 | 1.5% | 2851/196,252 | 1.6% |
| Boudin et al., 2020 [28] | 77.3% | 521/674 | 73.8% | 135/183 | 77.1% | 54/70 | 74.5% | 553/742 | 75.7% |
| Coluk et al., 2021 [29] | 68.3% | 69/101 | 62.5% | 20/32 | 55.6% | 5/9 | 72.5% | 50/69 | 68.2% |
| Haizler-Cohen et al., 2021 [30] | 15.2% | 145/955 | 14.2% | 72/508 | 14.9% | 22/148 | 15.8% | 209/1319 | 15.3% |
| Horspool et al., 2021 [31] | 17.4% | 4/23 | 22.2% | 2/9 | 0.0% | 0/2 | 13.3% | 4/30 | 15.6% |
| Ibrahim et al., 2021 [32] | 10.2% | 18/176 | 8.0% | 7/88 | 6.3% | 1/16 | 13.1% | 40/306 | 11.3% |
| Khosroshahi et al., 2021 [33] | 9.3% | 21/225 | 6.9% | 11/160 | 0.0% | 0/52 | 5.2% | 12/233 | 6.6% |
| Latz et al., 2020 [35] | 16.6% | 440/2649 | 19.4% | 201/1035 | 19.8% | 61/308 | 16.1% | 587/3656 | 16.9% |
| Lehrer et al., 2021 [36] | 5.9% | 323/5516 | 5.3% | 66/1238 | 5.3% | 23/431 | 5.7% | 308/5390 | 5.7% |
| Levi et al., 2021 [37] | 32.6% | 816/2505 | 33.2% | 237/713 | 30.0% | 71/237 | 30.4% | 913/3002 | 31.5% |
| Mahallawi et al., 2021 [38] | 29.2% | 117/401 | 12.6% | 32/253 | 16.4% | 9/55 | 15.1% | 76/503 | 19.3% |
| Niles et al., 2020 [39] | 11.8% | 11,017/93,750 | 11.8% | 4282/36,140 | 11.4% | 1153/10,133 | 13.0% | 17,739/136,513 | 12.4% |
| Quiroga et al., 2021 [40] | 21.9% | 34/155 | 15.2% | 5/33 | 25.0% | 2/8 | 15.3% | 19/124 | 18.8% |
| Ray et al., 2021 [41] | 3.0% | 2420/81,797 | 4.1% | 1378/33,536 | 3.8% | 390/10,221 | 2.9% | 2883/100,002 | 3.1% |
| Schetelig et al., 2021 [42] | 5.3% | 2345/44,131 | 4.8% | 570/11,866 | 5.3% | 285/5370 | 4.7% | 1916/40,975 | 5.0% |
| Zhang et al., 2021 [43] | 9.4% | 728/7744 | 10.0% | 177/1763 | 9.1% | 56/613 | 9.1% | 682/7466 | 9.3% |
| (a) | ||||||
|---|---|---|---|---|---|---|
| Study | Selection | Exposure | ||||
| Is the Case Definition Adequate? | Representativeness of the Cases | Selection of Controls | Definition of Controls | Ascertainment of Exposure | Same Method of Ascertainment for Cases and Controls | |
| Ad’hiah AH, et al., 2020 [22] | * | * | * | * | * | * |
| Anderson JL, et al., 2021 [23] | * | * | * | * | * | * |
| Negro P, et al., 2021 [18] | * | * | * | * | * | * |
| Platton S, et al., 2021 [24] | * | * | * | * | ||
| Singh N, et al., 2021 [25] | * | * | * | * | * | |
| (b) | ||||||
| Study | Selection | Outcome | ||||
| Representativeness of the exposed cohort | Selection of the non-exposed cohort | Ascertainment of exposure | Demonstration that outcome of interest was not present at start of study | Assessment of outcome | ||
| Ahmed I, et al., 2021 [26] | * | * | * | * | * | |
| Barnkob MB, et al., 2020 [27] | * | * | * | * | * | |
| Boudin L, et al., 2020 [28] | * | * | * | * | * | |
| Coluk Y, et al., 2021 [29] | * | * | * | * | * | |
| Haizler-Cohen L, et al., 2021 [30] | * | * | * | * | * | |
| Horspool A, et al., 2021 [31] | * | * | * | * | * | |
| Ibrahim SA, et al., 2021 [32] | * | * | * | * | * | |
| Khosroshahi HT, et al., 2021 [33] | * | * | * | * | * | |
| Latz CA, et al., 2020 [35] | * | * | * | * | * | |
| Lehrer S, et al., 2021 [36] | * | * | * | * | * | |
| Levi JE, et al., 2021 [37] | * | * | * | * | * | |
| Mahallawi AH, et al., 2021 [38] | * | * | * | * | * | |
| Niles JK, et al., 2021 [39] | * | * | * | * | * | |
| Quiroga B, et al., 2021 [40] | * | * | * | |||
| Ray JG, et al., 2021 [41] | * | * | * | * | * | |
| Schetelig J, et al., 2021 [42] | * | * | * | * | * | |
| Zhang J, et al., 2021 [43] | * | * | * | * | * | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Banchelli, F.; Negro, P.; Guido, M.; D’Amico, R.; Fittipaldo, V.A.; Grima, P.; Zizza, A. The Role of ABO Blood Type in Patients with SARS-CoV-2 Infection: A Systematic Review. J. Clin. Med. 2022, 11, 3029. https://doi.org/10.3390/jcm11113029
Banchelli F, Negro P, Guido M, D’Amico R, Fittipaldo VA, Grima P, Zizza A. The Role of ABO Blood Type in Patients with SARS-CoV-2 Infection: A Systematic Review. Journal of Clinical Medicine. 2022; 11(11):3029. https://doi.org/10.3390/jcm11113029
Chicago/Turabian StyleBanchelli, Federico, Pierpaolo Negro, Marcello Guido, Roberto D’Amico, Veronica Andrea Fittipaldo, Pierfrancesco Grima, and Antonella Zizza. 2022. "The Role of ABO Blood Type in Patients with SARS-CoV-2 Infection: A Systematic Review" Journal of Clinical Medicine 11, no. 11: 3029. https://doi.org/10.3390/jcm11113029
APA StyleBanchelli, F., Negro, P., Guido, M., D’Amico, R., Fittipaldo, V. A., Grima, P., & Zizza, A. (2022). The Role of ABO Blood Type in Patients with SARS-CoV-2 Infection: A Systematic Review. Journal of Clinical Medicine, 11(11), 3029. https://doi.org/10.3390/jcm11113029